
Well-Controlled Viremia Predicts the Outcome of Hepatocellular Carcinoma in Chronic Viral Hepatitis Patients Treated with Sorafenib

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
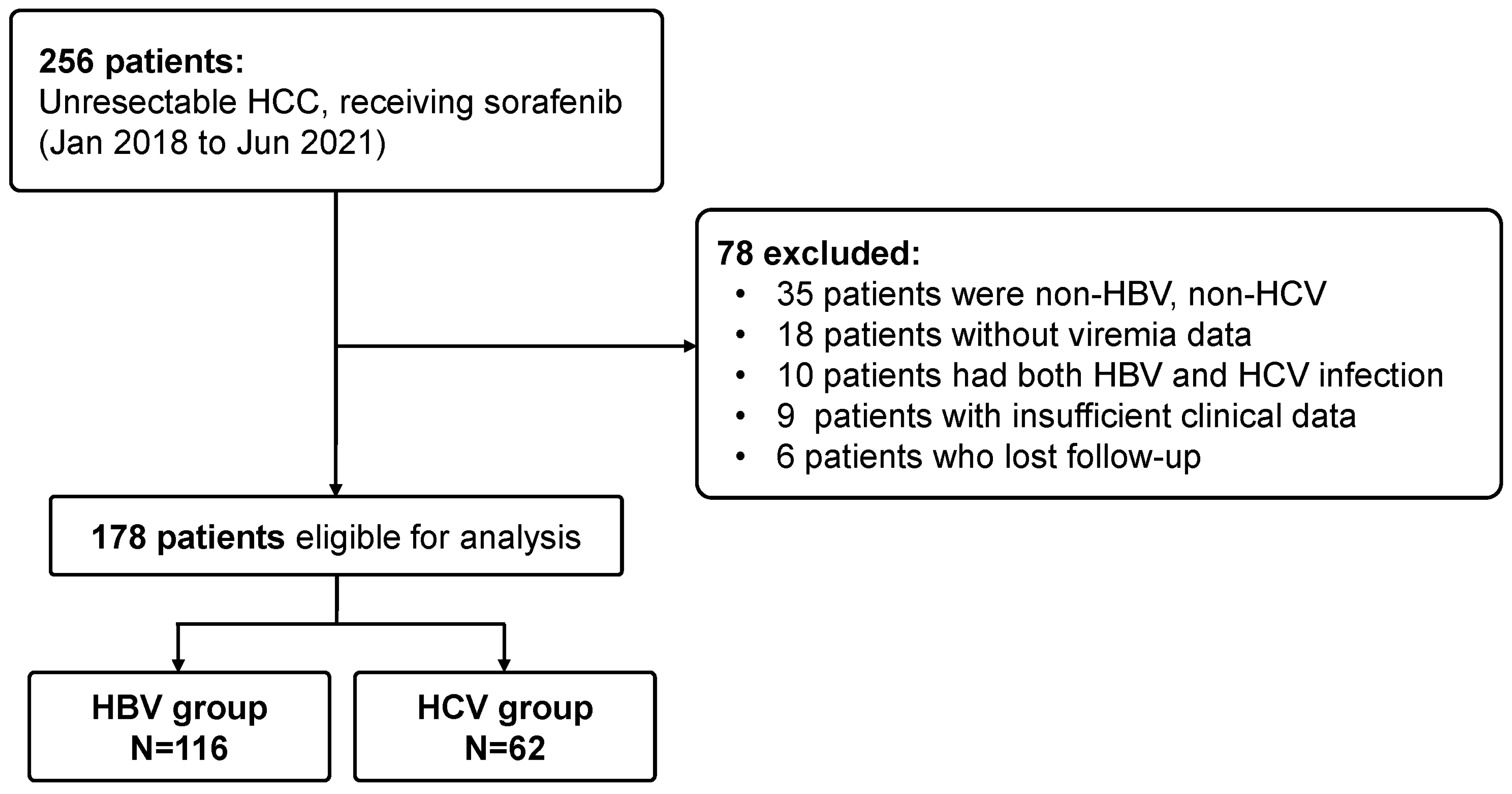
2.1. Study Cohort
2.2. Treatment Outcome
2.3. Management of Antiviral Therapy
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Status of Viremia Control
3.3. Treatment Response
3.4. Treatment Safety
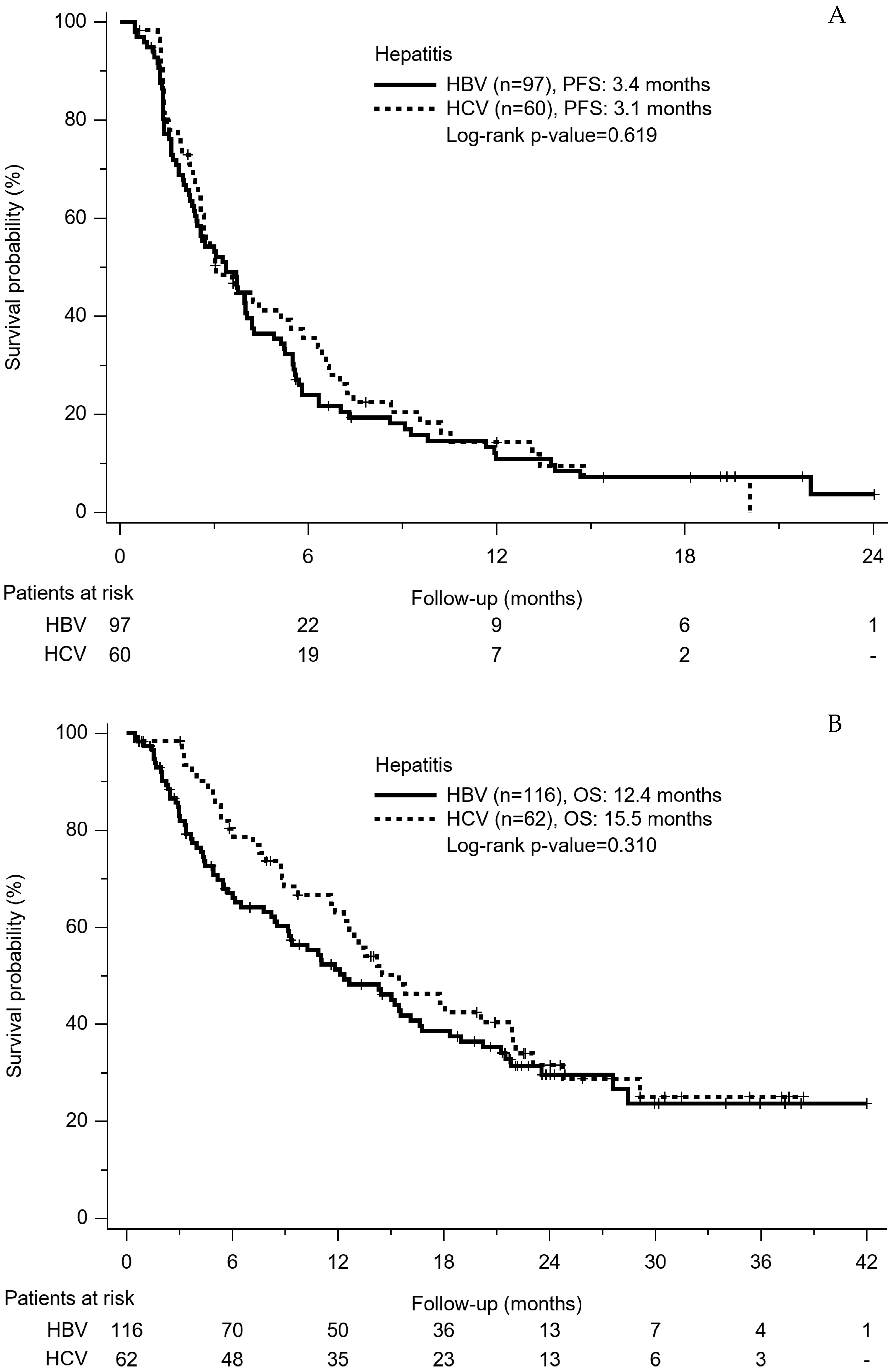
3.5. PFS and OS Based on Virus Hepatitis
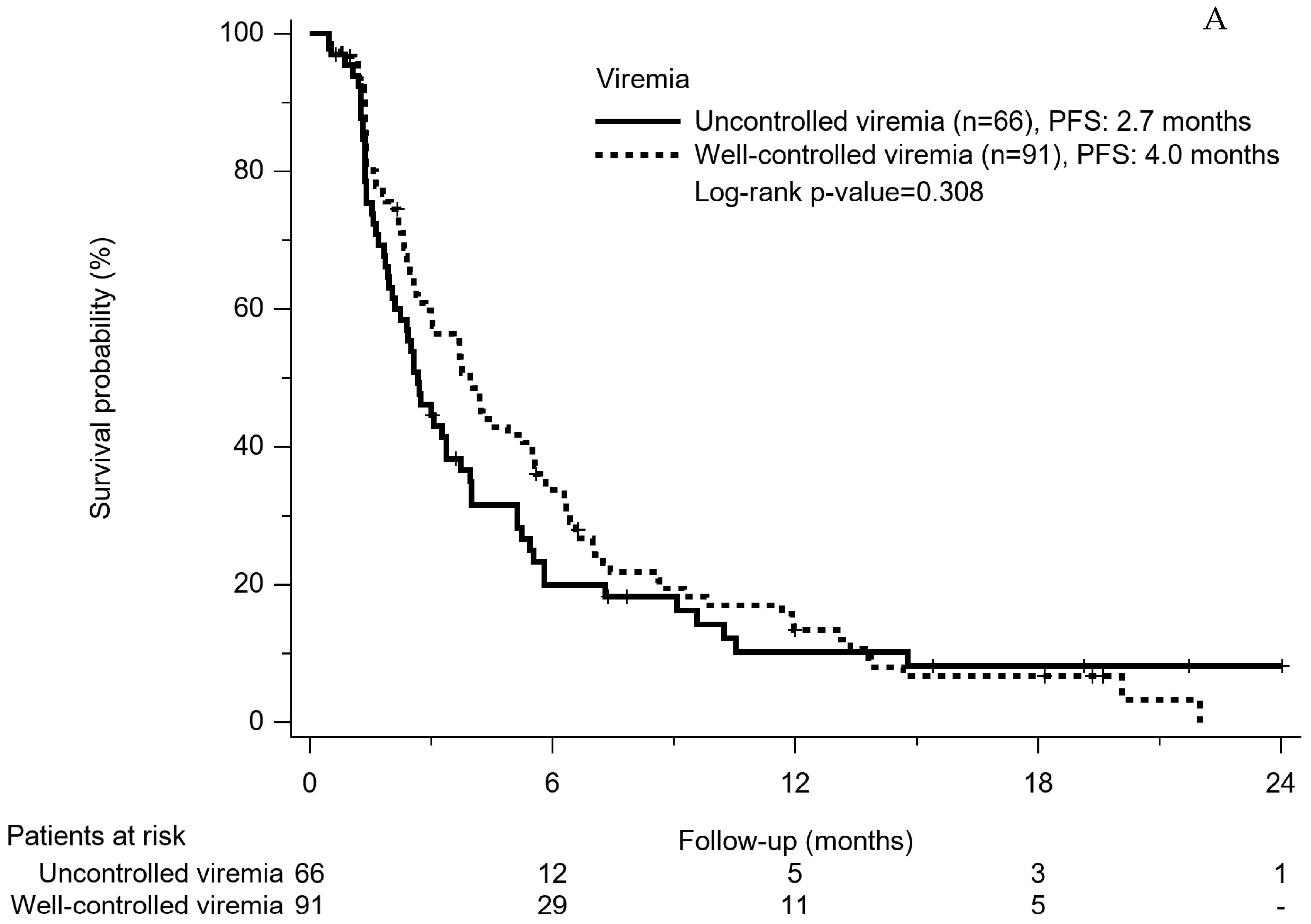
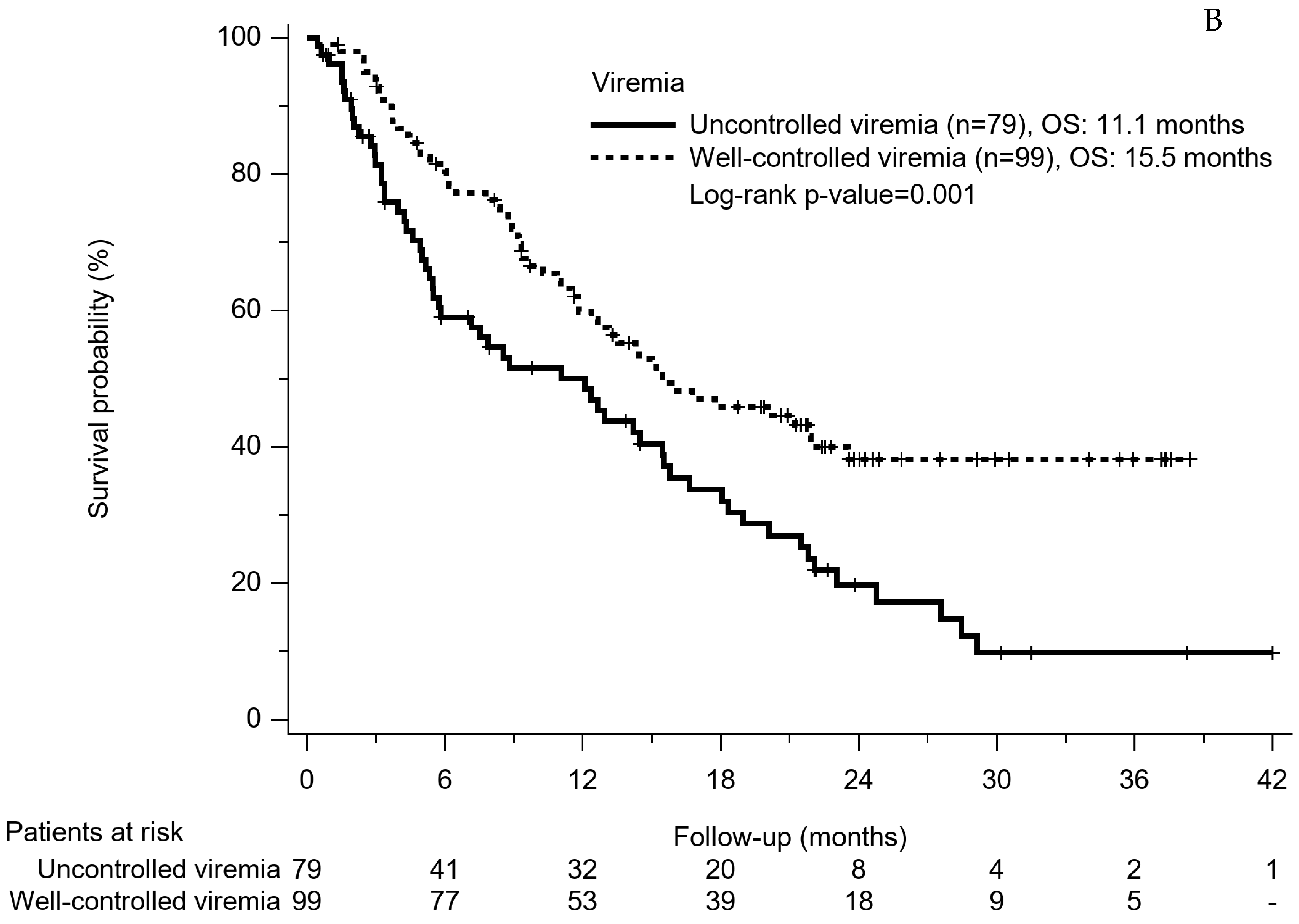
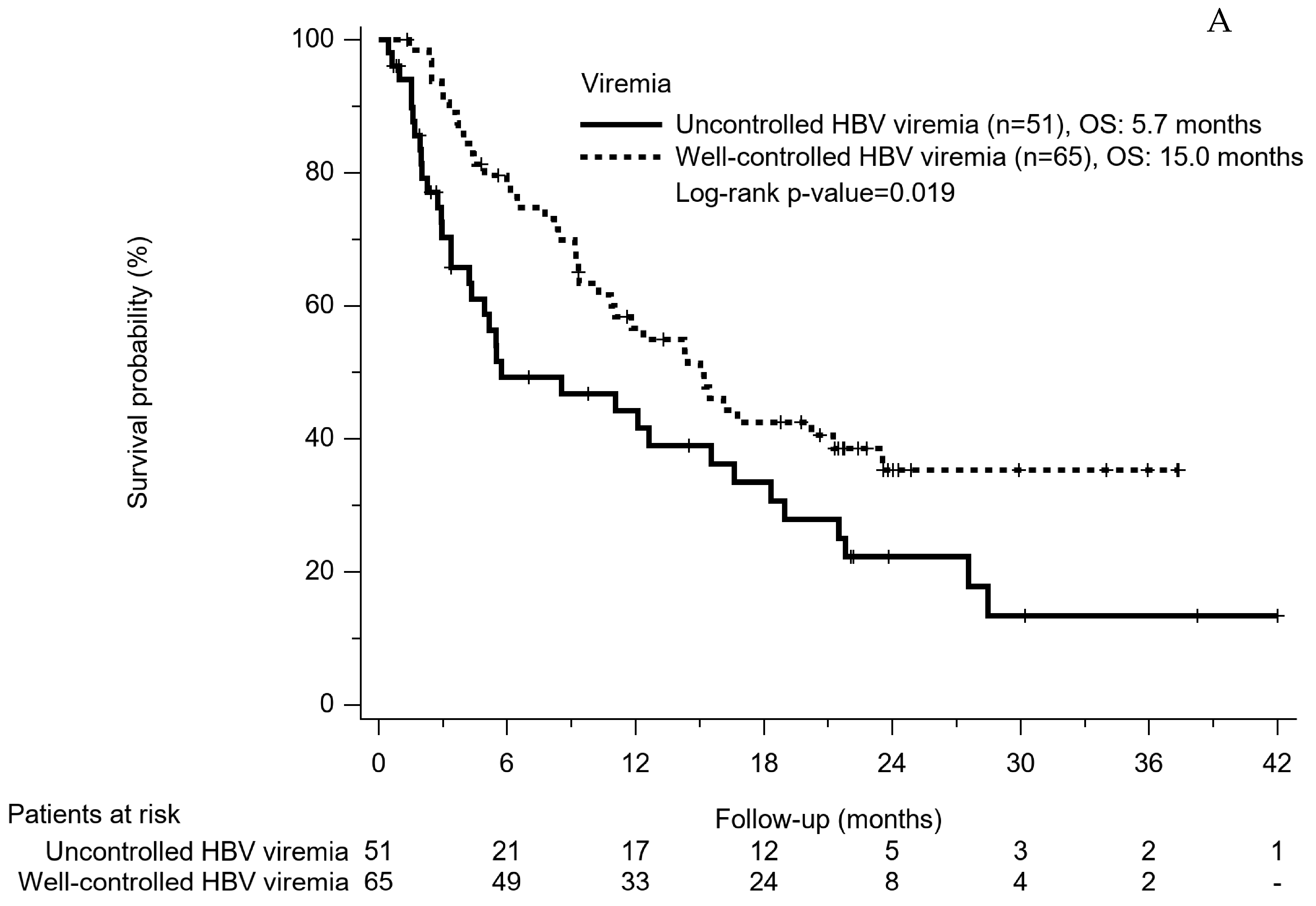
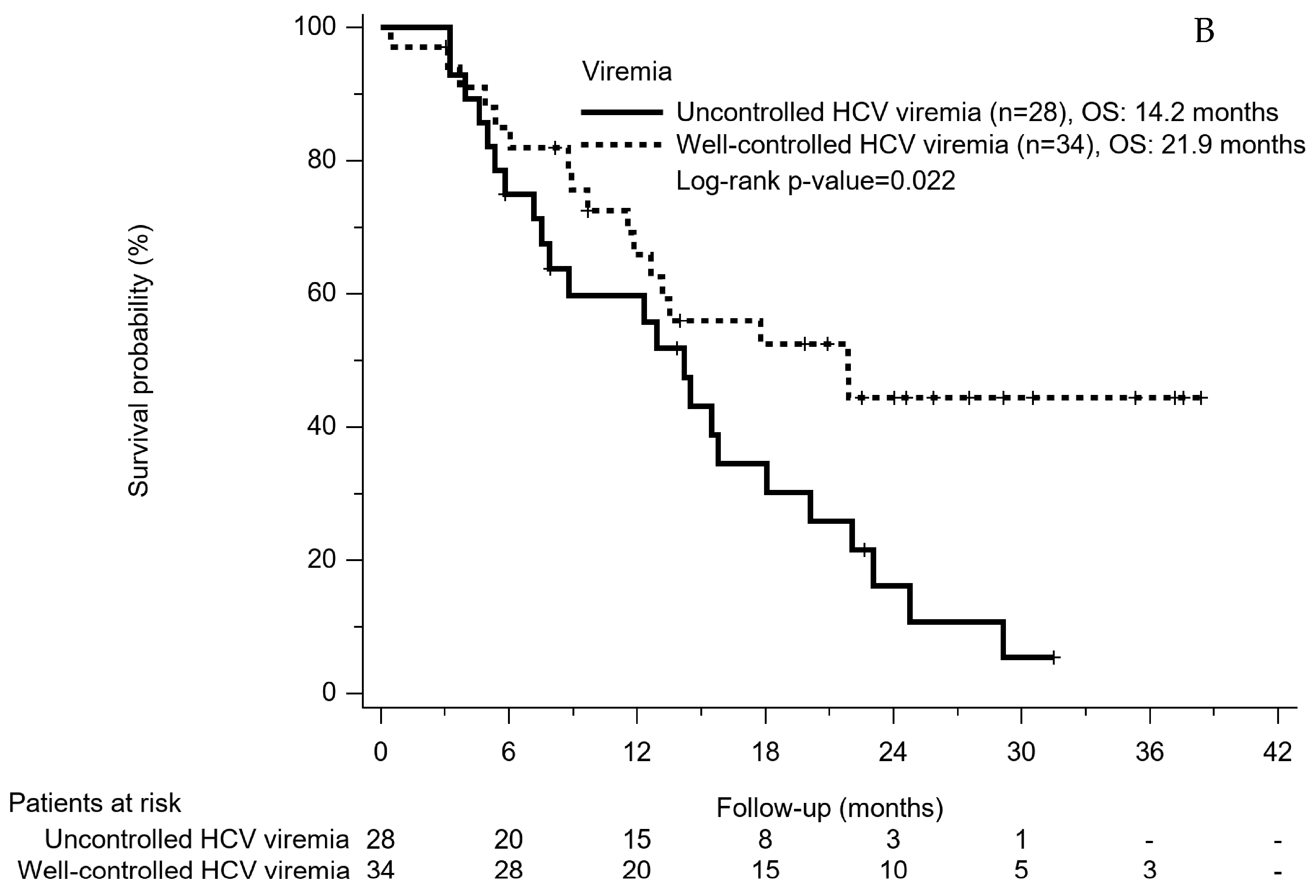
3.6. PFS and OS Based on Viremia Control
3.7. PFS and OS Based on Virus Hepatitis plus Viremia Control
3.8. Factors Associated with OS
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare of Taiwan. Cancer Registry Annual Report 1972–2015; Health Promotion Administration, Ministry of Health and Welfare: Taipei, Taiwan, 2015. [Google Scholar]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rsomorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.H.; Park, J.W.; et al. Cabozantinib in Patients with Advanced and rogressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Parcht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Trojan, J.; Welling, T.H.; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Finn, R.S.; Ryoo, B.Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.Y.; Breder, V.V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Pembrolizumab As Second-Line Therapy in Patients with Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2020, 38, 193–202. [Google Scholar] [CrossRef]
