
Efficacy and Optimal Pressure of Continuous Positive Airway Pressure in Intensity-Modulated Radiotherapy for Locally Advanced Lung Cancer
 , , , and
, , , and
Abstract
:Simple Summary
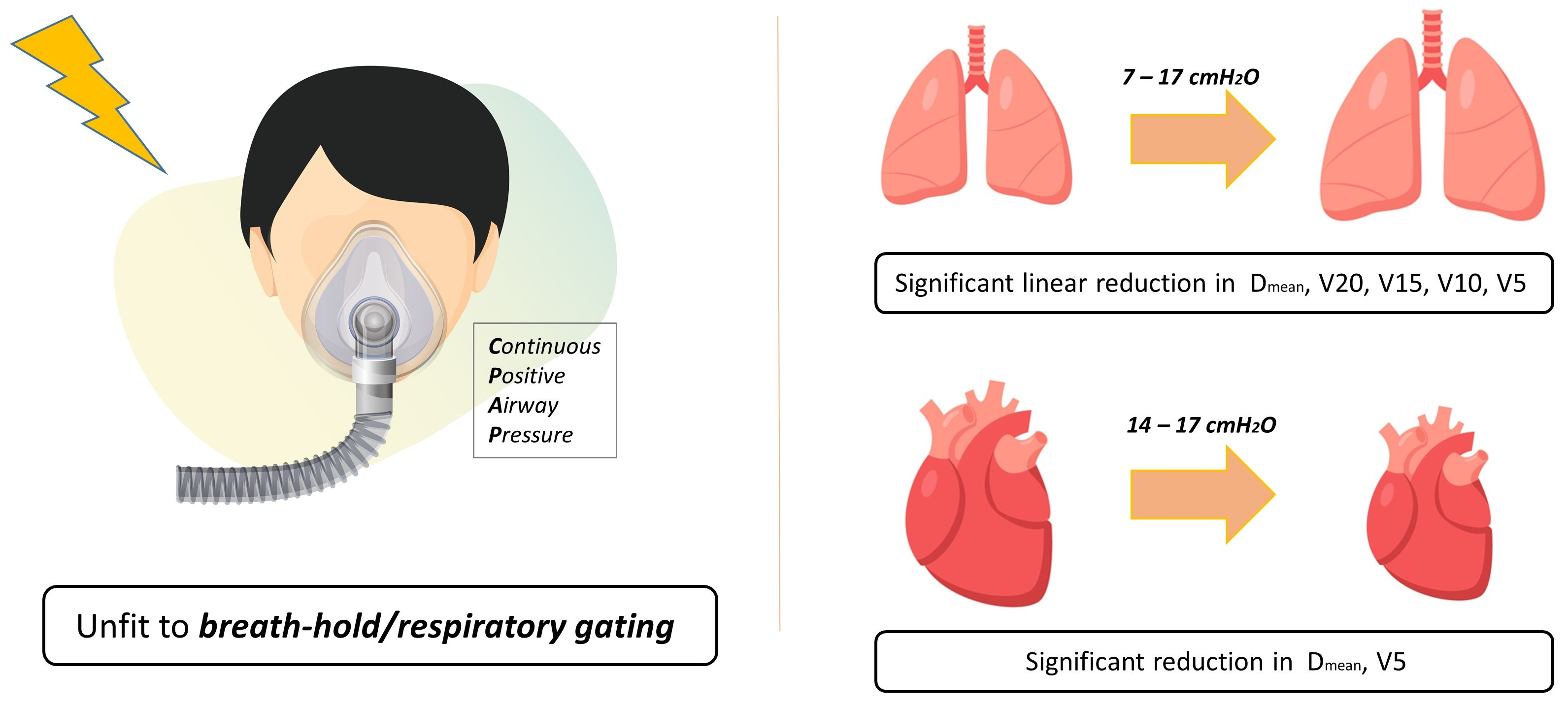
Abstract

1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Application of CPAP on CT-Simulation
2.3. Contouring and RT Planning
2.4. Statistics
3. Results
3.1. Change in Lung Volume and Dose Parameters
3.2. Change in Heart Volume and Dose Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, G.; Lock, M.; D’Souza, D.; Yu, E.; Van Dyk, J. Prediction of radiation pneumonitis by dose-volume histogram parameters in lung cancer—a systematic review. Radiother. Oncol. 2004, 71, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Senan, S.; Tsujino, K.; Barriger, R.B.; Rengan, R.; Moreno, M.; Bradley, J.D.; Kim, T.H.; Ramella, S.; Marks, L.B.; et al. Predicting radiation pneumonitis after chemoradiation therapy for lung cancer: An international individual patient data meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Shaverdian, N.; Lisberg, A.E.; Bornazyan, K.; Veruttipong, D.; Goldman, J.W.; Formenti, S.C.; Garon, E.B.; Lee, P. Previous radiotherapy and the clinical activity and toxicity of pembrolizumab in the treatment of non-small-cell lung cancer: A secondary analysis of the KEYNOTE-001 phase 1 trial. Lancet Oncol. 2017, 18, 895–903. [Google Scholar] [CrossRef]
- Theelen, W.; Peulen, H.M.U.; Lalezari, F.; van der Noort, V.; de Vries, J.F.; Aerts, J.; Dumoulin, D.W.; Bahce, I.; Niemeijer, A.N.; de Langen, A.J.; et al. Effect of Pembrolizumab After Stereotactic Body Radiotherapy vs. Pembrolizumab Alone on Tumor Response in Patients with Advanced Non-Small Cell Lung Cancer: Results of the PEMBRO-RT Phase 2 Randomized Clinical Trial. JAMA Oncol. 2019, 5, 1276–1282. [Google Scholar] [CrossRef]
- Marks, L.B.; Bentzen, S.M.; Deasy, J.O.; Kong, F.M.; Bradley, J.D.; Vogelius, I.S.; El Naqa, I.; Hubbs, J.L.; Lebesque, J.V.; Timmerman, R.D.; et al. Radiation dose-volume effects in the lung. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S70–S76. [Google Scholar] [CrossRef]
- Becker, H.F.; Jerrentrup, A.; Ploch, T.; Grote, L.; Penzel, T.; Sullivan, C.E.; Peter, J.H. Effect of nasal continuous positive airway pressure treatment on blood pressure in patients with obstructive sleep apnea. Circulation 2003, 107, 68–73. [Google Scholar] [CrossRef]
- Epstein, L.J.; Kristo, D.; Strollo, P.J., Jr.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar]
