
Socio-Economic Inequalities in Lung Cancer Outcomes: An Overview of Systematic Reviews
 ,
,  , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
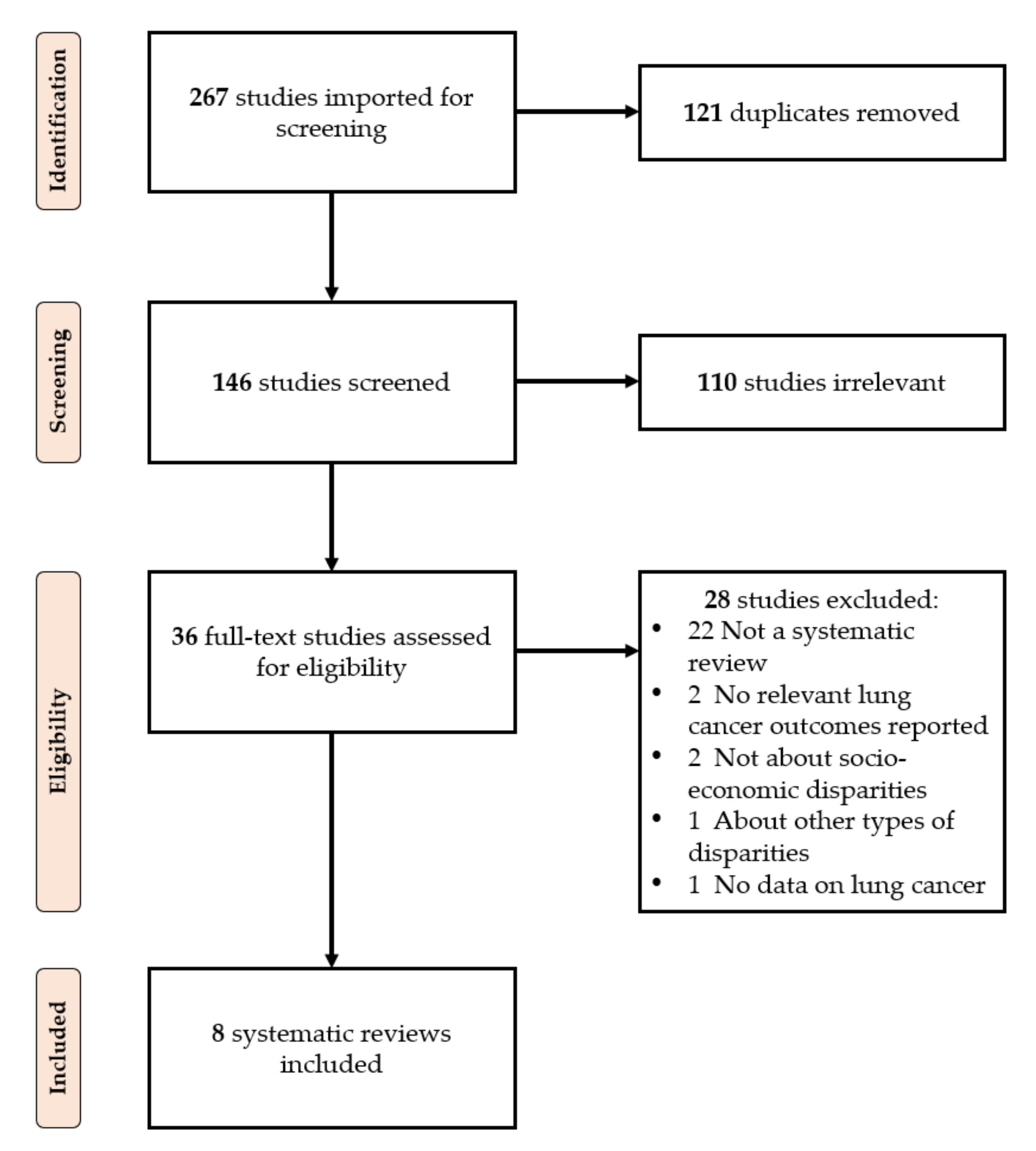
2. Materials and Methods
3. Results
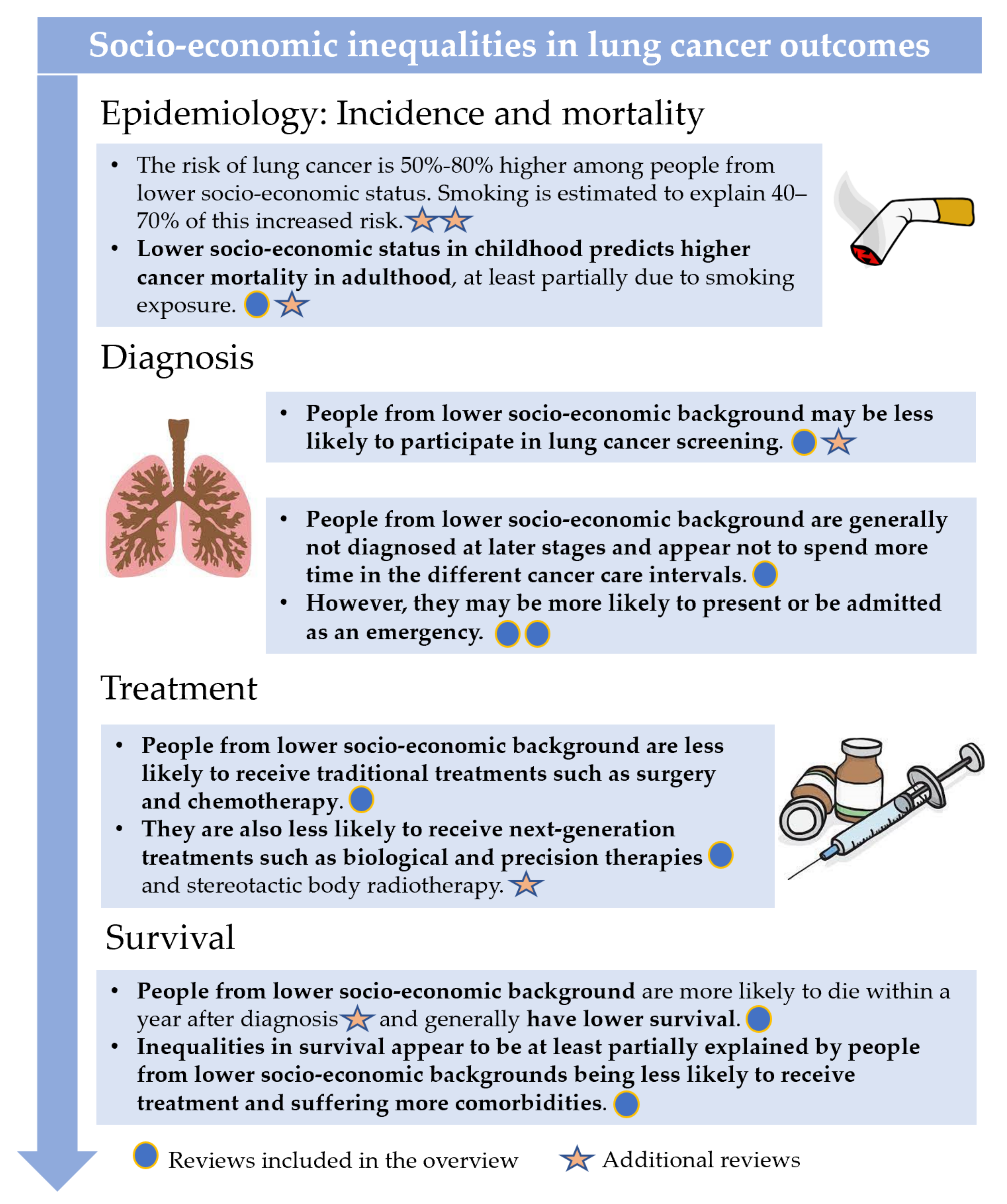
3.1. Incidence and Mortality
3.2. Diagnosis-Related Outcomes
3.3. Treatment-Related Outcomes
3.4. Survival
4. Discussion

5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37,513,025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Francisci, S.; Minicozzi, P.; Pierannunzio, D.; Ardanaz, E.; Eberle, A.; Grimsrud, T.K.; Knijn, A.; Pastorino, U.; Salmerón, D.; Trama, A.; et al. Survival patterns in lung and pleural cancer in Europe 1999–2007: Results from the EUROCARE-5 study. Eur. J. Cancer 2015, 51, 2242–2253. [Google Scholar] [CrossRef]
- Woods, L.; Rachet, B.; Coleman, M. Origins of socio-economic inequalities in cancer survival: A review. Ann. Oncol. 2005, 17, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Quaglia, A.; Lillini, R.; Mamo, C.; Ivaldi, E.; Vercelli, M. Socio-economic inequalities: A review of methodological issues and the relationships with cancer survival. Crit. Rev. Oncol. 2013, 85, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Afshar, N.; English, D.R.; Milne, R.L. Factors Explaining Socio-Economic Inequalities in Cancer Survival: A Systematic Review. Cancer Control 2021, 28, 10732748211011956. [Google Scholar] [CrossRef]
- Landrine, H.; Corral, I.; Lee, J.G.; Efird, J.T.; Hall, M.B.; Bess, J.J. Residential segregation and racial cancer disparities: A systematic review. J. Racial Ethn. Health Disparities 2017, 4, 1195–1205. [Google Scholar] [CrossRef]
- Afshar, N.; English, D.R.; Milne, R.L. Rural–urban residence and cancer survival in high-income countries: A systematic review. Cancer 2019, 125, 2172–2184. [Google Scholar] [CrossRef] [Green Version]
