Addition of Chromosome 17 Polysomy and HER2 Amplification Status Improves the Accuracy of Clinicopathological Factor-Based Progression Risk Stratification and Tumor Grading of Non-Muscle-Invasive Bladder Cancer

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection and Data Collection
2.2. Immunohistochemistry (IHC) and Fluorescence In Situ Hybridization (FISH) Analysis
2.3. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
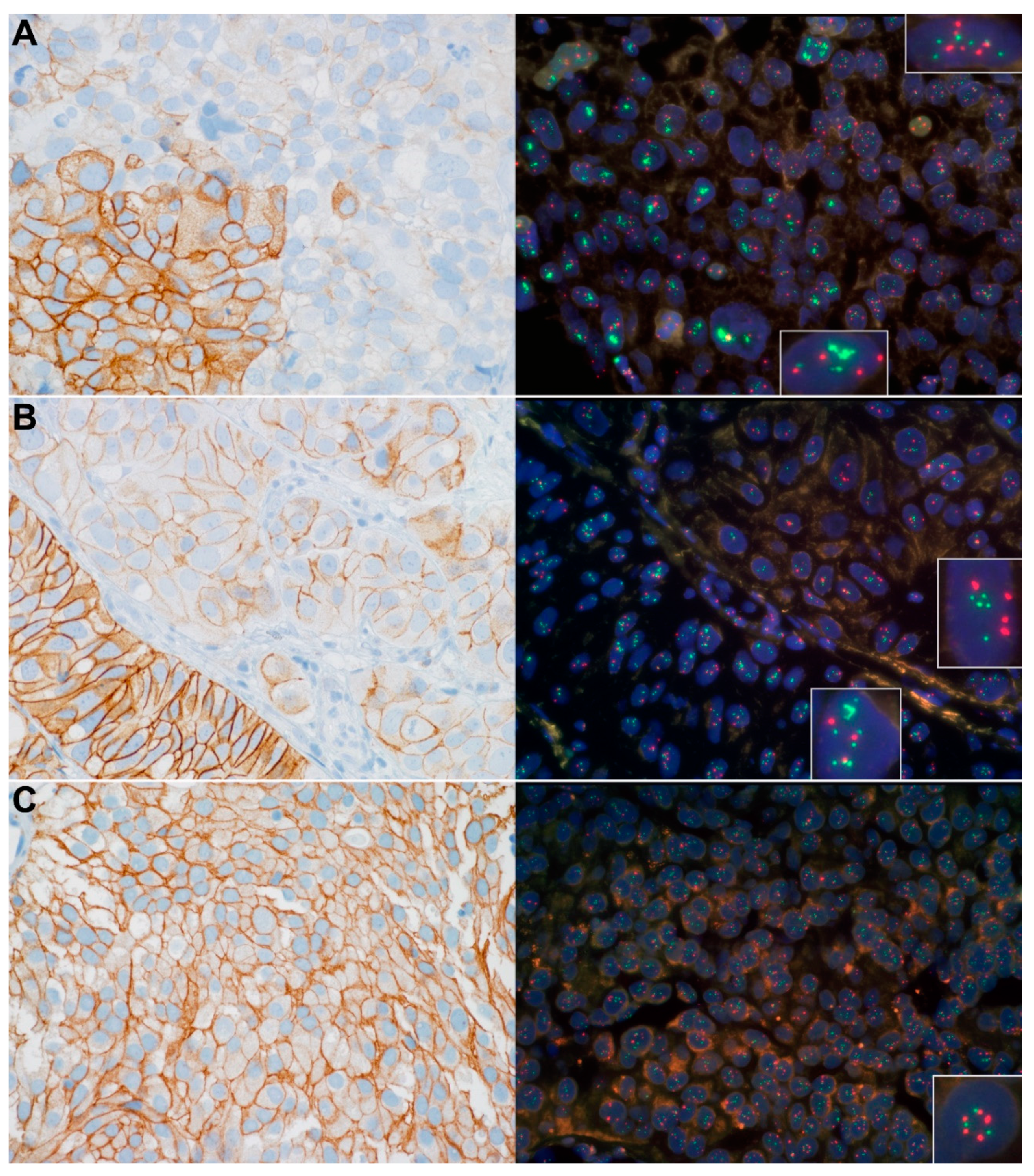
3.2. Chr17 Polysomy, HER2 Expression and Gene Amplification Status of the NMIBCs
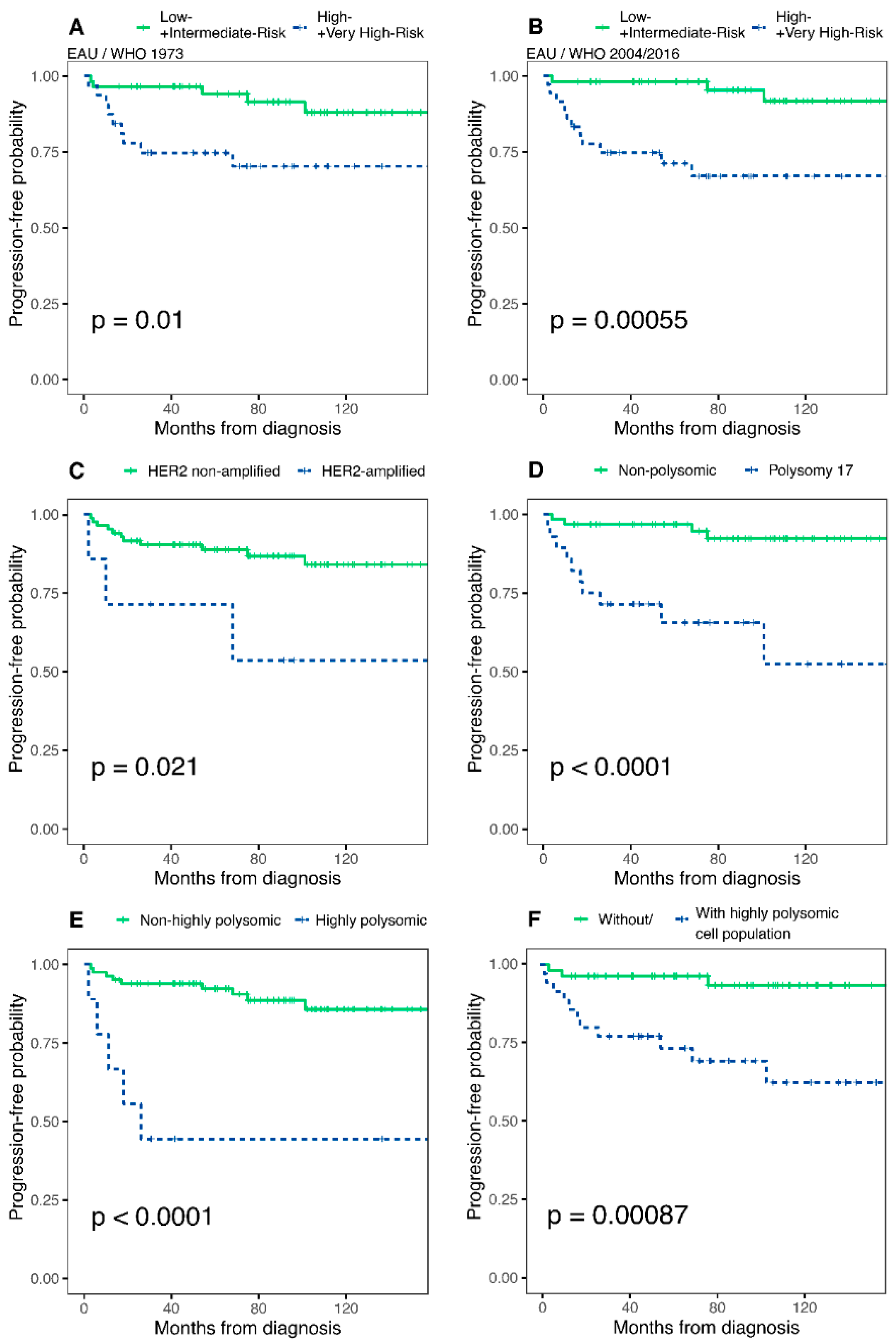
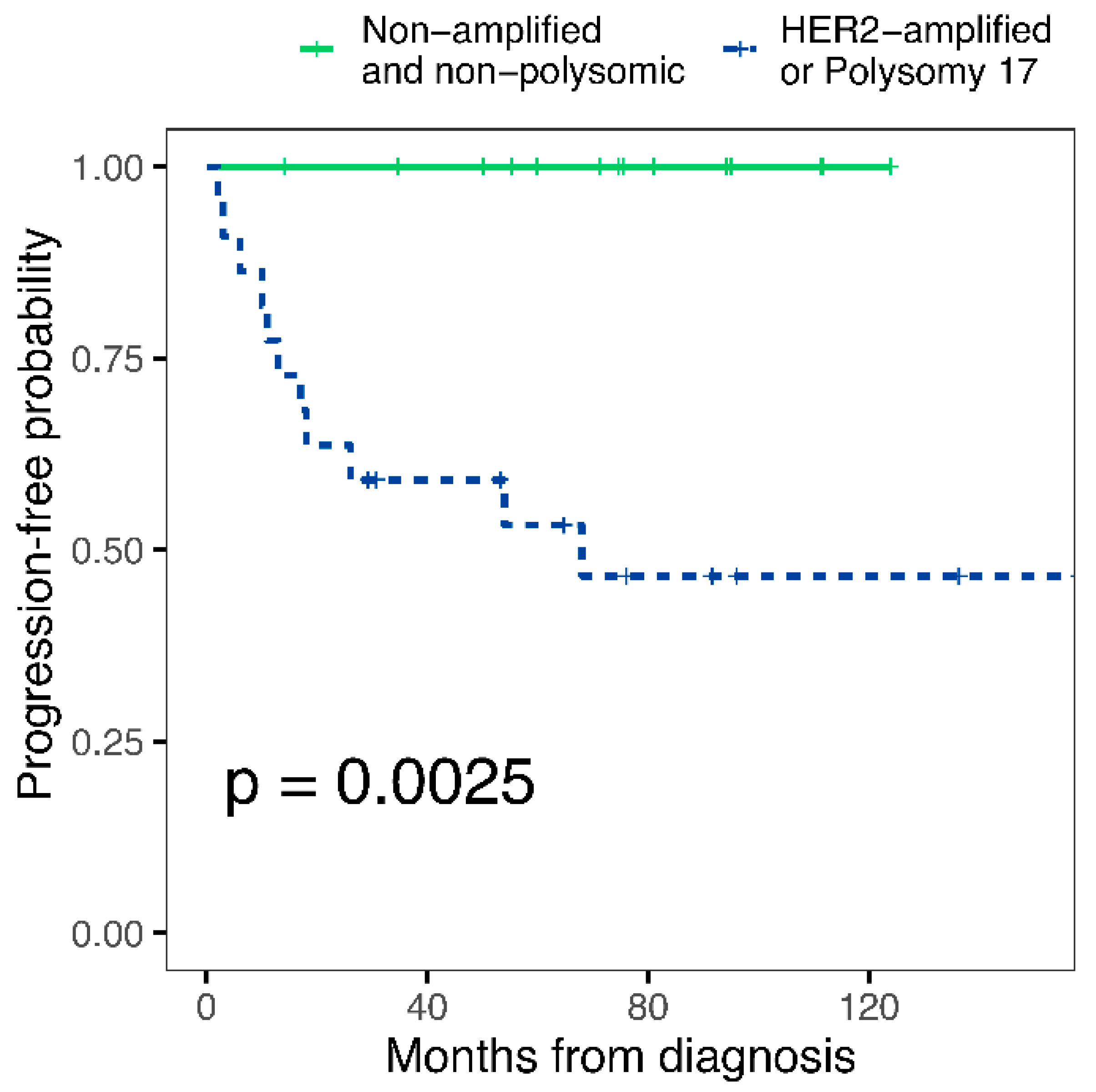
3.3. Potential Predictor Variables and Progression of NMIBCs
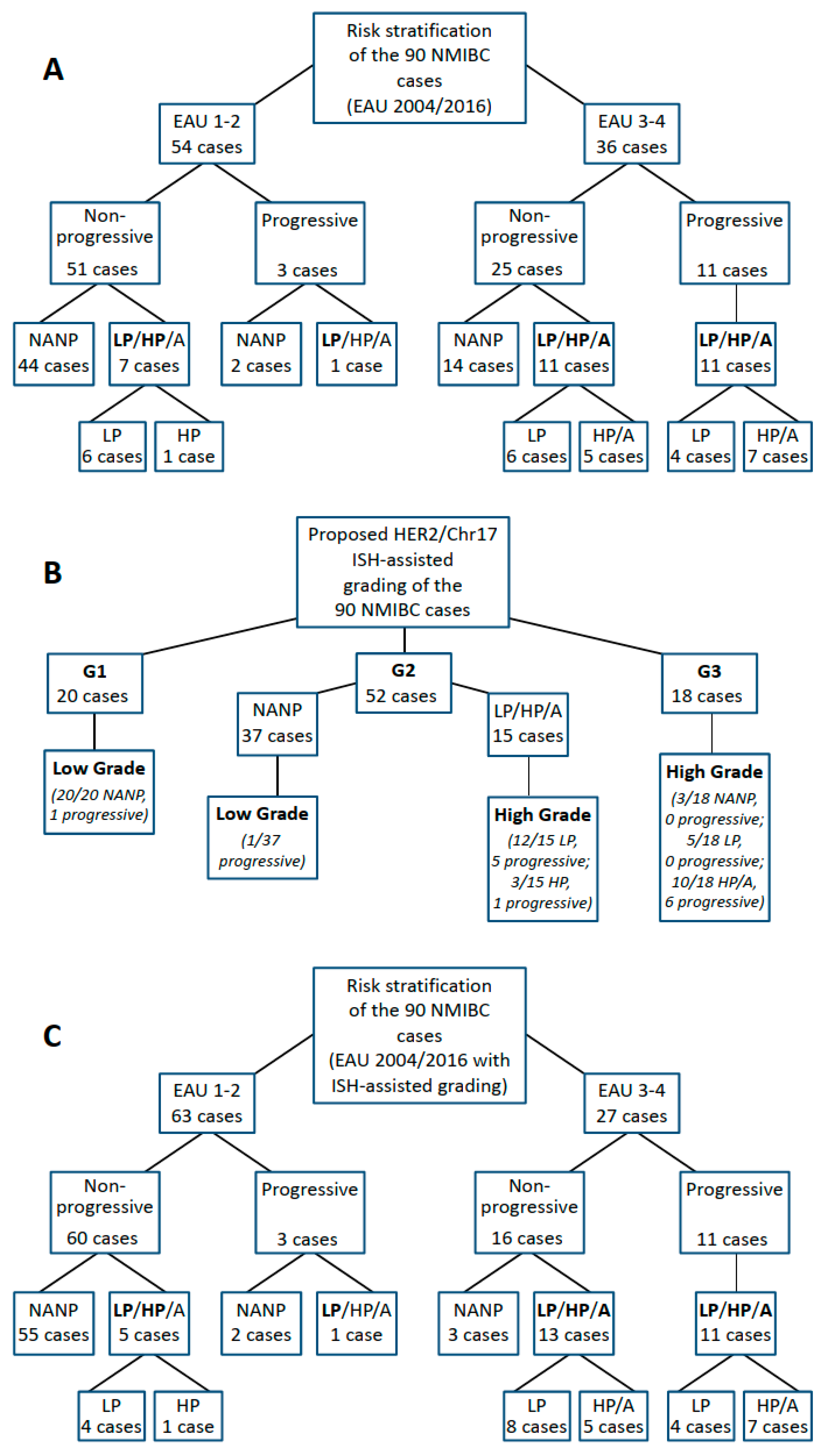
3.4. Addition of Chr17 Polysomy and HER2 Amplification Status Improves Accuracy of EAU and AUA Risk Stratifications
3.5. Reclassification of G2 Tumors by Molecular Grading Could Improve the Accuracy of the EAU 2004/2016 Risk Stratification System
3.6. Potential Applications of Chromosome 17/HER2 Copy Number Status in the Diagnostic Practice of Non-Muscle-Invasive Bladder Cancer to Improve the Prediction of Progression
3.7. Correlation of p53 Protein Expression with Chromosome 17/HER2 Copy Number Status and Progression of Non-Muscle-Invasive Bladder Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Roupret, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, R.J.; van der Meijden, A.P.