
Speech and Language Errors during Awake Brain Surgery and Postoperative Language Outcome in Glioma Patients: A Systematic Review


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
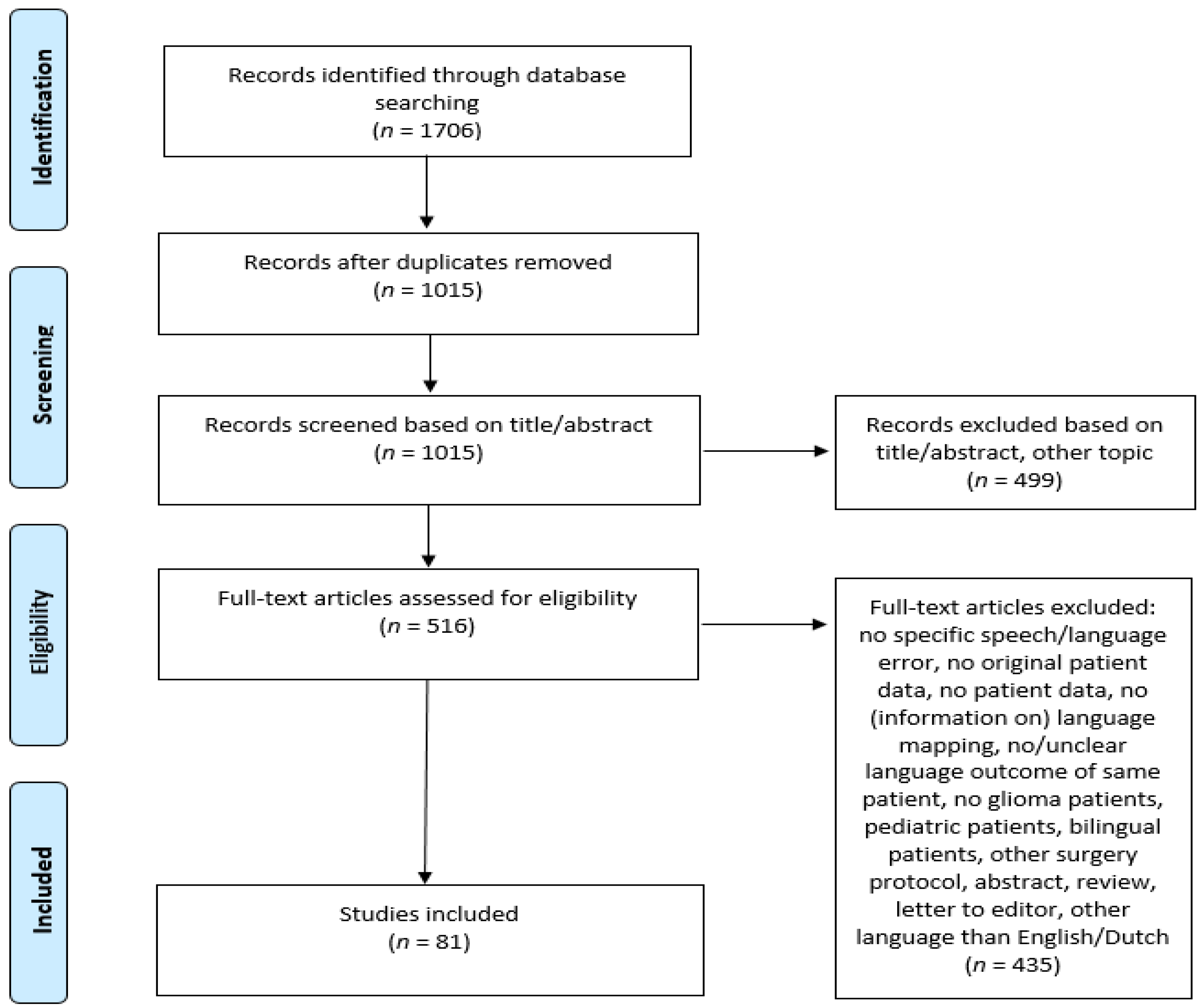
2.1. Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Organization
2.4. Analyses
3. Results
3.1. Intraoperative Speech and Language Errors and Language Status
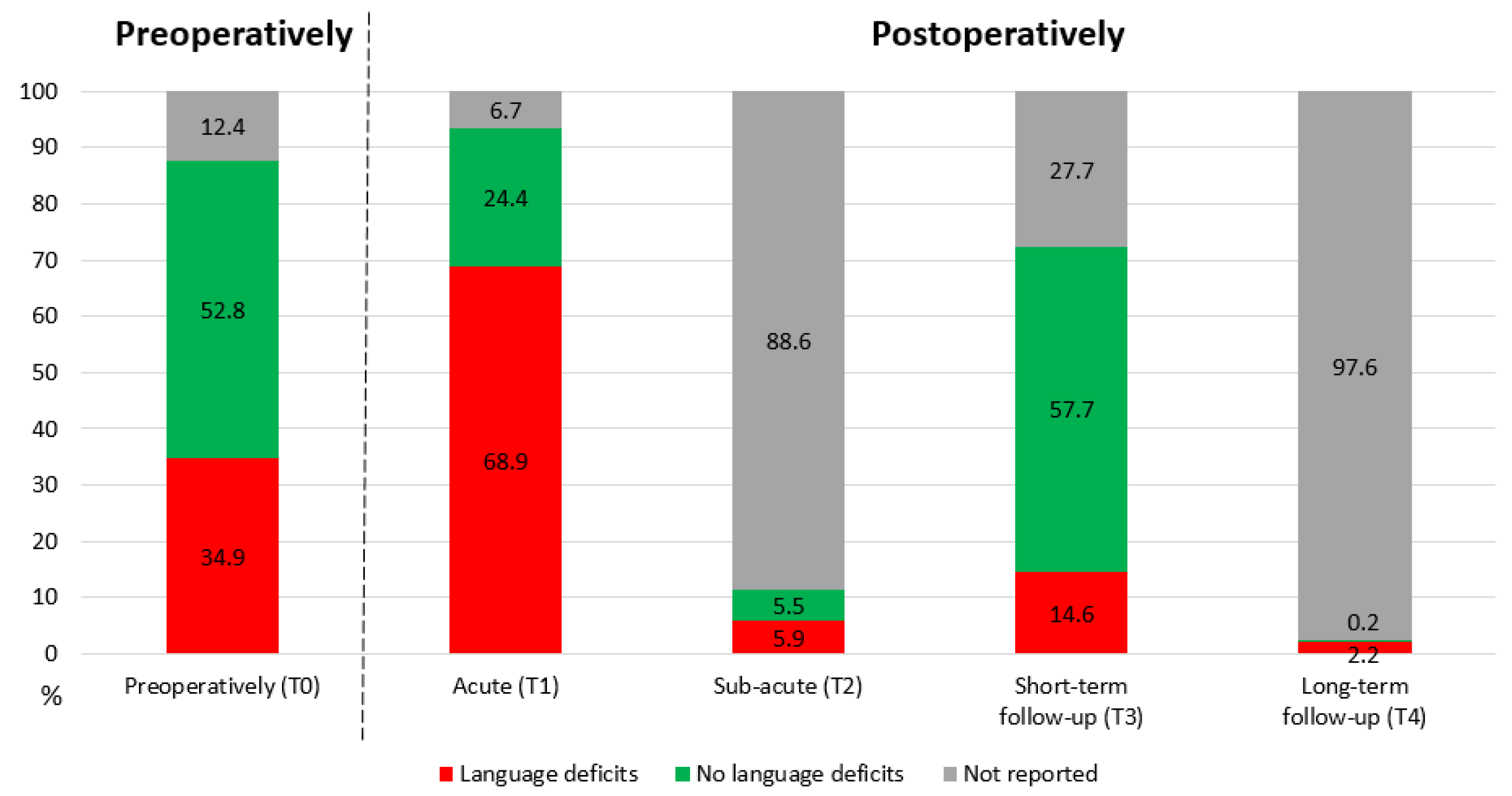
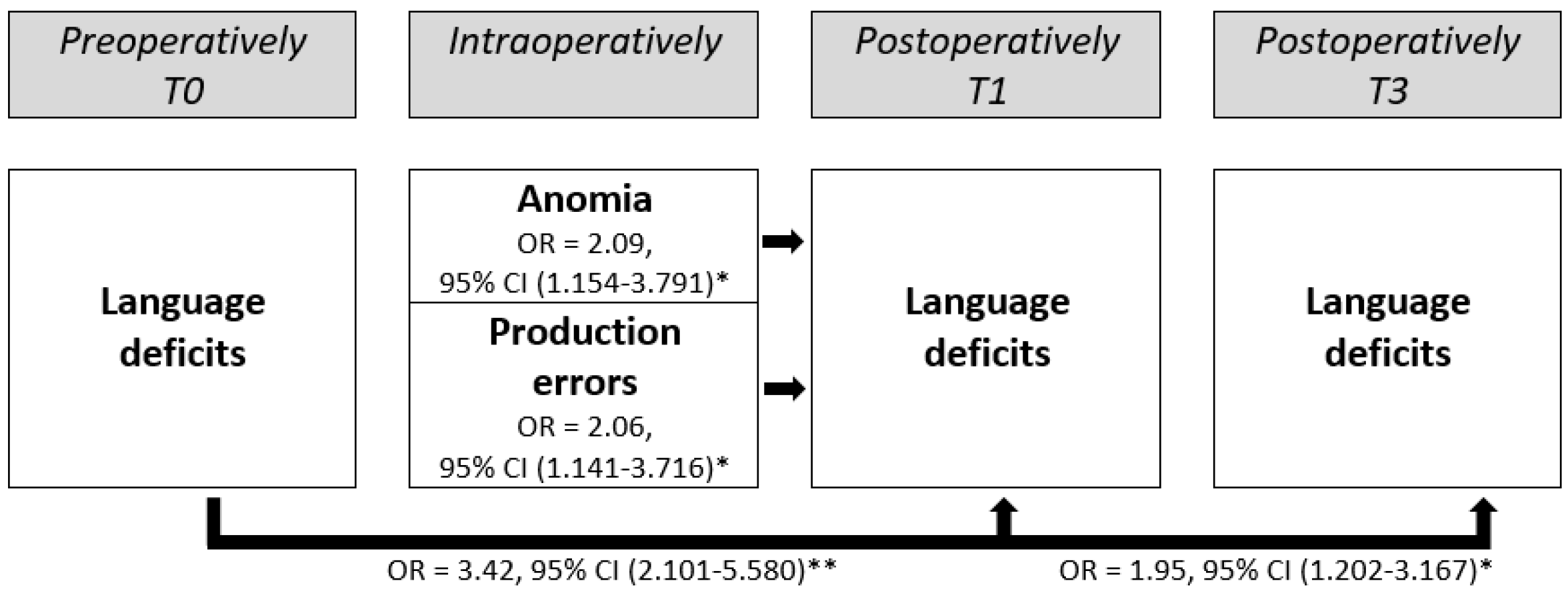
3.2. Relation to Postoperative Acute and Short-Term Language Outcome (T1 and T3)
3.3. Relation to the Type of Postoperative Acute Language Outcome (T1)
4. Discussion
4.1. Intraoperative Speech and Language Errors and Language Status
4.2. Relation to Postoperative Acute and Short-Term Language Outcome (T1 and T3)
4.3. Relation to the Type of Postoperative Acute Language Outcome (T1)
4.4. Clinical Relevance
4.5. Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Witt Hamer, P.C.; Robles, S.G.; Zwinderman, A.H.; Duffau, H.; Berger, M.S. Impact of intraoperative stimulation brain mapping on glioma surgery outcome: A meta-analysis. J. Clin. Oncol. 2012, 30, 2559–2565. [Google Scholar] [CrossRef] [Green Version]
- Sanai, N.; Berger, M.S. Glioma extent of resection and its impact on patient outcome. Neurosurgery 2008, 62, 753–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerritsen, J.K.W.; Arends, L.; Klimek, M.; Dirven, C.M.F.; Vincent, A.J.-P.E. Impact of intraoperative stimulation mapping on high-grade glioma surgery outcome: A meta-analysis. Acta Neurochir. 2019, 161, 99–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borchers, S.; Himmelbach, M.; Logothetis, N.; Karnath, H.O. Direct electrical stimulation of human cortex—The gold standard for mapping brain functions? Nat. Rev. Neurosci. 2012, 13, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Desmurget, M.; Song, Z.; Mottolese, C.; Sirigu, A. Re-establishing the merits of electrical brain stimulation. Trends Cogn. Sci. 2013, 17, 442–449. [Google Scholar] [CrossRef]
- Santini, B.; Talacchi, A.; Squintani, G.; Casagrande, F.; Capasso, R.; Miceli, G. Cognitive outcome after awake surgery for tumors in language areas. J. Neuro-Oncol. 2012, 108, 319–326. [Google Scholar] [CrossRef]
- Racine, C.A.; Li, J.; Molinaro, A.M.; Butowski, N.; Berger, M.S. Neurocognitive function in newly diagnosed low-grade glioma patients undergoing surgical resection with awake mapping techniques. Neurosurgery 2015, 77, 371–379. [Google Scholar] [CrossRef]
- Satoer, D.; Visch-Brink, E.; Smits, M.; Kloet, A.; Looman, C.; Dirven, C.; Vincent, A. Long-term evaluation of cognition after glioma surgery in eloquent areas. J. Neuro-Oncol. 2014, 116, 153–160. [Google Scholar] [CrossRef]
- Duffau, H.; Capelle, L.; Sichez, N.; Denvil, D.; Lopes, M.; Sichez, J.; Bitar, A.; Fohanno, D. Intraoperative mapping of the subcortical language pathways using direct stimulations: An anatomo-functional study. Brain 2002, 125, 199–214. [Google Scholar] [CrossRef] [Green Version]
- Satoer, D.; Vincent, A.; Ruhaak, L.; Smits, M.; Dirven, C.; Visch-Brink, E. Spontaneous speech in patients with gliomas in eloquent areas: Evaluation until 1 year after surgery. Clin. Neurol. Neurosurg. 2018, 167, 112–116. [Google Scholar] [CrossRef]
- Hilari, K.; Needle, J.J.; Harrison, K.L. What are the important factors in health-related quality of life for people with aphasia? A systematic review. Arch. Phys. Med. Rehabil. 2012, 93, S86–S95. [Google Scholar] [CrossRef] [PubMed]
- Talacchi, A.; Santini, B.; Savazzi, S.; Gerosa, M. Cognitive effects of tumour and surgical treatment in glioma patients. J. Neuro-Oncol. 2011, 103, 541–549. [Google Scholar] [CrossRef]
- Satoer, D.; Vork, J.; Visch-Brink, E.; Smits, M.; Dirven, C.; Vincent, A. Cognitive functioning early after surgery of gliomas in eloquent areas. J. Neurosurg. 2012, 117, 831–838. [Google Scholar] [CrossRef] [Green Version]
- Antonsson, M.; Jakola, A.; Longoni, F.; Carstam, L.; Hartelius, L.; Thordstein, M.; Tisell, M. Post-surgical effects on language in patients with presumed low-grade glioma. Acta Neurol. Scand. 2017, 137, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Taphoorn, M.J.; Klein, M. Cognitive deficits in adult patients with brain tumours. Lancet Neurol. 2004, 3, 159–168. [Google Scholar] [CrossRef]