- Mihor, A.; Tomsic, S.; Zagar, T.; Lokar, K.; Zadnik, V. Socioeconomic inequalities in cancer incidence in Europe: A comprehensive review of population-based epidemiological studies. Radiol. Oncol. 2020, 54, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Forrest, L.F.; Adams, J.; Wareham, H.; Rubin, G.; White, M. Socioeconomic inequalities in lung cancer treatment: Systematic review and meta-analysis. PLoS Med. 2013, 10, e1001376. [Google Scholar] [CrossRef] [Green Version]
- Finke, I.; Behrens, G.; Weisser, L.; Brenner, H.; Jansen, L. Socioeconomic differences and lung cancer Survival—Systematic review and meta-analysis. Front. Oncol. 2018, 8, 536. [Google Scholar] [CrossRef] [PubMed]
- Chouaïd, C.; Goussault, H.; Gendarme, S.; Assié, J.B.; Bylicki, O. Factors Associated with Early Lung Cancer Mortality: A Systematic Review. Expert Rev. Anticancer Ther. 2021. accepted. [Google Scholar]
- Ching-López, A.; Luque-Fernandez, M.A.; Sánchez, M.J. Social Disparities in Survival from Lung Cancer in Europe. In Social Environment and Cancer in Europe; Springer: Cham, Switzerland, 2021; pp. 121–140. [Google Scholar]
- Sidorchuk, A.; Agardh, E.E.; Aremu, O.; Hallqvist, J.; Allebeck, P.; Moradi, T. Socioeconomic differences in lung cancer incidence: A systematic review and meta-analysis. Cancer Causes Control 2009, 20, 459–471. [Google Scholar] [CrossRef]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non–small cell lung cancer: Epidemiology, screening, diagnosis, and treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef]
