
The Decision-Making Process for Palliative Sedation for Patients with Advanced Cancer–Analysis from a Systematic Review of Prospective Studies

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
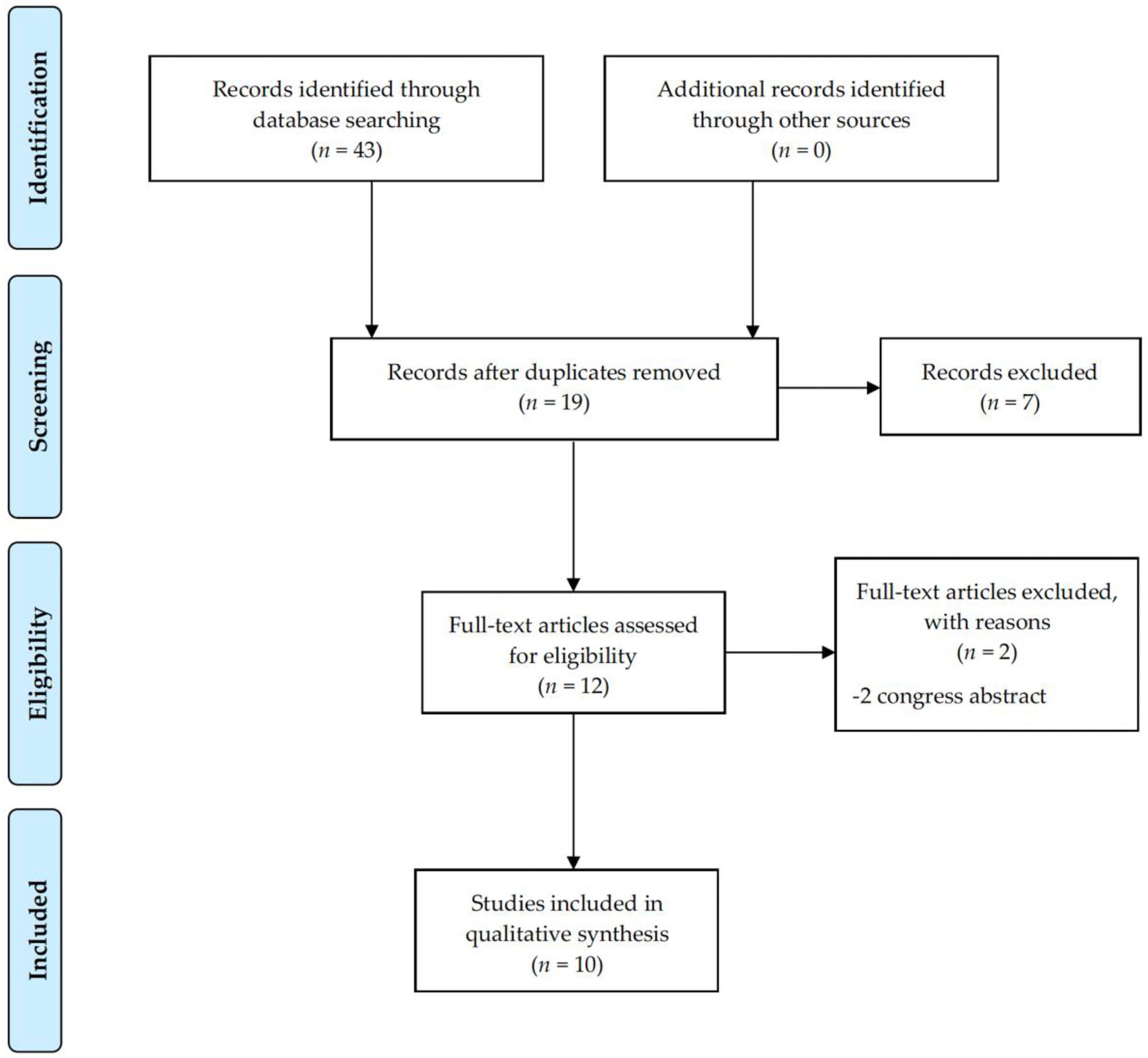
2. Materials and Methods
3. Results
3.1. When and by Whom the Decision-Making Process about Palliative Sedation Is Initiated
3.2. Patients’ Involvement
3.3. Family Involvement
3.4. Healthcare Involvement
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Waldrop, D.P.; Meeker, M.A. Communication and advanced care planning in palliative and end-of-life care. Nurs. Outlook 2012, 60, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Griffioen, I.P.M.; Rietjens, J.A.C.; Melles, M.; Snelders, D.; Homs, M.Y.V.; van Eijck, C.H.; Stiggelbout, A.M. The bigger picture of shared decision making: A service design perspective using the care path of locally advanced pancreatic cancer as a case. Cancer Med. 2021, 10, 5907–5916. [Google Scholar] [CrossRef] [PubMed]
- Chewning, B.; Bylund, C.L.; Shah, B.; Arora, N.K.; Gueguen, J.A.; Makoul, G. Patient preferences for shared decisions: A systematic review. Patient Educ. Couns. 2012, 86, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinkman-Stoppelenburg, A.; Rietjens, J.A.C.; van der Heide, A. The effects of advance care planning on end-of-life care: A systematic review. Palliat. Med. 2014, 28, 1000–1025. [Google Scholar] [CrossRef] [PubMed]
- Paladino, J.; Koritsanszky, L.; Neal, B.J.; Lakin, J.R.; Kavanagh, J.; Lipsitz, S.; Fromme, E.K.; Sanders, J.; Benjamin, E.; Block, S.; et al. Effect of the Serious Illness Care Program on Health Care Utilization at the End of Life for Patients with Cancer. J. Palliat. Med. 2020, 23, 1365–1369. [Google Scholar] [CrossRef] [PubMed]
- Cherny, N.I.; Radbruch, L. European Association for Palliative Care (EAPC) recommended framework for the use of sedation in palliative care. Palliat. Med. 2009, 23, 581–593. [Google Scholar] [CrossRef]
- Belar, A.; Arantzamendi, M.; Payne, S.; Preston, N.; Lee-Rijpstra, M.; Hasselaar, J.; Radbruch, L.; Vanderelst, M.; Ling, J.; Centeno, C. How to measure the effects and potential adverse events of palliative sedation? An integrative review. Palliat. Med. 2021, 35, 295–314. [Google Scholar] [CrossRef]
- van Deijck, R.H.P.D.; Hasselaar, J.G.J.; Verhagen, S.C.A.H.H.V.M.; Vissers, K.C.P.; Koopmans, R.T.C.M. Patient-Related Determinants of the Administration of Continuous Palliative Sedation in Hospices and Palliative Care Units: A Prospective, Multicenter, Observational Study. J. Pain Symptom Manag. 2016, 51, 882–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Graeff, A.; Dean, M. Palliative sedation therapy in the last weeks of life: A literature review and recommendations for standards. J. Palliat. Med. 2007, 10, 67–85. [Google Scholar] [CrossRef] [PubMed]