- Bello, L.; Gallucci, M.; Fava, M.; Carrabba, G.; Giussani, C.; Acerbi, F.; Baratta, P.; Songa, V.; Conte, V.; Branca, V.; et al. Intraoperative subcortical language tract mapping guides surgical removal of gliomas involving speech areas. Neurosurgery 2007, 60, 67–82. [Google Scholar] [CrossRef]
- Ilmberger, J.; Ruge, M.; Kreth, F.W.; Briegel, J.; Reulen, H.J.; Tonn, J.C. Intraoperative mapping of language functions: A longitudinal neurolinguistic analysis. J. Neurosurg. 2008, 109, 583–592. [Google Scholar] [CrossRef] [Green Version]
- Rolston, J.D.; Englot, D.J.; Benet, A.; Li, J.; Cha, S.; Berger, M.S. Frontal operculum gliomas: Language outcome following resection. J. Neurosurg. 2015, 122, 725–734. [Google Scholar] [CrossRef] [Green Version]
- Wolthuis, N.; Bosma, I.; Bastiaanse, R.; Cherian, P.J.; Smits, M.; Veenstra, W.; Wagemakers, M.; Vincent, A.; Satoer, D. Distinct Slow-Wave Activity Patterns in Resting-State Electroencephalography and Their Relation to Language Functioning in Low-Grade Glioma and Meningioma Patients. Front. Hum. Neurosci. 2022, 16, 1–14. [Google Scholar] [CrossRef]
- Chang, W.H.; Pei, Y.C.; Wei, K.C.; Chao, Y.P.; Chen, M.H.; Yeh, H.A.; Jaw, F.S.; Chen, P.Y. Intraoperative linguistic performance during awake brain surgery predicts postoperative linguistic deficits. J. Neuro-Oncol. 2018, 139, 215–223. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H.; Gatignol, P.; Mandonnet, E.; Capelle, L.; Taillandier, L. Intraoperative subcortical stimulation mapping of language pathways in a consecutive series of 115 patients with Grade II glioma in the left dominant hemisphere. J. Neurosurg. 2008, 109, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Satoer, D.; Kloet, A.; Vincent, A.; Dirven, C.; Visch-Brink, E. Dynamic aphasia following low-grade glioma surgery near the supplementary motor area: A selective spontaneous speech deficit. Neurocase 2014, 20, 704–716. [Google Scholar] [CrossRef] [PubMed]
- De Witte, E.; Satoer, D.; Robert, E.; Colle, H.; Verheyen, S.; Visch-Brink, E.; Mariën, P. The Dutch linguistic intraoperative protocol: A valid linguistic approach to awake brain surgery. Brain Lang 2015, 140, 35–48. [Google Scholar] [CrossRef]
- Alimohamadi, M.; Shirani, M.; Shariat Moharari, R.; Pour-Rashidi, A.; Ketabchi, M.; Khajavi, M.; Arami, M.; Amirjamshidi, A. Application of Awake Craniotomy and Intraoperative Brain Mapping for Surgical Resection of Insular Gliomas of the Dominant Hemisphere. World Neurosurg. 2016, 92, 151–158. [Google Scholar] [CrossRef]
- Bartha, L.; Knosp, E.; Pfisterer, W.; Benke, T. Intra- and perioperative monitoring of language functions in patients with tumours in the left perisylvian area. Aphasiology 2000, 14, 779–793. [Google Scholar] [CrossRef]
- Breshears, J.; Sharma, M.; Anderson, N.R.; Rashid, S.; Leuthardt, E.C. Electrocorticographic frequency alteration mapping of speech cortex during an awake craniotomy: Case report. Stereotact. Funct. Neurosurg. 2010, 88, 11–15. [Google Scholar] [CrossRef] [Green Version]
- Bresson, D.; Madadaki, C.; Poisson, I.; Habas, C.; Mandonnet, E. Functionally tailored transcortical approach of deep-seated lesions: An alternative to the transulcal approach? A technical case report. Neurochirurgie 2013, 59, 159–162. [Google Scholar] [CrossRef]
- Chang, E.F.; Wang, D.D.; Perry, D.W.; Barbaro, N.M.; Berger, M.S. Homotopic organization of essential language sites in right and bilateral cerebral hemispheric dominance: Clinical article. J. Neurosurg. 2011, 114, 893–902. [Google Scholar] [CrossRef]
- Chan-Seng, E.; Moritz-Gasser, S.; Duffau, H. Awake mapping for low-grade gliomas involving the left sagittal stratum: Anatomofunctional and surgical considerations: Clinical article. J. Neurosurg. 2014, 120, 1069–1077. [Google Scholar] [CrossRef]
- De Benedictis, A.; Moritz-Gasser, S.; Duffau, H. Awake mapping optimizes the extent of resection for low-grade gliomas in eloquent areas. Neurosurgery 2010, 66, 1074–1084. [Google Scholar] [CrossRef] [PubMed]
- De Benedictis, A.; Sarubbo, S.; Duffau, H. Subcortical surgical anatomy of the lateral frontal region: Human white matter dissection and correlations with functional insights provided by intraoperative direct brain stimulation: Laboratory investigation. J. Neurosurg. 2012, 117, 1053–1069. [Google Scholar] [CrossRef]