- Castro, S.; Sosa, E.; Lozano, V.; Akhtar, A.; Love, K.; Duffels, J.; Raz, D.J.; Kim, J.Y.; Sun, V.; Erhunmwunsee, L. The impact of income and education on lung cancer screening utilization, eligibility, and outcomes: A narrative review of socioeconomic disparities in lung cancer screening. J. Thorac. Dis. 2021, 13, 3745. [Google Scholar] [CrossRef]
- Sosa, E.; D’Souza, G.; Akhtar, A.; Sur, M.; Love, K.; Duffels, J.; Raz, D.J.; Kim, J.Y.; Sun, V.; Erhunmwunsee, L. Racial and socioeconomic disparities in lung cancer screening in the United States: A systematic review. CA A Cancer J. Clin. 2021, 71, 299–314. [Google Scholar] [CrossRef]
- Lin, Y.; Mak, K.S. Racial and socioeconomic disparities in the use of stereotactic body radiotherapy for treating non-small cell lung cancer: A narrative review. J. Thorac. Dis. 2021, 13, 3764. [Google Scholar] [CrossRef]
- Norris, R.P.; Dew, R.; Sharp, L.; Greystoke, A.; Rice, S.; Johnell, K.; Todd, A. Are there socio-economic inequalities in utilization of predictive biomarker tests and biological and precision therapies for cancer? A systematic review and meta-analysis. BMC Med. 2020, 18, 282. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid.-Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Fusar-Poli, P.; Radua, J. Ten simple rules for conducting umbrella reviews. Evid.-Based Ment. Health 2018, 21, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollock, M.; Fernandes, R.M.; Becker, L.A.; Featherstone, R.; Hartling, L. What guidance is available for researchers conducting overviews of reviews of healthcare interventions? A scoping review and qualitative metasummary. Syst. Rev. 2016, 5, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollock, M.; Fernandes, R.M.; Becker, L.A.; Pieper, D.; Hartling, L. Chapter V: Overviews of reviews. Cochrane Handb. Syst. Rev. Interv. Version 2018, 6. Available online: https://training.cochrane.org/handbook/current/chapter-v (accessed on 20 December 2021).
