
Radiomics-Based Detection of Radionecrosis Using Harmonized Multiparametric MRI

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
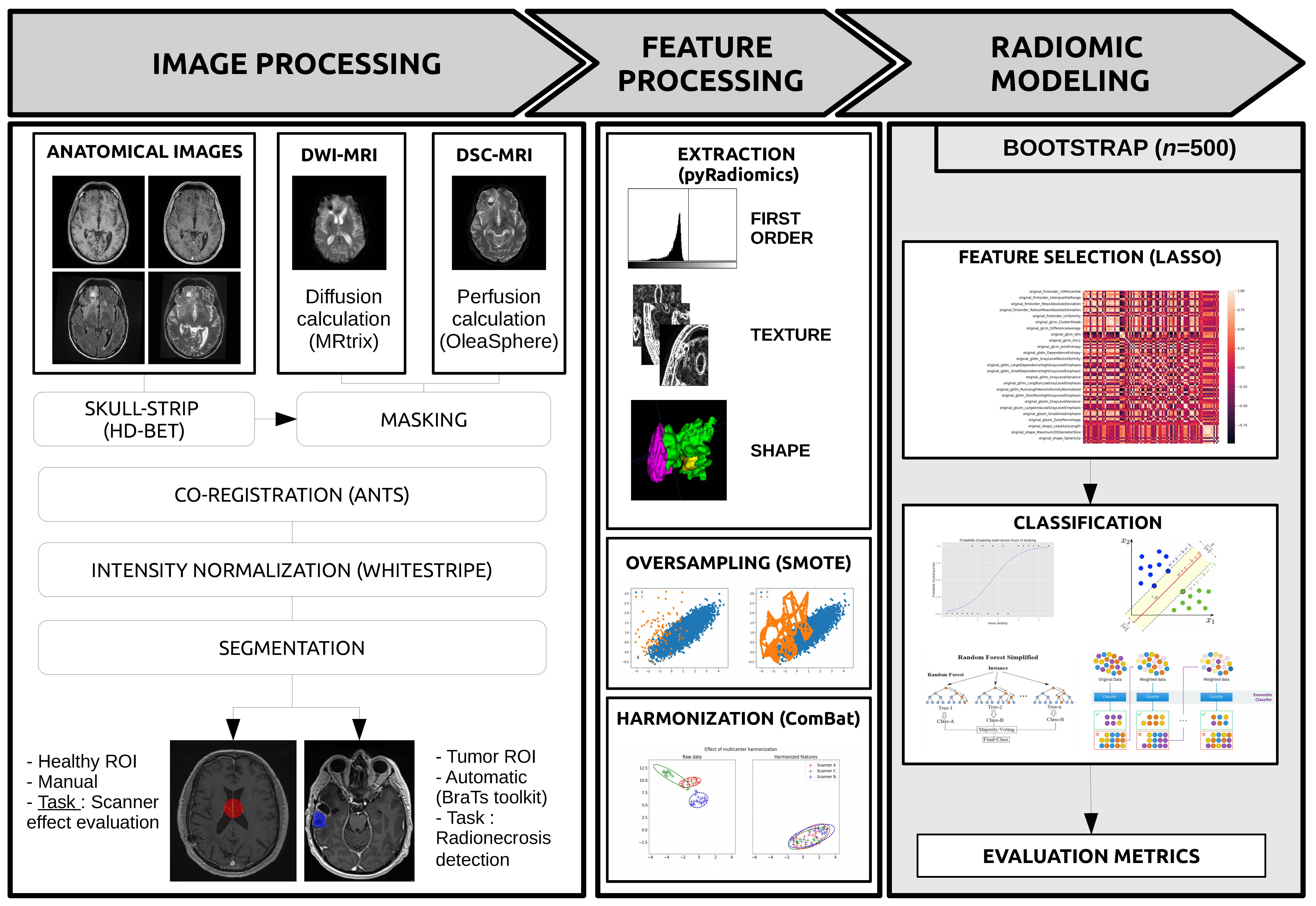
2.2. Images Preprocessing
2.3. Feature Processing
2.4. Radiomics Modeling
3. Results
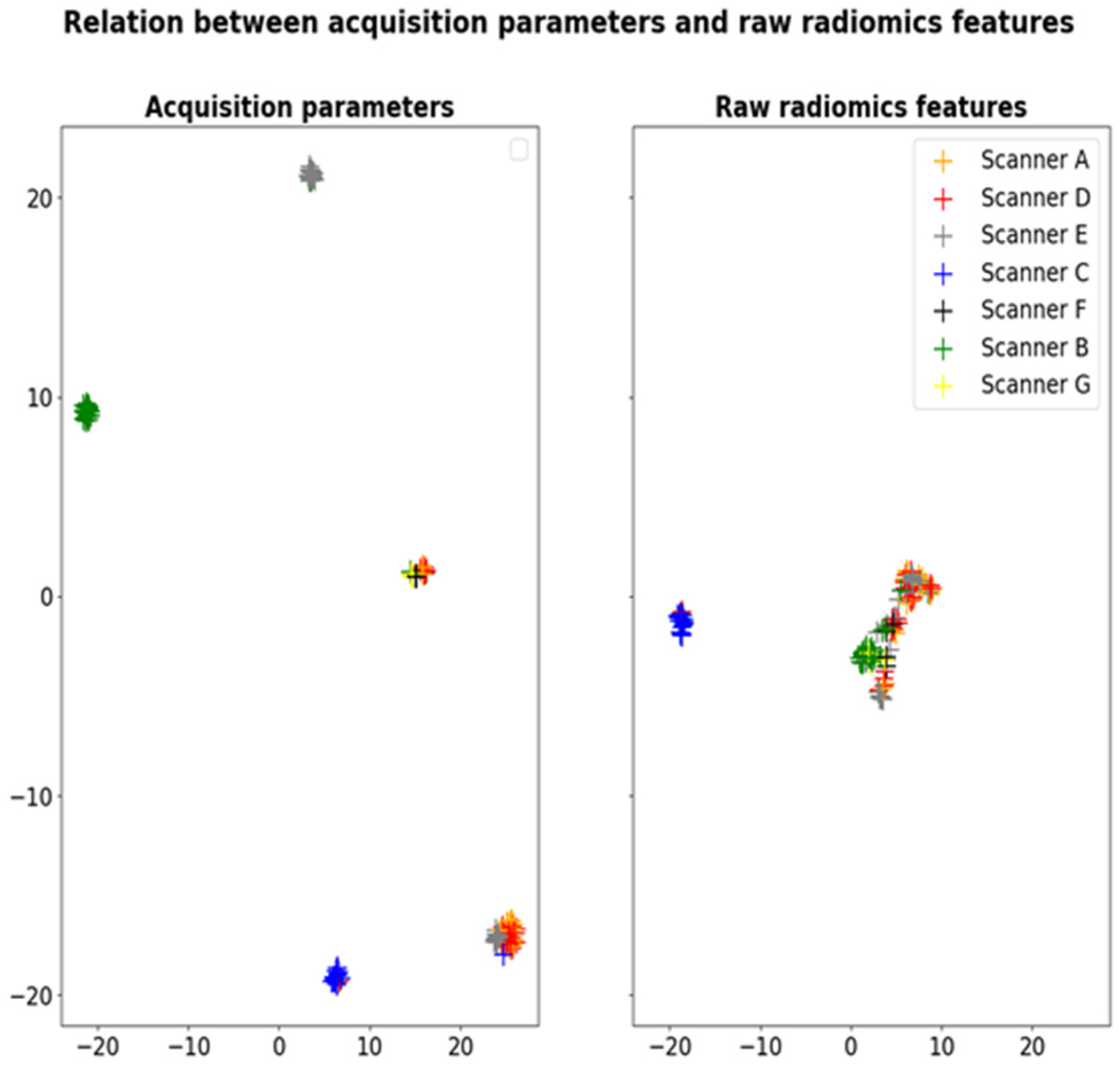
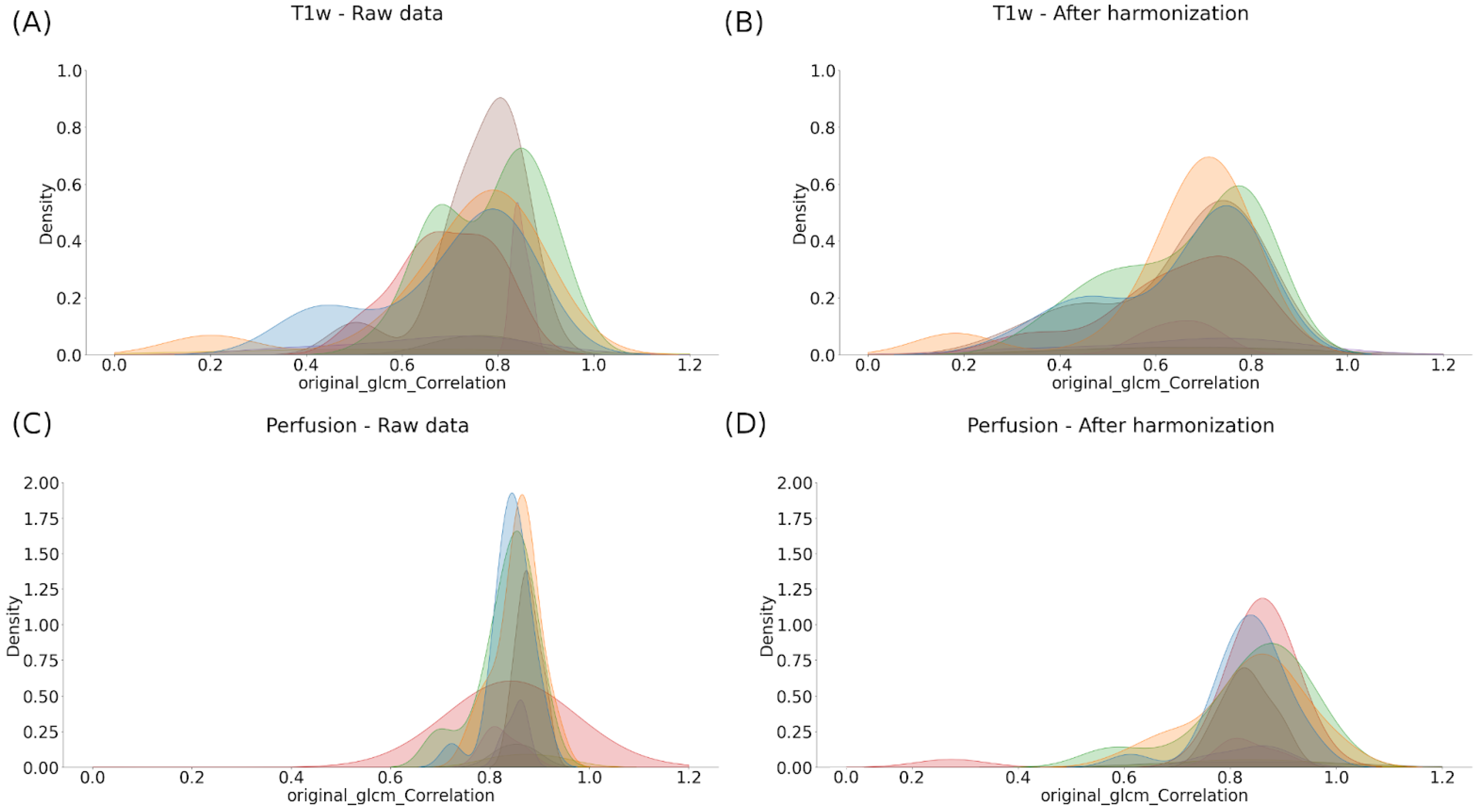
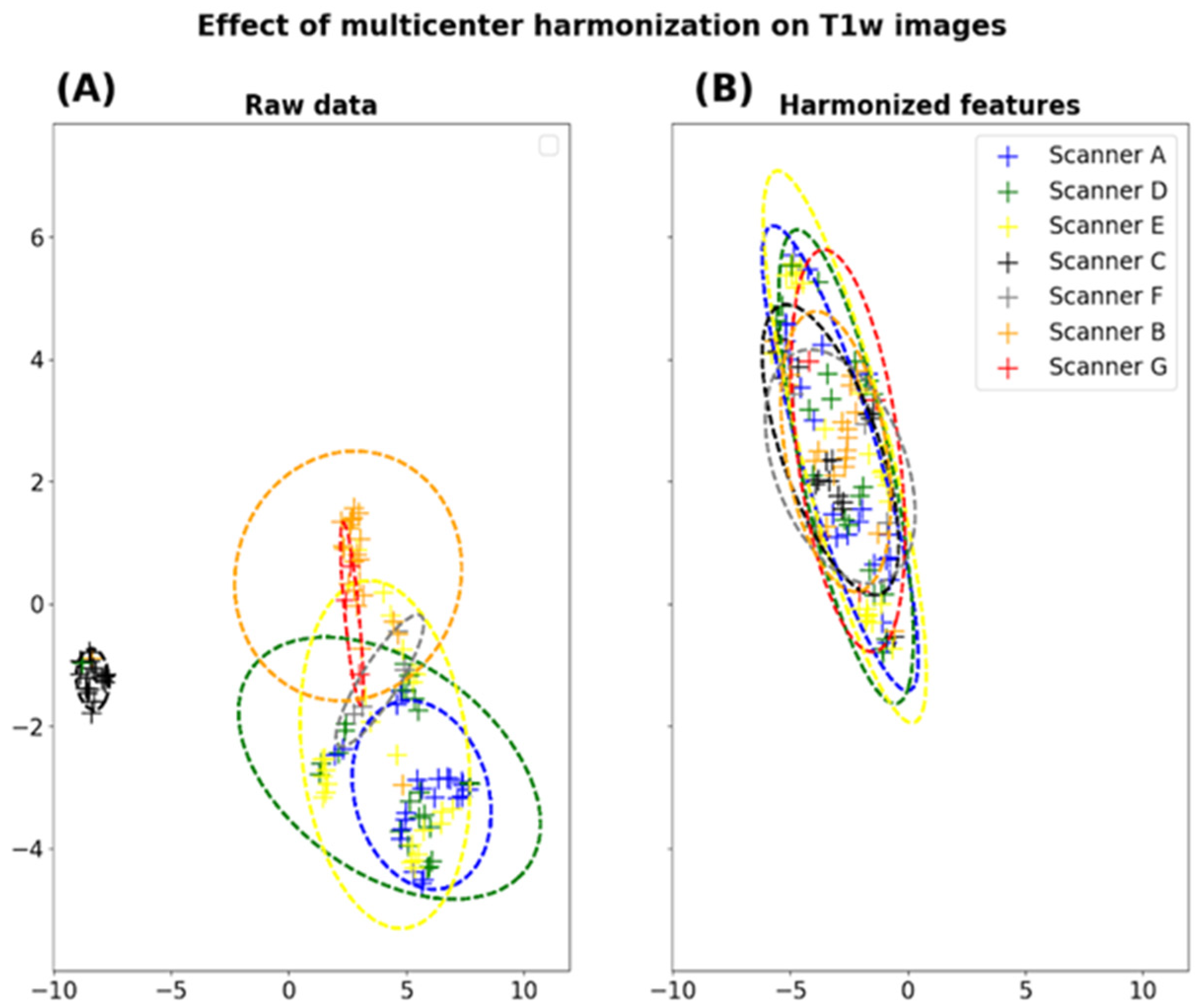
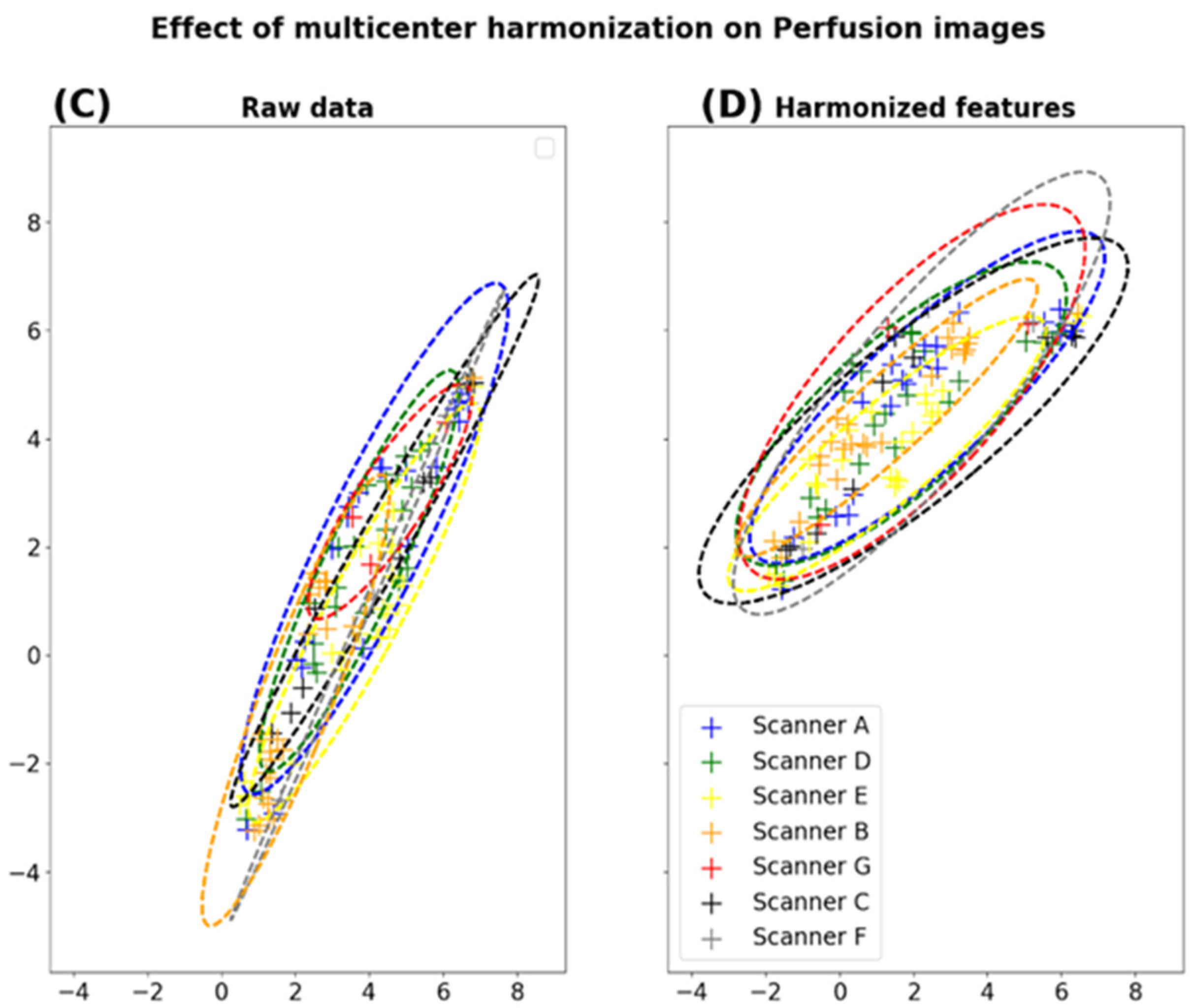
3.1. Characterization and Correction of the “Scanner Effects”
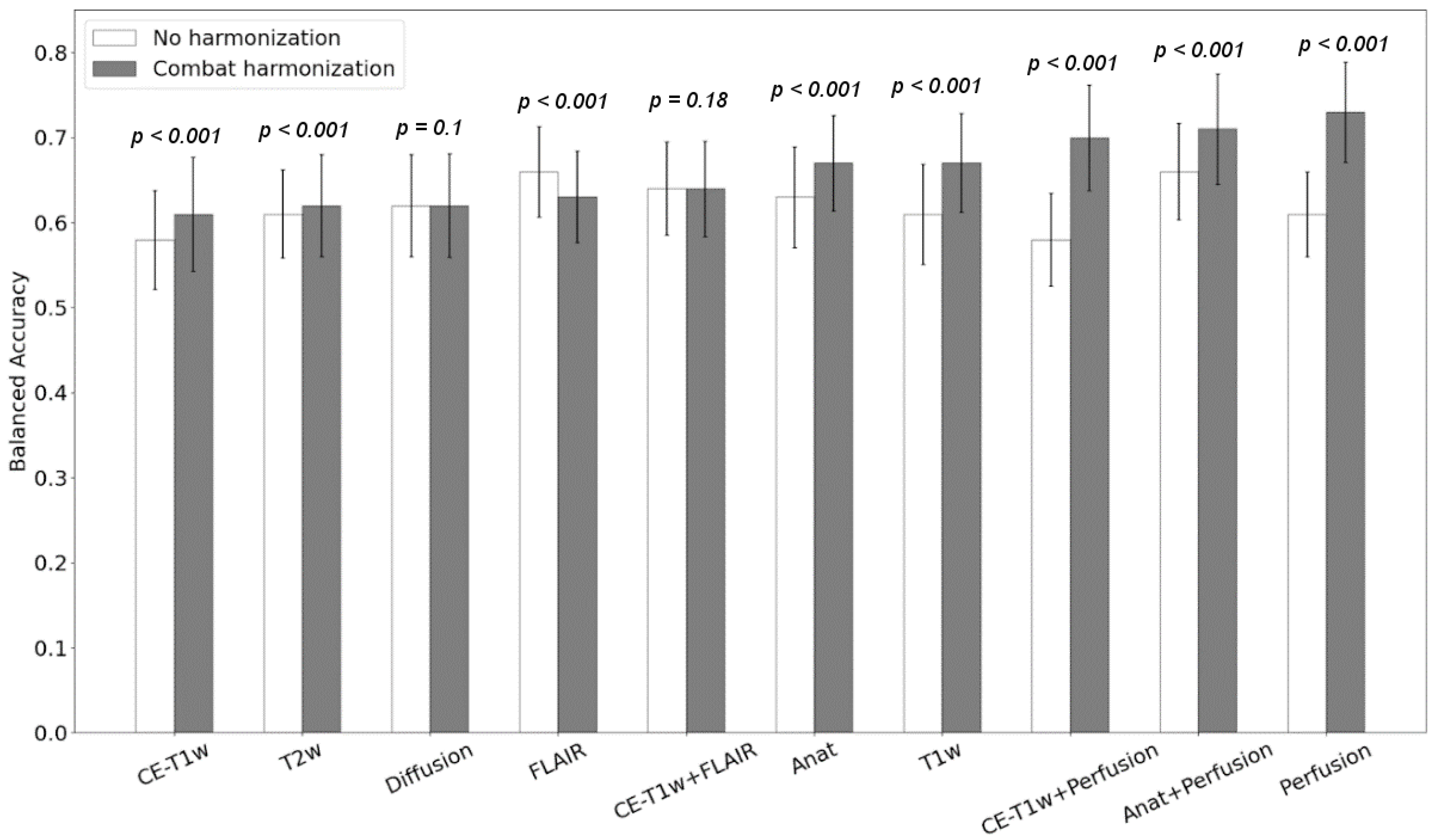
3.2. Prediction of the Radionecrosis
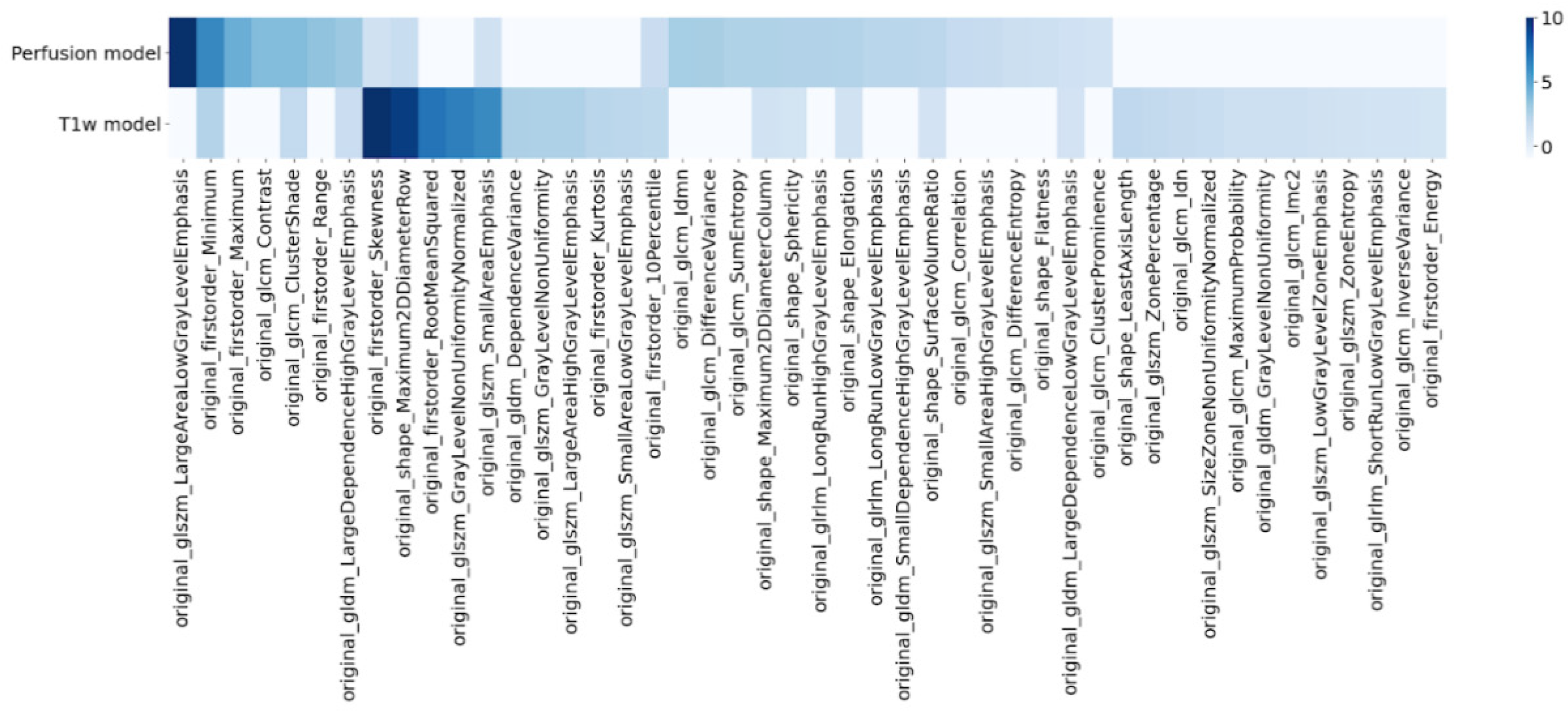
3.3. Radiomics Signature
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MRI | Magnetic Resonance Imaging |
| GBM | Glioblastoma |
| hFSRT | Hypofractionated Stereotactic Radiotherapy |
| CE-T1w | Contrast-Enhancement T1w |
| CBV | Cerebral Blood Volume |
| ADC | Apparent Diffusion Coefficient |
| DWI | Diffusion-Weighted Imaging |
| DSC | Dynamic Susceptibility Contrast |
| ROI | Region of Interest |
| SMOTE | Synthetic Minority Oversampling Technique |
| CRF | Case Report Form |
| LASSO | Least Absolute Shrinkage and Selection Operator |
| LR | Logistic Regression |
| SVC | Support Vector Classifier |
| RF | Random Forest |
| AD | AdaBoost |
| WS | WhiteStripe |
References
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Weller, M.; van den Bent, M.; Tonn, J.C.; Stupp, R.; Preusser, M.; Cohen-Jonathan-Moyal, E.; Henriksson, R.; Le Rhun, E.; Balana, C.; Chinot, O.; et al. European Association for Neuro-Oncology (EANO) Task Force on Gliomas. European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment ofadult astrocytic and oligodendroglial gliomas. Lancet Oncol. 2017, 18, e315–e329. [Google Scholar] [CrossRef] [Green Version]
