
Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma in the Gastrointestinal Tract in the Modern Era


Abstract
:Simple Summary
Abstract
1. Introduction
2. Clinicopathological Features of GI Lymphomas
2.1. Gastric Lymphomas
2.2. Intestinal Lymphomas
3. Pathogenesis in Relation to Bacterial Infection or Chronic Antigenic Stimulation
4. Molecular Pathology
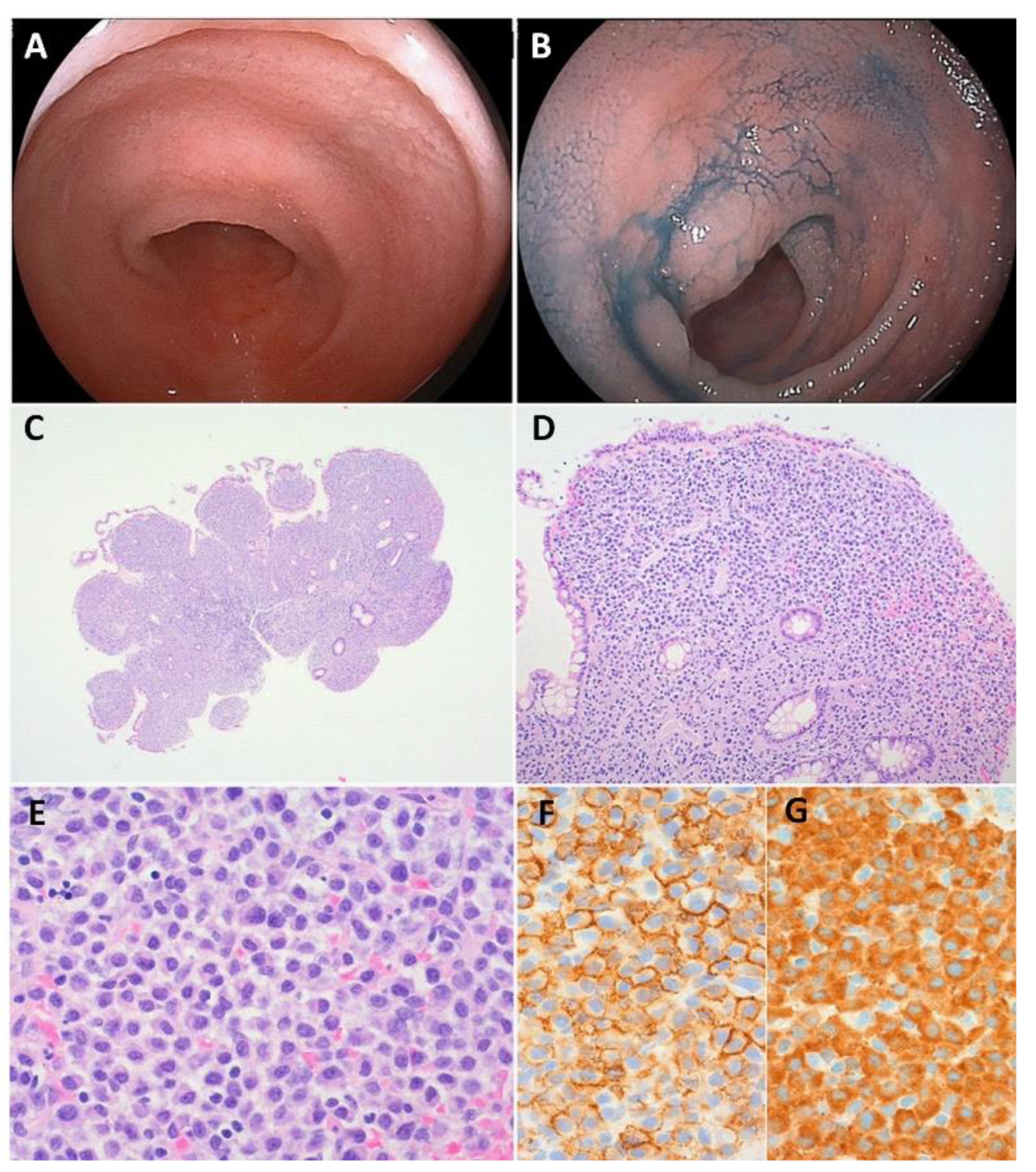
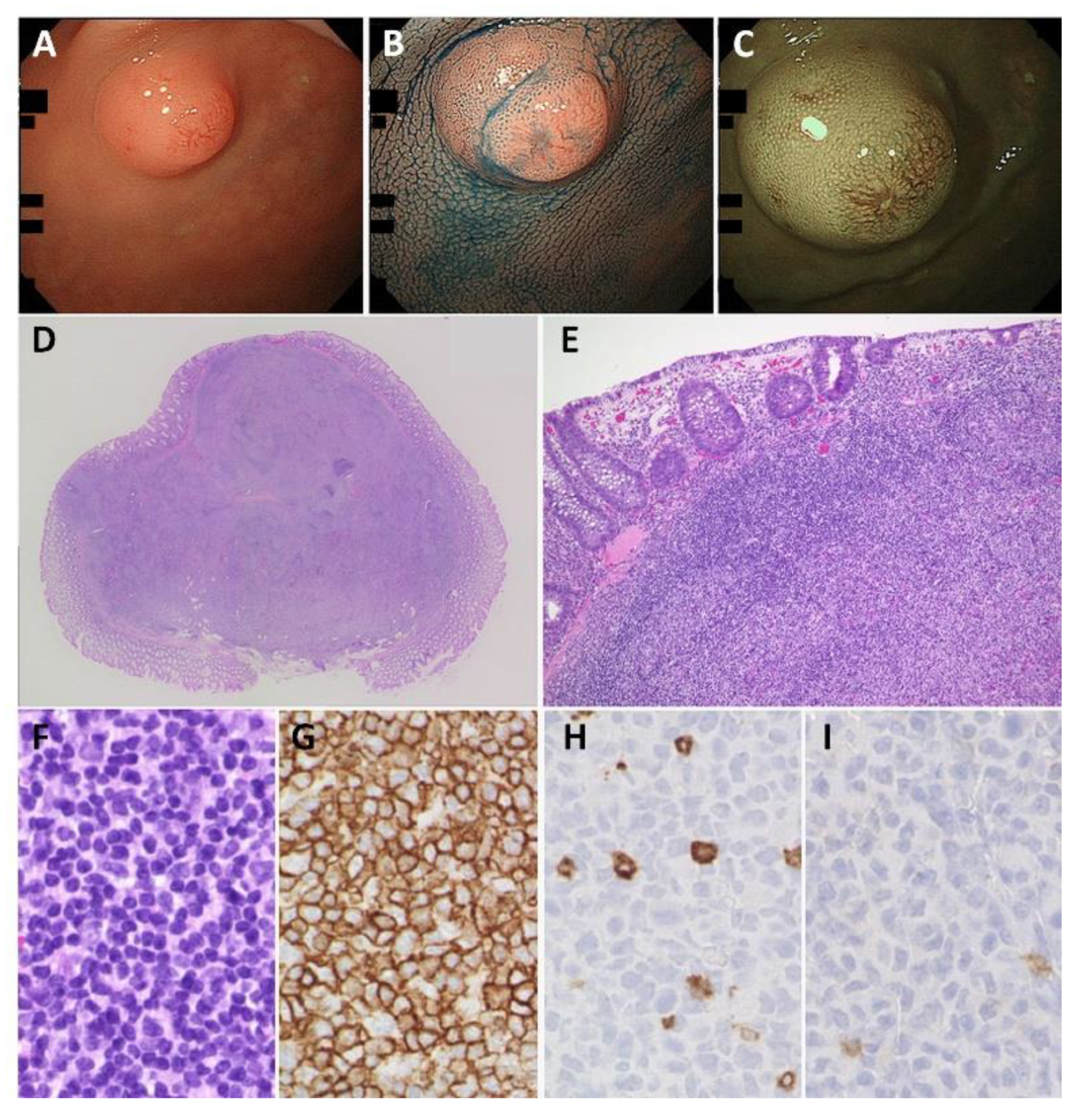
5. Pathological Findings
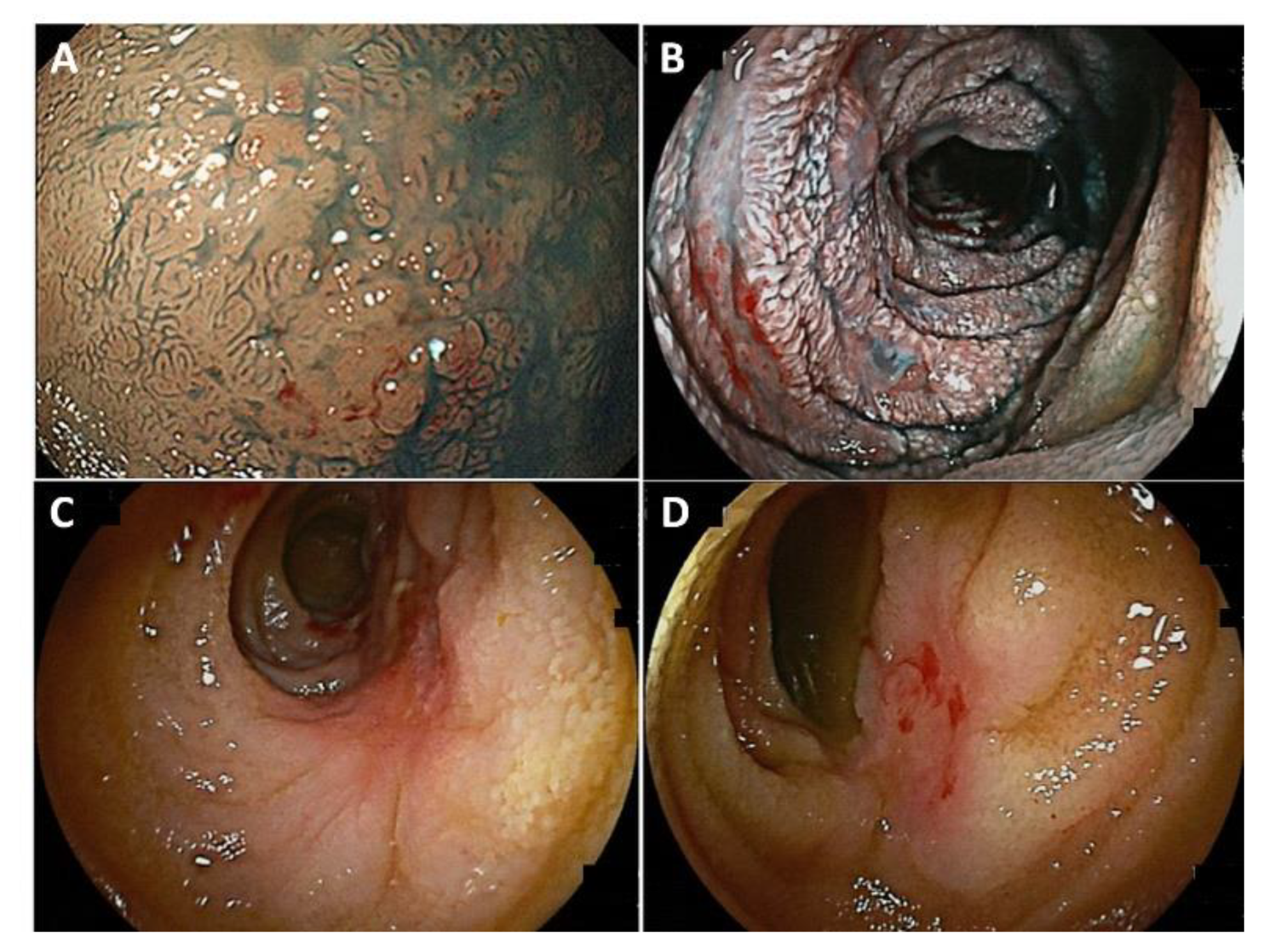
6. Endoscopic Findings
7. Treatment and Clinical Response
7.1. Antibiotic Therapy
7.2. Watch-and-Wait Strategy and Re-Eradication after Eradication Therapy
7.3. Radiotherapy
7.4. Chemo/Immunotherapy
7.5. Endoscopic Resection
7.6. Surgery
7.7. Outcome
8. The Risk of Developing Carcinoma and Other Malignancies
9. Epstein–Barr Virus (EBV)-Negative Post-Transplant EMZL in the GI Tract
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Khalil, M.O.; Morton, L.M.; Devesa, S.S.; Check, D.P.; Curtis, R.E.; Weisenburger, D.D.; Dores, G.M. Incidence of marginal zone lymphoma in the United States, 2001-2009 with a focus on primary anatomic site. Br. J. Haematol. 2014, 165, 67–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wotherspoon, A.C.; Doglioni, C.; Diss, T.C.; Pan, L.X.; Moschini, A.; Deboni, M.; Isaacson, P.G. Regression of primary low-grade b-cell gastric lymphoma of mucosa-associated lymphoid-tissue type after eradication of helicobacter-pylori. Lancet 1993, 342, 575–577. [Google Scholar] [CrossRef]
- Chanudet, E.; Zhou, Y.; Bacon, C.M.; Wotherspoon, A.C.; Müller-Hermelink, H.K.; Adam, P.; Dong, H.Y.; de Jong, D.; Li, Y.; Wei, R.; et al. Chlamydia psittaci is variably associated with ocular adnexal MALT lymphoma in different geographical regions. J. Pathol. 2006, 209, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Carugi, A.; Onnis, A.; Antonicelli, G.; Rossi, B.; Mannucci, S.; Luzzi, A.; Lazzi, S.; Bellan, C.; Tosi, G.M.; Sayed, S.; et al. Geographic variation and environmental conditions as cofactors in Chlamydia psittaci association with ocular adnexal lymphomas: A comparison between Italian and African samples. Hematol. Oncol. 2010, 28, 20–26. [Google Scholar]
- Zucca, E.; Bertoni, F. The spectrum of MALT lymphoma at different sites: Biological and therapeutic relevance. Blood 2016, 127, 2082–2092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teckie, S.; Qi, S.; Chelius, M.; Lovie, S.; Hsu, M.; Noy, A.; Portlock, C.; Yahalom, J. Long-term outcome of 487 patients with early-stage extra-nodal marginal zone lymphoma. Ann. Oncol. 2017, 28, 1064–1069. [Google Scholar] [CrossRef]
- Nakamura, S.; Sugiyama, T.; Matsumoto, T.; Iijima, K.; Ono, S.; Tajika, M.; Tari, A.; Kitadai, Y.; Matsumoto, H.; Nagaya, T.; et al. Long-term clinical outcome of gastric MALT lymphoma after eradication of Helicobacter pylori: A multicentre cohort follow-up study of 420 patients in Japan. Gut 2012, 61, 507–513. [Google Scholar] [CrossRef]
- Gong, E.J.; Ahn, J.Y.; Jung, H.Y.; Park, H.; Ko, Y.B.; Na, H.K.; Jung, K.W.; Kim, D.H.; Lee, J.H.; Choi, K.D.; et al. Helicobacter pylori Eradication Therapy Is Effective as the Initial Treatment for Patients with H. pylori-Negative and Disseminated Gastric Mucosa-Associated Lymphoid Tissue Lymphoma. Gut Liver 2016, 10, 706–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matysiak-Budnik, T.; Jamet, P.; Ruskon-Fourmestraux, A.; de Mascarel, A.; Velten, M.; Maynadi, M.; Woronoff, A.S.; Trtarre, B.; Marrer, E.; Delafosse, P.; et al. Gastric MALT lymphoma in a population-based study in France: Clinical features, treatments and survival. Aliment. Pharmacol. Ther. 2019, 50, 654–663. [Google Scholar] [CrossRef]
- Kiesewetter, B.; Copie-Bergman, C.; Levy, M.; Wu, F.T.; Dupuis, J.; Barau, C.; Arcaini, L.; Paulli, M.; Lucioni, M.; Bonometti, A.; et al. Genetic Characterization and Clinical Features of Helicobacter pylori Negative Gastric Mucosa-Associated Lymphoid Tissue Lymphoma. Cancers 2021, 13, 2993. [Google Scholar] [CrossRef]
- Lecuit, M.; Abachin, E.; Martin, A.; Poyart, C.; Pochart, P.; Suarez, F.; Bengoufa, D.; Feuillard, J.; Lavergne, A.; Gordon, J.I.; et al. Immunoproliferative small intestinal disease associated with Campylobacter jejuni. N. Engl. J. Med. 2004, 350, 239–248. [Google Scholar] [CrossRef]
- Bianchi, G.; Sohani, A.R. Heavy Chain Disease of the Small Bowel. Curr. Gastroenterol. Rep. 2018, 20, 3. [Google Scholar] [CrossRef] [PubMed]
- Galera, P.; Flavin, R.; Savage, N.M.; Saksena, A.; Gong, S.; Wang, H.Y.; Swan, N.; Xi, L.; Raffeld, M.; Pittaluga, S.; et al. Epstein-Barr Virus-negative Marginal Zone Lymphoma as an Uncommon Form of Monomorphic Posttransplant Lymphoproliferative Disorder. Am. J. Surg. Pathol. 2020, 44, 1340–1352. [Google Scholar] [CrossRef]
- Nakamura, S.; Matsumoto, T.; Iida, M.; Yao, T.; Tsuneyoshi, M. Primary gastrointestinal lymphoma in Japan: A clinicopathologic analysis of 455 patients with special reference to its time trends. Cancer 2003, 97, 2462–2473. [Google Scholar] [CrossRef] [PubMed]