- Pollock, M.; Fernandes, R.M.; Pieper, D.; Tricco, A.C.; Gates, M.; Gates, A.; Hartling, L. Preferred Reporting Items for Overviews of Reviews (PRIOR): A protocol for development of a reporting guideline for overviews of reviews of healthcare interventions. Syst. Rev. 2019, 8, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bougioukas, K.I.; Liakos, A.; Tsapas, A.; Ntzani, E.; Haidich, A. Preferred reporting items for overviews of systematic reviews including harms checklist: A pilot tool to be used for balanced reporting of benefits and harms. J. Clin. Epidemiol. 2018, 93, 9–24. [Google Scholar] [CrossRef]
- Martinic, M.K.; Pieper, D.; Glatt, A.; Puljak, L. Definition of a systematic review used in overviews of systematic reviews, meta-epidemiological studies and textbooks. BMC Med. Res. Methodol. 2019, 19, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
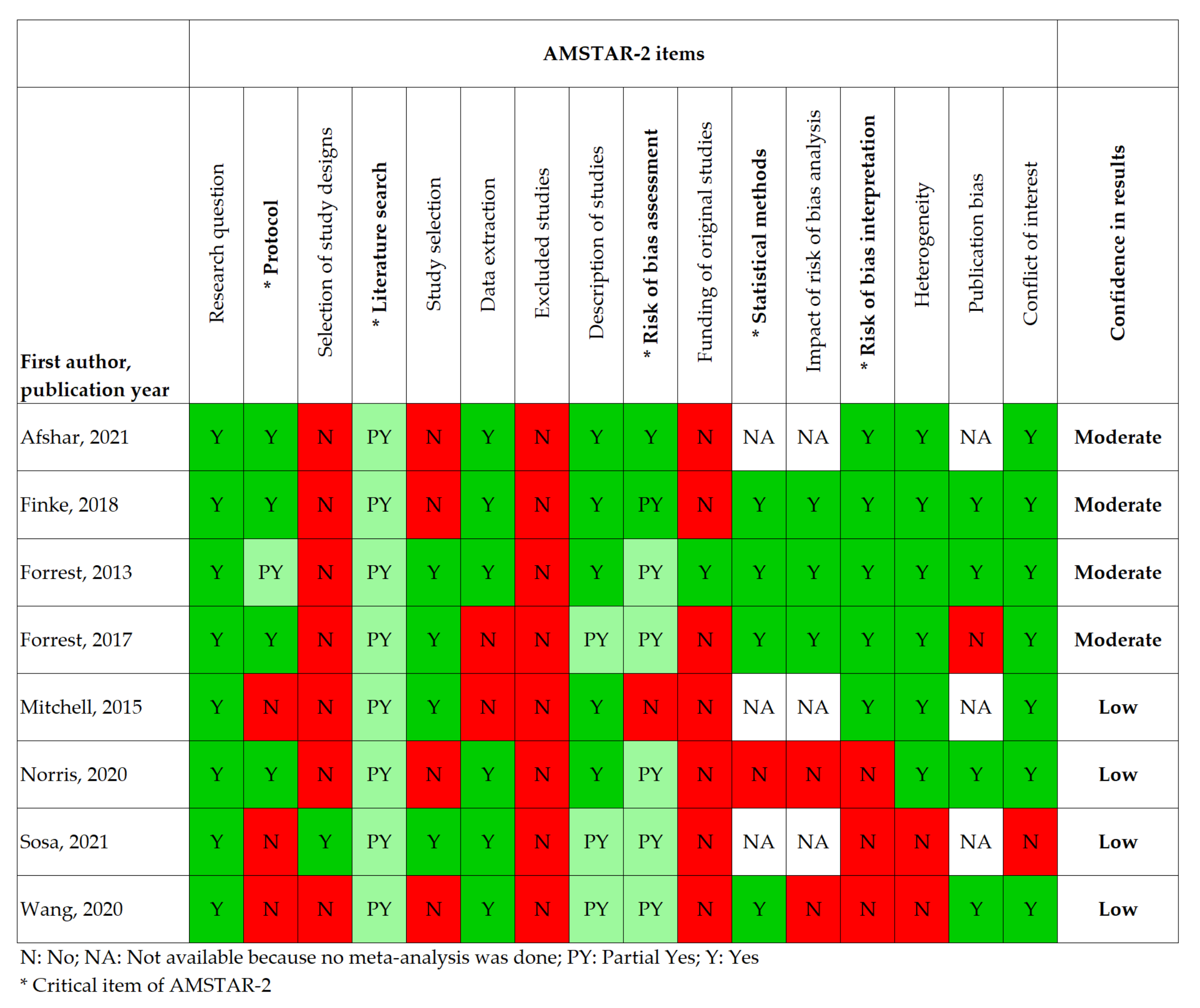
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; Li, C.; Huo, Z.; Ge, F.; Zhong, R.; Jiang, Y.; Wen, Y.; Su, Z.; Liang, H.; Cheng, B.; et al. Family Socioeconomic Position and Lung Cancer Risk: A Meta-analysis and a Mendelian Randomization Study. 2020. Available online: https://www.researchsquare.com/article/rs-89906/v1 (accessed on 20 December 2021). [CrossRef]
- Moyer, V.A. Screening for lung cancer: US Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2014, 160, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Kubik, M.; et al. Screening for lung cancer: US preventive services task force recommendation statement. JAMA 2021, 325, 962–970. [Google Scholar]
- Forrest, L.F.; Sowden, S.; Rubin, G.; White, M.; Adams, J. Socio-economic inequalities in stage at diagnosis, and in time intervals on the lung cancer pathway from first symptom to treatment: Systematic review and meta-analysis. Thorax 2017, 72, 430–436. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, E.D.; Pickwell-Smith, B.; Macleod, U. Risk factors for emergency presentation with lung and colorectal cancers: A systematic review. BMJ Open 2015, 5, e006965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiscock, R.; Bauld, L.; Amos, A.; Fidler, J.A.; Munafò, M. Socioeconomic status and smoking: A review. Ann. N. Y. Acad. Sci. 2012, 1248, 107–123. [Google Scholar] [CrossRef]
- Vohra, J.; Marmot, M.G.; Bauld, L.; Hiatt, R.A. Socioeconomic position in childhood and cancer in adulthood: A rapid-review. J. Epidemiol. Community Health 2016, 70, 629–634. [Google Scholar] [CrossRef]
- Weller, D.; Vedsted, P.; Rubin, G.; Walter, F.M.; Emery, J.; Scott, S.; Campbell, C.; Andersen, R.S.; Hamilton, W.; Olesen, F.; et al. The Aarhus statement: Improving design and reporting of studies on early cancer diagnosis. Br. J. Cancer 2012, 106, 1262. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.; Tammemagi, M. Contemporary issues in the implementation of lung cancer screening. Eur. Respir. Rev. 2021, 30, 200288. [Google Scholar] [CrossRef]
- National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [Green Version]
- De Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.W.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- Schütte, S.; Dietrich, D.; Montet, X.; Flahault, A. Participation in lung cancer screening programs: Are there gender and social differences? A systematic review. Public Health Rev. 2018, 39, 23. [Google Scholar] [CrossRef] [PubMed]
- Haddad, D.N.; Sandler, K.L.; Henderson, L.M.; Rivera, M.P.; Aldrich, M.C. Disparities in lung cancer screening: A review. Ann. Am. Thorac. Soc. 2020, 17, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Vaughan, J.P.; Barros, F.C.; Silva, A.C.; Tomasi, E. Explaining trends in inequities: Evidence from Brazilian child health studies. Lancet 2000, 356, 1093–1098. [Google Scholar] [CrossRef]
- Huey, R.W.; Hawk, E.; Offodile, A.C. Mind the gap: Precision oncology and its potential to widen disparities. J. Oncol. Pract. 2019, 15, 301–304. [Google Scholar] [CrossRef]