- Guan, Y.; Xiong, J.; Pan, M.; Shi, W.; Li, J.; Zhu, H.; Gong, X.; Li, C.; Mei, G.; Liu, X.; et al. Safety and efficacy of Hypofractionated stereotactic radiosurgery for high-grade Gliomas at first recurrence: A single-center experience. BMC Cancer 2021, 21, 123. [Google Scholar] [CrossRef] [PubMed]
- Minniti, G.; Clarke, E.; Lanzetta, G.; Osti, M.F.; Trasimeni, G.; Bozzao, A.; Romano, A.; Enrici, R.M. Stereotactic radiosurgery forbrain metastases: Analysis of outcome and risk of brain radionecrosis. Radiat. Oncol. 2011, 6, 48. [Google Scholar] [CrossRef] [Green Version]
- Combs, S.E.; Thilmann, C.; Edler, L.; Debus, J.; Schulz-Ertner, D. Efficacy of fractionated stereotactic reirradiation inrecurrent gliomas: Long-term results in 172 patients treated in a single institution. J. Clin. Oncol. 2005, 23, 8863–8869. [Google Scholar] [CrossRef]
- Nael, K.; Bauer, A.H.; Hormigo, A.; Lemole, M.; Germano, I.M.; Puig, J.; Stea, B. Multiparametric MRI for Differentiationof Radiation Necrosis From Recurrent Tumor in Patients With Treated Glioblastoma. Am. J. Roentgenol. 2018, 210, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Zhao, B.; Zhang, Y.; Ge, M.; Zhao, P.; Li, C.; Pang, Q.; Xu, S.; Liu, Y. Absolute CBV for the differentiation of recurrence and radionecrosis of brain metastases after gamma knife radiotherapy: A comparison with relative CBV. Clin. Radiol. 2018, 73, 758.e1–758.e7. [Google Scholar] [CrossRef] [PubMed]
- Metaweh, N.A.K.; Azab, A.O.; El Basmy, A.A.E.H.; Mashhour, K.N.; El Mahdy, W.M. Contrast-Enhanced Perfusion MR Imaging to Differentiate Between Recurrent/Residual Brain Neoplasms and Radiation Necrosis. Asian Pac. J. Cancer Prev. 2018, 19, 941–948. [Google Scholar] [CrossRef]
