
Stereotactic Radiosurgery for Benign Cavernous Sinus Meningiomas: A Multicentre Study and Review of the Literature

 , , , , ,
, , , , ,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Conceptualization
2.2. Multicentric Database
2.3. Data Retrieval
2.4. Cohort Description
2.5. Endpoints
2.6. Imaging Follow-Up
2.7. Neurological Assessment and Clinical Follow-Up
2.8. Survey of Patients
2.9. Statistics
3. Results
3.1. Local Tumour Control Assessment
3.2. Neurological Assessment
4. Discussion
4.1. Our Results
4.2. CSM and Microsurgical Management
4.3. Radiation Therapy for CSMs
4.4. Challenging Aspects Related to SRS
4.5. Further Aspects of CSM Management
4.6. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pollock, B.E.; Stafford, S.L.; Link, M.J.; Garces, Y.I.; Foote, R.L. Single-fraction radiosurgery of benign cavernous sinus meningiomas. Comparative Study. J. Neurosurg. 2013, 119, 675–682. [Google Scholar] [CrossRef]
- Pollock, B.E.; Stafford, S.L. Results of stereotactic radiosurgery for patients with imaging defined cavernous sinus meningiomas. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 1427–1431. [Google Scholar] [CrossRef]
- Selch, M.T.; Ahn, E.; Laskari, A.; Lee, S.P.; Agazaryan, N.; Solberg, T.D.; Cabatan-Awang, C.; Frighetto, L.; Desalles, A.A. Stereotactic radiotherapy for treatment of cavernous sinus meningiomas. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 101–111. [Google Scholar] [CrossRef]
- Lee, J.Y.; Niranjan, A.; McInerney, J.; Kondziolka, D.; Flickinger, J.C.; Lunsford, L.D. Stereotactic radiosurgery providing long-term tumor control of cavernous sinus meningiomas. J. Neurosurg. 2002, 97, 65–72. [Google Scholar] [CrossRef]
- Al-Mefty, O. Management of the cavernous sinus and carotid siphon. Otolaryngol. Clin. N. Am. 1991, 24, 1523–1533. [Google Scholar] [CrossRef]
- Al-Mefty, O.; Ayoubi, S.; Smith, R.R. Direct surgery of the cavernous sinus: Patient selection. Acta Neurochir. Suppl. 1991, 53, 117–121. [Google Scholar]
- Al-Mefty, O.; Holoubi, A.; Rifai, A.; Fox, J.L. Microsurgical removal of suprasellar meningiomas. Neurosurgery 1985, 16, 364–372. [Google Scholar] [CrossRef]
- De Jesus, O.; Sekhar, L.N.; Parikh, H.K.; Wright, D.C.; Wagner, D.P. Long-term follow-up of patients with meningiomas involving the cavernous sinus: Recurrence, progression, and quality of life. Neurosurgery 1996, 39, 915–919; discussion 919–920. [Google Scholar] [CrossRef]
- Cusimano, M.D.; Sekhar, L.N.; Sen, C.N.; Pomonis, S.; Wright, D.C.; Biglan, A.W.; Jannetta, P.J. The results of surgery for benign tumors of the cavernous sinus. Comparative Study. Neurosurgery 1995, 37, 1–9; discussion 9–10. [Google Scholar] [CrossRef]
- O’Sullivan, M.G.; van Loveren, H.R.; Tew, J.M., Jr. The surgical resectability of meningiomas of the cavernous sinus. Neurosurgery 1997, 40, 238–244; discussion 245–247. [Google Scholar] [CrossRef]
- Jacob, M.; Wydh, E.; Vighetto, A.; Sindou, M. Visual outcome after surgery for cavernous sinus meningioma. Acta Neurochir. 2008, 150, 421–429; discussion 429. [Google Scholar] [CrossRef]
- Sindou, M.; Wydh, E.; Jouanneau, E.; Nebbal, M.; Lieutaud, T. Long-term follow-up of meningiomas of the cavernous sinus after surgical treatment alone. J. Neurosurg. 2007, 107, 937–944. [Google Scholar] [CrossRef]
- Sindou, M.; Chavez, J.M.; Pierre, G.S.; Jouvet, A. Percutaneous biopsy of cavernous sinus tumors through the foramen ovale. Neurosurgery 1997, 40, 106–110. [Google Scholar]