- Petrova, D.; Borrás, J.M.; Pollán, M.; Bayo Lozano, E.; Vicente, D.; Jiménez Moleón, J.J.; Sánchez, M.J. Public Perceptions of the Role of Lifestyle Factors in Cancer Development: Results from the Spanish Onco-Barometer 2020. Int. J. Environ. Res. Public Health 2021, 18, 10472. [Google Scholar] [CrossRef]
- Albreht, T.; Molina-Barceló, A. Social Inequalities in Cancer: The Policies of the European Commission. In Social Environment and Cancer in Europe; Springer: Cham, Switzerland, 2021; pp. 309–317. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| First Author and Pub. Year | Measure(s) of SES | Lung Cancer Outcome(s) | Search Period | Number of Original Studies Included (k) | Geographical Representation of the Included Studies | Total Number of Participants/Patients | Main Results Regarding the Outcomes of Interest |
|---|---|---|---|---|---|---|---|
| Afshar 2021 | Diverse individual and area-based | Survival (cancer-specific and overall) | 2005–2020 | 7 | UK (k = 3), Denmark (k = 1), Germany (k = 1), Sweden (k = 1), and US (k = 1) | 111,275 | Inequalities in survival appear to be partly explained by receipt of treatment and co-morbidities. Results regarding the mediating role of stage at diagnosis were mixed. No meta-analysis was performed. |
| Finke 2018 | Diverse individual and area-based | Survival | Start–2017 | 94 (23 based on individual measures and 70 on area-based measures, 1 on both levels). 17 included in meta-analysis. | Individual measures: mostly from Scandinavia, US, and Italy; Area-based measures: mostly from US, UK, and Australia/New Zealand | >187,000 in studies with individual measures; >4,250,000 in studies with area-based measures. | Individual measures: There was no effect of education (HR = 1.03 (0.96, 1.10, ref = high education), I2 = 55%, k = 13). Lower income was associated with lower survival (HR = 1.13 (1.08, 1.19), ref = high income), I2 = 0%, k = 7). Occupations associated with lower SES did not show lower survival (k = 3), no meta-analysis. Area-based measures: Education (k = 3), income (k = 19), SES-index (k = 22). No meta-analyses could be conducted overall but results were generally consistent with lower survival among patients residing in lower SES areas. Comparison: The range of differences between survival rates for lowest and highest SES groups was larger in studies considering area-based SES than in studies assessing individual SES (Individual SES: range 1.0–12.8% units; area-based SES: range 0.9–22.9% units) but did not depend on the SES measure or the population size of the area. |
| Forrest 2013 | Diverse individual and area-based | Receipt of treatment (surgery, chemotherapy, radiotherapy, unspecified treatment) | start–2012 | 46 (1 based on an individual measure and 45 on area-based measures of SES) | US (k = 18), UK (k = 19), Canada (k = 2), Sweden (k = 1), Australia (k = 1), Italy (k = 1), France (k = 1), and New Zealand (k = 3) | Surgery: >656,000 Chemotherapy: >359,000 Radiotherapy: >235,000 Unspecified treatment: >115,000 | Overall: Lower SES was associated with lower likelihood of receiving treatment: OR = 0.79 [95% CI 0.73 to 0.86], p < 0.001, I2 = 77%, k = 26. Surgery: Patients of lower SES were less likely to undergo surgery: OR = 0.72 (95% CI 0.65 to 0.80), p < 0.001, I2 = 80%, k = 16 (also when controlling for histology and stage at diagnosis). Chemotherapy: Patients with lower SES were less likely to undergo chemotherapy, OR = 0.81 (95% CI 0.73 to 0.89), p < 0.001, I2 = 68%, k = 10. Radiotherapy: There was no association of SES with the receipt of radiotherapy, OR = 0.99 [95% CI 0.86 to 1.14], p = 0.89, I2 = 54%, k = 7. Unspecified treatment type: Patients with lower SES were less likely to receive treatment, OR = 0.78 [95% CI 0.74 to 0.83], p < 0.001, I2 = 0, k = 5. |