- Capelle, L.G.; de Vries, A.C.; Looman, C.W.N.; Casparie, M.K.; Boot, H.; Meijer, G.A.; Kuipers, E.J. Gastric MALT lymphoma: Epidemiology and high adenocarcinoma risk in a nation-wide study. Eur. J. Cancer 2008, 44, 2470–2476. [Google Scholar] [CrossRef]
- Luminari, S.; Cesaretti, M.; Marcheselli, L.; Rashid, I.; Madrigali, S.; Maiorana, A.; Federico, M. Decreasing incidence of gastric MALT lymphomas in the era of anti-Helicobacter pylori interventions: Results from a population-based study on extranodal marginal zone lymphomas. Ann. Oncol. 2010, 21, 855–859. [Google Scholar] [CrossRef]
- Mendes LS, T.; Attygalle, A.D.; Wotherspoon, A.C. Helicobacter pylori infection in gastric extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT) lymphoma: A re-evaluation. Gut 2014, 63, 1526–1527. [Google Scholar] [CrossRef]
- Raderer, M.; Wöhrer, S.; Streubel, B.; Troch, M.; Turetschek, K.; Jäger, U.; Skrabs, C.; Gaiger, A.; Drach, J.; Puespoek, A.; et al. Assessment of disease dissemination in gastric compared with extragastric mucosa-associated lymphoid tissue lymphoma using extensive staging: A single-center experience. J. Clin. Oncol. 2006, 24, 3136–3141. [Google Scholar] [CrossRef]
- Kiesewetter, B.; Simonitsch-Klupp, I.; Dolak, W.; Mayerhoefer, M.E.; Raderer, M. Depth of Remission Following First-Line Treatment Is an Independent Prognostic Marker for Progression-Free Survival in Gastric Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma. Cancers 2020, 12, 492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takigawa, H.; Yuge, R.; Masaki, S.; Otani, R.; Kadota, H.; Naito, T.; Hayashi, R.; Urabe, Y.; Oka, S.; Tanaka, S.; et al. Involvement of non-Helicobacter pylori helicobacter infections in Helicobacter pylori-negative gastric MALT lymphoma pathogenesis and efficacy of eradication therapy. Gastric Cancer 2021, 24, 937–945. [Google Scholar] [CrossRef]
- Kuo, S.H.; Yeh, K.H.; Wu, M.S.; Lin, C.W.; Wei, M.F.; Liou, J.M.; Wang, H.P.; Chen, L.T.; Cheng, A.L. First-line antibiotic therapy in Helicobacter pylori-negative low-grade gastric mucosa-associated lymphoid tissue lymphoma. Sci. Rep. 2017, 7, 14333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moleiro, J.; Ferreira, S.; Lage, P.; Dias Pereira, A. Gastric malt lymphoma: Analysis of a series of consecutive patients over 20 years. United Eur. Gastroenterol. J. 2016, 4, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Raderer, M.; Wöhrer, S.; Kiesewetter, B.; Dolak, W.; Lagler, H.; Wotherspoon, A.; Muellauer, L.; Chott, A. Antibiotic treatment as sole management of Helicobacter pylori-negative gastric MALT lymphoma: A single center experience with prolonged follow-up. Ann. Hematol. 2015, 94, 969–973. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Kim, N.; Paik, J.H.; Kim, J.M.; Lee, S.H.; Park, Y.S.; Hwang, J.H.; Kim, J.W.; Jeong, S.H.; Lee, D.H.; et al. Characteristics of Helicobacter pylori-positive and Helicobacter pylori-negative gastric mucosa-associated lymphoid tissue lymphoma and their influence on clinical outcome. Helicobacter 2013, 18, 197–205. [Google Scholar] [CrossRef]
- Asano, N.; Iijima, K.; Terai, S.; Jin, X.; Ara, N.; Chiba, T.; Fushiya, J.; Koike, T.; Imatani, A.; Shimosegawa, T. Eradication therapy is effective for Helicobacter pylori-negative gastric mucosa-associated lymphoid tissue lymphoma. Tohoku. J. Exp. Med. 2012, 228, 223–227. [Google Scholar] [CrossRef] [Green Version]
- Ono, S.; Kato, M.; Takagi, K.; Kodaira, J.; Kubota, K.; Matsuno, Y.; Komatsu, Y.; Asaka, M. Long-term treatment of localized gastric marginal zone B-cell mucosa associated lymphoid tissue lymphoma including incidence of metachronous gastric cancer. J. Gastroenterol. Hepatol. 2010, 25, 804–809. [Google Scholar] [CrossRef]
- Stathis, A.; Chini, C.; Bertoni, F.; Proserpio, I.; Capella, C.; Mazzucchelli, L.; Pedrinis, E.; Cavalli, F.; Pinotti, G.; Zucca, E. Long-term outcome following Helicobacter pylori eradication in a retrospective study of 105 patients with localized gastric marginal zone B-cell lymphoma of MALT type. Ann. Oncol. 2009, 20, 1086–1093. [Google Scholar] [CrossRef]
- Ishioka, M.; Hirasawa, T.; Mishima, Y. Latest trends in the incidence of Helicobacter pylori-uninfected gastric mucosa-associated lymphoid tissue lymphoma at the Cancer Institute Hospital, Japan. Int. J. Hematol. 2021, 113, 770–771. [Google Scholar] [CrossRef]
- Hirose, Y.; Kaida, H.; Ishibashi, M.; Uozumi, J.; Arikawa, S.; Kurata, S.; Hayabuchi, N.; Nakahara, K.; Ohshima, K. Comparison Between Endoscopic Macroscopic Classification and F-18 FDG PET Findings in Gastric Mucosa-Associated Lymphoid Tissue Lymphoma Patients. Clin. Nucl. Med. 2012, 37, 152–157. [Google Scholar] [CrossRef]
- Yoneda, K.; Takahashi, H.; Abe, Y.; Inamori, M.; Kato, S.; Uchiyama, T.; Iida, H.; Mawatari, H.; Hosono, K.; Endo, H.; et al. A mucosa-associated lymphoid tissue (MALT) lymphoma of the small intestine that was difficult to diagnose endoscopically. Endoscopy 2010, 42, E175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinkade, Z.; Esan, O.A.; Rosado, F.G.; Craig, M.; Vos, J.A. Ileal mucosa-associated lymphoid tissue lymphoma presenting with small bowel obstruction: A case report. Diagn. Pathol. 2015, 10, 105. [Google Scholar] [CrossRef] [Green Version]