- De Witte, E.; Satoer, D.; Colle, H.; Robert, E.; Visch-Brink, E.; Mariën, P. Subcortical language and non-language mapping in awake brain surgery: The use of multimodal tests. Acta Neurochir. 2015, 157, 577–588. [Google Scholar] [CrossRef]
- Duffau, H.; Bauchet, L.; Lehéricy, S.; Capelle, L. Functional compensation of the left dominant insula for language. NeuroReport 2001, 12, 2159–2163. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H.; Capelle, L.; Denvil, D.; Gatignol, P.; Sichez, N.; Lopes, M.; Sichez, J.P.; Van Effenterre, R. The role of dominant premotor cortex in language: A study using intraoperative functional mapping in awake patients. NeuroImage 2003, 20, 1903–1914. [Google Scholar] [CrossRef]
- Duffau, H.; Capelle, L.; Denvil, D.; Sichez, N.; Gatignol, P.; Lopes, M.; Mitchell, M.-C.; Sichez, J.-P.; Van Effenterre, R. Functional recovery after surgical resection of low grade gliomas in eloquent brain: Hypothesis of brain compensation. J. Neurol. Neurosurg. Psychiatry 2003, 74, 901–907. [Google Scholar] [CrossRef] [Green Version]
- Duffau, H.; Denvil, D.; Lopes, M.; Gasparini, F.; Cohen, L.; Capelle, L.; van Effenterre, R. Intraoperative mapping of the cortical areas involved in multiplication and subtraction: An electrostimulation study in a patient with a left parietal glioma. J. Neurol. Neurosurg. Psychiatry 2002, 73, 733–738. [Google Scholar] [CrossRef] [Green Version]
- Duffau, H.; Gatignol, P.; Denvil, D.; Lopes, M.; Capelle, L. The articulatory loop: Study of the subcortical connectivity by electrostimulation. Neuroreport 2003, 14, 2005–2008. [Google Scholar] [CrossRef]
- Duffau, H.; Gatignol, P.; Moritz-Gasser, S.; Mandonnet, E. Is the left uncinate fasciculus essential for language?: AA cerebral stimulation study. J. Neurol. 2009, 256, 382–389. [Google Scholar] [CrossRef]
- Duffau, H.; Leroy, M.; Gatignol, P. Cortico-subcortical organization of language networks in the right hemisphere: An electrostimulation study in left-handers. Neuropsychologia 2008, 46, 3197–3209. [Google Scholar] [CrossRef] [PubMed]
- Gatignol, P.; Capelle, L.; Le Bihan, R.; Duffau, H. Double dissociation between picture naming and comprehension: An electrostimulation study. NeuroReport 2004, 15, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Gil-Robles, S.; Carvallo, A.; Jimenez, M.D.M.; Gomez Caicoya, A.; Martinez, R.; Ruiz-Ocaña, C.; Duffau, H. Double dissociation between visual recognition and picture naming: A study of the visual language connectivity using tractography and brain stimulation. Neurosurgery 2013, 72, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Gonen, T.; Gazit, T.; Korn, A.; Kirschner, A.; Perry, D.; Hendler, T.; Ram, Z. Intra-operative multi-site stimulation: Expanding methodology for cortical brain mapping of language functions. PLoS ONE 2017, 12, e0180740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gras-Combe, G.; Moritz-Gasser, S.; Herbet, G.; Duffau, H. Intraoperative subcortical electrical mapping of optic radiations in awake surgery for glioma involving visual pathways. J. Neurosurg. 2012, 117, 466–473. [Google Scholar] [CrossRef]
- Hamer, P.C.D.W.; Moritz-Gasser, S. Is the human left middle longitudinal fascicle essential for language? A brain electrostimulation study. Hum. Brain Mapp. 2011, 32, 962–973. [Google Scholar] [CrossRef]
- Herbet, G.; Lafargue, G.; Almairac, F.; Moritz-Gasser, S.; Bonnetblanc, F.; Duffau, H. Disrupting the right pars opercularis with electrical stimulation frees the song: Case report. J. Neurosurg. 2015, 123, 1401–1404. [Google Scholar] [CrossRef] [Green Version]
- Herbet, G.; Moritz-Gasser, S.; Duffau, H. Direct evidence for the contributive role of the right inferior fronto-occipital fasciculus in non-verbal semantic cognition. Brain Struct. Funct. 2017, 222, 1597–1610. [Google Scholar] [CrossRef]
- Hiroshima, S.; Anei, R.; Murakami, N.; Kamada, K. Functional localization of the supplementary motor area. Neurol. Med.-Chir. 2014, 54, 511–520. [Google Scholar] [CrossRef] [Green Version]
- Huang, M.; Baskin, D.S.; Fung, S. Glioblastoma Presenting with Pure Alexia and Palinopsia Involving the Left Inferior Occipital Gyrus and Visual Word Form Area Evaluated with Functional Magnetic Resonance Imaging and Diffusion Tensor Imaging Tractography. World Neurosurg. 2016, 89, 725.e5–725.e10. [Google Scholar] [CrossRef]