- Materstvedt, L.J.; Bosshard, G. Deep and continuous palliative sedation (terminal sedation): Clinical-ethical and philosophical aspects. Lancet Oncol. 2009, 10, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Roeland, E.; Cain, J.; Onderdonk, C.; Kerr, K.; Mitchell, W.; Thornberry, K. When open-ended questions don’t work: The role of palliative paternalism in difficult medical decisions. J. Palliat. Med. 2014, 17, 415–420. [Google Scholar] [CrossRef]
- Morita, T.; Ikenaga, M.; Adachi, I.; Narabayashi, I.; Kizawa, Y.; Honke, Y.; Kohara, H.; Mukaiyama, T.; Akechi, T.; Kurihara, Y.; et al. Concerns of family members of patients receiving palliative sedation therapy. Support. Care Cancer 2004, 12, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Brajtman, S. The impact on the family of terminal restlessness and its management. Palliat. Med. 2003, 17, 454–460. [Google Scholar] [CrossRef]
- Rietjens, J.A.C.; Hauser, J.; Van Der Heide, A.; Emanuel, L. Having a difficult time leaving: Experiences and attitudes of nurses with palliative sedation. Palliat. Med. 2007, 21, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Miyashita, M.; Kimura, R.; Adachi, I.; Shima, Y. Emotional burden of nurses in palliative sedation therapy. Palliat. Med. 2004, 18, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Arantzamendi, M.; Belar, A.; Payne, S.; Rijpstra, M.; Preston, N.; Menten, J.; Van der Elst, M.; Radbruch, L.; Hasselaar, J.; Centeno, C. Clinical Aspects of Palliative Sedation in Prospective Studies. A Systematic Review. J. Pain Symptom Manag. 2021, 61, 831–844.e10. [Google Scholar] [CrossRef]
- Heaton, J. Secondary analysis of qualitative data: An overview. Hist. Soc. Res. Sozialforsch. 2008, 33, 33–45. [Google Scholar]
- Oliver, D.P.; Washington, K.; Demiris, G.; Wallace, A.; Propst, M.R.; Uraizee, A.M.; Craig, K.; Clayton, M.F.; Rebrin, M.; Ellington, L. Shared Decision Making in Home Hospice Nursing Visits: A Qualitative Study. J. Pain Symptom Manag. 2018, 55, 922–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunleavy, L.J.; Walshe, C.; Oriani, A.; Preston, N. Using the ‘Social Marketing Mix Framework’ to explore recruitment barriers and facilitators in palliative care randomised controlled trials? A narrative synthesis review. Palliat. Med. 2018, 32, 990–1009. [Google Scholar] [CrossRef] [Green Version]
- Parra Palacio, S.; Giraldo Hoyos, C.E.; Arias Rodríguez, C.; Mejía Arrieta, D.; Vargas Gómez, J.J.; Krikorian, A. Palliative sedation in advanced cancer patients hospitalized in a specialized palliative care unit. Support. Care Cancer 2018, 26, 3173–3180. [Google Scholar] [CrossRef]
- Monreal-Carrillo, E.; Allende-Perez, S.; Hui, D.; Garcia-Salamanca, M.-F.; Bruera, E.; Verastegui, E. Bispectral Index monitoring in cancer patients undergoing palliative sedation: A preliminary report. Support. Care Cancer. 2017, 25, 3143–3149. [Google Scholar] [CrossRef]