- Patel, C.R.; Fernandez-Miranda, J.C.; Wang, W.H.; Wang, E.W. Skull Base Anatomy. Otolaryngol. Clin. N. Am. 2016, 49, 9–20. [Google Scholar] [CrossRef]
- Raheja, A.; Couldwell, W.T. Cavernous sinus meningioma. Handb. Clin. Neurol. 2020, 170, 69–85. [Google Scholar] [CrossRef]
- Miyazaki, Y.; Yamamoto, I.; Shinozuka, S.; Sato, O. Microsurgical anatomy of the cavernous sinus. Neurol. Med. Chir. 1994, 34, 150–163. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, J.; Anand, M.K.; Camacho, A.; Rodriguez, F.; Watson, C.; Caskey, E.L.; Dumont, A.S.; Tubbs, R.S. Surgical anatomy of the internal carotid plexus branches to the abducens nerve in the cavernous sinus. Clin. Neurol. Neurosurg. 2020, 191, 105690. [Google Scholar] [CrossRef]
- Kano, H.; Park, K.-J.; Kondziolka, D.; Iyer, A.; Liu, X.; Tonetti, D.; Flickinger, J.C.; Lunsford, L.D. Does prior microsurgery improve or worsen the outcomes of stereotactic radiosurgery for cavernous sinus meningiomas? Research Support, Non-U.S. Gov’t. Neurosurgery 2013, 73, 401–410. [Google Scholar] [CrossRef]
- Franzin, A.; Vimercati, A.; Medone, M.; Serra, C.; Marzoli, S.B.; Forti, M.; Gioia, L.; Valle, M.; Picozzi, P. Neuroophthalmological evaluation after Gamma Knife surgery for cavernous sinus meningiomas. Neurosurg. Focus 2007, 23, E10. [Google Scholar] [CrossRef]
- Dufour, H.; Muracciole, X.; Metellus, P.; Regis, J.; Chinot, O.; Grisoli, F. Long-term tumor control and functional outcome in patients with cavernous sinus meningiomas treated by radiotherapy with or without previous surgery: Is there an alternative to aggressive tumor removal? Neurosurgery 2001, 48, 285–294; discussion 294–296. [Google Scholar]
- Goldbrunner, R.; Minniti, G.; Preusser, M.; Jenkinson, M.D.; Sallabanda, K.; Houdart, E.; von Deimling, A.; Stavrinou, P.; Lefranc, F.; Lund-Johansen, M.; et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016, 17, e383–e391. [Google Scholar] [CrossRef]
- Kuo, J.S.; Yu, C.; Giannotta, S.L.; Petrovich, Z.; Apuzzo, M.L. The Leksell gamma knife Model U versus Model C: A quantitative comparison of radiosurgical treatment parameters. Neurosurgery 2004, 55, 168–172; discussion 172–173. [Google Scholar] [CrossRef]
- Larsson, B.; Leksell, L.; Rexed, B.; Sourander, P.; Mair, W.; Andersson, B. The high-energy proton beam as a neurosurgical tool. Nature 1958, 182, 1222–1223. [Google Scholar] [CrossRef]
- Santacroce, A.; Walier, M.; Régis, J.; Liščák, R.; Motti, E.; Lindquist, C.; Kemeny, A.; Kitz, K.; Lippitz, B.; Álvarez, R.M.; et al. Long-term tumor control of benign intracranial meningiomas after radiosurgery in a series of 4565 patients. Research Support, Non-U.S. Gov’t. Neurosurgery 2012, 70, 32–39; discussion 39. [Google Scholar] [CrossRef]
- Kondziolka, D.; Mathieu, D.; Lunsford, L.D.; Martin, J.J.; Madhok, R.; Niranjan, A.; Flickinger, J.C. Radiosurgery as definitive management of intracranial meningiomas. Clin. Trial Neurosurg. 2008, 62, 53–58; discussion 58–60. [Google Scholar] [CrossRef]
- Subach, B.R.; Lunsford, L.D.; Kondziolka, D.; Maitz, A.H.; Flickinger, J.C. Management of petroclival meningiomas by stereotactic radiosurgery. Neurosurgery 1998, 42, 437–443; discussion 443–445. [Google Scholar]
- Duma, C.M.; Lunsford, L.D.; Kondziolka, D.; Harsh GRt Flickinger, J.C. Stereotactic radiosurgery of cavernous sinus meningiomas as an addition or alternative to microsurgery. Neurosurgery 1993, 32, 699–704; discussion 704–705. [Google Scholar] [CrossRef]