- McGlynn, K.A.; Petrick, J.L.; London, W.T. Global epidemiology of hepatocellular carcinoma: An emphasis on demographic and regional variability. Clin. Liver. Dis. 2015, 19, 223–238. [Google Scholar] [CrossRef]
- Wang, C.C.; Kao, J.H. How have the recent advances in antiviral therapy impacted the management of virus-related hepatocellular carcinoma? Expert Opin. Pharmacother. 2016, 17, 911–919. [Google Scholar] [CrossRef]
- Wu, C.Y.; Chen, Y.J.; Ho, H.J.; Hsu, Y.C.; Kuo, K.N.; Wu, M.S.; Lin, J.T. Association between nucleoside analogues and risk of hepatitis B virus–related hepatocellular carcinoma recurrence following liver resection. JAMA 2012, 308, 1906–1914. [Google Scholar] [CrossRef]
- Wu, K.C.; Lee, I.C.; Chi, C.T.; Lei, H.J.; Chau, G.Y.; Yeh, Y.C.; Su, C.W.; Huo, T.I.; Chao, Y.; Lin, H.C.; et al. Comparable benefits of HCV eradication by direct acting antivirals and interferon-based therapy in patients with hepatocellular carcinoma undergoing surgical resection. Am. J. Cancer Res. 2021, 11, 5526–5542. [Google Scholar] [PubMed]
- Lim, S.; Han, J.; Kim, G.M.; Han, K.H.; Choi, H.J. Hepatitis B viral load predicts survival in hepatocellular carcinoma patients treated with sorafenib. J. Gastroenterol. Hepatol. 2015, 30, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Gao, H.; Huang, J.; Wang, H.; Zhou, Z.; Zhang, Y.; Li, S.; Chen, M. Antiviral therapy in the improvement of survival of patients with hepatitis B virus-related hepatocellular carcinoma treated with sorafenib. J. Gastroenterol. Hepatol. 