- Barajas, R.F.; Chang, J.S.; Segal, M.R.; Parsa, A.T.; McDermott, M.W.; Berger, M.S.; Cha, S. Differentiation of Recurrent Glioblastoma Multiforme from Radiation Necrosis after External Beam Radiation Therapy with Dynamic Susceptibility-weighted Contrast-enhanced Perfusion MR Imaging. Radiology 2009, 253, 486–496. [Google Scholar] [CrossRef]
- Chaddad, A.; Kucharczyk, M.J.; Daniel, P.; Sabri, S.; Jean-Claude, B.J.; Niazi, T.; Abdulkarim, B. Radiomics in Glioblastoma: Current Status and Challenges Facing Clinical Implementation. Front. Oncol. 2019, 9, 374. [Google Scholar] [CrossRef] [Green Version]
- Hettal, L.; Stefani, A.; Salleron, J.; Courrech, F.; Behm-Ansmant, I.; Constans, J.M.; Gauchotte, G.; Vogin, G. Radiomics Method for the Differential Diagnosis of Radionecrosis Versus Progression after Fractionated Stereotactic Body Radiotherapy for Brain Oligometastasis. Radiat. Res. 2020, 193, 471–480. [Google Scholar] [CrossRef]
- Peng, L.; Parekh, V.; Huang, P.; Lin, D.D.; Sheikh, K.; Baker, B.; Kirschbaum, T.; Silvestri, F.; Son, J.; Robinson, A.; et al. Distinguishing True Progression From Radionecrosis After Stereotactic Radiation Therapy for Brain Metastases With Machine Learning and Radiomics. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1236–1243. [Google Scholar] [CrossRef]
- Park, Y.W.; Choi, D.; Park, J.E.; Ahn, S.S.; Kim, H.; Chang, J.H.; Kim, S.H.; Kim, H.S.; Lee, S.K. Differentiation of recurrent glioblastoma from radiation necrosis using diffusion radiomics with machine learning model development and external validation. Sci. Rep. 2021, 11, 2913. [Google Scholar] [CrossRef]