- Skeie, B.S.; Enger, P.O.; Skeie, G.O.; Thorsen, F.; Pedersen, P.H. Gamma knife surgery of meningiomas involving the cavernous sinus: Long-term follow-up of 100 patients. Neurosurgery 2010, 66, 661–668; discussion 668–669. [Google Scholar] [CrossRef]
- Spiegelmann, R.; Nissim, O.; Menhel, J.; Alezra, D.; Pfeffer, M.R. Linear accelerator radiosurgery for meningiomas in and around the cavernous sinus. Neurosurgery 2002, 51, 1373–1379; discussion 1379–1380. [Google Scholar] [CrossRef]
- Spiegelmann, R.; Cohen, Z.R.; Nissim, O.; Alezra, D.; Pfeffer, R. Cavernous sinus meningiomas: A large LINAC radiosurgery series. J. Neurooncol. 2010, 98, 195–202. [Google Scholar] [CrossRef]
- Nicolato, A.; Foroni, R.; Alessandrini, F.; Bricolo, A.; Gerosa, M. Radiosurgical treatment of cavernous sinus meningiomas: Experience with 122 treated patients. Neurosurgery 2002, 51, 1153–1159; discussion 1159–1161. [Google Scholar] [CrossRef] [PubMed]
- Nicolato, A.; Foroni, R.; Alessandrini, F.; Maluta, S.; Bricolo, A.; Gerosa, M. The role of Gamma Knife radiosurgery in the management of cavernous sinus meningiomas. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 992–1000. [Google Scholar] [CrossRef]
- Metellus, P.; Regis, J.; Muracciole, X.; Fuentes, S.; Dufour, H.; Nanni, I.; Chinot, O.; Martin, P.-M.; Grisoli, F. Evaluation of fractionated radiotherapy and gamma knife radiosurgery in cavernous sinus meningiomas: Treatment strategy. Neurosurgery 2005, 57, 873–886; discussion 873–886. [Google Scholar] [CrossRef] [PubMed]
- Roche, P.H.; Régis, J.; Dufour, H.; Fournier, H.D.; Delsanti, C.; Pellet, W.; Grisoli, F.; Peragut, J.C. Gamma knife radiosurgery in the management of cavernous sinus meningiomas. J. Neurosurg. 2000, 93 (Suppl. 3), 68–73. [Google Scholar] [CrossRef]
- Corniola, M.; Roche, P.H.; Brunea, M.; Cavallo, L.M.; Daniel, R.T.; Messerer, M.; Froelich, S.; Gardner, P.A.; Gentili, F.; Kawase, T.; et al. Management of cavernous sinus meningiomas: Consensus statement on behalf of the EANS skull base section. Brain Spine 2022, 2, 100864. [Google Scholar] [CrossRef]
- Fariselli, L.; Biroli, A.; Signorelli, A.; Broggi, M.; Marchetti, M.; Biroli, F. The cavernous sinus meningiomas’ dilemma: Surgery or stereotactic radiosurgery? Rep. Pract. Oncol. Radiother. 2016, 21, 379–385. [Google Scholar] [CrossRef]
- Tanaka, S.; Pollock, B.E.; Stafford, S.L.; Link, M.J. Stereotactic radiosurgery for trigeminal pain secondary to benign skull base tumors. World Neurosurg. 2013, 80, 371–377. [Google Scholar] [CrossRef]
- Leroy, H.A.; Tuleasca, C.; Reyns, N.; Levivier, M. Radiosurgery and fractionated radiotherapy for cavernous sinus meningioma: A systematic review and meta-analysis. Acta Neurochir. 2018, 160, 2367–2378. [Google Scholar] [CrossRef]
- Kollova, A.; Liscak, R.; Novotny, J., Jr.; Vladyka, V.; Simonova, G.; Janouskova, L. Gamma Knife surgery for benign meningioma. J. Neurosurg. 2007, 107, 325–336. [Google Scholar] [CrossRef]
- Park, K.-J.; Kano, H.; Iyer, A.; Liu, X.; Tonetti, D.A.; Lehocky, C.; Faramand, A.; Niranjan, A.; Flickinger, J.C.; Kondziolka, D.; et al. Gamma Knife stereotactic radiosurgery for cavernous sinus meningioma: Long-term follow-up in 200 patients. J. Neurosurg. 2018, 130, 1799–1808. [Google Scholar] [CrossRef]
- Al-Mefty, O.; Topsakal, C.; Pravdenkova, S.; Sawyer, J.R.; Harrison, M.J. Radiation-induced meningiomas: Clinical, pathological, cytokinetic, and cytogenetic characteristics. J. Neurosurg. 2004, 100, 1002–1013. [Google Scholar] [CrossRef] [PubMed]