- Joswig, H.; Bratelj, D.; Brunner, T.; Jacomet, A. Awake Craniotomy: First-Year Experiences and Patient Perception; Elsevier: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Kamada, K.; Todo, T.; Masutani, Y.; Aoki, S.; Ino, K.; Morita, A.; Saito, N. Visualization of the frontotemporal language fibers by tractography combined with functional magnetic resonance imaging and magnetoencephalography. J. Neurosurg. 2007, 106, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Kemerdere, R.; de Champfleur, N.M.; Deverdun, J.; Cochereau, J.; Moritz-Gasser, S.; Herbet, G.; Duffau, H. Role of the left frontal aslant tract in stuttering: A brain stimulation and tractographic study. J. Neurol. 2016, 263, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, M.; de Champfleur, N.M.; Deverdun, J.; Moritz-Gasser, S.; Herbet, G.; Duffau, H. Role of fronto-striatal tract and frontal aslant tract in movement and speech: An axonal mapping study. Brain Struct. Funct. 2015, 220, 3399–3412. [Google Scholar] [CrossRef] [PubMed]
- Kurimoto, M.; Takaiwa, A.; Nagai, S.; Hayashi, N.; Endo, S. Anomia for people’s names after left anterior temporal lobe resection-Case report. Neurol. Med.-Chir. 2010, 50, 36–40. [Google Scholar] [CrossRef] [Green Version]
- Lang, F.F.; Olansen, N.E.; Demonte, F.; Gokaslan, Z.L.; Holland, E.C.; Kalhorn, C.; Sawaya, R. Surgical resection of intrinsic insular tumors: Complication avoidance. J. Neurosurg. 2001, 95, 638–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.T.; Faltermeier, C.; Morshed, R.A.; Young, J.S.; Kakaizada, S.; Valdivia, C.; Berger, M.S. The impact of high functional connectivity network hub resection on language task performance in adult low- and high-grade glioma. J. Neurosurg. 2020, 134, 1102–1112. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Wu, J.; Yao, C.; Zhuang, D.; Qiu, T.; Hu, X.; Zhang, J.; Gong, X.; Liang, W.; Mao, Y.; et al. Awake language mapping and 3-Tesla intraoperative MRI-guided volumetric resection for gliomas in language areas. J. Clin. Neurosci. 2013, 20, 1280–1287. [Google Scholar] [CrossRef] [PubMed]
- Magrassi, L.; Bongetta, D.; Bianchini, S.; Berardesca, M.; Arienta, C. Central and peripheral components of writing critically depend on a defined area of the dominant superior parietal gyrus. Brain Res. 2010, 1346, 145–154. [Google Scholar] [CrossRef]
- Maldonado, I.L.; Moritz-Gasser, S.; Duffau, H. Does the left superior longitudinal fascicle subserve language semantics? A brain electrostimulation study. Brain Struct. Funct. 2011, 216, 263–274. [Google Scholar] [CrossRef]
- Mandonnet, E.; De Witt Hamer, P.; Poisson, I.; Whittle, I.; Bernat, A.L.; Bresson, D.; Madaki, C.; Bouazza, S.; Ursu, R.; Carpentier, A.F.; et al. Initial experience using awake surgery for glioma: Oncological, functional, and employment outcomes in a consecutive series of 25 cases. Neurosurgery 2015, 76, 382–389. [Google Scholar] [CrossRef]
- Martino, J.; de Lucas, E.M.; Ibanez-Plagaro, F.J.; Valle-Folgueral, J.M.; Vazquez-Barquero, A. Foix-Chavany-Marie syndrome caused by a disconnection between the right pars opercularis of the inferior frontal gyrus and the supplementary motor area. J. Neurosurg. 2012, 117, 844–850. [Google Scholar] [CrossRef]
- Matsuda, R.; Moritz-Gasser, S.; Duvaux, S.; Fernández Coello, A.; Martinoni, M.; Duffau, H. The persistent crucial role of the left hemisphere for language in left-handers with a left low grade glioma: A stimulation mapping study. Acta Neurochir. 2014, 156, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Moritz-Gasser, S.; Herbet, G.; Duffau, H. Mapping the connectivity underlying multimodal (verbal and non-verbal) semantic processing: A brain electrostimulation study. Neuropsychologia 2013, 51, 1814–1822. [Google Scholar] [CrossRef] [PubMed]
- Motomura, K.; Chalise, L.; Ohka, F.; Aoki, K.; Tanahashi, K.; Hirano, M.; Nishikawa, T.; Wakabayashi, T.; Natsume, A. Supratotal Resection of Diffuse Frontal Lower Grade Gliomas with Awake Brain Mapping, Preserving Motor, Language, and Neurocognitive Functions. World Neurosurg. 2018, 119, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Motomura, K.; Chalise, L.; Ohka, F.; Aoki, K.; Tanahashi, K.; Hirano, M.; Nishikawa, T.; Yamaguchi, J.; Shimizu, H.; Wakabayashi, T.; et al. Neurocognitive and functional outcomes in patients with diffuse frontal lower-grade gliomas undergoing intraoperative awake brain mapping. J. Neurosurg. 2019, 132, 1–9. [Google Scholar] [CrossRef]