- Um, H.; Tixier, F.; Bermudez, D.; Deasy, J.O.; Young, R.J.; Veeraraghavan, H. Impact of image preprocessing on the scanner dependence of multi-parametric MRI radiomic features and covariate shift in multi-institutional glioblastoma datasets. Phys. Med. Biol. 2019, 64, 16. [Google Scholar] [CrossRef] [PubMed]
- Orlhac, F.; Lecler, A.; Savatovski, J.; Goya-Outi, J.; Nioche, C.; Charbonneau, F.; Ayache, N.; Frouin, F.; Duron, L.; Buvat, I. How can we combat multicenter variability in MR radiomics? Validation of a correction procedure. Eur. J. Radiol. 2020, 31, 2272–2280. [Google Scholar] [CrossRef]
- Johnson, W.E.; Li, C.; Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2006, 8, 118–127. [Google Scholar] [CrossRef]
- Da-Ano, R.; Masson, I.; Lucia, F.; Doré, M.; Robin, P.; Alfieri, J.; Rousseau, C.; Mervoyer, A.; Reinhold, C.; Castelli, J.; et al. Performance comparison of modified ComBat for harmonization of radiomic features for multicenter studies. Sci. Rep. 2020, 10, 10248. [Google Scholar] [CrossRef] [PubMed]
- Pouessel, D.; Mervoyer, A.; Larrieu-Ciron, D.; Cabarrou, B.; Attal, J.; Robert, M.; Frenel, J.S.; Olivier, P.; Poublanc, M.; Mounier, M.; et al. Hypofractionnated stereotactic radiotherapy and anti-PDL1 durvalumab combination in recurrent glioblastoma: Results of the phase I part of the phase I/II STERIMGLI trial. J. Clin. Oncol. 2018, 36, 2046. [Google Scholar] [CrossRef]
- Okada, H.; Weller, M.; Huang, R.; Finocchiaro, G.; Gilbert, M.R.; Wick, W.; Ellingson, B.M.; Hashimoto, N.; Pollack, I.F.; Brandes, A.A.; et al. Immunotherapy response assessment in neuro-oncology: A report of the RANO working group. Lancet Oncol. 2015, 16, e534–e542. [Google Scholar] [CrossRef] [Green Version]
