
Conversion Strategy in Left-Sided RAS/BRAF Wild-Type Metastatic Colorectal Cancer Patients with Unresectable Liver-Limited Disease: A Multicenter Cohort Study

 , ,
, ,  , , , ,
, , , ,  ,
,  , , ,
, , ,  ,
,  ,
,  and add
Show full author list
and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics of the Sample
3.2. Primary Endpoint
3.3. Secondary Endpoints
4. Discussion
Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jegatheeswaran, S.; Mason, J.M.; Hancock, H.C.; Siriwardena, A.K. The liver-first approach to the management of colorectal cancer with synchronous hepatic metastases: A systematic review. JAMA Surg. 2013, 148, 385–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Velde, C.J.H. Treatment of liver metastases of colorectal cancer. Ann. Oncol. 2005, 16, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Associazione Italiana Oncologia Medica (AIOM). Linee Guida TUMORI DEL COLON. 2020. Available online: https://www.aiom.it/wp-content/uploads/2020/10/2020_LG_AIOM_Colon.pdf (accessed on 30 June 2022).
- Arnold, D.; Lueza, B.; Douillard, J.-Y.; Peeters, M.; Lenz, H.-J.; Venook, A.; Heinemann, V.; Van Cutsem, E.; Pignon, J.-P.; Tabernero, J.; et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann. Oncol. 2017, 28, 1713–1729. [Google Scholar] [CrossRef] [PubMed]
- Parisi, A.; Porzio, G.; Cannita, K.; Venditti, O.; Avallone, A.; Filippi, R.; Salvatore, L.; Tortora, G.; Ribelli, M.; Nigro, O.; et al. Clinicians’ Attitude to Doublet Plus Anti-EGFR Versus Triplet Plus Bevacizumab as First-line Treatment in Left-Sided RAS and BRAF Wild-Type Metastatic Colorectal Cancer Patients: A Multicenter, “Real-Life”, Case-Control Study. Clin. Colorectal Cancer 2021, 20, 318–325. [Google Scholar] [CrossRef]
- Parisi, A.; Ghidini, M.; Giampieri, R.; Tomasello, G.; Luciani, A.; Ferri, C.; Berardi, R.; Petrelli, F. Post-induction Strategies in Metastatic Colorectal Cancer Patients Treated with First-Line Anti-EGFR-Based Treatment: A Systematic Review and Meta-Analysis. Clin. Colorectal Cancer 2022, 21, 162–170. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. NCCN Guidelines for Colon Cancer. JNCCN J. Natl. Compr. Cancer Netw. 2021, 19. [Google Scholar] [CrossRef]
- Wang, L.; Sun, Y.; Zhao, B.; Zhang, H.; Yu, Q.; Yuan, X. Chemotherapy plus targeted drugs in conversion therapy for potentially resectable colorectal liver metastases: A metaanalysis. Oncotarget 2016, 7, 55732–55740. [Google Scholar] [CrossRef] [Green Version]
- Ye, L.C.; Liu, T.S.; Ren, L.; Wei, Y.; Zhu, D.X.; Zai, S.Y.; Ye, Q.H.; Yu, Y.; Xu, B.; Qin, X.Y.; et al. Randomized controlled trial of cetuximab plus chemotherapy for patients with KRAS wild-type unresectable colorectal liver-limited metastases. J. Clin. Oncol. 2013, 31, 1931–1938. [Google Scholar] [CrossRef] [Green Version]
- Falcone, A.; Ricci, S.; Brunetti, I.; Pfanner, E.; Allegrine, G.; Barbara, C.; Crinò, L.; Benedetti, G.; Evangelista, W.; Fanchini, L.; et al. Phase III trial of infusional fluorouracil, leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) compared with infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI) as first-line treatment for metastatic colorectal cancer: The gruppo oncologico nord ovest. J. Clin. Oncol. 2007, 25, 1670–1676. [Google Scholar] [CrossRef]