- Nehme, F.; Alderson, J.; Nassif, I. Small Bowel Obstruction Secondary to Ileal Mucosa-Associated Lymphoid Tissue Lymphoma. J. Gastrointest. Cancer 2018, 49, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleem, T.; Al-Mondhiry, H. Immunoproliferative small intestinal disease (IPSID): A model for mature B-cell neoplasms. Blood 2005, 105, 2274–2280. [Google Scholar] [CrossRef]
- Subbiah, A.K.; Das, P.; Bagchi, S.; Shalimar; Agarwal, S.K. Recurrent diarrhoea in a renal transplant recipient: Early immunoproliferative small intestinal disease may be missed if not considered. Nephrology 2017, 22, 265–267. [Google Scholar] [CrossRef] [PubMed]
- Orfanoudaki, E.; Iliadis, A.; Goulis, I.; Xylouri, E.; Voumvouraki, A.; Samonakis, D.N. Immunoproliferative Small Intestinal Disease in a Liver Transplant Recipient: A Case Report and Literature Review. Exp. Clin. Transplant. 2021, 19, 620–623. [Google Scholar] [CrossRef]
- Evangelista-Leite, D.; Affonso Madaloso, B.; Shouta Yamashita, B.; Enrico Aloise, F.; Polito Verdasca, L.; Lopes de Mello, M.; Murata Hayashi, R.; Zimberg Chehter, E. Treating chronic diarrhea: A systematic review on Immunoproliferative Small Intestinal Disease (IPSID). PLoS ONE. 2021, 16, e0253695. [Google Scholar] [CrossRef]
- Ahlawat, S.; Kanber, Y.; Charabaty-Pishvaian, A.; Ozdemirli, M.; Cohen, P.; Benjamin, S.; Haddad, N. Primary mucosa-associated lymphoid tissue (MALT) lymphoma occurring in the rectum: A case report and review of the literature. South Med. J. 2006, 99, 1378–1384. [Google Scholar] [CrossRef] [PubMed]
- Won, J.H.; Kim, S.M.; Kim, J.W.; Park, J.H.; Kim, J.Y. Clinical features, treatment and outcomes of colorectal mucosa-associated lymphoid tissue (MALT) lymphoma: Literature reviews published in English between 1993 and 2017. Cancer Manag. Res. 2019, 11, 8577–8587. [Google Scholar] [CrossRef] [Green Version]
- Kawashima, K.; Katakura, K.; Takahashi, Y.; Asama, H.; Fujiwara, T.; Kumakawa, H.; Ohira, H. Primary rectal mucosa-associated lymphoid tissue lymphoma in a patient with previously identified primary biliary cirrhosis and secondary Sjögren’s syndrome. Clin. J. Gastroenterol. 2016, 9, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Jeon, M.K.; So, H.; Huh, J.; Hwang, H.S.; Hwang, S.W.; Park, S.H.; Yang, D.H.; Choi, K.D.; Ye, B.D.; Myung, S.J.; et al. Endoscopic features and clinical outcomes of colorectal mucosa-associated lymphoid tissue lymphoma. Gastrointest. Endosc. 2018, 87, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Kelley, S.R. Mucosa-associated lymphoid tissue (MALT) variant of primary rectal lymphoma: A review of the English literature. Int. J. Colorectal. Dis. 2017, 32, 295–304. [Google Scholar] [CrossRef]
- Saito, T.; Tamaru, J.; Kishi, H.; Kayao, J.; Kuzuu, Y.; Wakita, H.; Adachi, A.; Itoyama, S.; Mikata, I. Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) arising in the small intestine with monoclonal cryoglobulinemia. Pathol. Int. 2004, 54, 712–718. [Google Scholar] [CrossRef]
- Akasaka, R.; Chiba, T.; Dutta, A.K.; Toya, Y.; Mizutani, T.; Shozushima, T.; Abe, K.; Kamei, M.; Kasugai, S.; Shibata, S.; et al. Colonic mucosa-associated lymphoid tissue lymphoma. Case Rep. Gastroenterol. 2012, 6, 569–575. [Google Scholar] [CrossRef]
- Farinha, P.; Gascoyne, R.D. Molecular pathogenesis of mucosa-associated lymphoid tissue lymphoma. J. Clin. Oncol. 2005, 23, 6370–6378. [Google Scholar] [CrossRef]
- Du, M.Q. MALT lymphoma: A paradigm of NF-κB dysregulation. Semin. Cancer Biol. 2016, 39, 49–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgner, A.; Lehn, N.; Andersen, L.P.; Thiede, C.; Bennedsen, M.; Trebesius, K.; Neubauer, B.; Neubauer, A.; Stolte, M.; Bayerdorffer, E. Helicobacter heilmannii-associated primary gastric low-grade MALT lymphoma: Complete remission after curing the infection. Gastroenterology 2000, 118, 821–828. [Google Scholar] [CrossRef]
- Okiyama, Y.; Matsuzawa, K.; Hidaka, E.; Sano, K.; Akamatsu, T.; Ota, H. Helicobacter heilmannii infection: Clinical, endoscopic and histopathological features in Japanese patients. Pathol. Int. 2005, 55, 398–404. [Google Scholar] [CrossRef]
- Heilmann, K.L.; Borchard, F. Gastritis due to spiral shaped bacteria other than helicobacter-pylori-clinical, histological, and ultrastructural findings. Gut 1991, 32, 137–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, M.; Overby, A.; Michimae, H.; Matsui, H.; Takahashi, S.; Mabe, K.; Shimoyama, T.; Sasaki, M.; Terao, S.; Kamada, T.; et al. PCR analysis and specific immunohistochemistry revealing a high prevalence of non-Helicobacter pyloriHelicobacters inHelicobacter pylori-negative gastric disease patients in Japan: High susceptibility to an Hp eradication regimen. Helicobacter 2020, 25, e12700. [Google Scholar] [CrossRef]
- Yang, L.; Yamamoto, K.; Nishiumi, S.; Nakamura, M.; Matsui, H.; Takahashi, S.; Dohi, T.; Okada, T.; Kakimoto, K.; Hoshi, N.; et al. Interferon-γ-producing B cells induce the formation of gastric lymphoid follicles after Helicobacter suis infection. Mucosa Immunol. 2015, 8, 279–295. [Google Scholar] [CrossRef] [Green Version]