| Forrest 2017 | Diverse individual and area-based | Stage (at diagnosis or start of treatment); duration of time intervals on the lung cancer pathway | start–2016 | 39 (23 for stage, 12 for intervals, and 8 for proxy measures of delay) | UK (k = 20), US (k = 10), Canada (k = 2), Denmark (k = 2), Sweden (k = 1), Australia (k = 1), Italy (k = 1), Korea (k = 1), and New Zealand (k = 1). | >267,500 for stage, >79,700 for intervals, >569,100 for proxy measures | Stage: There was no evidence of socio-economic inequalities in late stage at diagnosis in the most, compared with the least, deprived groups (OR = 1.04, 95% CI = 0.92 to 1.19, I2 = 60%, k = 7). Studies that were not suitable for meta-analysis (k = 16) showed the same pattern of results. Intervals: 12 studies examined 8 intervals from the cancer care pathway (e.g., patient interval, GP referral interval, diagnostic interval, etc.). There was no evidence of socio-economic inequalities. No meta-analysis was performed. Proxy measures of delay: These included acute presentation, emergency admission, number of times to consult and diagnosis at death (k = 8). More deprived patients were more likely to present and to be admitted as an emergency, but socio-economic inequalities were not found in the number of times to consult or in diagnosis at death. |
| Mitchell 2015 | Diverse individual and area-based | Emergency presentation: a diagnosis of cancer that arose during an unscheduled (or emergency or unplanned) hospital admission. | 1996–2014 | 4 | UK (k = 3), US (k = 1) | 163,050 | Higher socio-economic deprivation (as measured by area-based indices) increased the likelihood of emergency presentation in all 3 studies identified. There was no association between annual household income and emergency presentation in the one study identified. No meta-analysis was conducted. |
| Norris 2020 | Diverse individual and area-based (the large majority area-based) | Utilization of predictive biomarker tests and biological and precision therapies | 1998–2019 | 11 (2 on predictive biomarkers and 9 on biological and precision therapies) | US (k = 11) | 505,105 (15,588 for biomarker tests and 534,517 for therapy) | Predictive biomarkers: There was no relationship between SES and utilization of predictive biomarker tests (epidermal growth factor receptor and/or anapestic lymphoma kinase): OR = 0.92 (95% CI 0.35, 2.40), I2 = 97%, k = 2 (the two studies found relationships in the opposite direction). Biological and precision therapies: Lower SES was related to lower utilization of these therapies, OR = 0.71 (95% CI 0.51, 1.00), I2 = 95%, k = 6 (low compared to high SES). |
| Sosa 2021 | Individual income and education | Screening eligibility; screening completion/intention; late stage diagnosis; lung cancer-specific mortality | 2010–2020 | 6 | US (k = 6) | 163,418 | Screening eligibility: There was evidence that higher household income was associated with greater screening eligibility (k = 1) but results regarding education were mixed (k = 2). Screening completion/intentions: There was some evidence that patients with lower income were less likely to complete screening or have the intention to be screened (found in k = 2 out of k = 3). Stage: There was no difference in stage at diagnosis as a function of SES (k = 1). Mortality: High risk smokers with higher education had lower cancer-specific mortality (k = 1). |
| Wang 2020 | Childhood SES based on education level, socio-economic position of parents, and/or childhood housing conditions | Lung cancer-specific mortality | Start–2020 | 13 (8 in meta-analysis, 7 in dose–response analysis) | UK (k = 9), Norway (k = 3), Netherlands (k = 1) | 2,779,242 | Lower childhood SES was associated with higher lung cancer mortality, HR = 1.25 (95% CI, 1.10, 1.43), I2 = 49%, p = 0.04, k = unclear (from adjusted analysis). There was also a dose–response relationship. |
| First Author and Pub. Year | Are Results and Conclusions Based on Adjusted Analysis in Original Studies? | Instrument Used to Assess the Methodological Quality of Original Studies | Overall Methodological Quality of Included Studies | Main Limitations of the Review | |
|---|---|---|---|---|---|