- Motomura, K.; Fujii, M.; Maesawa, S.; Kuramitsu, S.; Natsume, A.; Wakabayashi, T. Association of dorsal inferior frontooccipital fasciculus fibers in the deep parietal lobe with both reading and writing processes: A brain mapping study. J. Neurosurg. 2014, 121, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Mukae, N.; Mizoguchi, M.; Mori, M.; Hashiguchi, K.; Kawaguchi, M.; Hata, N.; Amano, T.; Nakamizo, A.; Yoshimoto, K.; Sayama, T.; et al. The usefulness of arcuate fasciculus tractography integrated navigation for glioma surgery near the language area; Clinical Investigation. Interdiscip. Neurosurg. Adv. Tech. Case Manag. 2017, 7, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Nomura, K.; Kazui, H.; Tokunaga, H.; Hirata, M.; Goto, T.; Goto, Y.; Hashimoto, N.; Yoshimine, T.; Takeda, M. Possible roles of the dominant uncinate fasciculus in naming objects: A case report of intraoperative electrical stimulation on a patient with a brain tumour. Behav. Neurol. 2013, 27, 229–234. [Google Scholar] [CrossRef]
- Ogawa, H.; Kamada, K.; Kapeller, C.; Hiroshima, S.; Prueckl, R.; Guger, C. Rapid and minimum invasive functional brain mapping by real-time visualization of high gamma activity during awake craniotomy. World Neurosurg. 2014, 82, 912.e1–912.e10. [Google Scholar] [CrossRef]
- Pallud, J.; Dezamis, E. Functional and oncological outcomes following awake surgical resection using intraoperative cortico-subcortical functional mapping for supratentorial gliomas located in eloquent areas. Neurochirurgie 2017, 63, 208–218. [Google Scholar] [CrossRef]
- Pallud, J.; Roux, A.; Mellerio, C. Glioma Resection Unmasks Eloquent Brain Areas. World Neurosurg. 2019, 132, 251–252. [Google Scholar] [CrossRef]
- Petrovich, N.M.; Holodny, A.I. Isolated translocation of Wernicke’s area to the right hemisphere in a 2004, 62-year-man with a temporo-parietal glioma. Am. J. Neuroradiol. 2004, 25, 130–133. [Google Scholar] [PubMed]
- Plaza, M.; Gatignol, P.; Leroy, M.; Duffau, H. Speaking without Broca’s area after tumor resection. Neurocase 2009, 15, 294–310. [Google Scholar] [CrossRef]
- Rech, F.; Duffau, H.; Pinelli, C.; Masson, A.; Roublot, P.; Billy-Jacques, A.; Civit, T. Intraoperative identification of the negative motor network during awake surgery to prevent deficit following brain resection in premotor regions. Neurochirurgie 2017, 63, 235–242. [Google Scholar] [CrossRef]
- Rech, F.; Herbet, G.; Moritz-Gasser, S.; Duffau, H. Somatotopic organization of the white matter tracts underpinning motor control in humans: An electrical stimulation study. Brain Struct. Funct. 2016, 221, 3743–3753. [Google Scholar] [CrossRef] [PubMed]
- Ribas, E.S.C.; Duffau, H. Permanent anosmia and ageusia after resection of a left temporoinsular low-grade glioma: Anatomofunctional considerations-Case report. J. Neurosurg. 2012, 116, 1007–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robles, S.G.; Gatignol, P.; Capelle, L.; Mitchell, M.C.; Duffau, H. The role of dominant striatum in language: A study using intraoperative electrical stimulations. J. Neurol. Neurosurg. Psychiatry 2005, 76, 940–946. [Google Scholar] [CrossRef] [Green Version]
- Rofes, A.; Spena, G.; Talacchi, A.; Santini, B.; Miozzo, A.; Miceli, G. Mapping nouns and finite verbs in left hemisphere tumors: A direct electrical stimulation study. Neurocase 2017, 23, 105–113. [Google Scholar] [CrossRef]
- Ruge, M.I.; Victor, J.; Hosain, S.; Correa, D.D. Concordance between functional magnetic resonance imaging and intraoperative language mapping. Ster. Funct. Neurosurg. 1999, 72, 95–102. [Google Scholar] [CrossRef]
- Saito, T.; Muragaki, Y.; Maruyama, T.; Tamura, M.; Nitta, M.; Tsuzuki, S.; Konishi, Y.; Kamata, K.; Kinno, R.; Sakai, K.L.; et al. Difficulty in identification of the frontal language area in patients with dominant frontal gliomas that involve the pars triangularis. J. Neurosurg. 2016, 125, 803–811. [Google Scholar] [CrossRef] [Green Version]
- Saito, T.; Tamura, M.; Muragaki, Y.; Maruyama, T.; Kubota, Y.; Fukuchi, S.; Nitta, M.; Chernov, M.; Okamoto, S.; Sugiyama, K.; et al. Intraoperative cortico-cortical evoked potentials for the evaluation of language function during brain tumor resection: Initial experience with 13 cases. J. Neurosurg. 2014, 121, 827–838. [Google Scholar] [CrossRef]