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.; Kurth, K. Predicting Recurrence and Progression in Individual Patients with Stage Ta T1 Bladder Cancer Using EORTC Risk Tables: A Combined Analysis of 2596 Patients from Seven EORTC Trials. Eur. Urol. 2006, 49, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Soukup, V.; Čapoun, O.; Cohen, D.; Hernández, V.; Burger, M.; Compérat, E.; Gontero, P.; Lam, T.; Mostafid, A.H.; Palou, J.; et al. Risk Stratification Tools and Prognostic Models in Non–muscle-invasive Bladder Cancer: A Critical Assessment from the European Association of Urology Non-muscle-invasive Bladder Cancer Guidelines Panel. Eur. Urol. Focus 2020, 6, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Hendricksen, K.; Aziz, A.; Bes, P.; Chun, F.K.-H.; Dobruch, J.; Kluth, L.A.; Gontero, P.; Necchi, A.; Noon, A.P.; van Rhijn, B.W.; et al. Discrepancy Between European Association of Urology Guidelines and Daily Practice in the Management of Non–muscle-invasive Bladder Cancer: Results of a European Survey. Eur. Urol. Focus 2019, 5, 681–688. [Google Scholar] [CrossRef]
- Sylvester, R.J.; Rodríguez, O.; Hernández, V.; Turturica, D.; Bauerová, L.; Bruins, H.M.; Bründl, J.; van der Kwast, T.H.; Brisuda, A.; Rubio-Briones, J.; et al. European Association of Urology (EAU) Prognostic Factor Risk Groups for Non–muscle-invasive Bladder Cancer (NMIBC) Incorporating the WHO 2004/2016 and WHO 1973 Classification Systems for Grade: An Update from the EAU NMIBC Guidelines Panel. Eur. Urol. 2021, 79, 480–488. [Google Scholar] [CrossRef]
- Sokolova, I.A.; Halling, K.C.; Jenkins, R.B.; Burkhardt, H.M.; Meyer, R.G.; Seelig, S.A.; King, W. The Development of a Multitarget, Multicolor Fluorescence in Situ Hybridization Assay for the Detection of Urothelial Carcinoma in Urine. J. Mol. Diagn. 2000, 2, 116–123. [Google Scholar] [CrossRef]