- Cremolini, C.; Casagrande, M.; Loupakis, F.; Aprile, G.; Bergamo, F.; Masi, G.; Moretto, R.R.; Pietrantonio, F.; Marmorino, F.; Zucchelli, G.; et al. Efficacy of FOLFOXIRI plus bevacizumab in liver-limited metastatic colorectal cancer: A pooled analysis of clinical studies by Gruppo Oncologico del Nord Ovest. Eur. J. Cancer 2017, 73, 74–84. [Google Scholar] [CrossRef]
- Tomasello, G.; Petrelli, F.; Ghidini, M.; Russo, A.; Passalacqua, R.; Barni, S. FOLFOXIRI plus bevacizumab as conversion therapy for patients with initially unresectable metastatic colorectal cancer: A systematic review and pooled analysis. JAMA Oncol. 2017, 3, e170278. [Google Scholar] [CrossRef]
- Adam, R.; Delvart, V.; Pascal, G.; Valeanu, A.; Castaing, D.; Azoulay, D.; Giacchetti, S.; Paule, B.; Kunstlinger, F.; Ghémard, O.; et al. Rescue surgery for unresectable colorectal liver metastases downstaged by chemotherapy: A model to predict long-term survival. Ann. Surg. 2004, 240, 644–658. [Google Scholar] [CrossRef]
- Charnsangavej, C.; Clary, B.; Fong, Y.; Grothey, A.; Pawlik, T.M.; Choti, M.A. Selection of patients for resection of hepatic colorectal metastases: Expert consensus statement. Ann. Surg. Oncol. 2006, 13, 1261–1268. [Google Scholar] [CrossRef]
- Kaczirek, K. ASCO 2016—Update colorectal liver metastases. Memo Mag. Eur. Med. Oncol. 2017, 10, 103–105. [Google Scholar] [CrossRef] [Green Version]
- González, H.D.; Figueras, J. Practical questions in liver metastases of colorectal cancer: General principles of treatment. HPB 2007, 9, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Bittoni, A.; Scartozzi, M.; Giampieri, R.; Faloppi, L.; Maccaroni, E.; Del Prete, M.; Bianconi, M.; Cascinu, S. The Tower of Babel of liver metastases from colorectal cancer: Are we ready for one language? Crit. Rev. Oncol. Hematol. 2013, 85, 332–341. [Google Scholar] [CrossRef]
- Adam, R.; De Gramont, A.; Figueras, J.; Guthrie, A.; Kokudo, N.; Kunstlinger, F.; Loyer, E.; Poston, G.; Rougier, P.; Rubbia-Brandt, L.; et al. The Oncosurgery Approach to Managing Liver Metastases from Colorectal Cancer: A Multidisciplinary International Consensus. Oncologist 2012, 17, 1225–1239. [Google Scholar] [CrossRef] [Green Version]
- Fong, Y.; Fortner, J.; Sun, R.L.; Brennan, M.F.; Blumgart, L.H. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: Analysis of 1001 consecutive cases. Ann. Surg. 1999, 230, 309. [Google Scholar] [CrossRef]
- Adam, R.; de Gramont, A.; Figueras, J.; Kokudo, N.; Kunstlinger, F.; Loyer, E.; Poston, G.; Rougier, P.; Rubbia-Brandt, L.; Sobrero, A.; et al. Managing synchronous liver metastases from colorectal cancer: A multidisciplinary international consensus. Cancer Treat. Rev. 2015, 41, 729–741. [Google Scholar] [CrossRef]
