
Is Lymphocyte C-Reactive Protein Ratio Useful for Predicting Survival in Patients with Non-Metastatic Soft Tissue Sarcoma?


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient, Tumor, and Treatment Characteristics
3.2. The Relationship between the LCR and Clinical Characteristics
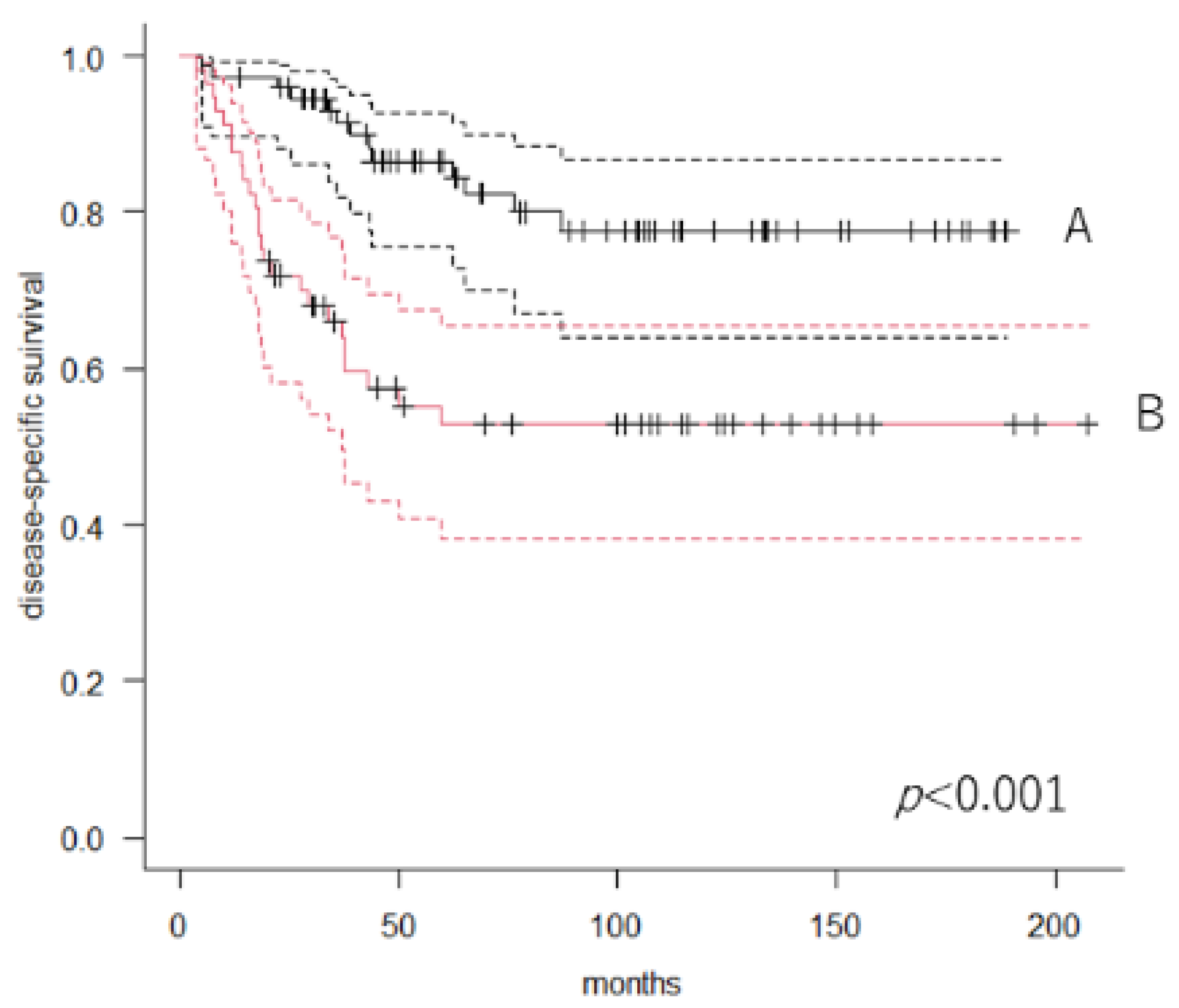
3.3. Overall DSS and Predictors of Mortality
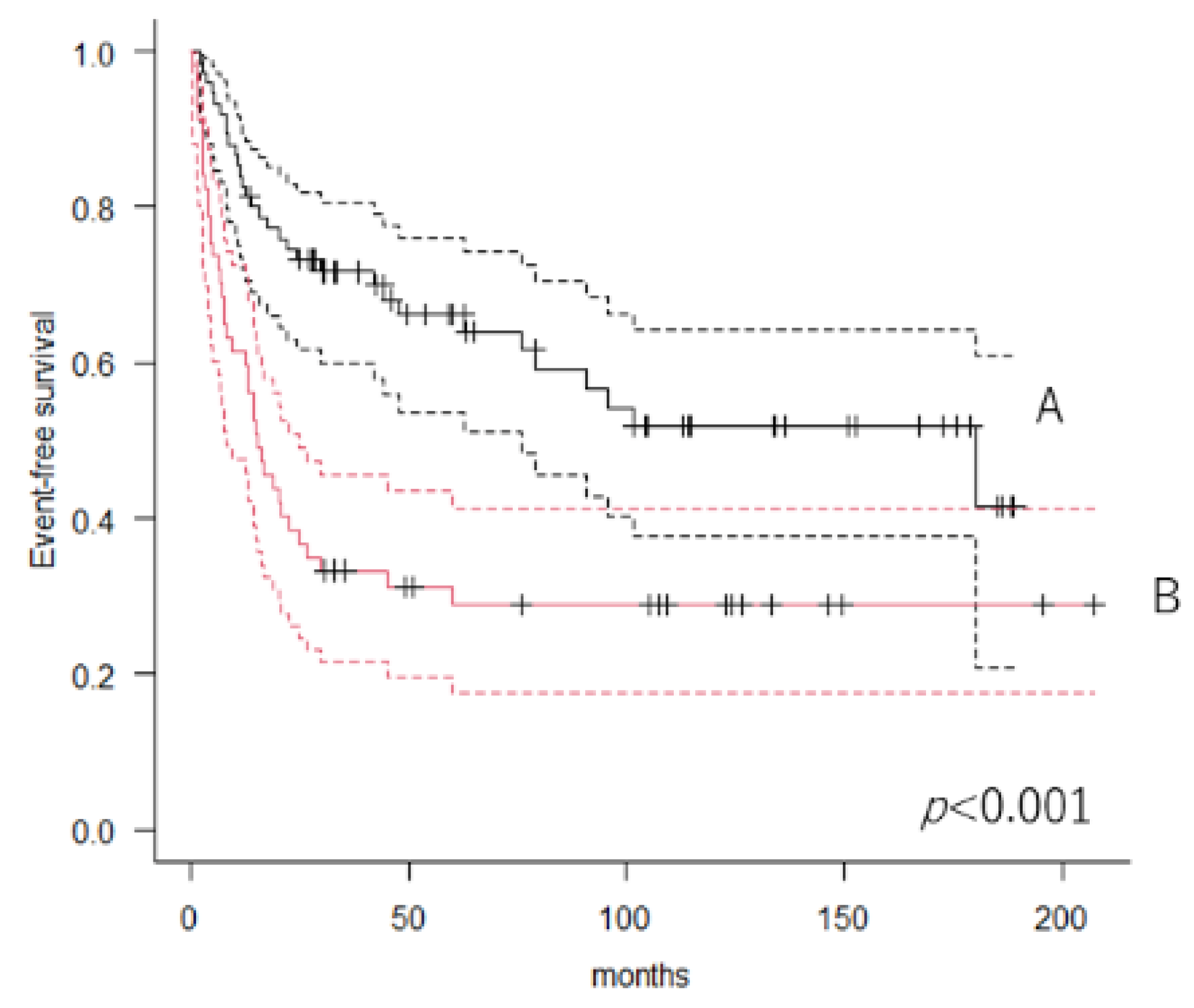
3.4. Event-Free Rate and Predictors of Events
3.5. ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clark, M.A.; Fisher, C.; Judson, I.; Thomas, J.M. Soft-Tissue Sarcomas in Adults. N. Engl. J. Med. 2005, 353, 701–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunar, K.Z.; Matthew, T.B.; Peter, W.T.; Raphael, E.P.; Shreyaskumar, R.P.; Robert, S.B.; Harry, L.E. Prognostic factors for patients with localized soft-tissue sarcoma treated with conservation surgery and radiation therapy. Cancer 2003, 97, 2530–2543. [Google Scholar] [CrossRef]
- Nakamura, T.; Asanuma, K.; Takao, M.; Yamanaka, T.; Koike, H.; Chen-Yoshikawa, T.F.; Tsukushi, S.; Kuroda, H.; Kozawa, E.; Sano, M.; et al. Clinical Outcome in Soft Tissue Sarcoma Patients with Lung Metastasis Who Received Metastasectomy and/or Radiofrequency Ablation: Tokai Musculoskeletal Oncology Consortium Study. Cancer Manag. Res. 2021, 13, 8473–8480. [Google Scholar] [CrossRef]
- Wang, X.; Liu, S.; Zhao, X.; Fang, E.; Zhao, X. The value of C-reactive protein as an independent prognostic indicator for disease-specific survival in patients with soft tissue sarcoma: A meta-analysis. PLoS ONE 2019, 14, e0219215. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Matsumine, A.; Matsubara, T.; Asanuma, K.; Uchida, A.; Sudo, A. Clinical significance of pretreatment serum C-reactive protein level in soft tissue sarcoma. Cancer 2011, 118, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Grimer, R.; Gaston, C.; Francis, M.; Charman, J.; Graunt, P.; Uchida, A.; Sudo, A.; Jeys, L. The value of C-reactive protein and comorbidity in