- Streubel, B.; Simonitsch-Klupp, I.; Mullauer, L.; Lamprecht, A.; Huber, D.; Siebert, R.; Stolte, M.; Trautinger, F.; Lukas, J.; Puspok, A.; et al. Variable frequencies of MALT lymphoma-associated genetic aberrations in MALT lymphomas of different sites. Leukemia 2004, 18, 1722–1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remstein, E.D.; Dogan, A.; Einerson, R.R.; Paternoster, S.F.; Fink, S.R.; Law, M.; Dewald, G.W.; Kurtin, P.J. The incidence and anatomic site specificity of chromosomal translocations in primary extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) in North America. Am. J. Surg. Pathol. 2006, 30, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Sakugawa, S.T.; Yoshino, T.; Nakamura, S.; Inagaki, H.; Sadahira, Y.; Nakamine, H.; Okabe, M.; Ichimura, K.; Tanimoto, M.; Akagi, T. API2-MALT1 fusion gene in colorectal lymphoma. Mod. Pathol. 2003, 16, 1232–1241. [Google Scholar] [CrossRef] [PubMed]
- Hyeon, J.; Lee, B.; Shin, S.H.; Yoo, H.Y.; Kim, S.J.; Kim, W.S.; Park, W.Y.; Ko, Y.H. Targeted deep sequencing of gastric marginal zone lymphoma identified alterations of TRAF3 and TNFAIP3 that were mutually exclusive for MALT1 rearrangement. Mod. Pathol. 2018, 31, 1418–1428. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wei, J.M.; Wang, Z.X.; Feng, Y.; Wei, Z.W.; Hou, X.; Xu, J.B.; He, Y.L.; Yang, D.J. Transcriptome hallmarks in Helicobacter pylori infection influence gastric cancer and MALT lymphoma. Epigenomics 2020, 12, 661–671. [Google Scholar] [CrossRef]
- Nakamura, S.; Ponzoni, M. Marginal zone B-cell lymphoma: Lessons from Western and Eastern diagnostic approaches. Pathology 2020, 52, 15–29. [Google Scholar] [CrossRef] [Green Version]
- Zucca, E.; Arcaini, L.; Buske, C.; Johnson, P.W.; Ponzoni, M.; Raderer, M.; Ricardi, U.; Salar, A.; Stamatopoulos, K.; Thieblemont, C.; et al. Marginal zone lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 17–29. [Google Scholar] [CrossRef] [Green Version]
- Pervez, S.; Mumtaz, K.; Ullah, S.S.; Akhtar, N.; Ali, N.; Aaqil, H. Immunoproliferative small intestinal disease (IPSID). J. Coll. Physicians Surg. Pak. 2011, 21, 57–58. [Google Scholar]
- Hong, J.T.; Kim, E.R.; Park, S.W.; Kim, J.W.; Hong, S.N.; Chang, D.K.; Kim, Y.H.; Cho, J.H. Long-term Prognosis of Localized Lymphoid Hyperplasia of the Rectum. Gut Liver 2021, 15, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Copie-Bergman, C.; Gaulard, P.; Lavergne-Slove, A.; Brousse, N.; Flejou, J.F.; Dordonne, K.; de Mascarel, A.; Wotherspoon, A.C.; GELA. Proposal for a new histological grading system for post-treatment evaluation of gastric MALT lymphoma. Gut 2003, 52, 1656. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, S.; Yao, T.; Aoyagi, K.; Iida, M.; Fujishima, M.; Tsuneyoshi, M. Helicobacter pylori and primary gastric lymphoma. A histopathologic and immunohistochemical analysis of 237 patients. Cancer 1997, 79, 3–11. [Google Scholar] [CrossRef]
- Nakamura, S.; Matsumoto, T.; Ye, H.T.; Nakamura, S.; Suekane, H.; Matsumoto, H.; Yao, T.; Tsuneyoshi, M.; Du, M.Q.; Iida, M. Helicobacter pylori-negative gastric mucosa-associated lymphoid tissue lymphoma—A clinicopathologic and molecular study with reference to antibiotic treatment. Cancer 2006, 107, 2770–2778. [Google Scholar] [CrossRef]
- Takigawa, H.; Masaki, S.; Naito, T.; Yuge, R.; Urabe, Y.; Tanaka, S.; Sentani, K.; Matsuo, T.; Matsuo, K.; Chayama, K.; et al. Helicobacter suis infection is associated with nodular gastritis-like appearance of gastric mucosa-associated lymphoid tissue lymphoma. Cancer Med. 2019, 8, 4370–4379. [Google Scholar] [CrossRef] [Green Version]
- Nonaka, K.; Ishikawa, K.; Shimizu, M.; Sakurai, T.; Nakai, Y.; Nakao, M.; Yoshino, K.; Arai, S.; Kita, H. Gastrointestinal: Gastric mucosa-associated lymphoma presented with unique vascular features on magnified endoscopy combined with narrow-band imaging. J. Gastroenterol. Hepatol. 2009, 24, 1697. [Google Scholar]
- Isomoto, H.; Matsushima, K.; Hayashi, T.; Imaizumi, Y.; Shiota, J.; Ishii, H.; Minami, H.; Ohnita, K.; Takeshima, F.; Shikuwa, S.; et al. Endocytoscopic findings of lymphomas of the stomach. BMC Gastroenterol. 2013, 13, 174. [Google Scholar] [CrossRef] [Green Version]
- Terada, T. Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) of the ileum in a 35-year-old Japanese woman. Int. J. Clin. Exp. Pathol. 2013, 6, 951–956. [Google Scholar]
- Ohashi, S.; Yazumi, S.; Watanabe, N.; Matsumoto, S.; Fukui, T.; Nishio, A.; Chiba, T. Education and imaging. Gastrointestinal: MALT lymphoma of the terminal ileum. J. Gastroenterol. Hepatol. 2006, 21, 1495. [Google Scholar] [CrossRef] [PubMed]
- Kai, K.; Miyahara, M.; Tokuda, Y.; Kido, S.; Masuda, M.; Takase, Y.; Tokunaga, O. A case of mucosa-associated lymphoid tissue lymphoma of the gastrointestinal tract showing extensive plasma cell differentiation with prominent Russell bodies. World J. Clin. Cases 2013, 1, 176–180. [Google Scholar] [CrossRef]