2015, 30, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.H.; Wang, J.H.; Chang, K.C.; Hung, C.H.; Lu, S.N.; Hu, T.H.; Yen, Y.H.; Kee, K.M.; Chen, C.H. The influence of direct-acting antivirals in hepatitis C virus related hepatocellular carcinoma after curative treatment. Investig. New Drugs 2020, 38, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Jackson, R.; Psarelli, E.E.; Berhane, S.; Khan, H.; Johnson, P. Impact of Viral Status on Survival in Patients Receiving Sorafenib for Advanced Hepatocellular Cancer: A Meta-Analysis of Randomized Phase III Trials. J. Clin. Oncol. 2017, 35, 622–628. [Google Scholar] [CrossRef]
- Bruix, J.; Cheng, A.L.; Meinhardt, G.; Nakajima, K.; De Sanctis, Y.; Llovet, J. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: Analysis of two phase III studies. J. Hepatol. 2017, 67, 999–1008. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- Omata, M.; Kanda, T.; Wei, L.; Yu, M.L.; Chuang, W.L.; Ibrahim, A.; Lsemana, C.R.A.; Sollano, J.; Kumar, M.; Jindal, A.; et al. APASL consensus statements and recommendation on treatment of hepatitis C. Hepatol. Int. 2016, 10, 702–726. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.; Park, J.W.; Finn, R.S.; Cheng, A.L.; Mathurin, P.; Edeline, J.; Kudo, M.; Harding, J.; Merle, P.; Rosmorduc, O.; et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): A randomised, multicentre, open-label, phase 3 trial. Lancet. Oncol. 2022, 23, 77–90. [Google Scholar] [CrossRef]