- van Deijck, R.H.P.D.; Hasselaar, J.G.J.; Verhagen, S.C.A.H.H.V.M.; Vissers, K.C.P.; Koopmans, R.T.C.M. Level of Discomfort Decreases After the Administration of Continuous Palliative Sedation: A Prospective Multicenter Study in Hospices and Palliative Care Units. J. Pain Symptom Manag. 2016, 52, 361–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caraceni, A.; Speranza, R.; Spoldi, E.; Ambroset, C.S.; Canestrari, S.; Marinari, M.; Marzi, A.M.; Orsi, L.; Piva, L.; Rocchi, M.; et al. Palliative Sedation in Terminal Cancer Patients Admitted to Hospice or Home Care Programs: Does the Setting Matter? Results From a National Multicenter Observational Study. J. Pain Symptom Manag. 2018, 56, 33–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, K.; Morita, T.; Yokomichi, N.; Mori, M.; Naito, A.S.; Tsukuura, H.; Yamauchi, T.; Kawaguchi, T.; Fukuta, K.; Inoue, S. Efficacy of two types of palliative sedation therapy defined using intervention protocols: Proportional vs. deep sedation. Support. Care Cancer 2018, 26, 1763–1771. [Google Scholar] [CrossRef] [PubMed]
- Maeda, I.; Morita, T.; Yamaguchi, T.; Inoue, S.; Ikenaga, M.; Matsumoto, Y.; Sekine, R.; Yamaguchi, T.; Hirohashi, T.; Tajima, T.; et al. Effect of continuous deep sedation on survival in patients with advanced cancer (J-Proval), a propensity score-weighted analysis of a prospective cohort study. Lancet Oncol. 2016, 17, 115–122. [Google Scholar] [CrossRef]
- Mercadante, S.; Porzio, G.; Valle, A.; Aielli, F.; Casuccio, A. Palliative Sedation in Patients with Advanced Cancer Followed at Home: A Prospective Study. J. Pain Symptom Manag. 2014, 47, 860–866. [Google Scholar] [CrossRef] [Green Version]
- Pype, P.; Teuwen, I.; Mertens, F.; Sercu, M.; De Sutter, A. Suboptimal palliative sedation in primary care: An exploration. Acta Clin. Belg. 2017, 73, 21–28. [Google Scholar] [CrossRef]
- Claessens, P.; Menten, J.; Schotsmans, P.; Broeckaert, B. Food and fluid intake and palliative sedation in palliative care units: A longitudinal prospective study. Prog. Palliat. Care 2013, 22, 1–8. [Google Scholar] [CrossRef]
- Benítez-Rosario, M.A.; Ascanio-León, B. Palliative sedation: Beliefs and decision-making among Spanish palliative care physicians. Support. Care Cancer 2020, 28, 2651–2658. [Google Scholar] [CrossRef]
- Olsen, M.L.; Swetz, K.M.; Mueller, P.S. Ethical decision making with end-of-life care: Palliative sedation and withholding or withdrawing life-sustaining treatments. Mayo Clin. Proc. 2010, 85, 949–954. [Google Scholar] [CrossRef] [Green Version]
- De Roo, M.L.; Leemans, K.; Claessen, S.J.J.; Cohen, J.; Pasman, H.R.W.; Deliens, L.; Francke, A.L.; EURO IMPACT. Quality indicators for palliative care: Update of a systematic review. J. Pain Symptom Manag. 2013, 46, 556–572. [Google Scholar] [CrossRef] [PubMed]
- Martins Pereira, S.; Fradique, E.; Hernández-Marrero, P. End-of-Life Decision Making in Palliative Care and Recommendations of the Council of Europe: Qualitative Secondary Analysis of Interviews and Observation Field Notes. J. Palliat. Med. 2018, 21, 604–615. [Google Scholar] [CrossRef]