- Sakurada, K.; Sato, S.; Sonoda, Y.; Kokubo, Y.; Saito, S.; Kayama, T. Surgical resection of tumors located in subcortex of language area. Acta Neurochir. 2007, 149, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Sarubbo, S.; Bars, E.L.; Sylvie, M.G.; Duffau, H.; Sarubbo, S. Complete recovery after surgical resection of left Wernicke’s area in awake patient: A brain stimulation and functional MRI study. Neurosurg. Rev. 2012, 35, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Sarubbo, S.; Latini, F.; Panajia, A.; Candela, C. Awake Surgery in Low-Grade Gliomas Harboring Eloquent Areas: 3-Year Mean Follow-Up; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Sarubbo, S.; Latini, F.; Sette, E.; Milani, P.; Granieri, E.; Fainardi, E.; Cavallo, M.A. Is the resection of gliomas in Wernicke’s area reliable? Wernicke’s area resection. Acta Neurochir. 2012, 154, 1653–1662. [Google Scholar] [CrossRef]
- Schapiro, R.; Ferson, D.; Prabhu, S.; Tummula, S.; Wefel, J.; Rao, G. A Technique for Mapping Cortical Areas Associated with Speech Arrest. Stereotact Funct Neurosurg. 2012, 90, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Sierpowska, J.; Gabarrós, A.; Fernandez-Coello, A.; Camins, À.; Castañer, S.; Juncadella, M.; Morís, J.; Rodríguez-Fornells, A. Words are not enough: Nonword repetition as an indicator of arcuate fasciculus integrity during brain tumor resection. J. Neurosurg. 2017, 126, 435–445. [Google Scholar] [CrossRef] [Green Version]
- Sierpowska, J.; Gabarrós, A.; Fernandez-Coello, A.; Camins, T.; Castañer, S.; Juncadella, M.; De Diego-Balaguer, R.; Rodríguez-Fornells, A. Morphological derivation overflow as a result of disruption of the left frontal aslant white matter tract. Brain Lang 2015, 142, 54–64. [Google Scholar] [CrossRef]
- Spena, G.; Costi, E.; Panciani, P.P.; Roca, E.; Migliorati, K.; Fontanella, M.M. Acute functional reactivation of the language network during awake intraoperative brain mapping. Neurocase 2015, 21, 403–407. [Google Scholar] [CrossRef]
- Suess, O.; Picht, T.; Kuehn, B.; Mularski, S.; Brock, M.; Kombos, T. Neuronavigation without rigid pin fixation of the head in left frontotemporal tumor surgery with intraoperative speech mapping. Neurosurgery 2007, 60, 330–338, discussion 338. [Google Scholar] [CrossRef]
- Kumabe, T.; Nakasato, N.; Suzuki, K.; Sato, K.; Sonoda, Y.; Kawagishi, J.; Yoshimoto, T. Two-staged Resection of a Left Frontal Astrocytoma Involving the Operculum and Insula Using Intraoperative Neurophysiological Monitoring—Case Report. Neurol. Med.-Chir. 1998, 38, 503–507. [Google Scholar] [CrossRef] [Green Version]
- Tamura, Y.; Ogawa, H.; Kapeller, C.; Prueckl, R.; Takeuchi, F.; Anei, R.; Kamada, K. Passive language mapping combining real-time oscillation analysis with cortico-cortical evoked potentials for awake craniotomy. J. Neurosurg. 2016, 125, 1580–1588. [Google Scholar] [CrossRef]
- Tomasino, B.; Marin, D.; Maieron, M.; Agostini, S.D. A Multimodal Mapping Study of Conduction Aphasia with Impaired Repetition and Spared Reading Aloud; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar]
- van Geemen, K.; Herbet, G.; Moritz-Gasser, S.; Duffau, H. Limited plastic potential of the left ventral premotor cortex in speech articulation: Evidence From intraoperative awake mapping in glioma patients. Hum. Brain Mapp. 2014, 35, 1587–1596. [Google Scholar] [CrossRef]
- Vassal, F.; Boutet, C.; Lemaire, J.J. New insights into the functional significance of the frontal aslant tract: An anatomo–functional study using intraoperative electrical stimulations combined with diffusion tensor imaging-based fiber tracking. Br. J. Neurosurg. 2014, 28, 685–687. [Google Scholar] [CrossRef]
- Vassal, M.; Le Bars, E.; Moritz-Gasser, S.; Menjot, N.; Duffau, H. Crossed aphasia elicited by intraoperative cortical and subcortical stimulation in awake patients: Clinical article. J. Neurosurg. 2010, 113, 1251–1258. [Google Scholar] [CrossRef]
- Vidorreta, J.G.; Garcia, R.; Moritz-Gasser, S.; Duffau, H. Double dissociation between syntactic gender and picture naming processing: A brain stimulation mapping study. Hum. Brain Mapp. 2011, 32, 331–340. [Google Scholar] [CrossRef]
- Whittle, I.R.; Borthwick, S.; Haq, N. Brain dysfunction following ‘awake’ craniotomy, brain mapping and resection of glioma. Br. J. Neurosurg. 2003, 17, 130–137. [Google Scholar] [CrossRef]