- Kofler, F.; Berger, C.; Waldmannstetter, D.; Lipkova, J.; Ezhov, I.; Tetteh, G.; Kirschke, J.; Zimmer, C.; Wiestler, B.; Menze, B.H. BraTS Toolkit: Translating BraTS Brain Tumor Segmentation Algorithms Into Clinical and Scientific Practice. Front. Neurosci. 2020, 14, 125. [Google Scholar] [CrossRef]
- Isensee, F.; Schell, M.; Pflueger, I.; Brugnara, G.; Bonekamp, D.; Neuberger, U.; Wick, A.; Schlemmer, H.P.; Heiland, S.; Wick, W.; et al. Automated brain extraction of multisequence MRI using artificial neural networks. Hum. Brain Mapp. 2019, 40, 4952–4964. [Google Scholar] [CrossRef] [Green Version]
- Tournier, J.D.; Smith, R.; Raffelt, D.; Tabbara, R.; Dhollander, T.; Pietsch, M.; Christiaens, D.; Jeurissen, B.; Yeh, C.H.; Connelly, A. MRtrix3: A fast, flexible and open software framework for medical image processing and visualisation. NeuroImage 2019, 202, 116137. [Google Scholar] [CrossRef]
- Shinohara, R.T.; Sweeney, E.M.; Goldsmith, J.; Shiee, N.; Mateen, F.J.; Calabresi, P.A.; Jarso, S.; Pham, D.L.; Reich, D.S.; Crainiceanu, C.M. Statistical normalization techniques for magnetic resonance imaging. Neuroimage Clin. 2014, 6, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Ammari, S.; Balleyguier, C.; Lassau, N.; Chouzenoux, E. Impact of Preprocessing and Harmonization Methods on the Removal of Scanner Effects in Brain MRI Radiomic Features. Cancers 2021, 13, 3000. [Google Scholar] [CrossRef]
- Piram, L.; Acquitter, C.; Sabatini, U.; Lemasson, B.; Moyal, E.; El Idrissi, S.; Ken, S. P04.06 Can BraTS Toolkit Brain Tumor Segmentation Algorithms be relevant when dealing with post-operative MRI in clinical practice? Neuro-Oncol. 2021, 23, ii19–ii20. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. Ser. B (Methodol.) 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Shah, R.; Vattoth, S.; Jacob, R.; Manzil, F.F.P.; O’Malley, J.P.; Borghei, P.; Patel, B.N.; Curé, J.K. Radiation Necrosis in the Brain: Imaging Features and Differentiation from Tumor Recurrence. Radiographics 2012, 32, 1343–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dequesada, I.M.; Quisling, R.G.; Yachnis, A.; Friedman, W.A. Can standard magnetic resonance imaging reliably distinguish recurrent tumor from radiation necrosis after radiosurgery for brain metastases? A radiographic-pathological study. Neurosurgery 2008, 63, 898–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cetin-Karayumak, S.; Stegmayer, K.; Walther, S.; Szeszko, P.R.; Crow, T.; James, A.; Keshavan, M.; Kubicki, M.; Rathi, Y. Exploring the limits of ComBat method for multi-site diffusion MRI harmonization. BioRxiv Prepr. Serv. Biol. 2020. [Google Scholar] [CrossRef]
- Chuang, M.T.; Liu, Y.S.; Tsai, Y.S.; Chen, Y.C.; Wang, C.K. Differentiating Radiation-Induced Necrosis from Recurrent Brain Tumor Using MR Perfusion and Spectroscopy: A Meta-Analysis. PLoS ONE 2016, 11, e0141438. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Phase I | Phase II | ||
|---|---|---|---|---|
| Arm A | Arm B | |||
| Total | 6 | 6 | 16 | |
| Age (mean = 56) | ||||
| Sex | Male | 3 | 4 | 12 |
| Female | 3 | 2 | 4 | |
| Surgery | Biopsy | 2 | 1 | 3 |
| Near-complete resection | 3 | 4 | 7 | |
| Complete resection | 2 | 1 | 9 | |
| MGMT Status | Methylated | 3 | 3 | 11 |
| Unmethylated | 3 | 3 | 5 | |
| Radionecrosis status | Positive | 2 | 1 | 9 |
| Negative | 4 | 5 | 7 | |
| A | B | C | D | E | F | G | ||