- Sandberg, A.A.; Berger, C.S. Review of Chromosome Studies in Urological Tumors. II. Cytogenetics and Molecular Genetics of Bladder Cancer. J. Urol. 1994, 151, 545–560. [Google Scholar] [CrossRef]
- Ribal, M.J.; Alcaraz, A.; Mengual, L.; Carrió, A.; Lopez-Guillermo, A.; Mallofre, C.; Palou, J.; Gelabert, A.; Villavicencio, H. Chromosomal High-Polysomies Predict Tumour Progression in T1 Transitional Cell Carcinoma of the Bladder. Eur. Urol. 2004, 45, 593–599. [Google Scholar] [CrossRef]
- Kocsmár, I.; Pajor, G.; Gyöngyösi, B.; Székely, E.; Varga, M.; Kocsmár, É.; Kenessey, I.; Beöthe, T.; Süle, N.; Majoros, A.; et al. Development and Initial Testing of a Modified UroVysion-Based Fluorescence In Situ Hybridization Score for Prediction of Progression in Bladder Cancer. Am. J. Clin. Pathol. 2020, 153, 274–284. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; Dowsett, M.; Fitzgibbons, P.L.; Hanna, W.M.; Langer, A.; et al. American Society of Clinical Oncology/College of American Pathologists Guideline Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer. J. Clin. Oncol. 2007, 25, 118–145. [Google Scholar] [CrossRef] [PubMed]
- Ding, W.; Tong, S.; Gou, Y.; Sun, C.; Wang, H.; Chen, Z.; Tan, J.; Xu, K.; Xia, G.; Ding, Q. Human epidermal growth factor receptor 2: A significant indicator for predicting progression in non-muscle-invasive bladder cancer especially in high-risk groups. World J. Urol. 2015, 33, 1951–1957. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, A.E.; Rashed, H.E.; Elkady, E.; Elsebai, E.A.; El-Azony, A.; Matar, I. Fatty acid synthase, Her2/neu, and E2F1 as prognostic markers of progression in non-muscle invasive bladder cancer. Ann. Diagn. Pathol. 2019, 39, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Sanguedolce, F.; Cormio, A.; Massenio, P.; Pedicillo, M.C.; Cagiano, S.; Fortunato, F.; Calò, B.; Di Fino, G.; Carrieri, G.; Bufo, P.; et al. Altered expression of HER-2 and the mismatch repair genes MLH1 and MSH2 predicts the outcome of T1 high-grade bladder cancer. J. Cancer Res. Clin. Oncol. 2018, 144, 637–644. [Google Scholar] [CrossRef]
- Chen, P.C.-H.; Yu, H.-J.; Chang, Y.-H.; Pan, C.-C. Her2 amplification distinguishes a subset of non-muscle-invasive bladder cancers with a high risk of progression. J. Clin. Pathol. 2013, 66, 113–119. [Google Scholar] [CrossRef]
- Ohta, J.I.; Miyoshi, Y.; Uemura, H.; Fujinami, K.; Mikata, K.; Hosaka, M.; Tokita, Y.; Kubota, Y. Fluorescence in situ hybridization evaluation of c-erbB-2 gene amplification and chromosomal anomalies in bladder cancer. Clin Cancer Res. 2001, 7, 2463–2467. [Google Scholar]
- Merola, R.; Mottolese, M.; Orlandi, G.; Vico, E.; Cognetti, F.; Sperduti, I.; Fabi, A.; Vitelli, G.; Cianciulli, A. Analysis of aneusomy level and HER-2 gene copy number and their effect on amplification rate in breast cancer specimens read as 2+ in immunohistochemical analysis. Eur. J. Cancer 2006, 42, 1501–1506. [Google Scholar] [CrossRef]