- Reddy, S.K.; Barbas, A.S.; Turley, R.S.; Steel, J.L.; Tsung, A.; Marsh, J.W.; Geller, D.A.; Clary, B.M. A standard definition of major hepatectomy: Resection of four or more liver segments. HPB 2011, 13, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bridgewater, J.A.; Pugh, S.A.; Maishman, T.; Eminton, Z.; Mellor, J.; Whitehead, A.; Stanton, L.; Radford, M.; Corkhill, A.; Griffiths, G.O.; et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis (New EPOC): Long-term results of a multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 398–411. [Google Scholar] [CrossRef]
- Douillard, J.Y.; Siena, S.; Cassidy, J.; Tabernero, J.; Burkes, R.; Barugel, M.; Humblet, Y.; Bodoky, G.; Cunningham, D.; Jassem, J.; et al. Randomized, Phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) Versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: The PRIME study. J. Clin. Oncol. 2010, 28, 4697–4705. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Köhne, C.-H.; Hitre, E.; Zaluski, J.; Chang Chien, C.-R.; Makhson, A.; D’Haens, G.; Pintér, T.; Lim, R.; Bodoky, G.; et al. Cetuximab and Chemotherapy as Initial Treatment for Metastatic Colorectal Cancer. N. Engl. J. Med. 2009, 360, 1408–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, R.; Avisar, E.; Ariche, A.; Giachetti, S.; Azoulay, D.; Castaing, D.; Kunstlinger, F.; Levi, F.; Bismuth, F. Five-year survival following hepatic resection after neoadjuvant therapy for nonresectable colorectal [liver] metastases. Ann. Surg. Oncol. 2001, 8, 347–353. [Google Scholar] [CrossRef]
- Rivera, F.; Karthaus, M.; Hecht, J.R.; Sevilla, I.; Forget, F.; Fasola, G.; Canon, J.L.; Guan, X.; Demonty, G.; Schwartzberg, L.S. Final analysis of the randomised PEAK trial: Overall survival and tumour responses during first-line treatment with mFOLFOX6 plus either panitumumab or bevacizumab in patients with metastatic colorectal carcinoma. Int. J. Colorectal Dis. 2017, 32, 1179–1190. [Google Scholar] [CrossRef] [Green Version]
- Oki, E.; Emi, Y.; Yamanaka, T.; Uetake, H.; Muro, K.; Takahashi, T.; Nagasaka, T.; Hatano, E.; Ojima, H.; Manaka, D.; et al. Randomised phase II trial of mFOLFOX6 plus bevacizumab versus mFOLFOX6 plus cetuximab as first-line treatment for colorectal liver metastasis (ATOM trial). Br. J. Cancer 2019, 121, 222–229. [Google Scholar] [CrossRef] [Green Version]
- Tang, W.; Ren, L.; Liu, T.; Ye, Q.; Wei, Y.; He, G.; Lin, Q.; Wang, X.; Wang, M.; Liang, F.; et al. Bevacizumab plus mFOLFOX6 versus mFOLFOX6 alone as first-line treatment for RAS mutant unresectable colorectal liver-limited metastases: The BECOME randomized controlled trial. J. Clin. Oncol. 2020, 38, 3175–3184. [Google Scholar] [CrossRef]
- Schmoll, H.; Garlipp, B.; Junghanß, C.; Vogel, A.; Kaiser, U.; Florschütz, A.; Kanzler, S.; Hannig, C.; Meinert, F.; Cygon, F.; et al. FOLFOX/bevacizumab +/- irinotecan in advanced colorectal cancer (CHARTA): Long term outcome. Ann. Oncol. 2018, 29, v108. [Google Scholar] [CrossRef]
- Gruenberger, T.; Bridgewater, J.; Chau, I.; García Alfonso, P.; Rivoire, M.; Mudan, S.; Lasserre, S.; Hermann, F.; Waterkamp, D.; Adam, R. Bevacizumab plus mFOLFOX-6 or FOLFOXIRI in patients with initially unresectable liver metastases from colorectal cancer: The OLIVIA multinational randomised phase II trial. Ann. Oncol. 2015, 26, 702–708. [Google Scholar] [CrossRef]