| Afshar 2021 | Yes | Studies adjusted for a variable combination of some of the following variables: Sex, age, stage, smoking, histopathology, treatment, comorbidity, performance status. | ROBINS-E (Risk of Bias in Non-Randomized Studies of Exposures) tool assessing confounding, selection of participants into the study, classification of the exposure, adjustment for mediators, level of missing data, measurement of the outcome, and reporting of results. | 68 of 74 articles had critical risk of bias, the majority due to inappropriate adjustment. | Large between-study heterogeneity in the measures of SES and the methods used to identify the underlying causes of socio-economic inequalities. Frequent use of overall survival as outcome (instead of cancer-specific, which would be more useful for studying potential mediators in the context of lung cancer and considering competing risk of death). |
| Finke 2018 | Yes | The majority of studies adjusted for age, gender, and stage. Some but not all studies also for smoking and treatment. Overall, adjustment was variable. Whenever possible, subgroup analyses were performed by adjustment for smoking status, stage, and treatment. | A modified version of the Newcastle-Ottawa-Scale (NOS) that assesses the quality of a study regarding the selection and comparability of study groups and ascertainment of the outcome (cohort studies) or exposure (case–control studies) | Mean quality scores of both individual and area-based studies were overall high, between 7 and 8 out of 8 possible points. The majority of studies used data from cancer registries, and hence many studies scored high on selection and outcome, adequacy of follow-up or representativeness of study population. | Studies were very heterogeneous, not only in the use of socioeconomic measures and aggregated levels but also in reporting of survival measures and in the level of adjustment. The generalizability of results to low-income countries is limited. No meta-analysis stratified by gender or subtype of lung cancer was possible. |
| Forrest 2013 | Yes | The majority of studies adjusted for age, sex, and histology. However, it was variable and the ORs used in the meta-analyses were not consistently adjusted for the same covariates. | A study quality tool, adapted from existing quality tools (SIGN 50 and STROBE) that assessed population representativeness, internal validity, external validity, study reporting, confounding, and analysis (uni- or multi-variable). | Quality was variable but only studies conducting multivariable analysis (with high quality scores) were included in the meta-analysis. | Only one study measured SES on the individual level. Not all studies reported details of stage and histology—both of which influence treatment type—and some studies did not take comorbidity into account. The possibility for publication bias could not be excluded. |
| Forrest 2017 | Partially | Stage: Only studies conducting multivariable analysis were included in the meta-analysis. However, the ORs used in the meta-analyses were not consistently adjusted for the same covariates. Other outcomes without meta-analysis: the presence of adjustment was variable. | A quality checklist adapted from Forrest et al., 2013 and the Aarhus checklist assessing validity and reliability of the outcome and exposure measures, analysis (adjustment and reporting), and study population. | No information on overall quality is reported. Only studies with sufficient quality were considered for meta-analysis (based on adjusted analysis). | Very few of the studies included in this current review took account of patient health status when examining time intervals. The included studies reported observational data only and use very diverse measures of socio-economic status. The meta-analysis may be underpowered to detect differences between early and late-stage presentation. The ORs used in the meta-analyses were not consistently adjusted for the same covariates. Many of the studies included in the narrative review were not of high quality. Publication bias is a possibility. |