- Heth, J.A.; Al-Mefty, O. Cavernous sinus meningiomas. Review. Neurosurg. Focus 2003, 14, e3. [Google Scholar] [CrossRef] [PubMed]
- Couldwell, W.T.; Heros, R.; Dolenc, V. Skull base meningiomas. Introductory. Neurosurg. Focus 2011, 30, 1p prior to E1. [Google Scholar] [CrossRef]
- Shaffrey, M.E.; Dolenc, V.V.; Lanzino, G.; Wolcott, W.P.; Shaffrey, C.I. Invasion of the internal carotid artery by cavernous sinus meningiomas. Surg. Neurol. 1999, 52, 167–171. [Google Scholar] [CrossRef]
- Dolenc, V. Microsurgical removal of large sphenoidal bone meningiomas. Acta Neurochir. Suppl. 1979, 28, 391–396. [Google Scholar]
- Metellus, P.; Batra, S.; Karkar, S.; Kapoor, S.; Weiss, S.; Kleinberg, L.; Rigamonti, D. Fractionated conformal radiotherapy in the management of cavernous sinus meningiomas: Long-term functional outcome and tumor control at a single institution. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 836–843. [Google Scholar] [CrossRef]
- Litré, C.F.; Colin, P.; Noudel, R.; Peruzzi, P.; Bazin, A.; Sherpereel, B.; Bernard, M.H.; Rousseaux, P. Fractionated stereotactic radiotherapy treatment of cavernous sinus meningiomas: A study of 100 cases. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 1012–1017. [Google Scholar] [CrossRef]
- Milker-Zabel, S.; Zabel-du Bois, A.; Huber, P.; Schlegel, W.; Debus, J. Fractionated stereotactic radiation therapy in the management of benign cavernous sinus meningiomas: Long-term experience and review of the literature. Strahlenther. Onkol. 2006, 182, 635–640. [Google Scholar] [CrossRef]
- Brell, M.; Villa, S.; Teixidor, P.; Lucas, A.; Ferrán, E.; Marín, S.; Acebes, J.J. Fractionated stereotactic radiotherapy in the treatment of exclusive cavernous sinus meningioma: Functional outcome, local control, and tolerance. Surg. Neurol. 2006, 65, 28–33; discussion 33–34. [Google Scholar] [CrossRef]
- Sibtain, A.; Plowman, P.N. Stereotactic radiosurgery. VII. Radiosurgery versus conventionally-fractionated radiotherapy in the treatment of cavernous sinus meningiomas. Br. J. Neurosurg. 1999, 13, 158–166. [Google Scholar] [CrossRef]
- Sims, E.; Doughty, D.; Macaulay, E.; Royle, N.; Wraith, C.; Darlison, R.; Plowman, P. Stereotactically delivered cranial radiation therapy: A ten-year experience of linac-based radiosurgery in the UK. Clin. Oncol. (R Coll Radiol.) 1999, 11, 303–320. [Google Scholar] [CrossRef] [PubMed]
- Maguire, P.D.; Clough, R.; Friedman, A.H.; Halperin, E.C. Fractionated external-beam radiation therapy for meningiomas of the cavernous sinus. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 75–79. [Google Scholar] [CrossRef]
- DeMonte, F.; Smith, H.K.; al-Mefty, O. Outcome of aggressive removal of cavernous sinus meningiomas. J. Neurosurg. 1994, 81, 245–251. [Google Scholar] [CrossRef]
- Aziz, K.M.A.; Froelich, S.C.; Dagnew, E.; Jean, W.; Breneman, J.C.; Zuccarello, M.; van Loveren, H.R.; Tew, J.M. Large sphenoid wing meningiomas involving the cavernous sinus: Conservative surgical strategies for better functional outcomes. Neurosurgery 2004, 54, 1375–1383; discussion 1383–1384. [Google Scholar] [CrossRef]
- Lee, C.-C.; Trifiletti, D.M.; Sahgal, A.; DeSalles, A.; Fariselli, L.; Hayashi, M.; Levivier, M.; Ma, L.; Álvarez, R.M.; Paddick, I.; et al. Stereotactic Radiosurgery for Benign (World Health Organization Grade I) Cavernous Sinus Meningiomas-International Stereotactic Radiosurgery Society (ISRS) Practice Guideline: A Systematic Review. Neurosurgery 2018, 83, 1128–1142. [Google Scholar] [CrossRef]