predicting survival of patients with high grade soft tissue sarcoma. Eur. J. Cancer 2013, 49, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.S.; Oduyebo, T.; Cobb, L.P.; Cholakian, D.; Kong, X.; Fader, A.N.; Levinson, K.L.; Tanner, E.J.; Stone, R.L.; Piotrowski, A.; et al. Lymphopenia and its association with survival in patients with locally advanced cervical cancer. Gynecol. Oncol. 2015, 140, 76–82. [Google Scholar] [CrossRef] [Green Version]
- Clark, E.; Connor, S.; Taylor, M.; Madhavan, K.; Garden, O.; Parks, R. Preoperative lymphocyte count as a prognostic factor in resected pancreatic ductal adenocarcinoma. HPB 2007, 9, 456–460. [Google Scholar] [CrossRef] [Green Version]
- Feng, J.-F.; Liu, J.-S.; Huang, Y. Lymphopenia Predicts Poor Prognosis in Patients With Esophageal Squamous Cell Carcinoma. Medicine 2014, 93, e257. [Google Scholar] [CrossRef]
- Okugawa, Y.; Toiyama, Y.; Yamamoto, A.; Shigemori, T.; Ide, S.; Kitajima, T.; Fujikawa, H.; Yasuda, H.; Hiro, J.; Yoshiyama, S.; et al. Lymphocyte-C-reactive Protein Ratio as Promising New Marker for Predicting Surgical and Oncological Outcomes in Colorectal Cancer. Ann. Surg. 2019, 272, 342–351. [Google Scholar] [CrossRef]
- Angin, Y.S.; Yildirim, M.; Dasiran, F.; Okan, I. Could lymphocyte to C-reactive protein ratio predict the prognosis in patients with gastric cancer? ANZ J. Surg. 2021, 91, 1521–1527. [Google Scholar] [CrossRef]
- Iseda, N.; Itoh, S.; Yoshizumi, T.; Tomiyama, T.; Morinaga, A.; Shimagaki, T.; Wang, H.; Kurihara, T.; Toshima, T.; Nagao, Y.; et al. Lymphocyte-to-C-reactive protein ratio as a prognostic factor for hepatocellular carcinoma. Int. J. Clin. Oncol. 2021, 26, 1890–1900. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, M.; Kawakubo, H.; Hoshino, S.; Matsuda, S.; Mayanagi, S.; Irino, T.; Fukuda, K.; Nakamura, R.; Wada, N.; Kitagawa, Y. Lymphocyte-to-C-Reactive Protein Ratio as a Novel Marker for Predicting Oncological Outcomes in Patients with Esophageal Cancer. World J. Surg. 2021, 45, 3370–3377. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Lee, J.; Kim, H.; Shin, K.; Lee, M.; Park, J.M.; Choi, M.-G.; Park, C.H.; Song, K.Y.; Lee, H.H.; et al. Association between absolute lymphocyte count and overall mortality in patients with surgically resected gastric cancer. Korean J. Intern. Med. 2021, 36, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Karantanos, T.; Karanika, S.; Seth, B.; Gignac, G. The absolute lymphocyte count can predict the overall survival of patients with non-small cell lung cancer on nivolumab: A clinical study. Clin. Transl. Oncol. 2018, 21, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Suekane, S.; Kurose, H.; Ogasawara, N.; Hiroshige, T.; Chikui, K.; Uemura, K.; Nakiri, M.; Nishihara, K.; Matsuo, M.; et al. Absolute lymphocyte count is an independent predictor of survival in patients with metastatic renal cell carcinoma treated with nivolumab. Jpn. J. Clin. Oncol. 2021, 52, 179–186. [Google Scholar] [CrossRef]
- Suriu, C.; Akria, L.; Azoulay, D.; Shaoul, E.; Barhoum, M.; Braester, A. Absolute lymphocyte count as a prognostic marker in newly diagnosed multiple myeloma patients. Int. J. Lab. Hematol. 2016, 38, e56–e59. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.E.; Zhu, F.; Li, T.; Wu, H.; Galloway, T.J.; Farma, J.M.; Perlis, C.S.; Turaka, A. Absolute lymphocyte count: A potential prognostic factor for Merkel cell carcinoma. J. Am. Acad. Dermatol. 2014, 70, 1028–1035. [Google Scholar] [CrossRef]
- Brewster, R.; Purington, N.; Henry, S.; Wood, D.; Ganjoo, K.; Bui, N. Evaluation of Absolute Lymphocyte Count at Diagnosis and Mortality Among Patients With Localized Bone or Soft Tissue Sarcoma. JAMA Netw. Open 2021, 4, e210845. [Google Scholar] [CrossRef]
- Seo, S.T.; Singh, V.A.; Yasin, N.F. Preoperative lymphocyte count in relation to sarcoma prognosis. J. Orthop. Surg. 2019, 27, 2309499019854957. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, N.; Liu, H.; Gong, X.; Zhu, R.; Li, X.; Sun, Z.; Zong, X.; Li, N.; Meng, C.; et al. Circulating activated lymphocyte subsets as potential blood biomarkers of cancer progression. Cancer Med. 2020, 9, 5086–5094. [Google Scholar] [CrossRef] [PubMed]