- Kurimoto, M.; Sonoki, T.; Nakamura, Y.; Yamamoto, Y.; Maeda, Y.; Kuriyama, K.; Mushino, T.; Hosoi, H.; Murata, S.; Shimanuki, M.; et al. Severe enteropathy caused by α-heavy chain disease lacking detectable M-proteins. Intern. Med. 2014, 53, 581–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.H.; Jung, J.T.; Kim, E.J.; Kim, T.W.; Kim, S.Y.; Kwon, J.G.; Kim, E.Y.; Sung, W.J. A case of mucosa-associated lymphoid tissue lymphoma of the sigmoid colon presenting as a semipedunculated polyp. Clin. Endosc. 2014, 47, 192–196. [Google Scholar] [CrossRef]
- Seo, S.W.; Lee, S.H.; Lee, D.J.; Kim, K.M.; Kang, J.K.; Kim, D.W.; Lee, J.H. Colonic mucosa-associated lymphoid tissue lymphoma identified by chromoendoscopy. World J. Gastroenterol. 2014, 20, 18487–18494. [Google Scholar] [CrossRef] [PubMed]
- Chahil, N.; Bloom, P.; Tyson, J.; Jazwari, S.; Robilotti, J.; Gaultieri, N. Novel approach to treatment of rectal mucosa-associated lymphoid tissue lymphoma. BMJ Case Rep. 2011, 2011, 2969. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, D.; Yoshida, N.; Ishii, M.; Takamasu, M.; Kishimoto, M.; Yagi, N.; Naitou, Y.; Yanagisawa, A. A case of colonic mucosa-associated lymphoid tissue lymphoma observed under endoscopy with narrow-band imaging. Nihon Shokakibyo Gakkai Zasshi 2013, 110, 2100–2106. [Google Scholar] [PubMed]
- Satoh, T.; Hotta, K.; Imai, K. Endocytoscopy for the diagnosis of marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue type in the rectum: Report of two cases. Dig. Endosc. 2020, 32, E54–E56. [Google Scholar] [CrossRef]
- Zullo, A.; Hassan, C.; Cristofari, F.; Andriani, A.; De Francesco, V.; Ierardi, E.; Tomao, S.; Stolte, M.; Morini, S.; Vaira, D. Effects of Helicobacter pylori Eradication on Early Stage Gastric Mucosa-Associated Lymphoid Tissue Lymphoma. Clin. Gastroenterol. Hepatol. 2010, 8, 105–110. [Google Scholar] [CrossRef]
- Fischbach, W.; Goebeler, M.E.; Ruskone-Fourmestraux, A.; Wundisch, T.; Neubauer, A.; Raderer, M.; Savio, A.; Grp, E. Most patients with minimal histological residuals of gastric MALT lymphoma after successful eradication of Helicobacter pylori can be managed safely by a watch and wait strategy: Experience from a large international series. Gut 2007, 56, 1685–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruskoné-Fourmestraux, A.; Fischbach, W.; Aleman, B.M.; Boot, H.; Du, M.Q.; Megraud, F.; Montalban, C.; Raderer, M.; Savio, A.; Wotherspoon, A. EGILS consensus report. Gastric extranodal marginal zone B-cell lymphoma of MALT. Gut 2011, 60, 747–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, S.; Matsumoto, T.; Suekane, H.; Nakamura, S.; Matsumoto, H.; Esaki, M.; Yao, T.; Iida, M. Long-term clinical outcome of Helicobacter pylori eradication for gastric mucosa-associated lymphoid tissue lymphoma with a reference to second-line treatment. Cancer 2005, 104, 532–540. [Google Scholar] [CrossRef]
- Nakamura, S.; Ye, H.T.; Bacon, C.M.; Goatly, A.; Liu, H.X.; Banham, A.H.; Ventura, R.; Matsumoto, T.; Iida, M.; Ohji, Y.; et al. Clinical impact of genetic aberrations in gastric MALT lymphoma: A comprehensive analysis using interphase fluorescence in situ hybridisation. Gut 2007, 56, 1358–1363. [Google Scholar] [CrossRef] [Green Version]
- Yokoi, T.; Nakamura, T.; Kasugai, K.; Yatabe, Y.; Fujita, M.; Kuroda, M.; Akaza, K.; Nomura, C.; Hamajima, E.; Suchi, T.; et al. Primary low-grade gastric mucosa-associated lymphoid tissue (MALT) lymphoma with polypoid appearance. Polypoid gastric MALT lymphoma: A clinicopathologic study of eight cases. Pathol. Int. 1999, 49, 702–709. [Google Scholar]
- Nakamura, T.; Seto, M.; Tajika, M.; Kawai, H.; Yokoi, T.; Yatabe, Y.; Nakamura, S. Clinical features and prognosis of gastric MALT lymphoma with special reference to responsiveness to H-Pylori eradication and API2-MALT1 status. Am. J. Gastroenterol. 2008, 103, 62–70. [Google Scholar] [CrossRef]
- Raderer, M.; Streubel, B.; Wohrer, S.; Hafner, M.; Chott, A. Successful antibiotic treatment of Helicobacter pylori negative gastric mucosa associated lymphoid tissue lymphomas. Gut 2006, 55, 616–618. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.; Kim, D.H.; Seo, H.I.; Gong, E.J.; Bang, C.S. Efficacy of eradication therapy in Helicobacter pylori-negative gastric mucosa-associated lymphoid tissue lymphoma: A meta-analysis. Helicobacter 2021, 26, e12774. [Google Scholar] [CrossRef]
- Hirata, N.; Tominaga, K.; Ohta, K.; Kadouchi, K.; Okazaki, H.; Tanigawa, T.; Shiba, M.; Watanabe, T.; Fujiwara, Y.; Nakamura, S.; et al. A case of mucosa-associated lymphoid tissue lymphoma forming multiple lymphomatous polyposis in the small intestine. World J. Gastroenterol. 2007, 13, 1453–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Na, H.K.; Won, S.H.; Ahn, J.Y.; Kim, G.H.; Jung, K.W.; Lee, J.H.; Kim, D.H.; Choi, K.D.; Song, H.J.; Lee, G.H.; et al. Clinical course of duodenal mucosa-associated lymphoid tissue lymphoma: Comparison with gastric mucosa-associated lymphoid tissue lymphoma. J. Gastroenterol. Hepatol. 2021, 36, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Iida, M.; Shimizu, M. Regression of mucosa-associated lymphoid-tissue lymphoma of rectum after eradication of Helicobacter pylori. Lancet 1997, 350, 115–116. [Google Scholar] [CrossRef]