- Kondziolka, D.; Flickinger, J.C.; Perez, B. Judicious resection and/or radiosurgery for parasagittal meningiomas: Outcomes from a multicenter review. Gamma Knife Meningioma Study Group. Neurosurgery 1998, 43, 405–413; discussion 413–414. [Google Scholar] [CrossRef]
- Marchetti, M.; Bianchi, S.; Pinzi, V.; Tramacere, I.; Fumagalli, M.L.; Milanesi, I.M.; Ferroli, P.; Franzini, A.; Saini, M.; DiMeco, F.; et al. Multisession Radiosurgery for Sellar and Parasellar Benign Meningiomas: Long-term Tumor Growth Control and Visual Outcome. Neurosurgery 2016, 78, 638–646. [Google Scholar] [CrossRef]
- Tuleasca, C.; Leroy, H.A.; Regis, J.; Levivier, M. Gamma Knife radiosurgery for cervical spine lesions: Expanding the indications in the new era of Icon. Acta Neurochir. 2016, 158, 2235–2236. [Google Scholar] [CrossRef]
- Kaul, D.; Badakhshi, H.; Gevaert, T.; Pasemann, D.; Budach, V.; Tuleasca, C.; Gruen, A.; Prasad, V.; Levivier, M.; Kufeld, M. Erratum to: Dosimetric comparison of different treatment modalities for stereotactic radiosurgery of meningioma. Acta Neurochir. 2015, 157, 565. [Google Scholar] [CrossRef]
- Leavitt, J.A.; Stafford, S.L.; Link, M.J.; Pollock, B.E. Long-term evaluation of radiation-induced optic neuropathy after single-fraction stereotactic radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 524–527. [Google Scholar] [CrossRef]
- Sheehan, J.P.; Starke, R.M.; Kano, H.; Kaufmann, A.M.; Mathieu, D.; Zeiler, F.A.; West, M.; Chao, S.T.; Varma, G.; Chiang, V.L.S.; et al. Gamma Knife radiosurgery for sellar and parasellar meningiomas: A multicenter study. J. Neurosurg. 2014, 120, 1268–1277. [Google Scholar] [CrossRef] [PubMed]
- Friedman, W.A.; Murad, G.J.; Bradshaw, P.; Amdur, R.J.; Mendenhall, W.M.; Foote, K.; Bova, F.J. Linear accelerator surgery for meningiomas. J. Neurosurg. 2005, 103, 206–209. [Google Scholar] [CrossRef] [PubMed]
- Hakim, R.; Alexander, E., 3rd; Loeffler, J.S.; Shrieve, D.C.; Wen, P.; Fallon, M.P.; Stieg, P.E.; Black, P.M. Results of linear accelerator-based radiosurgery for intracranial meningiomas. Neurosurgery 1998, 42, 446–453; discussion 453–454. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Kida, Y.; Mori, Y. Long-term results of stereotactic gamma radiosurgery of meningiomas. Surg. Neurol. 2001, 55, 325–331. [Google Scholar] [CrossRef]
- Kida, Y.; Kobayashi, T.; Tanaka, T.; Oyama, H.; Niwa, M.; Maesawa, S. Radiosurgery of cavernous sinus meningiomas with gamma-knife. No Shinkei Geka 1996, 24, 529–533. [Google Scholar]
- Kondziolka, D.; Levy, E.I.; Niranjan, A.; Flickinger, J.C.; Lunsford, L.D. Long-term outcomes after meningioma radiosurgery: Physician and patient perspectives. J. Neurosurg. 1999, 91, 44–50. [Google Scholar] [CrossRef]
- Kondziolka, D.; Nathoo, N.; Flickinger, J.C.; Niranjan, A.; Maitz, A.H.; Lunsford, L.D. Long-term results after radiosurgery for benign intracranial tumors. Neurosurgery 2003, 53, 815–821; discussion 821–822. [Google Scholar] [CrossRef]
- Kreil, W.; Luggin, J.; Fuchs, I.; Weigl, V.; Eustacchio, S.; Papaefthymiou, G. Long term experience of gamma knife radiosurgery for benign skull base meningiomas. J. Neurol. Neurosurg. Psychiatry 2005, 76, 1425–1430. [Google Scholar] [CrossRef]
- Tuleasca, C.; Levivier, M. A virtual musician quartet with vestibular schwannoma. Lancet Oncol. 2018, 19, 1025. [Google Scholar] [CrossRef]