- Nagai, H.; Mukozu, T.; Matsui, D.; Kanekawa, T.; Kanayama, M.; Wakui, N.; Momiyama, K.; Shinohara, M.; Iida, K.; Ishii, K.; et al. Sorafenib prevents escape from host immunity in liver cirrhosis patients with advanced hepatocellular carcinoma. Clin. Dev. Immunol. 2012, 2012, 607851. [Google Scholar] [CrossRef]
- Lee, Y.C.; Wang, J.H.; Chen, C.H.; Hung, C.H.; Lo, K.C.; Yen, Y.H.; Kee, K.M.; Hu, T.H.; Lu, S.N.; Kuo, Y.H. Sorafenib use in hepatitis B virus- or hepatitis C virus-related hepatocellular carcinoma: A propensity score matching study. Kaohsiung J. Med. Sci. 2021, 37, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Lau, G.K.K.; Wei, L.; Moriyama, M.; Yu, M.L.; Chuang, W.L.; Ibrahim, A.; Lesmana, C.R.A.; Sollano, J.; Kumar, M.; et al. APASL HCV guidelines of virus-eradicated patients by DAA on how to monitor HCC occurrence and HBV reactivation. Hepatol. Int. 2019, 13, 649–661. [Google Scholar] [CrossRef]
- Lin, W.C.; Lin, Y.S.; Chang, C.W.; Chang, C.W.; Wang, T.E.; Wang, H.Y.; Chen, M.J. Impact of direct-acting antiviral therapy of hepatitis C-related hepatocellular carcinoma. PLoS ONE 2020, 15, e0233212. [Google Scholar] [CrossRef]
- Kuwano, A.; Yada, M.; Nagasawa, S.; Tanaka, K.; Morita, Y.; Masumoto, A.; Motomuro, K. Hepatitis C virus eradication ameliorates the prognosis of advanced hepatocellular carcinoma treated with sorafenib. J. Viral. Hepat. 2022, 29, 543–550. [Google Scholar] [CrossRef]
- Seko, Y.; Moriguchi, M.; Takahashi, A.; Yamaguchi, K.; Umemura, A.; Okuda, K.; Kataoka, S.; Unozawa, H.; Kobayashi, K.; Ogasawara, S.; et al. Hepatitis C virus eradication prolongs overall survival in hepatocellular carcinoma patients receiving molecular-targeted agents. J. Gastroenterol. 2022, 57, 90–98. [Google Scholar] [CrossRef]