- Mellman, I.; Coukos, G.; Dranoff, G. Cancer immunotherapy comes of age. Nature 2011, 480, 480–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, P.; Chen, L.; Zhang, H. Natural Killer Cells in Liver Disease and Hepatocellular Carcinoma and the NK Cell-Based Immunotherapy. J. Immunol. Res. 2018, 2018, 1206737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanetti, M. Tapping CD4 T Cells for Cancer Immunotherapy: The Choice of Personalized Genomics. J. Immunol. 2015, 194, 2049–2056. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, T.; Matsumine, A.; Matsubara, T.; Asanuma, K.; Uchida, A.; Sudo, A. The combined use of the neutrophil-lymphocyte ratio and C-reactive protein level as prognostic predictors in adult patients with soft tissue sarcoma. J. Surg. Oncol. 2013, 108, 481–485. [Google Scholar] [CrossRef] [PubMed]
- García-Ortega, D.Y.; Álvarez-Cano, A.; Sánchez-Llamas, L.A.; Caro-Sanchez, C.H.; Martínez-Said, H.; Luna-Ortiz, K.; Cuéllar-Hübbe, M. Neutrophil/lymphocyte ratio is associated with survival in synovial sarcoma. Surg. Oncol. 2018, 27, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Que, Y.; Qiu, H.; Li, Y.; Chen, Y.; Xiao, W.; Zhou, Z.; Zhang, X. Preoperative platelet-lymphocyte ratio is superior to neutrophil-lymphocyte ratio as a prognostic factor for soft-tissue sarcoma. BMC Cancer 2015, 15, 648. [Google Scholar] [CrossRef] [Green Version]
- Szkandera, J.; Gerger, A.; Liegl-Atzwanger, B.; Absenger, G.; Stotz, M.; Friesenbichler, J.; Trajanoski, S.; Stojakovic, T.; Eberhard, K.; Leithner, A.; et al. The lymphocyte/monocyte ratio predicts poor clinical outcome and improves the predictive accuracy in patients with soft tissue sarcomas. Int. J. Cancer 2013, 135, 362–370. [Google Scholar] [CrossRef]