- Daniel, R.T.; Tuleasca, C.; George, M.; Pralong, E.; Schiappacasse, L.; Zeverino, M.; Maire, R.; Levivier, M. Preserving normal facial nerve function and improving hearing outcome in large vestibular schwannomas with a combined approach: Planned subtotal resection followed by gamma knife radiosurgery. Acta Neurochir. 2017, 159, 1197–1211. [Google Scholar] [CrossRef]
- Starnoni, D.; Berthiller, J.; Idriceanu, T.-M.; Meyronet, D.; D’Hombres, A.; Ducray, F.; Guyotat, J. Returning to work after multimodal treatment in glioblastoma patients. Neurosurg. Focus 2018, 44, E17. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D. The recurrence of intracranial meningiomas after surgical treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef]
- Condra, K.S.; Buatti, J.M.; Mendenhall, W.M.; Friedman, W.A.; Marcus, R.B., Jr.; Rhoton, A.L. Benign meningiomas: Primary treatment selection affects survival. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 427–436. [Google Scholar] [CrossRef]
- Pollock, B.E.; Stafford, S.L.; Utter, A.; Giannini, C.; Schreiner, S.A. Stereotactic radiosurgery provides equivalent tumor control to Simpson Grade 1 resection for patients with small- to medium-size meningiomas. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 1000–1005. [Google Scholar] [CrossRef]
- Sankila, R.; Kallio, M.; Jaaskelainen, J.; Hakulinen, T. Long-term survival of 1986 patients with intracranial meningioma diagnosed from 1953 to 1984 in Finland. Comparison of the observed and expected survival rates in a population-based series. Cancer 1992, 70, 1568–1576. [Google Scholar] [CrossRef]
- Kallio, M.; Sankila, R.; Hakulinen, T.; Jaaskelainen, J. Factors affecting operative and excess long-term mortality in 935 patients with intracranial meningioma. Neurosurgery 1992, 31, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Vernooij, M.W.; Ikram, M.A.; Tanghe, H.L.; Vincent, A.J.; Hofman, A.; Krestin, G.P.; Niessen, W.J.; Breteler, M.M.; van der Lugt, A. Incidental findings on brain MRI in the general population. N. Engl. J. Med. 2007, 357, 1821–1828. [Google Scholar] [CrossRef]
- Olivero, W.C.; Lister, J.R.; Elwood, P.W. The natural history and growth rate of asymptomatic meningiomas: A review of 60 patients. J. Neurosurg. 1995, 83, 222–224. [Google Scholar] [CrossRef]
- Van Havenbergh, T.; Carvalho, G.; Tatagiba, M.; Plets, C.; Samii, M. Natural history of petroclival meningiomas. Neurosurgery 2003, 52, 55–62; discussion 62–64. [Google Scholar] [CrossRef]
- Yoneoka, Y.; Fujii, Y.; Tanaka, R. Growth of incidental meningiomas. Acta Neurochir. 2000, 142, 507–511. [Google Scholar] [CrossRef]
- Nakamura, M.; Roser, F.; Michel, J.; Jacobs, C.; Samii, M. The natural history of incidental meningiomas. Neurosurgery 2003, 53, 62–70; discussion 70–71. [Google Scholar] [CrossRef] [PubMed]
- Niiro, M.; Yatsushiro, K.; Nakamura, K.; Kawahara, Y.; Kuratsu, J. Natural history of elderly patients with asymptomatic meningiomas. J. Neurol. Neurosurg. Psychiatry 2000, 68, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.; Naylor, K.; Tam, M.; Habibi, A.; Novotny, J.; Liščák, R.; Martinez-Moreno, N.; Martinez-Alvarez, R.; Sisterson, N.; Golfinos, J.G.; et al. Risk of radiation-associated intracranial malignancy after stereotactic radiosurgery: A retrospective, multicentre, cohort study. Lancet Oncol. 2019, 20, 159–164. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Group | Value |
|---|---|
| Age at treatment (years) * | 55 (±12.0) |