- Tsai, H.Y.; Chang, H.P.; Chen, C.J.; Hsu, W.L.; Huang, L.Y.; Lee, P.C. Effects of direct-acting antiviral therapy for patients with advanced hepatocellular carcinoma and concomitant hepatitis C-A population-based cohort study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7543–7552. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 178) | HBV-HCC (n = 116) | HCV-HCC (n = 62) | p-Value | |
|---|---|---|---|---|
| Follow-up interval, months | 13.4 ± 10.2 | 12.3 ± 10.1 | 15.3 ± 9.9 | 0.061 |
| Age(years) | 64.8 ± 11.4 | 61.7 ± 11.6 | 70.5 ± 8.7 | <0.001 |
| Male sex, n (%) | 135 (75.8) | 93 (80.2) | 42 (67.7) | 0.065 |
| Child-Pugh class, A, n (%) | 174 (97.8) | 115 (99.1) | 59 (95.2) | 0.088 |
| B, n (%) | 4 (2.2) | 1 (0.9) | 3 (4.8) | |
| ALBI grade 1, n (%) | 84 (47.2) | 53 (45.7) | 31 (50) | 0.563 |
| 2, n (%) | 94 (52.8) | 63 (54.3) | 31 (50) | |
| BCLC stage, B, n (%) | 32 (18) | 18 (15.5) | 14 (22.6) | 0.242 |
| C, n (%) | 146 (82) | 98 (84.5) | 48 (77.4) | |
| EHM, n (%) | 78 (43.8) | 55 (47.4) | 23 (37.1) | 0.186 |
| MVI, n (%) | 90 (50.6) | 60 (51.7) | 30 (48.4) | 0.671 |
| Tumor size ≥ 6 cm, n (%) | 57 (41.9) | 42 (46.7) | 15 (32.6) | 0.116 |
| AFP, ng/mL | 7701 ± 2022 | 8714 ± 2172 | 5774 ± 2077 | 0.333 |
| AFP ≥ 200 ng/mL, n (%) | 86 (48.8) | 62 (53.4) | 24 (39.3) | 0.074 |
| AST, IU/L | 69.6 ± 58.7 | 72.3 ± 63.3 | 64.3 ± 48.7 | 0.354 |
| ALT, IU/L | 54.5 ± 53.7 | 56.8 ± 59.9 | 50.0 ± 39.2 | 0.367 |