- Kuosmanen, L.; Hupli, M.; Ahtiluoto, S.; Haavisto, E. Patient participation in shared decision-making in palliative care—An integrative review. J. Clin. Nurs. 2021, 30, 3415–3428. [Google Scholar] [CrossRef]
- Belanger, E.; Rodríguez, C.; Groleau, D.; Légaré, F.; Macdonald, M.E.; Marchand, R. Initiating decision-making conversations in palliative care: An ethnographic discourse analysis. BMC Palliat. Care 2014, 13, 63. [Google Scholar] [CrossRef] [Green Version]
- Robijn, L.; Seymour, J.; Deliens, L.; Korfage, I.; Brown, J.; Pype, P.; Van Der Heide, A.; Chambaere, K.; Rietjens, J.; UNBIASED Consortium. The involvement of cancer patients in the four stages of decision-making preceding continuous sedation until death: A qualitative study. Palliat. Med. 2018, 32, 1198–1207. [Google Scholar] [CrossRef]
- Menezes, M.S.; de Assis Figueiredob, M.d.G.M.d.C. The role of end-of-life palliative sedation: Medical and ethical aspects-Review. Braz. J. Anesthesiol. 2019, 69, 72–77. [Google Scholar] [CrossRef]
- Fainsinger, R.L.; Nunez-Olarte, J.M.; Demoissac, D.M. The cultural differences in perceived value of disclosure and cognition: Spain and Canada. J. Palliat. Care 2003, 19, 43–48. [Google Scholar] [CrossRef]
- Nunez Olarte, J.M.; Guillen, D.G. Cultural issues and ethical dilemmas in palliative and end-of-life care in Spain. Cancer Control 2001, 8, 46–54. [Google Scholar] [CrossRef]
- Cain, C.L.; Surbone, A.; Elk, R.; Kagawa-Singer, M. Culture and Palliative Care: Preferences, Communication, Meaning, and Mutual Decision Making. J. Pain Symptom Manag. 2018, 55, 1408–1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristina, E.; Carlo, S.; Gabriella, D.; Mirella, P. Factors associated with the decision-making process in palliative sedation therapy. The experience of an Italian hospice struggling with balancing various individual autonomiess. Cogent Med. 2017, 4, 1290307. [Google Scholar] [CrossRef]
- Tursunov, O.; Cherny, N.; Ganz, F. Experiences of Family Members of Dying Patients Receiving Palliative Sedation. Oncol. Nurs. Forum 2016, 43, E226–E232. [Google Scholar] [CrossRef] [PubMed]
- Luna-Meza, A.; Godoy-Casasbuenas, N.; Calvache, J.A.; Díaz-Amado, E.; Gempeler Rueda, F.E.; Morales, O.; Leal, F.; Gómez-Restrepo, C.; de Vries, E. Decision making in the end-of-life care of patients who are terminally ill with cancer—A qualitative descriptive study with a phenomenological approach from the experience of healthcare workers. BMC Palliat. Care 2021, 20, 76. [Google Scholar] [CrossRef]