- Nomura, E.; Uchimi, K.; Abue, M.; Kon, H.; Noguchi, T.; Suzuki, S.; Suzuki, M.; Onodera, H.; Tateno, H.; Ota, Y. Regression of MALT lymphoma of the rectum after Helicobacter pylori eradication therapy in a patient negative for Helicobacter pylori. Nihon Shokakibyo Gakkai Zasshi 2010, 107, 1466–1473. [Google Scholar]
- Makino, Y.; Suzuki, H.; Nishizawa, T.; Kameyama, K.; Hisamatsu, T.; Imaeda, H.; Mukai, M.; Hibi, T. Ileal Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma with a Large-Cell Component That Regressed Spontaneously. Gut Liver 2010, 4, 117–121. [Google Scholar] [CrossRef]
- Ruskone-Fourmestraux, A.; Matysiak-Budnik, T.; Fabiani, B.; Cervera, P.; Brixi, H.; Le Malicot, K.; Nion-Larmurier, I.; Flejou, J.F.; Hennequin, C.; Quero, L.; et al. Exclusive moderate-dose radiotherapy in gastric marginal zone B-cell MALT lymphoma: Results of a prospective study with a long term follow-up. Radiother. Oncol. 2015, 117, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Goda, J.S.; Gospodarowicz, M.; Pintilie, M.; Wells, W.; Hodgson, D.C.; Sun, A.; Crump, M.; Tsang, R.W. Long-Term Outcome in Localized Extranodal Mucosa-Associated Lymphoid Tissue Lymphomas Treated with Radiotherapy. Cancer 2010, 116, 3815–3824. [Google Scholar] [CrossRef]
- Yahalom, J.; Xu, A.J.; Noy, A.; Lobaugh, S.; Chelius, M.; Chau, K.; Portlock, C.; Hajj, C.; Imber, B.S.; Straus, D.J.; et al. Involved-site radiotherapy for Helicobacter pylori-independent gastric MALT lymphoma: 26 years of experience with 178 patients. Blood Adv. 2021, 5, 1830–1836. [Google Scholar] [CrossRef] [PubMed]
- Schmelz, R.; Miehlke, S.; Thiede, C.; Brueckner, S.; Dawel, M.; Kuhn, M.; Ruskoné-Formestraux, A.; Stolte, M.; Jentsch, C.; Hampe, J.; et al. Sequential H. pylori eradication and radiation therapy with reduced dose compared to standard dose for gastric MALT lymphoma stages IE & II1E: A prospective randomized trial. J. Gastroenterol. 2019, 54, 388–395. [Google Scholar]
- Reinartz, G.; Pyra, R.P.; Lenz, G.; Liersch, R.; Stüben, G.; Micke, O.; Willborn, K.; Hess, C.F.; Probst, A.; Fietkau, R.; et al. Favorable radiation field decrease in gastric marginal zone lymphoma: Experience of the German Study Group on Gastrointestinal Lymphoma (DSGL). Strahlenther. Onkol. 2019, 195, 544–557. [Google Scholar] [CrossRef]
- Okamura, T.; Suga, T.; Iwaya, Y.; Ito, T.; Yokosawa, S.; Arakura, N.; Ota, H.; Tanaka, E. Helicobacter pylori-Negative Primary Rectal MALT Lymphoma: Complete Remission after Radiotherapy. Case Rep. Gastroenterol. 2012, 6, 319–327. [Google Scholar] [CrossRef]
- Reinartz, G.; Molavi Tabrizi, C.; Liersch, R.; Ullerich, H.; Hering, D.; Willborn, K.; Schultze, J.; Micke, O.; Ruebe, C.; Fischbach, W.; et al. Renaissance of Radiotherapy in Intestinal Lymphoma? 10-Year Efficacy and Tolerance in Multimodal Treatment of 134 Patients: Follow-up of Two German Multicenter Consecutive Prospective Phase II Trials. Oncologist 2020, 25, e816–e832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imber, B.S.; Chau, K.W.; Lee, J.; Lee, J.; Casey, D.L.; Yang, J.C.; Wijentunga, N.A.; Shepherd, A.; Hajj, C.; Qi, S.; et al. Excellent response to very-low-dose radiation (4 Gy) for indolent B-cell lymphomas: Is 4 Gy suitable for curable patients? Blood Adv. 2021, 5, 4185–4197. [Google Scholar] [CrossRef]
- Amiot, A.; Levy, M.; Copie-Bergman, C.; Dupuis, J.; Szablewski, V.; Le Baleur, Y.; Baia, M.; Belhadj, K.; Sobhani, I.; Leroy, K.; et al. Rituximab, alkylating agents or combination therapy for gastric mucosa-associated lymphoid tissue lymphoma: A monocentric non-randomised observational study. Aliment. Pharmacol. Ther. 2014, 39, 619–628. [Google Scholar] [CrossRef]
- Zucca, E.; Conconi, A.; Martinelli, G.; Bouabdallah, R.; Tucci, A.; Vitolo, U.; Martelli, M.; Pettengell, R.; Salles, G.; Sebban, C.; et al. Final Results of the IELSG-19 Randomized Trial of Mucosa-Associated Lymphoid Tissue Lymphoma: Improved Event-Free and Progression-Free Survival with Rituximab Plus Chlorambucil Versus Either Chlorambucil or Rituximab Monotherapy. J. Clin. Oncol. 2017, 35, 1905–1912. [Google Scholar] [CrossRef]
- Salar, A.; Domingo-Domenech, E.; Panizo, C.; Nicolas, C.; Bargay, J.; Muntanola, A.; Canales, M.; Bello, J.L.; Sancho, J.M.; Tomas, J.F.; et al. Long-term results of a phase 2 study of rituximab and bendamustine for mucosa-associated lymphoid tissue lymphoma. Blood 2017, 130, 1772–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsukamoto, A.; Nakamura, F.; Nannya, Y.; Kobayashi, Y.; Shibahara, J.; Ichikawa, M.; Fukayama, M.; Koike, K.; Kurokawa, M. MALT lymphoma of the small bowel with protein-losing enteropathy. Int. J. Hematol. 2014, 99, 198–201. [Google Scholar] [CrossRef]
- Marks, D.J.; Prodromou, A.; Silvanto, A.; Cox, A.; Pakzad, F.; Train, M.; Mitchell, I.C. Ileal MALT lymphoma causing massive gastrointestinal haemorrhage revealed on computed tomography angiography. Postgrad. Med. J. 2009, 85, 163–165. [Google Scholar] [CrossRef]