| Mitchell 2015 | Unclear | Nothing is reported in this respect. | Because included studies used methodologies that were often inapplicable to existing instruments, a method for assessing the strength of evidence of observational studies developed in previous systematic reviews was adapted, evaluating population, ascertainment, and analysis. | All studies reporting on SES were classified as “strong” (highest methodological classification). | Few evaluative studies were identified, with most researchers undertaking observational work utilizing routine data. |
| Norris 2020 | No | Unadjusted ORs were used to enable inclusion of as many studies as possible in a consistent way (because not many original studies reported adjusted ORs) | A modified version of the ISPOR checklist for retrospective database studies assessing data sources, statistical results of interest, and generalizability of conclusions drawn. | Quality scores for the lung cancer studies were variable: ranging from 6 to 10 points for the biomarker studies and 6 to 8.5 for the biological and precision therapies (from a maximum of 10). | ORs were determined from raw data unadjusted for confounders. There was large heterogeneity between studies. Title and abstract screening were carried out by a single reviewer. There were only a few studies available, and most were from the US and in older patients. |
| Sosa 2021 | Partially | All but one studies were judged as “adjusting statistically for confounders”; however, it is not specified with confounders. | The National Heart, Lung, and Blood Institute Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies that assesses potential flaws in study methods or implementation that may lead to bias and lower study quality. | Five studies were judged as “good” (best category) and one as “fair” (second best). | Only a small number of studies was available; no gender-related disparities were reviewed; most studies were observational and/or secondary analysis studies; only a qualitative synthesis could be conducted. |
| Wang 2020 | Yes | It is not reported what factors were adjusted for. | A score system based on the Newcastle-Ottawa Scale (NOS) tool assessing representativeness of exposure arm(s), selection of the comparative arm(s), origin of exposure source, demonstration that outcome of interest was not present at start of study, studies controlling the most important factors, studies controlling the other main factors, assessment of outcome with independency, adequacy of follow-up length (to assess outcome), lost to follow-up acceptable (less than 10% and reported). | Quality scores for the studies included in the meta-analysis ranged from 6 to 8 (out of maximum of 9), with 8 being the most frequent value. | The included studies do not cover diverse geographical regions and do not report data from recent years. Analyses based on cancer subtypes could not be conducted. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Redondo-Sánchez, D.; Petrova, D.; Rodríguez-Barranco, M.; Fernández-Navarro, P.; Jiménez-Moleón, J.J.; Sánchez, M.-J. Socio-Economic Inequalities in Lung Cancer Outcomes: An Overview of Systematic Reviews. Cancers 2022, 14, 398. https://doi.org/10.3390/cancers14020398
Redondo-Sánchez D, Petrova D, Rodríguez-Barranco M, Fernández-Navarro P, Jiménez-Moleón JJ, Sánchez M-J. Socio-Economic Inequalities in Lung Cancer Outcomes: An Overview of Systematic Reviews. Cancers. 2022; 14(2):398. https://doi.org/10.3390/cancers14020398
Chicago/Turabian StyleRedondo-Sánchez, Daniel, Dafina Petrova, Miguel Rodríguez-Barranco, Pablo Fernández-Navarro, José Juan Jiménez-Moleón, and Maria-José Sánchez. 2022. "Socio-Economic Inequalities in Lung Cancer Outcomes: An Overview of Systematic Reviews" Cancers 14, no. 2: 398. https://doi.org/10.3390/cancers14020398
APA StyleRedondo-Sánchez, D., Petrova, D., Rodríguez-Barranco, M., Fernández-Navarro, P., Jiménez-Moleón, J. J., & Sánchez, M. -J. (2022). Socio-Economic Inequalities in Lung Cancer Outcomes: An Overview of Systematic Reviews. Cancers, 14(2), 398. https://doi.org/10.3390/cancers14020398