- Hamano, J.; Morita, T.; Mori, M.; Uchitomi, Y. Talking About Palliative Sedation with the Family: Informed Consent vs. Assent and a Better Framework for Explaining Potential Risks. J. Pain Symptom Manag. 2018, 56, e5–e8. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.; Porterfield, P.; Bouchal, S.R.; Heyland, D. “Not yet” and “Just ask”: Barriers and facilitators to advance care planning--a qualitative descriptive study of the perspectives of seriously ill, older patients and their families. BMJ Support. Palliat. Care 2015, 5, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Zwakman, M.; Jabbarian, L.; van Delden, J.; van der Heide, A.; Korfage, I.; Pollock, K.; Rietjens, J.; Seymour, J.; Kars, M. Advance care planning: A systematic review about experiences of patients with a life-threatening or life-limiting illness. Palliat. Med. 2018, 32, 1305–1321. [Google Scholar] [CrossRef] [Green Version]
- Rietjens, J.A.C.; Sudore, R.L.; Connolly, M.; van Delden, J.J.; Drickamer, M.A.; Droger, M.; van der Heide, A.; Heyland, D.K.; Houttekier, D.; Janssen, D.J.A.; et al. Definition and recommendations for advance care planning: An international consensus supported by the European Association for Palliative Care. Lancet Oncol. 2017, 18, e543–e551. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Database | Concepts and Combinations | ||||
|---|---|---|---|---|---|
| Sedation | Palliative Care | Prospective | |||
| PubMed | Sedation (Title) | AND | Palliative care (MeSH) | AND | Prospective (MeSH) |
| Medline (WoS) | Sedation (Title) | AND | Palliative care (MeSH) | AND | “Prospective studies” (topic) |
| Embase | “Palliative sedation” (Title) | AND | “Palliative care” (Abstract) | AND | Prospective (All files) |
| Cinahl | Sedation (Title) | AND | “Palliative care” (Abstract) | AND | Prospective (abstract) |
| Cochrane Library | Sedation (Title, abstract, key word) | AND | “Palliative care” (Title, abstract, key word) | AND | Prospective |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belar, A.; Arantzamendi, M.; Menten, J.; Payne, S.; Hasselaar, J.; Centeno, C. The Decision-Making Process for Palliative Sedation for Patients with Advanced Cancer–Analysis from a Systematic Review of Prospective Studies. Cancers 2022, 14, 301. https://doi.org/10.3390/cancers14020301
Belar A, Arantzamendi M, Menten J, Payne S, Hasselaar J, Centeno C. The Decision-Making Process for Palliative Sedation for Patients with Advanced Cancer–Analysis from a Systematic Review of Prospective Studies. Cancers. 2022; 14(2):301. https://doi.org/10.3390/cancers14020301
Chicago/Turabian StyleBelar, Alazne, Maria Arantzamendi, Johan Menten, Sheila Payne, Jeroen Hasselaar, and Carlos Centeno. 2022. "The Decision-Making Process for Palliative Sedation for Patients with Advanced Cancer–Analysis from a Systematic Review of Prospective Studies" Cancers 14, no. 2: 301. https://doi.org/10.3390/cancers14020301
APA StyleBelar, A., Arantzamendi, M., Menten, J., Payne, S., Hasselaar, J., & Centeno, C. (2022). The Decision-Making Process for Palliative Sedation for Patients with Advanced Cancer–Analysis from a Systematic Review of Prospective Studies. Cancers, 14(2), 301. https://doi.org/10.3390/cancers14020301