- Nakamura, T.; Katagiri, H.; Shido, Y.; Hamada, S.; Yamada, K.; Nagano, A.; Yamada, S.; Tsukushi, S.; Ishimura, D.; Matsumine, A.; et al. Analysis of Factors for Predicting Survival in Soft-tissue Sarcoma with Metastatic Disease at Initial Presentation. Anticancer Res. 2017, 37, 3137–3141. [Google Scholar] [CrossRef] [Green Version]
- Fujibuchi, T.; Miyawaki, J.; Kidani, T.; Imai, H.; Miura, H. Prediction of Soft Tissue Sarcoma from Clinical Characteristics and Laboratory Data. Cancers 2020, 12, 679. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Unit | Value |
|---|---|---|
| Age | mean | 63 years |
| range | 21–89 years | |
| Sex | male | 79 |
| female | 53 | |
| Size | mean | 8.9 cm |
| range | 2–30 cm | |
| depth | superficial | 25 |
| Deep | 107 | |
| Grade | 1 | 12 |
| 2 | 38 | |
| 3 | 82 | |
| CRP | mg/dL | 0.155 |
| Range | 0.01–20.4 | |
| ALC | /µL | 1770 |
| Range | 380–3710 |
| Variables | Unit | Low LCR | High LCR | p Value |
|---|---|---|---|---|
| Age | mean | 63 | 63 | 0.843 |
| Sex | male | 39 | 40 | 0.107 |
| female | 18 | 35 | ||
| Size | mean | 5.7 | 4.9 | 0.011 |
| depth | superficial | 7 | 18 | 0.117 |
| deep | 50 | 57 | ||
| Grade | 1 | 1 | 11 | <0.001 |
| 2 | 11 | 27 | ||
| 3 | 45 | 37 |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Unit | HR | 95% CI | p Value | HR | 95% CI | p Value |
| Age | years | 1.019 | 0.994–1.044 | 0.139 | |||
| Sex | female | 1 | |||||
| male | 0.8772 | 0.461–1.671 | 0.69 | ||||
| Size | cm | 1.116 | 1.063–1.171 | <0.001 | 1.096 | 1.039–1.157 | <0.001 |
| Depth | deep | 1 | |||||
| s.c | 0.739 | 0.308–1.771 | 0.498 | ||||
| Grade | 1 | 1 | |||||
| 2 | 3.18 | 0.403–25.1 | 0.273 | ||||
| 3 | 5.372 | 0.731–39.53 | 0.099 | ||||
| Histology | MFS | 1 | |||||
| UPS | 2.034 | 0.680–6.080 | 0.204 | ||||
| Others | 1.874 | 0.715–4.915 | 0.202 | ||||
| Cx | No | 1 | |||||
| Yes | 1.58 | 0.797–3.133 | 0.190 | ||||
| LCR | high | 1 | 1 | ||||
| Low | 3.206 | 1.638–6.277 | <0.001 | 1.836 | 0.868–3.883 | 0.112 | |
| CRP | mg/dL | 1.177 | 1.109–1.25 | <0.001 | 1.128 | 1.052–1.209 | <0.001 |
| ALC | /µL | 0.999 | 0.999–1 | 0.35 | |||