- Hurwitz, H.I.; Tan, B.R.; Reeves, J.A.; Xiong, H.; Somer, B.; Lenz, H.-J.; Hochster, H.S.; Scappaticci, F.; Palma, J.F.; Price, R.; et al. Phase II Randomized Trial of Sequential or Concurrent FOLFOXIRI-Bevacizumab Versus FOLFOX-Bevacizumab for Metastatic Colorectal Cancer (STEAM). Oncologist 2019, 24, 921–932. [Google Scholar] [CrossRef] [Green Version]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- Cremolini, C.; Antoniotti, C.; Rossini, D.; Lonardi, S.; Loupakis, F.; Pietrantonio, F.; Bordonaro, R.; Latiano, T.P.; Tamburini, E.; Santini, D.; et al. Upfront FOLFOXIRI plus bevacizumab and reintroduction after progression versus mFOLFOX6 plus bevacizumab followed by FOLFIRI plus bevacizumab in the treatment of patients with metastatic colorectal cancer (TRIBE2): A multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol. 2020, 21, 497–507. [Google Scholar] [CrossRef]
- Villard, C.; Habib, M.; Nordenvall, C.; Nilsson, P.J.; Jorns, C.; Sparrelid, E. Conversion therapy in patients with colorectal liver metastases. Eur. J. Surg. Oncol. 2021, 47, 2038–2045. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Guidelines Version 1.2022 Colon Cancer. 2022. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1428 (accessed on 28 July 2022).
- Margonis, G.A.; Sasaki, K.; Gholami, S.; Kim, Y.; Andreatos, N.; Rezaee, N.; Deshwar, A.; Buettner, S.; Allen, P.J.; Kingham, T.P.; et al. Genetic And Morphological Evaluation (GAME) score for patients with colorectal liver metastases. Br. J. Surg. 2018, 105, 1210–1220. [Google Scholar] [CrossRef]
- Chen, Y.; Chang, W.; Ren, L.; Chen, J.; Tang, W.; Liu, T.; Jian, M.; Liu, Y.; Wei, Y.; Xu, J. Comprehensive Evaluation of Relapse Risk (CERR) Score for Colorectal Liver Metastases: Development and Validation. Oncologist 2020, 25, e1031–e1041. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, V.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.-E.; Heintges, T.; Lerchenmüller, C.; Kahl, C.; Seipelt, G.; et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): A randomised, open-label, phase 3 trial. Lancet Oncol. 2014, 15, 1065–1075. [Google Scholar] [CrossRef]
- Venook, A.P.; Niedzwiecki, D.; Innocenti, F.; Fruth, B.; Greene, C.; O’Neil, B.H.; Shaw, J.E.; Atkins, J.N.; Horvath, L.E.; Polite, B.N.; et al. Impact of primary (1o) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts) with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). J. Clin. Oncol. 2016, 34, 3504. [Google Scholar] [CrossRef]
- Yahagi, M.; Okabayashi, K.; Hasegawa, H.; Tsuruta, M.; Kitagawa, Y. The Worse Prognosis of Right-Sided Compared with Left-Sided Colon Cancers: A Systematic Review and Meta-analysis. J. Gastrointest. Surg. 2016, 20, 648–655. [Google Scholar] [CrossRef]
- Wang, F.; Bai, L.; Liu, T.S.; Yu, Y.Y.; He, M.M.; Liu, K.Y.; Luo, H.Y.; Zhang, D.S.; Jin, Y.; Wang, F.H.; et al. Right- and left-sided colorectal cancers respond differently to cetuximab. Chin. J. Cancer 2015, 34, 24. [Google Scholar] [CrossRef]