- Vodicka, P.; Andera, L.; Opattova, A.; Vodickova, L. The Interactions of DNA Repair, Telomere Homeostasis, and p53 Mutational Status in Solid Cancers: Risk, Prognosis, and Prediction. Cancers 2021, 13, 479. [Google Scholar] [CrossRef]
- Hodgson, A.; van Rhijn, B.W.; Kim, S.S.; Ding, C.; Saleeb, R.; Vesprini, D.; Liu, S.K.; Yousef, G.M.; van der Kwast, T.H.; Xu, B.; et al. Reassessment of p53 immunohistochemistry thresholds in invasive high grade bladder cancer shows a better correlation with TP53 and FGFR3 mutations. Pathol. Res. Pract. 2020, 216, 153186. [Google Scholar] [CrossRef]
- Hodgson, A.; Xu, B.; Downes, M.R. p53 immunohistochemistry in high-grade urothelial carcinoma of the bladder is prognostically significant. Histopathology 2017, 71, 296–304. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. (Eds.) TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2017. [Google Scholar]
- Chang, S.S.; Boorjian, S.A.; Chou, R.; Clark, P.E.; Daneshmand, S.; Konety, B.R.; Pruthi, R.; Quale, D.Z.; Ritch, C.R.; Seigne, J.D.; et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline. J. Urol. 2016, 196, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. Arch. Pathol. Lab. Med. 2018, 142, 1364–1382. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Lespagnard, L.; Durbecq, V.; Paesmans, M.; Desmedt, C.; Gomez-Galdon, M.; Veys, I.; Cardoso, F.; Sotiriou, C.; Di Leo, A.; et al. Polysomy 17 in HER-2/neu Status Elaboration in Breast Cancer: Effect on Daily Practice. Clin. Cancer Res. 2005, 11, 4393–4399. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; Available online: https://www.R-project.org/ (accessed on 18 May 2021).