| Female ** | 932 (76.3) |
| Male ** | 290 (24.7) |
| Patients with sporadic meningiomas ** | 1150 (94.1) |
| Patients with multiple meningiomas ***, ** | 62 (5.1) |
| Patients with NF 2 ***, ** | 10 (0.8) |
| Neurological Status ***** | |
| Headache ** | 173 (14.1) |
| Seizures ** | 23 (1.8) |
| Cranial nerve deficit ** | 973 (79.6) |
| Hemiparesis, hypoesthesia ** | 56 (4.6) |
| Imbalance, ataxia-vertigo ** | 69 (5.6) |
| Details of Stereotactic Radiosurgery | |
| Volume (cm3) *, **** | 6.3 (±7.0) |
| Imaging-defined benign meningiomas ** | 703 (55.2) |
| Histologically proven WHO Gr. 1 meningiomas ** | 569 (44.7) |
| Sporadic meningiomas ***, ** | 1164 (91.5) |
| Multiple meningiomas ***, ** | 95 (7.5) |
| NF2 meningiomas ***, ** | 12 (1.0) |
| Maximal dose (Gy) * | 28 (±7.0) |
| Marginal dose (Gy) * | 14.0 (±3.0) |
| Treatment marginal isodose (%) * | 50 (±5.0) |
| Isocentres *, **** | 11 (±9.0) |
| Dose to optic pathways * | 8.0 (±4.0) |
| Follow-up | |
| Imaging follow-up (months from treatment) * | 61 (±38) 67(±33) ***** |
| Clinical follow-up (months from treatment) * | 62 (±39) |
| Patients lost to follow-up ** | 134 (10.9%) |
| Tumours lost to follow-up ** | 156 (12.2%) |
| Tumours with follow-up > 5 years ** | 595 (46.7%) |
| Tumours with follow-up > 7.5 years ** | 261 (12.6%) |
| Tumours with follow-up > 10 years ** | 103 (8.4%) |
| Neurological Deficit | Number of Patients (%) | |
|---|---|---|
| Cranial nerve | Definitive SRS | Adjuvant SRS |
| I | 0 (0%) | 1 (0.1%) |
| II | 315 (81%) | 294 (51.6%) |
| III-IV-VI | 360 (51%) | 261 (45.8%) |
| V | 188 (26.7%) | 204(35.8%) |
| VII | 45 (6.4%) | 56 (9.8%) |
| VIII | 25 (3.5%) | 36 (6.3%) |
| IX-X-XI | 5 (0.7%) | 1 (0.1%) |
| XII | 1 (0.1%) | 1(0.1%) |
| Variable/Follow-Up Years | 5 years | 7.5 years | 10 years |
|---|---|---|---|
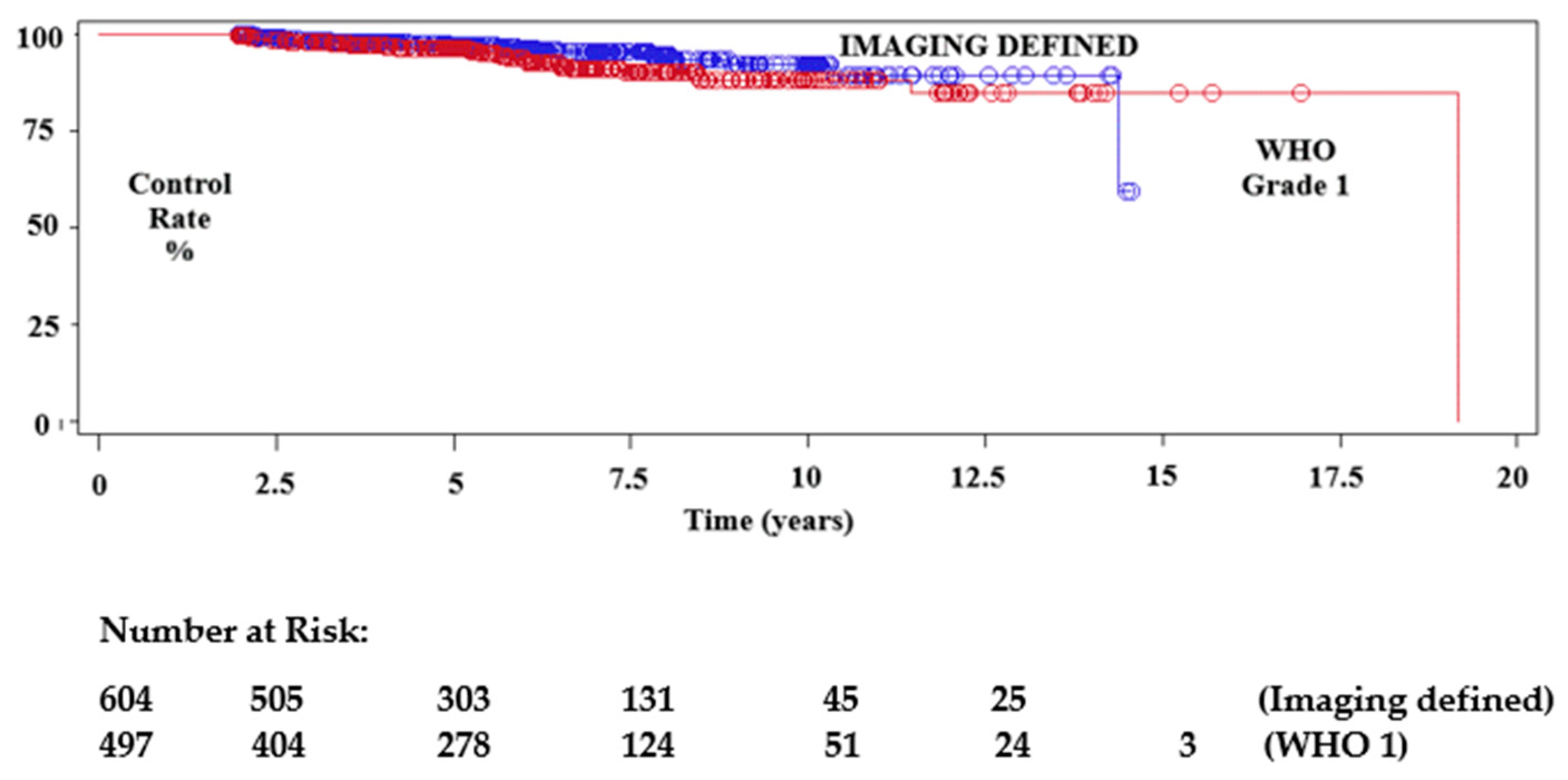
| Imaging Defined Meningiomas | 97.2% (95.6–98.4) | 95.3% (92.2–97.2) | 92.3% (86.8–95.5) |
| WHO Grade 1 Meningiomas | 96.2% (93.6–97.7) | 90.1% (85.3–93.3) | 87.9% (82.1–91.9) |
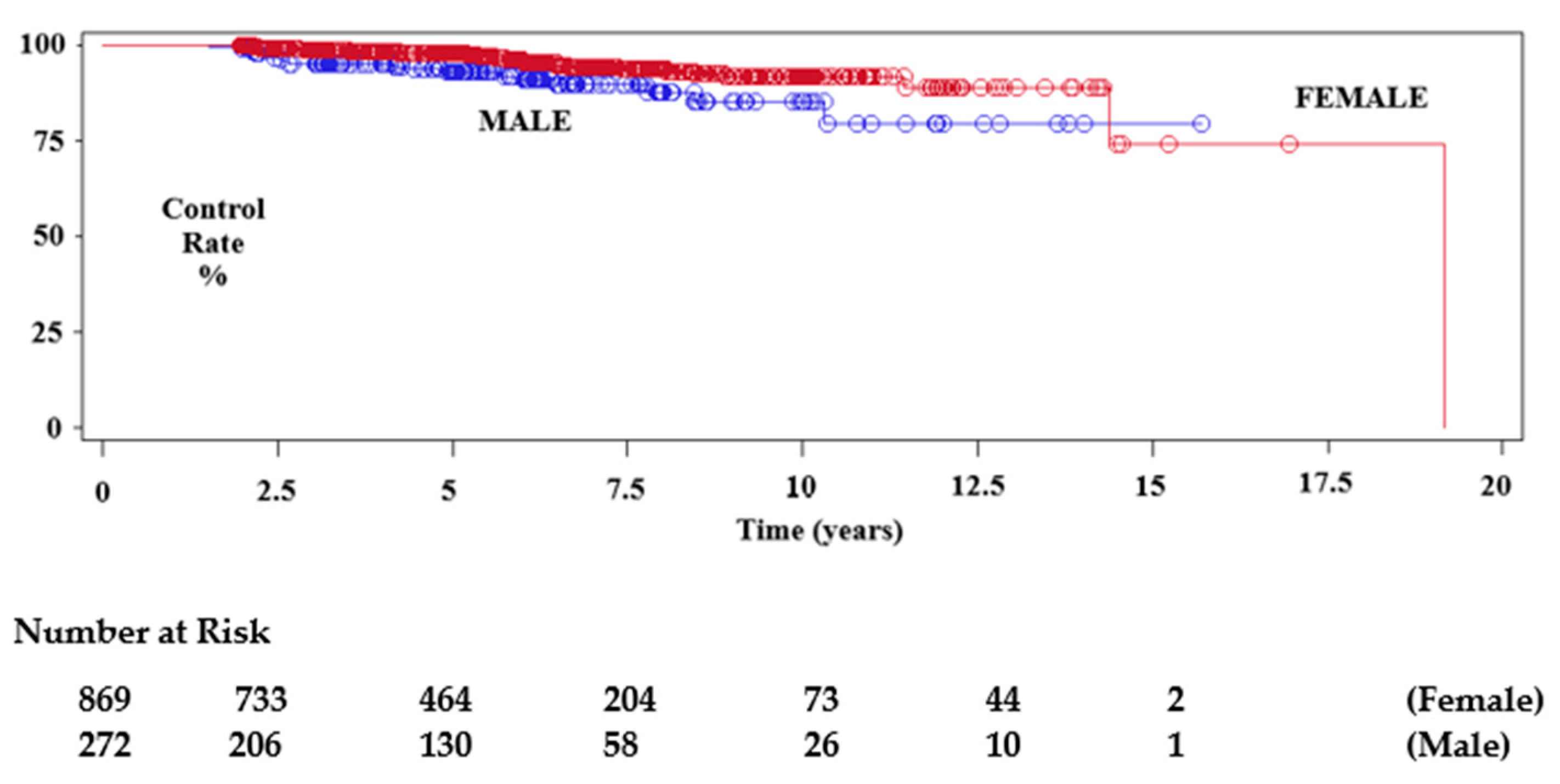
| Female | 97.7% (96.1–98.6) | 93.6% (90.6–95.7) | 91.6% (87.4–94.3) |
| Male | 92.9% (87.7–95.9) | 89.6% (82.8–93.7) | 85.1% (75.0–91.3) |
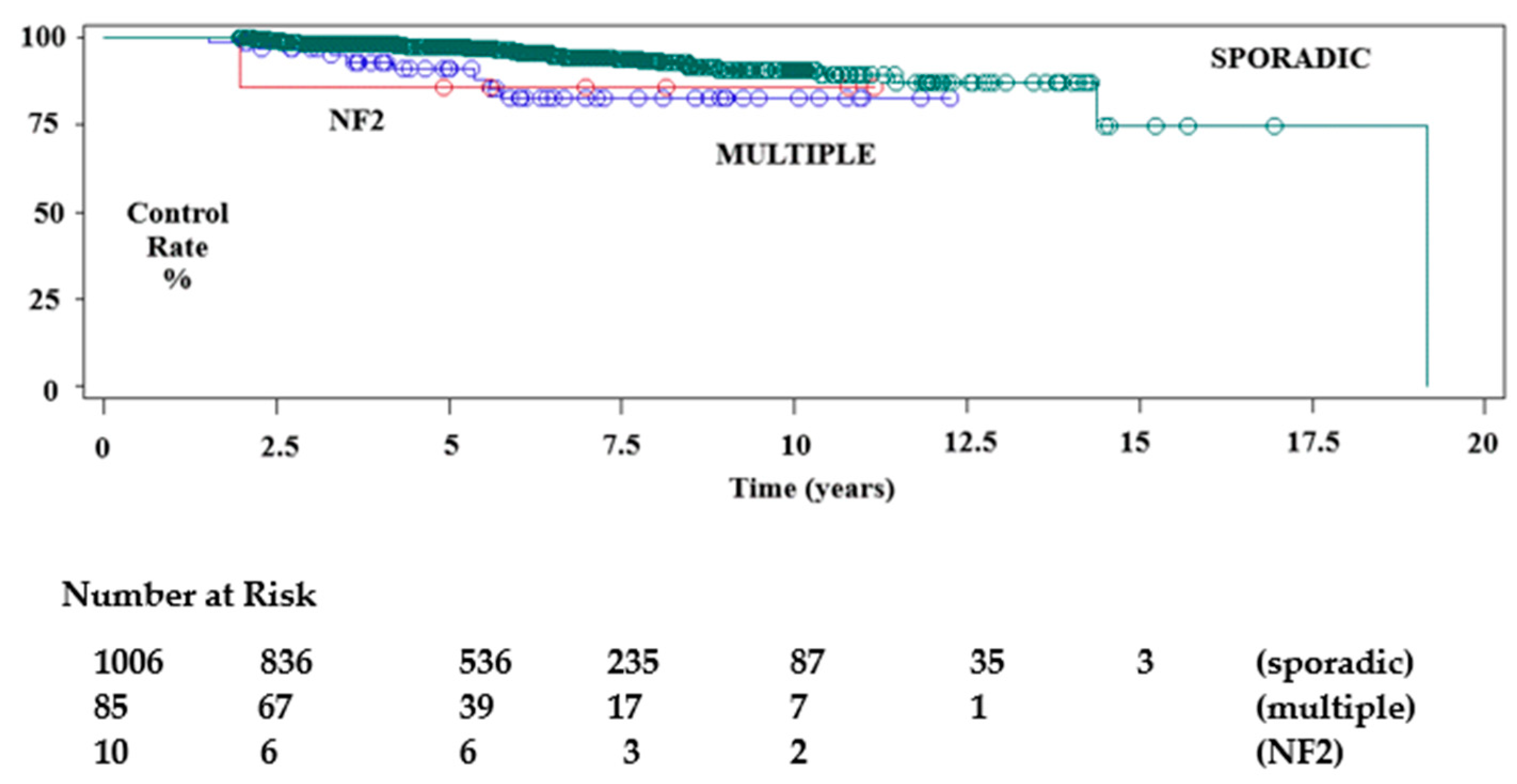
| Sporadic Meningiomas ** | 97.2% (95.7–98.2) | 93.7% (91.0–95.6) | 90.8% (86.8–93.6) |
| Multiple Meningiomas ** | 90.8% (79.3–96.1) | 85.3% (71.1–92.9) | 82.4% (67.2–91.0) |
| NF2 Meningiomas ** | 85.7% (33.4–97.8) |
| Univariate Chi-Squares for the Log-Rank Test | ||||
| Variable | Chi-Square | Prob. > Chi-Square | ||
| Previous surgery * | 2.4020 | 0.1212 | ||
| Gender | 7.0674 | 0.0079 | ||
| Multiple Meningiomas ** | 7.8110 | 0.0201 | ||
| Unifactorial Cox Proportional Hazard Model | ||||
| Variable | Pr. > Chi Square | Hazard Ratio | 95% Hazard Ratio Confidence Limits | |
| Centre | 0.0148 | |||
| Previous surgery * | 0.1242 | 0.643 | (0.366–1.129) | |
| Age | 0.6351 | 0.994 | (0.972–1.018) | |
| Gender | 0.0095 | 2.149 | (1.206–3.830) | |
| Volume | 0.6307 | 0.988 | (0.940–1.038) | |
| Prescription dose | 0.1929 | 1.056 | (0.973–1.145) | |
| Sporadic tumour vs. Meningiomatosis ** | 0.0097 | 2.725 | (1.275–5.824) | |
| Sporadic tumour vs. NF2 ** | 0.3776 | 2.446 | (0.335–17.851) | |
| Mutifactorial Cox Regression | ||||
|---|---|---|---|---|
| Variable | Pr. > Chi Square | Hazard Ratio | 95% Hazard Ratio Confidence Limits | |
| Centre | 0.0160 | |||