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Unit | HR | 95% CI | p Value | HR | 95% CI | p Value |
| Age | years | 1.018 | 1.001–1.036 | 0.037 | 1.017 | 0.999–1.036 | 0.063 |
| Sex | female | 1 | |||||
| male | 0.942 | 0.586–1.513 | 0.804 | ||||
| Size | cm | 1.108 | 1.064–1.154 | <0.001 | 1.079 | 1.028–1.133 | <0.001 |
| depth | deep | 1 | 0.81 | 0.379–1.73 | 0.586 | ||
| s.c | 0.4751 | 0.235–0.959 | 0.038 | ||||
| Grade | 1 | 1 | |||||
| 2 | 3.589 | 0.828–15.55 | 0.088 | 2.156 | 0.483–9.627 | 0.315 | |
| 3 | 6.171 | 1.498–25.42 | 0.012 | 3.385 | 0.79–14.5 | 0.101 | |
| Histology | MFS | 1 | |||||
| UPS | 1.442 | 0.673–3.087 | 0.347 | ||||
| Others | 1.711 | 0.902–3.246 | 0.1 | ||||
| Cx | No | 1 | |||||
| Yes | 1.635 | 0.987–2.709 | 0.0561 | ||||
| LCR | High | 1 | 1 | ||||
| Low | 2.438 | 1.522–3.905 | <0.001 | 1.462 | 0.849–2.52 | 0.171 | |
| CRP | mg/dL | 1.187 | 1.123–1.255 | <0.001 | 1.123 | 1.051–1.2 | <0.001 |
| ALC | /µL | 0.999 | 0.999–1 | 0.676 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, T.; Hagi, T.; Asanuma, K.; Sudo, A. Is Lymphocyte C-Reactive Protein Ratio Useful for Predicting Survival in Patients with Non-Metastatic Soft Tissue Sarcoma? Cancers 2022, 14, 5214. https://doi.org/10.3390/cancers14215214
Nakamura T, Hagi T, Asanuma K, Sudo A. Is Lymphocyte C-Reactive Protein Ratio Useful for Predicting Survival in Patients with Non-Metastatic Soft Tissue Sarcoma? Cancers. 2022; 14(21):5214. https://doi.org/10.3390/cancers14215214
Chicago/Turabian StyleNakamura, Tomoki, Tomohito Hagi, Kunihiro Asanuma, and Akihiro Sudo. 2022. "Is Lymphocyte C-Reactive Protein Ratio Useful for Predicting Survival in Patients with Non-Metastatic Soft Tissue Sarcoma?" Cancers 14, no. 21: 5214. https://doi.org/10.3390/cancers14215214
APA StyleNakamura, T., Hagi, T., Asanuma, K., & Sudo, A. (2022). Is Lymphocyte C-Reactive Protein Ratio Useful for Predicting Survival in Patients with Non-Metastatic Soft Tissue Sarcoma? Cancers, 14(21), 5214. https://doi.org/10.3390/cancers14215214