- Knowles, M.A.; Hurst, C.D. Molecular biology of bladder cancer: New insights into pathogenesis and clinical diversity. Nat. Rev. Cancer 2015, 15, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Lobo, N.; Hensley, P.J.; Bree, K.K.; Nogueras-Gonzalez, G.M.; Navai, N.; Dinney, C.P.; Sylvester, R.J.; Kamat, A.M. Updated European Association of Urology (EAU) Prognostic Factor Risk Groups Overestimate the Risk of Progression in Patients with Non–muscle-invasive Bladder Cancer Treated with Bacillus Calmette-Guérin. Eur. Urol. Oncol. 2022, 5, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Kanamaru, H.; Noriki, S.; Fukuda, M.; Okada, K. Numeric aberration of chromosome 17 is strongly correlated with p53 overexpression, tumor proliferation and histopathology in human bladder cancer. Int. J. Urol. 1998, 5, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Sauter, G.; Moch, H.; Gasser, T.C.; Mihatsch, M.J.; Waldman, F.M. Heterogeneity of chromosome 17 and erbB-2 gene copy number in primary and metastatic bladder cancer. Cytometry 1995, 21, 40–46. [Google Scholar] [CrossRef]
- Mohanty, S.K.; Mishra, S.K.; Tiwari, A.; Sharma, S.; Bhardwaj, M.; Pattnaik, N.; Jaiswal, S.; Baisakh, M.R.; Das, S.; Pradhan, M.R.; et al. Reappraisal of HER2 Amplification in High-Grade Urothelial Carcinoma Based on 2018 ASCO/CAP Clinical Practice Guidelines. Am. J. Clin. Pathol. 2021, 156, 1130–1141. [Google Scholar] [CrossRef]
- Soukup, V.; Čapoun, O.; Cohen, D.; Hernández, V.; Babjuk, M.; Burger, M.; Compérat, E.; Gontero, P.; Lam, T.; MacLennan, S.; et al. Prognostic Performance and Reproducibility of the 1973 and 2004/2016 World Health Organization Grading Classification Systems in Non–muscle-invasive Bladder Cancer: A European Association of Urology Non-muscle Invasive Bladder Cancer Guidelines Panel Systematic Review. Eur. Urol. 2017, 72, 801–813. [Google Scholar] [CrossRef]
- Dyrskjøt, L.; Reinert, T.; Algaba, F.; Christensen, E.; Nieboer, D.; Hermann, G.G.; Mogensen, K.; Beukers, W.; Marquez, M.; Segersten, U.; et al. Prognostic Impact of a 12-gene Progression Score in Non–muscle-invasive Bladder Cancer: A Prospective Multicentre Validation Study. Eur. Urol. 2017, 72, 461–469. [Google Scholar] [CrossRef]
- van Kessel, K.E.; van der Keur, K.A.; Dyrskjøt, L.; Algaba, F.; Welvaart, N.Y.; Beukers, W.; Segersten, U.; Keck, B.; Maurer, T.; Simic, T.; et al. Molecular Markers Increase Precision of the European Association of Urology Non–Muscle-Invasive Bladder Cancer Progression Risk Groups. Clin. Cancer Res. 2018, 24, 1586–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palou, J.; Sylvester, R.J.; Faba, O.R.; Parada, R.; Peña, J.A.; Algaba, F.; Villavicencio, H. Female Gender and Carcinoma In Situ in the Prostatic Urethra Are Prognostic Factors for Recurrence, Progression, and Disease-Specific Mortality in T1G3 Bladder Cancer Patients Treated With Bacillus Calmette-Guérin. Eur. Urol. 2011, 62, 118–125. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient characteristics | ||
| Age at diagnosis | mean | range |
| 65.84 | (40–91) | |
| Gender | n | % |
| Male | 46 | (51.11) |
| Female | 44 | (48.89) |
| Months of follow up | median | range |
| 77 | (2–158) | |
| Intravesical instillation (BCG/Chemo ever) | n | % |
| Yes | 61 | (67.78) |
| No | 22 | (24.44) |
| unknown | 7 | (7.78) |
| Tumor characteristics | n | % |
| Tumor type | ||
| Primary | 70 | (77.78) |
| Recurrent | 20 | (22.22) |
| Stage | ||
| pTa | 42 | (46.67) |
| pT1 | 47 | (52.22) |
| pTis | 1 | (1.11) |
| Grade | ||
| 1 | 20 | (22.22) |
| 2 | 52 | (57.78) |
| 3 | 18 | (20.00) |
| Low grade | 47 | (52.22) |
| High grade | 43 | (47.78) |
| Multiplicity | ||
| Solitary | 79 | (87.78) |
| Multiple | 11 | (12.22) |
| Tumor size | ||
| <3 cm | 68 | (75.56) |
| ≥3 cm | 22 | (24.44) |
| Recurrence | ||