| Gender | 0.0031 | 2.467 | (1.356–4.486) | |
| Sporadic tumour vs. Meningiomatosis * | 0.0056 | 3.082 | (1.389–6.840) | |
| Sporadic tumour vs. NF2 tumour * | 0.6359 | 1.630 | (0.216–12.309) | |
| Sign-Symptom | Patients with No Symptoms | Patients with Symptoms | Patients with No Symptoms at Last Follow-Up | Patients with Symptoms at Last Follow-Up |
|---|---|---|---|---|
| Headache | 889 85.3% | 153 14.7% | 940 90.2% | 102 9.8% |
| Cranial nerves deficit | 196 18.8% | 909 81.2% | 340 32.3% | 702 67.7% |
| Hemiplegia Hemiparesis | 1003 96.3% | 39 3.7% | 1006 96.6% | 36 3.4% |
| Dizziness Imbalance Vertigo | 993 94.3% | 59 5.7% | 998 95.4% | 54 4.6% |
| Dysesthesia Hypoesthesia | 1030 98.8% | 12 1.2% | 1030 98.9% | 12 1.1% |
| Seizures *** | 1025 98.4% | 17 1.6% | 1028 98.7% | 14 1.3% |
| Clinical improvement: 460 cases (44.2%) Resolution of symptoms: 241 cases (23.2%) Improvement in cranial nerve neuropathy: 288 cases (27.6%) Resolution of symptoms related to cranial nerve neuropathy: 144 cases (13.5%) | ||||
| Sign-Symptom | Mild | Continuous Not Disabling | Continuous Disabling | Temporary | Permanent |
|---|---|---|---|---|---|
| Imbalance ataxia Vertigo dizziness | 1 | 1 | 0 | 1 | 1 |
| Vision troubles | 3 | 2 | 3 | 0 | 8 |
| 3rd, 4th or 6th nerve palsy | 2 | 13 | 9 | 5 | 19 |
| Trigeminal symptoms | 15 | 14 | 2 | 17 | 14 |
| Facial palsy | 2 | 2 | 0 | 3 | 1 |
| Hearing loss tinnitus | 2 | 2 | 0 | 3 | 1 |
| Symptomatic oedema | 2 | 4 | 0 | 5 | 1 |
| Seizures *** | 4 | 4 | --- | 6 | 2 |
| Headache | 11 | 10 | 1 | 10 | 12 |
| Hemiplegia Hemiparesis | 1 | 0 | 0 | 1 | 0 |
| Other | 0 | 2 | 3 | 4 | 1 |
| Pituitary deficit | 0 | 2 | 0 | 2 | 0 |
| Permanent mild morbidity rate: 1.13% (15 cases) Permanent continuous (not disabling) morbidity rate: 2.78% (31 cases) Permanent continuous (disabling) morbidity rate: 1.34% (14 cases) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santacroce, A.; Tuleasca, C.; Liščák, R.; Motti, E.; Lindquist, C.; Radatz, M.; Gatterbauer, B.; Lippitz, B.E.; Martínez Álvarez, R.; Martínez Moreno, N.; et al. Stereotactic Radiosurgery for Benign Cavernous Sinus Meningiomas: A Multicentre Study and Review of the Literature. Cancers 2022, 14, 4047. https://doi.org/10.3390/cancers14164047
Santacroce A, Tuleasca C, Liščák R, Motti E, Lindquist C, Radatz M, Gatterbauer B, Lippitz BE, Martínez Álvarez R, Martínez Moreno N, et al. Stereotactic Radiosurgery for Benign Cavernous Sinus Meningiomas: A Multicentre Study and Review of the Literature. Cancers. 2022; 14(16):4047. https://doi.org/10.3390/cancers14164047
Chicago/Turabian StyleSantacroce, Antonio, Constantin Tuleasca, Roman Liščák, Enrico Motti, Christer Lindquist, Matthias Radatz, Brigitte Gatterbauer, Bodo E. Lippitz, Roberto Martínez Álvarez, Nuria Martínez Moreno, and et al. 2022. "Stereotactic Radiosurgery for Benign Cavernous Sinus Meningiomas: A Multicentre Study and Review of the Literature" Cancers 14, no. 16: 4047. https://doi.org/10.3390/cancers14164047
APA StyleSantacroce, A., Tuleasca, C., Liščák, R., Motti, E., Lindquist, C., Radatz, M., Gatterbauer, B., Lippitz, B. E., Martínez Álvarez, R., Martínez Moreno, N., Kamp, M. A., Sandvei Skeie, B., Schipmann, S., Longhi, M., Unger, F., Sabin, I., Mindermann, T., Bundschuh, O., Horstmann, G. A., ... Ewelt, C. (2022). Stereotactic Radiosurgery for Benign Cavernous Sinus Meningiomas: A Multicentre Study and Review of the Literature. Cancers, 14(16), 4047. https://doi.org/10.3390/cancers14164047