|---|---|---|---|---|---|---|---|---|
| MRI examination | 20 | 10 | 24 | 22 | 23 | 3 | 3 | |
| Radionecrosis | 5 | 1 | 10 | 11 | 9 | 1 | 1 | |
| MRI Model | Siemens Aera | GE Optima | Siemens Skyra | Siemens Aera | Siemens Skyra | GE Optima | GE Signa | |
| Magnetic Field | 1.5 | 1.5 | 3 | 1.5 | 3 | 1.5 | 3 | |
| T1w | TE (ms) | 11.0 | 7.6 | 220 | 11.0 | 2200 | 7.63 | 600 |
| TR (ms) | 5.37 | 3.16 | 2.49 | 5.37 | 2.48 | 3.1 | 10.4 | |
| FA (°) | 15 | 15 | 70 | 15 | 8 | 15 | 90 | |
| T2w | TE (ms) | 7540 | 6000 | 800 | 8250 | 5300 | 81 | 58 |
| TR (ms) | 115 | 100 | 20 | 115 | 111 | 48.5 | 30 | |
| FA (°) | 170 | 160 | 20 | 170 | 150 | 30 | 15 | |
| FLAIR | TE (ms) | 7000 | 12,000 | 8000 | 7000 | 6600 | 8000 | 9800 |
| TR (ms) | 124 | 131.3 | 140 | 124 | 349 | 123.3 | 141 | |
| FA (°) | 180 | 160 | 150 | 180 | 120 | 90 | 90 | |
| DWI | TE (ms) | 7800 | 8000 | 6430 | 7800 | 7110 | 4500 | 11,700 |
| TR (ms) | 70 | 72.4 | 71 | 107 | 64 | 69.9 | 72.7 | |
| FA (°) | 180 | 90 | 180 | 90 | 180 | 90 | 90 | |
| DSC | TE (ms) | 1880 | 1800 | 1980 | 1970 | 1770 | 2000 | 1770 |
| TR (ms) | 30 | 65 | 30 | 30 | 25 | 60 | 25 | |
| FA (°) | 90 | 90 | 90 | 90 | 90 | 90 | 90 | |
| Classification Score | Perfusion | T1w | |||
|---|---|---|---|---|---|
| Non-ComBat | ComBat | Non-ComBat | ComBat | ||
| Logistic Regression | B. Accuracy | 0.61 ± 0.05 | 0.73 ± 0.059 (*) | 0.61 ± 0.059 | 0.67 ± 0.058 (*) |
| Sensitivity | 0.6 ± 0.109 | 0.75 ± 0.09 | 0.6 ± 0.11 | 0.65 ± 0.108 | |
| Specificity | 0.61 ± 0.105 | 0.7 ± 0.101 | 0.63 ± 0.117 | 0.68 ± 0.097 | |
| Support Vector Classifier | B. Accuracy | 0.6 ± 0.057 | 0.72 ± 0.057 (*) | 0.61 ± 0.059 | 0.66 ± 0.062 (*) |
| Sensitivity | 0.62 ± 0.126 | 0.73 ± 0.094 | 0.61 ± 0.109 | 0.65 ± 0.12 | |