- O’Donoghue, F.J.; Catcheside, P.G.; Jordan, A.S.; Bersten, A.D.; McEvoy, R.D. Effect of CPAP on intrinsic PEEP, inspiratory effort, and lung volume in severe stable COPD. Thorax 2002, 57, 533–539. [Google Scholar] [CrossRef]
- Ferreyra, G.P.; Baussano, I.; Squadrone, V.; Richiardi, L.; Marchiaro, G.; Del Sorbo, L.; Mascia, L.; Merletti, F.; Ranieri, V.M. Continuous positive airway pressure for treatment of respiratory complications after abdominal surgery: A systematic review and meta-analysis. Ann. Surg. 2008, 247, 617–626. [Google Scholar] [CrossRef]
- Kil, W.J. Novel Use of Continuous Positive Airway Pressure Permits Heart- and Lung-Sparing Mediastinal Involved-Site Radiation Therapy for Patient with Hodgkin Lymphoma in Community Clinic When Deep Inspiration Breath-Hold Technique Is Not Available. Pract. Radiat. Oncol. 2019, 9, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Kil, W.J.; Pham, T.; Hossain, S.; Casaigne, J.; Jones, K.; Khalil, M. The impact of continuous positive airway pressure on radiation dose to heart and lung during left-sided postmastectomy radiotherapy when deep inspiration breath hold technique is not applicable: A case report. Radiat. Oncol. J. 2018, 36, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Kil, W.J.; Lee, I.J.; Pham, T.; Cho, I.H. Practical Heart Sparing Breast Cancer Radiation Therapy Using Continuous Positive Airway Pressure (CPAP) in Resource-Limited Radiation Oncology Clinics. Am. J. Clin. Oncol. 2019, 42, 797–801. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef]
- Wang, S.; Liao, Z.; Wei, X.; Liu, H.H.; Tucker, S.L.; Hu, C.S.; Mohan, R.; Cox, J.D.; Komaki, R. Analysis of clinical and dosimetric factors associated with treatment-related pneumonitis (TRP) in patients with non-small-cell lung cancer (NSCLC) treated with concurrent chemotherapy and three-dimensional conformal radiotherapy (3D-CRT). Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 1399–1407. [Google Scholar] [CrossRef]
- Lin, H.; Lu, H.; Shu, L.; Huang, H.; Chen, H.; Chen, J.; Cheng, J.; Pang, Q.; Peng, L.; Gu, J.; et al. Dosimetric study of a respiratory gating technique based on four-dimensional computed tomography in non-small-cell lung cancer. J. Radiat. Res. 2014, 55, 583–588. [Google Scholar] [CrossRef]
- Rouabhi, O.; Gross, B.; Bayouth, J.; Xia, J. The Dosimetric and Temporal Effects of Respiratory-Gated, High-Dose-Rate Radiation Therapy in Patients with Lung Cancer. Technol. Cancer Res. Treat. 2019, 18, 1533033818816072. [Google Scholar] [CrossRef]