| Total Bilirubin, mg/dL | 1.0 ± 0.5 | 1.1 ± 0.5 | 1.0 ± 0.5 | 0.122 |
| Albumin, g/dL | 3.9 ± 0.5 | 3.9 ± 0.6 | 3.9 ± 0.5 | 0.9 |
| Platelet, ×103 /uL | 161 ± 101 | 174 ± 106 | 136 ± 87 | 0.058 |
| PT INR | 1.06 ± 0.1 | 1.06 ± 0.1 | 1.06 ± 0.1 | 0.594 |
| Concurrent treatment, n (%) | 49 (27.5) | 30 (25.9) | 19 (30.6) | 0.496 |
| Post treatment, n (%) | 104 (59.8) | 58 (51.3) | 46 (75.4) | 0.02 |
| Second line systemic treatment, n (%) | 87 (48.9) | 49 (42.2) | 38 (61.3) | 0.015 |
| Regorafenib, n | 48 | 23 | 25 | |
| Nivolumab, n | 21 | 13 | 8 | |
| Lenvatinib, n | 13 | 8 | 5 | |
| Chemotherapy, n | 2 | 2 | 0 | |
| Others, n | 3 | 3 | 0 | |
| Antiviral treatment, n (%) | 134 (75.3) | 97 (83.6) | 37 (59.1) | <0.001 |
| Viremia at sorafenib-start, log IU/mL | 4.5 ± 1.7 | 5.6 ± 0.9 | <0.001 | |
| Well-controlled viremia, n (%) | 99 (55.6) | 65 (56) | 34 (54.8) | 0.878 |
| Sorafenib stop, n (%) | 174 (97.8) | 113 (97.4) | 61 (98.4) | 0.676 |
| Sorafenib-use, months | 5.4 ± 5.3 | 5.0 ± 5.3 | 6.2 ± 5.2 | 0.68 |
| Variables | HBV-HCC (n = 116) | HCV-HCC (n = 62) |
|---|---|---|
| Treatment response evaluation, n (%) | 98 (84.5) | 59 (95.2) |
| Complete response | 2 (2.0) | 3 (5.1) |
| Partial response | 7 (7.1) | 5 (8.5) |
| Stable disease | 39 (39.8) | 21 (35.6) |
| Progression disease | 50 (51.1) | 30 (50.8) |
| Objective response rate, % | 9.1 | 13.6 |
| Disease control rate, % | 48.9 | 46.4 |
| Durability of response, month | 8.3 (1.0–24) | 7.9 (1.0–20.1) |
| Death, n (%) | 73 (62.9) | 40 (64.5) |
| HBV-HCC (n = 83) * | HCV-HCC (n = 53) * | |||