| Specificity | 0.59 ± 0.115 | 0.71 ± 0.107 | 0.62 ± 0.118 | 0.67 ± 0.106 | |
| Random Forest | B. Accuracy | 0.63 ± 0.052 | 0.75 ± 0.06 (*) | 0.6 ± 0.059 | 0.64 ± 0.056 (*) |
| Sensitivity | 0.63 ± 0.126 | 0.75 ± 0.107 | 0.57 ± 0.13 | 0.63 ± 0.127 | |
| Specificity | 0.64 ± 0.121 | 0.76 ± 0.109 | 0.62 ± 0.142 | 0.65 ± 0.124 | |
| AdaBoost | B. Accuracy | 0.6 ± 0.059 | 0.76 ± 0.063 (*) | 0.58 ± 0.062 | 0.61 ± 0.063 (*) |
| Sensitivity | 0.6 ± 0.112 | 0.76 ± 0.102 | 0.57 ± 0.13 | 0.61 ± 0.114 | |
| Specificity | 0.6 ± 0.115 | 0.76 ± 0.102 | 0.59 ± 0.116 | 0.62 ± 0.119 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acquitter, C.; Piram, L.; Sabatini, U.; Gilhodes, J.; Moyal Cohen-Jonathan, E.; Ken, S.; Lemasson, B. Radiomics-Based Detection of Radionecrosis Using Harmonized Multiparametric MRI. Cancers 2022, 14, 286. https://doi.org/10.3390/cancers14020286
Acquitter C, Piram L, Sabatini U, Gilhodes J, Moyal Cohen-Jonathan E, Ken S, Lemasson B. Radiomics-Based Detection of Radionecrosis Using Harmonized Multiparametric MRI. Cancers. 2022; 14(2):286. https://doi.org/10.3390/cancers14020286
Chicago/Turabian StyleAcquitter, Clément, Lucie Piram, Umberto Sabatini, Julia Gilhodes, Elizabeth Moyal Cohen-Jonathan, Soleakhena Ken, and Benjamin Lemasson. 2022. "Radiomics-Based Detection of Radionecrosis Using Harmonized Multiparametric MRI" Cancers 14, no. 2: 286. https://doi.org/10.3390/cancers14020286
APA StyleAcquitter, C., Piram, L., Sabatini, U., Gilhodes, J., Moyal Cohen-Jonathan, E., Ken, S., & Lemasson, B. (2022). Radiomics-Based Detection of Radionecrosis Using Harmonized Multiparametric MRI. Cancers, 14(2), 286. https://doi.org/10.3390/cancers14020286