| Yes | 54 | (60.00) |
| No | 36 | (40.00) |
| Progression to T2 | ||
| No | 76 | (84.44) |
| Yes | 14 | (15.56) |
| HER2 Amplified | HER2 Non-Amplified | p | Chr17 Polysomic | Chr17 Non-Polysomic | p | Chr17 High Polysomic | Chr17 Non-High Polysomic | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tumor characteristics | n | % | n | % | n | % | n | % | n | % | n | % | |||
| Tumor type | |||||||||||||||
| Primary | 5 | (71.43) | 65 | (78.31) | 23 | (82.14) | 47 | (75.81) | 8 | (88.89) | 19 | (23.46) | |||
| Recurrent | 2 | (28.57) | 18 | (21.69) | 0.649 | 5 | (17.86) | 15 | (24.19) | 0.592 | 1 | (11.11) | 62 | (76.54) | <0.001 |
| CI of OR | 0.103–7.878 | CI of OR | 0.434–5.787 | CI of OR | 3.047–1168.346 | ||||||||||
| Stage * | |||||||||||||||
| pTa | 0 | (0.00) | 42 | (50.60) | 6 | (21.43) | 36 | (58.06) | 1 | (11.11) | 41 | (50.62) | |||
| pT1 | 7 | (100.00) | 40 | (48.19) | 0.013 | 21 | (75.00) | 26 | (41.94) | 0.002 | 7 | (77.78) | 40 | (49.38) | 0.062 |
| pTis | 0 | (0.00) | 1 | (1.20) | 1 | (3.57) | 0 | (0.00) | 1 | (11.11) | 0 | (0.00) | |||
| CI of OR | 0.000–0.718 | CI of OR | 0.061–0.634 | CI of OR | 0.003- 1.185 | ||||||||||
| Grade ** | |||||||||||||||
| 1 | 0 | (0.00) | 20 | (24.10) | 0 | (0.00) | 20 | (32.26) | 0 | (0.00) | 20 | (24.69) | |||
| 2 | 0 | (0.00) | 52 | (62.65) | <0.001 | 15 | (53.57) | 37 | (59.68) | <0.001 | 3 | (33.33) | 49 | (60.49) | 0.002 |
| 3 | 7 | (100.00) | 11 | (13.25) | 13 | (46.43) | 5 | (8.06) | 6 | (66.67) | 12 | (14.81) | |||
| CI of OR | 0.000–0.129 | CI of OR | 0.025–0.371 | CI of OR | 0.013–0.491 | ||||||||||
| Low grade | 0 | (0.00) | 47 | (56.63) | 4 | (14.29) | 43 | (69.35) | 0 | (0.00) | 47 | (58.02) | |||
| High grade | 7 | (100.00) | 36 | (43.37) | 0.004 | 24 | (85.71) | 19 | (30.65) | <0.001 | 9 | (100.00) | 34 | (41.98) | <0.001 |
| CI of OR | 0.000–0.579 | CI of OR | 0.017–0.263 | CI of OR | 0.000–0.402 | ||||||||||
| Tumor size | |||||||||||||||
| <3 cm | 5 | (71.43) | 63 | (75.90) | 20 | (71.43) | 48 | (77.42) | 5 | (55.56) | 63 | (77.78) | |||
| ≥3 cm | 2 | (28.57) | 20 | (24.10) | 1 | 8 | (28.57) | 14 | (22.58) | 0.600 | 4 | (44.44) | 18 | (22.22) | 0.214 |
| CI of OR | 0.119–8.965 | CI of OR | 0.240–2.346 | CI of OR | 0.070–2.022 | ||||||||||
| Multiplicity | |||||||||||||||
| Solitary | 7 | (100.00) | 72 | (86.75) | 27 | (96.43) | 52 | (83.87) | 9 | (100.00) | 70 | (86.42) | |||
| Multiple | 0 | (0.00) | 11 | (13.25) | 0.591 | 1 | (3.57) | 10 | (16.13) | 0.162 | 0 | (0.00) | 11 | (13.58) | 0.594 |
| CI of OR | 0.190-infinity | CI of OR | 0.665–233.295 | CI of OR | 0.264-infinity | ||||||||||
| Recurrence | |||||||||||||||
| Yes | 3 | (42.86) | 51 | (61.45) | 15 | (53.57) | 39 | (62.90) | 5 | (55.56) | 49 | (60.49) | |||
| No | 4 | (57.14) | 32 | (38.55) | 0.431 | 13 | (46.43) | 23 | (37.10) | 0.487 | 4 | (44.44) | 32 | (39.51) | 1 |
| CI of OR | 0.065–3.004 | CI of OR | 0.251–1.864 | CI of OR | 0.162–4.449 | ||||||||||
| Progression | |||||||||||||||
| Yes | 3 | (42.86) | 11 | (13.25) | 10 | (35.71) | 4 | (6.45) | 5 | (55.56) | 9 | (11.11) | |||
| No | 4 | (57.14) | 72 | (86.75) | 0.073 | 18 | (64.29) | 58 | (93.55) | <0.001 | 4 | (44.44) | 72 | (88.89) | 0.004 |
| CI of OR | 0.618–32.735 | CI of OR | 1.968–38.464 | CI of OR | 1.724–58.357 | ||||||||||
| Variable | Category | HR | 95% CI | p |
|---|---|---|---|---|
| TOTAL cohort—Univariate analyses | ||||
| Age, years | continuous variable | 1.032 | (0.982–1.086) | 0.216 |
| Tumor type | Recurrent vs. primary (Ref.) | 2.691 | (0.934–7.760) | 0.067 |
| T stage | Tis, T1 vs. Ta (Ref.) | 3.354 | (0.921–12.210) | 0.066 |
| Histologic grade (WHO 1973) | Grade 3 vs. grade 1–2 (Ref.) | 3.619 | (1.248–10.490) | 0.018 |
| Histologic grade (WHO 2004/2016) | High grade vs. low grade (Ref.) | 5.243 | (1.441–19.070) | 0.012 |