|---|---|---|---|---|
| Any, n (%) | Grade ≥ 3, n (%) | Any, n (%) | Grade ≥ 3, n (%) | |
| Total patients with TRAE n (%) | 53 (63.8) | 10 (12) | 41 (77.4) | 6 (11.4) |
| Hand foot skin reaction, n (%) | 27 (32.4) | 4 (4.8) | 20 (36.8) | 2 (3.8) |
| Diarrhea, n (%) | 21 (25.2) | 1 (1.2) | 12 (22.6) | 1 (1.9) |
| Decreased appetite, n (%) | 8 (9.6) | 0 | 1 (1.9) | 0 |
| Fatigue, n (%) | 3 (3.6) | 2 (2.4) | 5 (9.4) | 0 |
| Increased AST, n (%) | 3 (3.6) | 2 (2.4) | 0 | 0 |
| Dermatitis, n (%) | 3 (3.6) | 0 | 3 (5.7) | 0 |
| Pruritus, n (%) | 2 (2.4) | 0 | 0 | 0 |
| Increased T-bil, n (%) | 2 (2.4) | 1 (1.2) | 3 (5.7) | 3 (5.7) |
| Hypertension, n (%) | 1 (1.2) | 0 | 3 (5.7) | 0 |
| Hypothyroidism, n (%) | 1 (1.2) | 0 | 0 | 0 |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Comparison | H.R. | 95% CI | p-value | H.R. | 95% CI | p-value |
| Age, years | Increase per year | 0.99 | 0.98–1.01 | 0.439 | 1.01 | 0.99–1.03 | 0.592 |
| Sex | Female vs. Male | 1.10 | 0.72–1.69 | 0.65 | 0.97 | 0.61–1.55 | 0.911 |
| ALBI-grade | II vs. I | 2.05 | 1.40–2.99 | <0.001 | 1.80 | 1.19–2.73 | 0.006 |
| BCLC stage | C vs. B | 1.73 | 1.02–2.94 | 0.043 | 1.89 | 0.82–4.32 | 0.135 |
| EHM | Yes vs. No | 1.13 | 0.78–1.64 | 0.52 | 1.06 | 0.58–1.91 | 0.856 |
| MVI | Yes vs. No | 1.49 | 1.03–2.16 | 0.035 | 0.95 | 0.51–1.79 | 0.872 |
| AFP ≥ 200 ng/ml | Yes vs. No | 2.09 | 1.43–3.04 | <0.001 | 1.66 | 1.08–2.54 | 0.02 |
| Concurrent treatment | Yes vs. No | 1.04 | 0.70–1.55 | 0.858 | 0.89 | 0.58–1.34 | 0.568 |
| Post treatment | Yes vs. No | 0.27 | 0.18–0.40 | <0.001 | 0.34 | 0.22–0.53 | <0.001 |