- Pan, C.H.; Shiau, A.C.; Li, K.C.; Hsu, S.H.; Liang, J.A. The irregular breathing effect on target volume and coverage for lung stereotactic body radiotherapy. J. Appl. Clin. Med. Phys. 2019, 20, 109–120. [Google Scholar] [CrossRef]
- Berbeco, R.I.; Nishioka, S.; Shirato, H.; Jiang, S.B. Residual motion of lung tumors in end-of-inhale respiratory gated radiotherapy based on external surrogates. Med. Phys. 2006, 33, 4149–4156. [Google Scholar] [CrossRef]
- Chen, M.H.; Chuang, M.L.; Bornstein, B.A.; Gelman, R.; Harris, J.R.; Manning, W.J. Impact of respiratory maneuvers on cardiac volume within left-breast radiation portals. Circulation 1997, 96, 3269–3272. [Google Scholar] [CrossRef]
- Swanson, T.; Grills, I.S.; Ye, H.; Entwistle, A.; Teahan, M.; Letts, N.; Yan, D.; Duquette, J.; Vicini, F.A. Six-year experience routinely using moderate deep inspiration breath-hold for the reduction of cardiac dose in left-sided breast irradiation for patients with early-stage or locally advanced breast cancer. Am J. Clin. Oncol. 2013, 36, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Lu, H.M.; Cash, E.; Chen, M.H.; Chin, L.; Manning, W.J.; Harris, J.; Bornstein, B. Reduction of cardiac volume in left-breast treatment fields by respiratory maneuvers: A CT study. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 895–904. [Google Scholar] [CrossRef]
- Rosenzweig, K.E.; Hanley, J.; Mah, D.; Mageras, G.; Hunt, M.; Toner, S.; Burman, C.; Ling, C.C.; Mychalczak, B.; Fuks, Z.; et al. The deep inspiration breath-hold technique in the treatment of inoperable non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 81–87. [Google Scholar] [CrossRef]
- Hanley, J.; Debois, M.M.; Mah, D.; Mageras, G.S.; Raben, A.; Rosenzweig, K.; Mychalczak, B.; Schwartz, L.H.; Gloeggler, P.J.; Lutz, W.; et al. Deep inspiration breath-hold technique for lung tumors: The potential value of target immobilization and reduced lung density in dose escalation. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 603–611. [Google Scholar] [CrossRef]
- Josipovic, M.; Aznar, M.C.; Thomsen, J.B.; Scherman, J.; Damkjaer, S.M.; Nygård, L.; Specht, L.; Pøhl, M.; Persson, G.F. Deep inspiration breath hold in locally advanced lung cancer radiotherapy: Validation of intrafractional geometric uncertainties in the INHALE trial. Br. J. Radiol 2019, 92, 569. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.D.; Lawrence, Y.R.; Appel, S.; Landau, E.; Ben-David, M.A.; Rabin, T.; Benayun, M.; Dubinski, S.; Weizman, N.; Alezra, D.; et al. Continuous Positive Airway Pressure for Motion Management in Stereotactic Body Radiation Therapy to the Lung: A Controlled Pilot Study. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 391–399. [Google Scholar] [CrossRef]