- Wilden, J.A.; Voorhies, J.; Mosier, K.M.; O’Neill, D.P.; Cohen-Gadol, A.A. Strategies to maximize resection of complex, or high surgical risk, low-grade gliomas. Neurosurg. Focus 2013, 34, E5. [Google Scholar] [CrossRef] [Green Version]
- Yamao, Y.; Matsumoto, R.; Kunieda, T.; Arakawa, Y.; Kobayashi, K.; Usami, K.; Shibata, S.; Kikuchi, T.; Sawamoto, N.; Mikuni, N.; et al. Intraoperative dorsal language network mapping by using single-pulse electrical stimulation. Hum. Brain Mapp. 2014, 35, 4345–4361. [Google Scholar] [CrossRef] [Green Version]
- Zammar, S.G.; Specht, C.S.; Zacharia, B.E. Crossed Aphasia as a Manifestation of Glioblastoma. 2018. Available online: Ncbi.nlm.nih.gov (accessed on 17 October 2022).
- Zemmoura, I.; Herbet, G.; Moritz-Gasser, S.; Duffau, H. New insights into the neural network mediating reading processes provided by cortico-subcortical electrical mapping. Hum. Brain Mapp. 2015, 36, 2215–2230. [Google Scholar] [CrossRef]
- Finch, E.; Copland, D.A. Language outcomes following neurosurgery for brain tumours: A systematic review. NeuroRehabilitation 2014, 34, 499–514. [Google Scholar] [CrossRef]
- Satoer, D.; Visch-Brink, E.; Dirven, C.; Vincent, A. Glioma surgery in eloquent areas: Can we preserve cognition? Acta Neurochir. 2016, 158, 35–50. [Google Scholar] [CrossRef]
- Papagno, C.; Gallucci, M.; Casarotti, A.; Castellano, A.; Falini, A.; Fava, E.; Caramazza, A. Connectivity constraints on cortical reorganization of neural circuits involved in object naming. Neuroimage 2011, 55, 1306–1313. [Google Scholar] [CrossRef]
- Binder, J.R.; Desai, R.H.; Graves, W.W.; Conant, L.L. Where is the semantic system? A critical review and meta-analysis of 120 functional neuroimaging studies. Cereb. Cortex 2009, 19, 2767–2796. [Google Scholar] [CrossRef]
- Chang, E.F.; Raygor, K.P.; Berger, M.S. Contemporary model of language organization: An overview for neurosurgeons. J. Neurosurg. 2015, 122, 250–261. [Google Scholar] [CrossRef] [Green Version]
- Mandonnet, E.; Sarubbo, S.; Duffau, H. Proposal of an optimized strategy for intraoperative testing of speech and language during awake mapping. Neurosurg. Rev. 2017, 40, 29–35. [Google Scholar] [CrossRef]
- Satoer, D.; Witte, E.D.; Dragoy, O. Spontaneous Speech. In Intraoperative Mapping of Cognitive Networks; Springer: Cham, Switzerland, 2021; pp. 95–114. [Google Scholar]
- Costello, A.L.; Warrington, E.K. Dynamic aphasia: The selective impairment of verbal planning. Cortex 1989, 25, 103–114. [Google Scholar] [CrossRef]
- Satoer, D.; Vincent, A.; Smits, M.; Dirven, C.; Visch-Brink, E. Spontaneous speech of patients with gliomas in eloquent areas before and early after surgery. Acta Neurochir. 2013, 155, 685–692. [Google Scholar] [CrossRef]
- Chernoff, B.L.; Sims, M.H.; Smith, S.O.; Pilcher, W.H.; Mahon, B.Z. Direct electrical stimulation of the left frontal aslant tract disrupts sentence planning without affecting articulation. Cogn. Neuropsychol. 2019, 36, 178–192. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No | Speech and Language Errors | No | Speech and Language Errors |
|---|---|---|---|
| 1 | Anomia or word-finding difficulties | 4 | Semantic errors |
| Anomia | Non-speech semantic processing problem | ||
| Circumlocutions | Semantic association disturbance or error | ||
| Naming delay or delayed word retrieval | Semantic comprehension error | ||
| Word-finding, searching or retrieval difficulties | Semantic disorder, deficit or aphasia | ||
| 2 | Phonemic errors | Semantic disturbance or error | |
| Phonemic disturbance | Semantic jargon aphasic language | ||
| Phonemic paraphasias in writing | Semantic paraphasias in writing | ||
| Phonemic speech error or paraphasia | Semantic speech error or paraphasia | ||
| Phonological paraphasia | 5 | Speech arrest | |
| Phonological processing or disturbance | 6 | Other errors | |
| 3 | Production errors | Comprehension errors * | |
| Anarthria | Irrelevant paraphasia | ||
| Articulatory difficulty | Morpho-syntactic errors * | ||
| Dysarthria | Neologism | ||
| Hesitation | Perseveration | ||
| Slow speech | Reading errors * | ||
| Slurred speech | Speech initiation difficulties * | ||
| Speech delay | Speech apraxia | ||
| Stammering | Writing errors * | ||
| Stuttering |
| Language Outcome Categories | Language Outcome Categories |
|---|---|
| 1.A. Linguistic modality | 1.B. Aphasia syndrome |
| Comprehension | Broca, motor, or expressive aphasia |