| HCC Etiology | HCV vs. HBV | 0.82 | 0.56–1.21 | 0.311 | 0.92 | 0.59 | 1.43 |
| Well-controlled viremia | Yes vs. No | 0.55 | 0.38–0.80 | 0.002 | 0.63 | 0.42–0.93 | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, Y.-H.; Huang, T.-H.; Wang, J.-H.; Chen, Y.-Y.; Tsai, M.-C.; Chen, Y.-H.; Lu, S.-N.; Hu, T.-H.; Chen, C.-H.; Hung, C.-H. Well-Controlled Viremia Predicts the Outcome of Hepatocellular Carcinoma in Chronic Viral Hepatitis Patients Treated with Sorafenib. Cancers 2022, 14, 3971. https://doi.org/10.3390/cancers14163971
Kuo Y-H, Huang T-H, Wang J-H, Chen Y-Y, Tsai M-C, Chen Y-H, Lu S-N, Hu T-H, Chen C-H, Hung C-H. Well-Controlled Viremia Predicts the Outcome of Hepatocellular Carcinoma in Chronic Viral Hepatitis Patients Treated with Sorafenib. Cancers. 2022; 14(16):3971. https://doi.org/10.3390/cancers14163971
Chicago/Turabian StyleKuo, Yuan-Hung, Tzu-Hsin Huang, Jing-Houng Wang, Yen-Yang Chen, Ming-Chao Tsai, Yen-Hao Chen, Sheng-Nan Lu, Tsung-Hui Hu, Chien-Hung Chen, and Chao-Hung Hung. 2022. "Well-Controlled Viremia Predicts the Outcome of Hepatocellular Carcinoma in Chronic Viral Hepatitis Patients Treated with Sorafenib" Cancers 14, no. 16: 3971. https://doi.org/10.3390/cancers14163971
APA StyleKuo, Y. -H., Huang, T. -H., Wang, J. -H., Chen, Y. -Y., Tsai, M. -C., Chen, Y. -H., Lu, S. -N., Hu, T. -H., Chen, C. -H., & Hung, C. -H. (2022). Well-Controlled Viremia Predicts the Outcome of Hepatocellular Carcinoma in Chronic Viral Hepatitis Patients Treated with Sorafenib. Cancers, 14(16), 3971. https://doi.org/10.3390/cancers14163971