- Upadhyay, R.; Venkatesulu, B.P.; Giridhar, P.; Kim, B.K.; Sharma, A.; Elghazawy, H.; Dhanireddy, B.; Elumalai, T.; Mallick, S.; Harkenrider, M. Risk and impact of radiation related lymphopenia in lung cancer: A systematic review and meta-analysis. Radiother. Oncol. 2021, 157, 225–233. [Google Scholar] [CrossRef]
- Weizman, N.; Baidun, K.; Goldstein, A.; Amit, U.; Saad, A.; Lawrence, Y.R.; Appel, S.; Orion, I.; Alezra, D.; Abrams, R.; et al. Initial estimates of continuous positive airway pressure (CPAP) on heart volume, position and motion in patients receiving chest radiation. Med. Dosim. 2022, 47, 191–196. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | No. of Patients |
|---|---|
| Age (yr) | |
| Median (range) | 67 (51–82) |
| Gender | |
| Male | 28 |
| Female | 1 |
| Histology | |
| Non-small cell lung cancer | 22 |
| Squamous cell carcinoma | 15 |
| Adenocarcinoma | 5 |
| NOS | 2 |
| Small cell lung cancer | 7 |
| Staging (AJCC 8th edition) | |
| IIB | 3 |
| IIIA | 17 |
| IIIB | 6 |
| IIIC | 3 |
| Tumor location | |
| Right upper lobe | 14 |
| Right middle lobe | 1 |
| Right lower lobe | 5 |
| Left upper lobe | 7 |
| Left lower lobe | 1 |
| Both upper lobe | 1 |
| Respiratory comorbidity | |
| Chronic obstructive pulmonary disease | 11 |
| Emphysema | 1 |
| Idiopathic pulmonary fibrosis | 1 |
| Structure | Baseline | 4 cmH2O | p | 7 cmH2O | p | 10 cmH2O | p | 14 cmH2O | p | 17 cmH2O | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| GTV | |||||||||||
| Volume (cm3) | 77.3 ± 48.4 | 77.4 ± 47.9 | 0.85 | 76.7 ± 49.2 | 0.74 | 73.8 ± 44.8 | 0.37 | 75.5 ± 44.3 | 0.94 | 69.1 ± 39.8 | 0.69 |
| CTV | |||||||||||
| Volume (cm3) | 161.7 ± 78.3 | 162.9 ± 77.9 | 0.57 | 157.6 ± 81.6 | 0.32 | 156.3 ± 70.6 | 0.15 | 158.7 ± 70.6 | 0.11 | 151.4 ± 66.5 | 0.95 |
| PTV | |||||||||||
| Volume (cm3) | 292.3 ± 129.0 | 286.9 ± 137.2 | 0.47 | 291.0 ± 127.1 | 0.72 | 284.1 ± 118.3 | 0.12 | 287.8 ± 118.3 | 0.03 * | 284.3 ± 114.7 | 0.79 |
| Lung | |||||||||||
| Volume (cm3) | 3318.0 ± 742.4 | 3575.4 ± 762.1 | <0.01 * | 3840.1 ± 764.5 | <0.01 * | 4148.9 ± 820.5 | <0.01 * | 44529.5 ± 905.9 | <0.01 * | 4883.2 ± 799.4 | <0.01 * |