- Akbulut, H.; Soykan, I.; Yakaryilmaz, F.; Icii, F.; Aksoy, F.; Haznedaroglu, S.; Yildirim, S. Five-year results of the treatment of 23 patients with immunoproliferative small intestinal disease: A Turkish experience. Cancer 1997, 80, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, G.; Anderson, K.C.; Harris, N.L.; Sohani, A.R. The Heavy Chain Diseases: Clinical and Pathologic Features. Oncology 2014, 28, 45–53. [Google Scholar]
- Nadatani, Y.; Tanigawa, T.; Fukunaga, S.; Kinoshita, Y.; Ominami, M.; Obayashi, T.; Morimoto, K.; Sogawa, M.; Yamagami, H.; Shiba, M.; et al. Primary small intestinal mucosa-associated lymphoid tissue lymphoma diagnosed by balloon-assisted enteroscopy. Intern. Med. 2014, 53, 2671–2674. [Google Scholar] [CrossRef] [Green Version]
- Dhull, A.K.; Kaushal, V.; Singh, S.; Pal, M.; Lathwal, A. A journey into insidious world of MALT lymphoma of the ileum: From the beginning to the end. J. Gastrointest. Oncol. 2014, 5, E125–E127. [Google Scholar] [PubMed]
- Lin, P.C.; Chen, J.S.; Deng, P.; Wang, C.W.; Huang, C.H.; Tang, R.; Chiang, J.M.; Yeh, C.Y.; Hsieh, P.S.; Tsai, W.S.; et al. Concurrent colonic mucosa-associated lymphoid tissue lymphoma and adenoma diagnosed after a positive fecal occult blood test: A case report. J. Med. Case Rep. 2016, 10, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.H.; Lin, Y.M.; Yen, H.H. Primary mucosa-associated lymphoid tissue lymphoma of the colon. Clin. Gastroenterol. Hepatol. 2011, 9, e74–e75. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Zhu, Z.; Zhang, C.; Xie, H.P. Successful Endoscopic Resection of Primary Rectal Mucosa-Associated Lymphoid Tissue Lymphoma by Endoscopic Submucosal Dissection: A Case Report. Front. Med. 2021, 8, 715256. [Google Scholar] [CrossRef] [PubMed]
- Choi, J. Successful Endoscopic Resection of Residual Colonic Mucosa-Associated Lymphoid Tissue Lymphoma after Polypectomy. Clin. Endosc. 2021, 54, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Piotrowski, R.; Kramer, R.; Kamal, A. Image of the month. Extranodal marginal zone B-cell (mucosa-associated lymphoid tissue) lymphoma of the colon presenting as an obstructing mass. Clin. Gastroenterol. Hepatol. 2008, 6, e18–e19. [Google Scholar] [CrossRef]
- Nakamura, S.; Matsumoto, T.; Takeshita, M.; Kurahara, K.; Yao, T.; Tsuneyoshi, M.; Iida, M.; Fujishima, M. A clinicopathologic study of primary small intestine lymphoma: Prognostic significance of mucosa-associated lymphoid tissue-derived lymphoma. Cancer 2000, 88, 286–294. [Google Scholar] [CrossRef]
- Nakamura, S.; Aoyagi, K.; Iwanaga, S.; Yao, T.; Tsuneyoshi, M.; Fujishima, M. Synchronous and metachronous primary gastric lymphoma and adenocarcinoma—A clinicopathologic study of 12 patients. Cancer 1997, 79, 1077–1085. [Google Scholar] [CrossRef]
- Isaka, T.; Nakamura, T.; Tajika, M.; Kawai, H.; Imaoka, H.; Okamoto, Y.; Aoki, M.; Inoue, H.; Takahashi, K.; Mizuno, N.; et al. API2-MALT1 chimeric transcript-positive gastroduodenal MALT lymphoma with subsequent development of adenocarcinoma as a collision tumour over a clinical course of 7 years. Histopathology 2007, 51, 119–123. [Google Scholar] [CrossRef]
- Kobayashi, K.; Furukawa, K.; Ishikawa, E.; Mitsuma, A.; Funasaka, K.; Kakushima, N.; Furune, S.; Ito, N.; Wada, H.; Hirose, T.; et al. Collision Tumors of Gastric Adenocarcinoma and Mucosa-associated Lymphoid Tissue Lymphoma. Intern. Med. 2021, 60, 2419–2424. [Google Scholar] [CrossRef]
- Devi, P.; Pattanayak, L.; Samantaray, S. Synchronous adenocarcinoma and mucosa-associated lymphoid tissue lymphoma of the colon. Saudi J. Gastroenterol. 2011, 17, 69–71. [Google Scholar] [PubMed]
- Dierickx, D.; Habermann, T.M. Post-Transplantation Lymphoproliferative Disorders in Adults. N. Engl. J. Med. 2018, 378, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Le Meur, Y.; Pontoizeau-Potelune, N.; Jaccard, A.; Paraf, F.; Leroux-Robert, C. Regression of a gastric lymphoma of mucosa-associated lymphoid tissue after eradication of Helicobacter pylori in a kidney graft recipient. Am. J. Med. 1999, 107, 530. [Google Scholar]
- Shehab, T.M.; Hsi, E.D.; Poterucha, J.J.; Gunaratnam, N.T.; Fontana, R.J. Helicobacter pylori-associated gastric MALT lymphoma in liver transplant recipients. Transplantation 2001, 71, 1172–1175. [Google Scholar] [CrossRef] [Green Version]
- Aull, M.J.; Buell, J.F.; Peddi, V.R.; Trofe, J.; Beebe, T.M.; Hanaway, M.J.; Roy-Chaudhury, P.; Alloway, R.R.; First, M.R.; Woodle, E.S. MALToma: A Helicobacter pylori-associated malignancy in transplant patients: A report from the Israel Penn International Transplant Tumor Registry with a review of published literature. Transplantation 2003, 75, 225–228. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n | Stage | BIRC3-MALT1 | 1st-Tx | 2nd-Tx after Eradiation | Ref. | ||||
|---|---|---|---|---|---|---|---|---|---|
| Eradication | Other Tx | ||||||||
| n | CR Rate | n | CR Rate | n | CR Rate * | ||||
| 14 | I, II1 | NE | 14 | 33% | [27] | ||||
| 18 | I, II1 | 7 (64%) | 17 | 29% | 1 (RT) | 100% | 12 (WW 7, RT 5) | 100% | [25] |
| 44 | I–IV | NE | 44 | 14% | [7] | ||||