| Tumor size | ≥3 cm vs. <3 cm (Ref.) | 0.791 | (0.221–2.839) | 0.719 |
| Tumor multiplicity | Multiple vs. solitary (Ref.) | <0.01 | (0.000-infinity) | 0.998 |
| HER2 expression | 3+ vs. 1/2+ or 0 (Ref.) | 1.727 | (0.386–7.727) | 0.475 |
| Heterogeneity for HER2 expression | Heterogenous vs. non-heterogenous (Ref.) | 0.667 | (0.223–1.992) | 0.468 |
| HER2 gene amplification | Amplified vs. non-amplified (Ref.) | 4.036 | (1.122–14.520) | 0.033 |
| Chromosome 17 polysomy | ≥2.25 vs. <2.25 signal/cell (Ref.) | 7.440 | (2.306–24.000) | <0.001 |
| Chromosome 17 high polysomy | ≥3.45 vs. <3.45 signal/cell (Ref.) | 7.505 | (2.478–22.730) | <0.001 |
| Highly polysomic cell population | Yes vs. No (Ref.) | 6.577 | (1.832–23.610) | 0.004 |
| P53 IHC status | 1–49% vs. 0% and 50–100% | 2.427 | (0.7826–7.524) | 0.125 |
| MODEL 1—Multivariable analysis | 0.010 | |||
| Age, years | continuous variable | 1.03462 | (0.980–1.092) | 0.217 |
| Histologic grade (WHO 2004/2016) | High grade vs. low grade (Ref.) | 4.27592 | (1.111–16.457) | 0.035 |
| HER2 gene amplification | Amplified vs. non-amplified (Ref.) | 2.37480 | (0.615–9.174) | 0.210 |
| MODEL 2—Multivariable analysis | 0.001 | |||
| Age, years | continuous variable | 1.042 | (0.983–1.105) | 0.169 |
| Histologic grade (WHO 2004/2016) | High grade vs. low grade (Ref.) | 2.411 | (0.574–10.121) | 0.229 |
| Chromosome 17 polysomy | ≥2.25 vs. <2.25 signal/cell (Ref.) | 5.139 | (1.391–18.983) | 0.014 |
| MODEL 3—Multivariable analysis | 0.003 | |||
| Age, years | continuous variable | 1.02938 | (0.971–1.091) | 0.331 |
| Histologic grade (WHO 2004/2016) | High grade vs. low grade (Ref.) | 3.35917 | (0.828–13.632) | 0.090 |
| Chromosome 17 high polysomy | ≥3.45 vs. <3.45 signal/cell (Ref.) | 4.01119 | (1.206–13.339) | 0.024 |
| MODEL 4—Multivariable analysis | 0.001 | |||
| Age, years | continuous variable | 1.051 | (0.991–1.114) | 0.096 |
| Histologic grade (WHO 2004/2016) | High grade vs. low grade (Ref.) | 2.944 | (0.766–11.322) | 0.116 |
| Highly polysomic cell population | Yes vs. No (Ref.) | 5.403 | (1.004–12.259) | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kocsmár, I.; Kocsmár, É.; Pajor, G.; Kulka, J.; Székely, E.; Kristiansen, G.; Schilling, O.; Nyirády, P.; Kiss, A.; Schaff, Z.; et al. Addition of Chromosome 17 Polysomy and HER2 Amplification Status Improves the Accuracy of Clinicopathological Factor-Based Progression Risk Stratification and Tumor Grading of Non-Muscle-Invasive Bladder Cancer. Cancers 2022, 14, 4570. https://doi.org/10.3390/cancers14194570
Kocsmár I, Kocsmár É, Pajor G, Kulka J, Székely E, Kristiansen G, Schilling O, Nyirády P, Kiss A, Schaff Z, et al. Addition of Chromosome 17 Polysomy and HER2 Amplification Status Improves the Accuracy of Clinicopathological Factor-Based Progression Risk Stratification and Tumor Grading of Non-Muscle-Invasive Bladder Cancer. Cancers. 2022; 14(19):4570. https://doi.org/10.3390/cancers14194570
Chicago/Turabian StyleKocsmár, Ildikó, Éva Kocsmár, Gábor Pajor, Janina Kulka, Eszter Székely, Glen Kristiansen, Oliver Schilling, Péter Nyirády, András Kiss, Zsuzsa Schaff, and et al. 2022. "Addition of Chromosome 17 Polysomy and HER2 Amplification Status Improves the Accuracy of Clinicopathological Factor-Based Progression Risk Stratification and Tumor Grading of Non-Muscle-Invasive Bladder Cancer" Cancers 14, no. 19: 4570. https://doi.org/10.3390/cancers14194570
APA StyleKocsmár, I., Kocsmár, É., Pajor, G., Kulka, J., Székely, E., Kristiansen, G., Schilling, O., Nyirády, P., Kiss, A., Schaff, Z., Riesz, P., & Lotz, G. (2022). Addition of Chromosome 17 Polysomy and HER2 Amplification Status Improves the Accuracy of Clinicopathological Factor-Based Progression Risk Stratification and Tumor Grading of Non-Muscle-Invasive Bladder Cancer. Cancers, 14(19), 4570. https://doi.org/10.3390/cancers14194570