| Dmean (cGy) | 1573.5 ± 314.0 | 1545.9 ± 327.7 | 0.08 | 1495.3 ± 330.8 | <0.01 * | 1455.9 ± 334.6 | <0.01 * | 1392.8 ± 304.4 | <0.01 * | 1443.4 ± 268.7 | <0.01 * |
| V5 (%) | 65.1 ± 13.7 | 64.0 ± 13.6 | 0.07 | 62.7 ± 13.1 | <0.01 * | 61.1 ± 13.5 | <0.01 * | 58.6 ± 13.2 | <0.01 * | 59.6 ± 12.3 | <0.01 * |
| V10 (%) | 50.7 ± 13.3 | 49.5 ± 13.4 | 0.03 * | 48.2 ± 13.2 | <0.01 * | 47.1 ± 13.1 | <0.01 * | 44.8 ± 12.7 | <0.01 * | 46.8 ± 11.2 | <0.01 * |
| V15 (%) | 38.5 ± 10.7 | 37.5 ± 10.4 | 0.10 | 36.0 ± 10.2 | <0.01 * | 35.4 ± 10.1 | <0.01 * | 33.8 ± 9.6 | <0.01 * | 34.9 ± 8.0 | <0.01 * |
| V20 (%) | 28.1 ± 7.4 | 27.7 ± 7.5 | 0.24 | 26.6 ± 7.6 | <0.01 * | 26.0 ± 7.4 | <0.01 * | 25.1 ± 6.9 | <0.01 * | 26.0 ± 5.6 | <0.01 * |
| Heart | |||||||||||
| Volume (cm3) | 725.6 ± 155.4 | 719.3 ± 162.0 | 0.63 | 702.6 ± 167.5 | 0.06 | 683.8 ± 134.5 | 0.05 | 679.0 ± 109.3 | <0.01 * | 622.8 ± 102.4 | <0.01 * |
| Dmean (cGy) | 1277.4 ± 601.1 | 1174.7 ± 566.5 | 0.27 | 1238.1 ± 612.1 | 0.14 | 1243.1 ± 607.7 | 0.13 | 1212.2 ± 653.4 | 0.02 * | 1139.6 ± 651.9 | 0.01 * |
| V5 (%) | 55.5 ± 25.8 | 54.0 ± 26.4 | 0.15 | 53.5 ± 27.2 | 0.08 | 53.8 ± 27.4 | 0.07 | 52.1 ± 27.8 | <0.01 * | 49.7 ± 25.8 | <0.01 * |
| V50 (%) | 3.6 ± 2.6 | 3.6 ± 2.5 | 0.88 | 3.3 ± 2.4 | 0.28 | 3.3 ± 2.3 | 0.42 | 3.1 ± 2.4 | 0.33 | 3.1 ± 2.4 | 0.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Yea, J.W.; Oh, S.A.; Park, J.; Park, J.W.; Lee, J.E. Efficacy and Optimal Pressure of Continuous Positive Airway Pressure in Intensity-Modulated Radiotherapy for Locally Advanced Lung Cancer. Cancers 2022, 14, 4308. https://doi.org/10.3390/cancers14174308
Park J, Yea JW, Oh SA, Park J, Park JW, Lee JE. Efficacy and Optimal Pressure of Continuous Positive Airway Pressure in Intensity-Modulated Radiotherapy for Locally Advanced Lung Cancer. Cancers. 2022; 14(17):4308. https://doi.org/10.3390/cancers14174308
Chicago/Turabian StylePark, Jaehyeon, Ji Woon Yea, Se An Oh, Jongmoo Park, Jae Won Park, and Jeong Eun Lee. 2022. "Efficacy and Optimal Pressure of Continuous Positive Airway Pressure in Intensity-Modulated Radiotherapy for Locally Advanced Lung Cancer" Cancers 14, no. 17: 4308. https://doi.org/10.3390/cancers14174308
APA StylePark, J., Yea, J. W., Oh, S. A., Park, J., Park, J. W., & Lee, J. E. (2022). Efficacy and Optimal Pressure of Continuous Positive Airway Pressure in Intensity-Modulated Radiotherapy for Locally Advanced Lung Cancer. Cancers, 14(17), 4308. https://doi.org/10.3390/cancers14174308