| 13 | I, II1 | 5 (56%) | 5 | 40% | 5 (RT) | 80% | 3 (WW 1, RT 1, CTx 1) | 100% | [24] |
| 24 | I, II | 3 (23%) | 13 | 38% | 8 (CTx ± IM 8) | 100% | [23] | ||
| 28 | I–IV | NE | 28 | 57% | 12 (WW 5, RT 6, CTx 1) | 71% | [8] | ||
| 30 | I, II | NE | 18 | 33% | [22] | ||||
| 25 | I, II1 | 7 (28%) | 25 | 36% | 14 (RT 3, CTx ± IM 11) | 86% | [21] | ||
| 131 | I–IV | NE | 63 | 17% | 68 (RT or CTx ± IM or S) | 72% | [9] | ||
| 57 | I–IV | 22 (39%) † | 9 | 0% | 48 (WW 2, RT 1, CTx 44, other 1) | 33% | [10] | ||
| 34 | NE | NE | 34 | 44% | 19 (RT 19) | 100% | [20] | ||
| 37 | I–IV | 11 (30%) | 18 | 11% | 19 (RT 16, CTx 3) | 89% ‡ | 16 (WW 3, RT 12, CTx 1) | 92% | [28] |
| n | Stage | HP (−) | Non-CR, n (%) | 2nd-Tx | 2nd-Tx * | Ref. | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WW | RT | Other Tx | |||||||||||
| n | CR Rate | n | CR Rate | n | CR Rate | n | CR Rate | ||||||
| 105 | I, II1 | 13% | 24 | (24%) | 10 | NE | 14 (CTx ± IM 12, CTx + S 1, S 1) | 27% | [27] | ||||
| 60 | I, II1 | 12% | 10 | (17%) | 1 | 0% (SD 1) | 7 | 100% | 2 (RT + CTx 1, ER 1) | 100% | [26] | ||
| 420 | I–IV | 10% | 97 | (23%) | 15 | 0% (NC 15) | 82 † | 94% | [7] | ||||
| 66 | I, II1 | 20% | 16 | (29%) | 2 | 50% | 9 | 89% | 1 (CTx) | 0% | [24] | ||
| 345 | I–IV | 8% | 61 | (18%) | 42 | NE | 17 | 88% | 1 (CTx) | 100% | [8] | ||
| 339 | I–IV | 40% | 157 | (61%) | 57 | NE | 100 ‡ | 79% | [9] | ||||
| 96 | I–IV | 39% | 44 | (60%) | 3 | NE | 33 | 91% | 5 (CTx) | 63% | [28] | ||
| Age | Sex | Site | Macroscopic Findings | Stage | 1st-Tx | Response | FU Time, years | Ref. |
|---|---|---|---|---|---|---|---|---|
| 75 | M | Jejunum | Stricture, shallow ulcer | NA | E, R-CTx | PR | NA | [30] |
| 78 | F | Jejunum | Multiple ulcerative lesions | II1 | S (perforation) | CR | NA | [104] |
| 67 | F | Ileum | Long raised mucosal surface | II2 | S (obstruction) | CR | 0.5 | [32] |
| 58 | M | Ileum | 8 cm saccular dilation | IIIE | S + R | PR | 0.5 | [31] |
| 55 | M | Ileum | NA | NA | S + CTx (dilated segment) | CR | 1 | [105] |
| 56 | F | Ileum | NA | NA | R-CTx | CR | NA | [101] |
| 73 | F | Ileum | Cobble-stone-like erosion | NA | None (progression to T-prolymphocytic leukemia) | NA | 0.6 (DD) | [68] |
| 35 | F | Ileum | Multiple tumors and ulcers | Lo | CTx | CR | NA | [66] |
| 38 | M | TI | Multiple protruding lesions | Lo | None * | CR | 2 | [88] |
| 61 | F | TI | Multiple polypoid lesions | II | A, CTx | NA | NA | [67] |
| 73 | F | Entire | Nodular mucosal lesions | I | R-CTx | CR | NA | [100] |
| 50 | F | Entire | Multiple polypoid lesions | II | A, R-CTx | CR | 5 | [84] |
| Age | Sex | Site | Number | Size, mm | Stage | 1st-Tx | Response | FU Time, years | Ref. |
|---|---|---|---|---|---|---|---|---|---|
| n = 51 | Re, C, IC, Mul * | Sin:Mul 27:16 | I–V | ER 17, RT 12, S 8, CTx 4, ER + RT 4, S + RT 1, WW 5 | Rec 2, DOC 2 | 3.8 ‡ | [40] | ||
| n = 8 | Re/C, Mul † | Sin:Mul 4:4 | I–II | ER 2, S 4, CTx 1, S + CTx 1 | CR | 9 ‡ | [42] | ||
| 64 | F | C | Sin | NA | Lo | EMR | CR | 6 | [43] |
| 80 | F | C + A | Mul | NA | Lo | E (HP+) | PR→PD | 0.5 | [86] |
| 61 | M | A | Sin | 5 | Lo | EMR | CR | NA | [107] |
| 79 | M | T | Sin | 20 | I | ESD + E (HP+) | CR | 1 | [73] |
| 64 | M | T | Sin | NA | IIE | S | CR | 1 | [71] |
| 59 | M | Sig | Sin | 20 | Lo | EMR | CR | 3 | [106] |
| 54 | M | Sig | Sin | 20 | IE | EMR | CR | 0.8 | [70] |
| 50 | F | Sig | Sin | 18 | Lo | S | NA | NA | [43] |
| 83 | F | AV25cm | Sin | NA | IE | RT→ER | CR | NA | [110] |
| 57 | F | Re | Sin | NA | Lo | ESD | NA | NA | [43] |
| 58 | F | Re | Sin | 5 | Lo | ESD | CR | 0.8 | [108] |
| 54 | F | Re | Sin | 30 | IE | EMR→ESD for residual tumor | CR | 4 | [109] |
| 57 | F | Re | Sin | >30 | Lo | RT | CR | 0.8 | [43] |
| 65 | M | Re | Sin | 10 | I | RT | CR | 5.4 | [94] |
| 83 | F | Re | Sin | 30 | II2 | R | CR | 0.3 | [39] |
| 78 | F | Re | Sin | 30 | NA | E | NC | 3 | [72] |
| 53 | F | Re | Sin | 20 | I | E (HP−) | CR | 0.3 | [87] |
| 56 | F | Re | Mul | 10, 25 | I | EMR + RT | CR | 6.3 | [94] |
| 62 | F | Re | Mul | 6, 20 | I | RT | CR | 1.1 | [94] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishikawa, E.; Nakamura, M.; Satou, A.; Shimada, K.; Nakamura, S. Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma in the Gastrointestinal Tract in the Modern Era. Cancers 2022, 14, 446. https://doi.org/10.3390/cancers14020446
Ishikawa E, Nakamura M, Satou A, Shimada K, Nakamura S. Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma in the Gastrointestinal Tract in the Modern Era. Cancers. 2022; 14(2):446. https://doi.org/10.3390/cancers14020446
Chicago/Turabian StyleIshikawa, Eri, Masanao Nakamura, Akira Satou, Kazuyuki Shimada, and Shotaro Nakamura. 2022. "Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma in the Gastrointestinal Tract in the Modern Era" Cancers 14, no. 2: 446. https://doi.org/10.3390/cancers14020446
APA StyleIshikawa, E., Nakamura, M., Satou, A., Shimada, K., & Nakamura, S. (2022). Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma in the Gastrointestinal Tract in the Modern Era. Cancers, 14(2), 446. https://doi.org/10.3390/cancers14020446