| Production | Conduction aphasia |
| Reading | - |
| 2.A. Linguistic level | 2.B. Other |
| Phonology | Articulation |
| Semantics | Spontaneous speech * |
| Morpho-syntax | Speech apraxia |
| - | Word finding |
| Information from Incluced Articles | All Articles |
|---|---|
| Total articles | 81 |
| Total errors | 631 |
| Number of awake patients in articles (range) | 1–107 |
| Tumor Grade | |
| Low grade | 452 |
| High grade | 118 |
| Not stated | 61 |
| Tumor Location: Hemisphere | |
| Left | 552 |
| Right | 75 |
| Not stated | 4 |
| Tumor Location: Lobe | |
| Frontal | 256 |
| Parietal | 57 |
| Temporal | 87 |
| Occipital | 3 |
| Insular | 32 |
| Combination | 196 |
| Individual Error | Error Category | Absolute Number | Percentage |
|---|---|---|---|
| Anomia | Anomia | 132 | 20.9% |
| Speech arrest | Speech arrest | 132 | 20.9% |
| Production errors | Production errors | 124 | 19.7% |
| Semantic errors | Semantic errors | 88 | 13.9% |
| Phonemic errors | Phonemic errors | 76 | 12.0% |
| Perseveration | Other errors | 23 | 3.6% |
| Reading errors | Other errors | 20 | 3.2% |
| Morpho-syntactic errors | Other errors | 15 | 1.1% |
| Writing errors | Other errors | 7 | 0.8% |
| Speech initiation difficulties | Other errors | 5 | 0.8% |
| Comprehension errors | Other errors | 5 | 0.8% |
| Irrelevant paraphasia | Other errors | 2 | 0.3% |
| Neologism | Other errors | 1 | 0.2% |
| Speech apraxia | Other errors | 1 | 0.2% |
| (Possible) Predictors | T1 | T3 | ||||
|---|---|---|---|---|---|---|
| B (95% CI) | S.E. | Exp (B) | B (95% CI) | S.E. | Exp (B) | |
| Pre deficits (yes) | 1.231 ** (2.101–5.580) | 0.249 | 3.424 | 0.669 * (1.202–3.167) | 0.247 | 1.951 |
| Pre deficits (unknown) | −0.530 (0.346–1.002) | 0.271 | 0.589 | −1.704 * (0.042–0.781) | 0.744 | 0.182 |
| Intra anomia | 0.738 * (1.154–3.791) | 0.303 | 2.092 | 0.614 (0.873–3.914) | 0.383 | 1.848 |
| Intra phonemic errors | 0.381 (0.754–2.840) | 0.338 | 1.463 | 0.540 (0.741–3.973) | 0.428 | 1.716 |
| Intra production errors | 0.722 * (1.141–3.716) | 0.301 | 2.059 | -0.192 (0.363–1.875) | 0.419 | 0.825 |
| Intra semantic errors | 0.332 (0.731–2.657) | 0.329 | 1.394 | −0.098 (0.376–2.190) | 0.450 | 0.907 |
| Intra other errors | 0.064 (0.542–2.097) | 0.345 | 1.066 | 0.545 (0.723–4.114) | 0.444 | 1.725 |
| Constant | 0.385 | 0.213 | 1.470 | −1.783 | 0.327 | 0.168 |
| Postoperative Language Deficits | Intraoperative Speech and Language Errors | |||||
|---|---|---|---|---|---|---|
| Anomia | Phonemic Errors | Production Errors | Semantic Errors | Speech Arrest | Total | |
| By linguistic modality or aphasia syndrome | ||||||
| Production | 46 | 22 | 73 | 23 | 41 | 205 |
| Comprehension | 3 | 3 | 0 | 3 | 4 | 13 |
| Reading | 16 | 8 | 1 | 7 | 8 | 40 |
| Conduction aphasia | 3 | 5 | 2 | 0 | 2 | 12 |
| Broca’s aphasia | 3 | 0 | 9 | 0 | 10 | 22 |
| Total | 71 | 38 | 85 | 33 | 65 | 292 |
| By linguistic level or other level | ||||||
| Articulation | 6 | 3 | 18 | 2 | 9 | 38 |
| Morpho-syntax | 3 | 3 | 0 | 6 | 5 | 17 |
| Phonology | 0 | 5 | 3 | 1 | 0 | 9 |
| Semantics | 2 | 1 | 5 | 7 | 0 | 15 |
| Spontaneous speech | 12 | 8 | 10 | 2 | 9 | 41 |
| Speech apraxia | 0 | 0 | 2 | 2 | 0 | 4 |
| Word finding | 1 | 1 | 2 | 1 | 4 | 9 |
| Total | 24 | 21 | 40 | 21 | 27 | 133 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collée, E.; Vincent, A.; Dirven, C.; Satoer, D. Speech and Language Errors during Awake Brain Surgery and Postoperative Language Outcome in Glioma Patients: A Systematic Review. Cancers 2022, 14, 5466. https://doi.org/10.3390/cancers14215466
Collée E, Vincent A, Dirven C, Satoer D. Speech and Language Errors during Awake Brain Surgery and Postoperative Language Outcome in Glioma Patients: A Systematic Review. Cancers. 2022; 14(21):5466. https://doi.org/10.3390/cancers14215466
Chicago/Turabian StyleCollée, Ellen, Arnaud Vincent, Clemens Dirven, and Djaina Satoer. 2022. "Speech and Language Errors during Awake Brain Surgery and Postoperative Language Outcome in Glioma Patients: A Systematic Review" Cancers 14, no. 21: 5466. https://doi.org/10.3390/cancers14215466
APA StyleCollée, E., Vincent, A., Dirven, C., & Satoer, D. (2022). Speech and Language Errors during Awake Brain Surgery and Postoperative Language Outcome in Glioma Patients: A Systematic Review. Cancers, 14(21), 5466. https://doi.org/10.3390/cancers14215466