- Engstrand, J.; Kartalis, N.; Strömberg, C.; Broberg, M.; Stillström, A.; Lekberg, T.; Jonas, E.; Freedman, J.; Nilsson, H. The Impact of a Hepatobiliary Multidisciplinary Team Assessment in Patients with Colorectal Cancer Liver Metastases: A Population-Based Study. Oncologist 2017, 22, 1067–1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, Y.T.; Jiang, J.K.; Chang, S.C.; Yang, S.H.; Lin, C.C.; Lin, H.H.; Wang, H.S.; Chen, W.S.; Lin, T.C.; Lin, J.K. Improved outcomes of colorectal cancer patients with liver metastases in the era of the multidisciplinary teams. Int. J. Colorectal Dis. 2016, 31, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Wei, A.C.; Jarnagin, W.R. Questioning Why More Patients with Colorectal Liver Metastases Are Not Referred for Metastasectomy. JAMA Surg. 2020, 155, 909. [Google Scholar] [CrossRef] [PubMed]
- Dueland, S.; Grut, H.; Syversveen, T.; Hagness, M.; Line, P.D. Selection criteria related to long-term survival following liver transplantation for colorectal liver metastasis. Am. J. Transplant. 2020, 20, 530–537. [Google Scholar] [CrossRef] [Green Version]
- Dueland, S.; Smedman, T.M.; Røsok, B.; Grut, H.; Syversveen, T.; Jørgensen, L.H.; Line, P.D. Treatment of relapse and survival outcomes after liver transplantation in patients with colorectal liver metastases. Transpl. Int. 2021, 34, 2213–2250. [Google Scholar] [CrossRef]
- Varley, R.; Tarazi, M.; Davé, M.; Mobarak, S.; Stott, M.C.; Baltatzis, M.; Satyadas, T. Liver Transplantation for Non-Resectable Liver Metastases from Colorectal Cancer: A Systematic Review and Meta-Analysis. World J. Surg. 2021, 45, 3404–3413. [Google Scholar] [CrossRef]
- Bonney, G.K.; Chew, C.A.; Lodge, P.; Hubbard, J.; Halazun, K.J.; Trunecka, P.; Muiesan, P.; Mirza, D.F.; Isaac, J.; Laing, R.W.; et al. Liver transplantation for non-resectable colorectal liver metastases: The International Hepato-Pancreato-Biliary Association consensus guidelines. Lancet Gastroenterol. Hepatol. 2021, 6, 933–946. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Induction ST not Leading to Surgery (n = 176) N (%) | Ultimately Resectable (n = 56) N (%) | Potentially Resectable (n = 40) N (%) | Total (n = 272) N (%) | p |
|---|---|---|---|---|---|
| Age (median/IQR) | 65 (57.3–72.7) | 62 (52.8–70.7) | 62.5 (57.2–69.7) | 64 (56–71) | 0.34 |
| Male gender | 110 (62.5) | 46 (81.1) † | 29 (72.5) | 185 (68.0) | 0.03 |
| Site of primary tumor (rectum) | 54 (30.7) | 21 (38.9) | 17 (44.7) | 92 (34.3) | 0.186 |
| Histology (mucinous) | 31 (18.5) | 3 (5.7) | 7 (18.4) | 41 (15.8) | 0.075 |
| Grading | 0.63 | ||||
| G1 | 7 (5.0) | 1 (2.1) | 1 (3.2) | 9 (4.1) | |
| G2 | 96 (68.1) | 38 (79.2) | 21 (67.7) | 155 (70.5) | |
| G3 | 38 (27.0) | 9 (18.8) | 9 (29.0) | 56 (25.5) | |
| Primary tumor resected | 115 (65.7) | 52 (96.3) † | 36 (94.7) ‡ | 203 (76.0) | <0.001 |
| N+ | 65 (36.9) ^⁑ | 10 (18.5) | 5 (13.2) | 80 (29.9) | 0.002 |
| N° of liver metastases at diagnosis | <0.001 | ||||
| 1 | 9 (5.1) | 5 (8.9) | 10 (25.0) ‡ | 24 (8.8) | |
| 2–5 | 57 (32.4) | 28 (50.0) | 22 (55.5) ‡ | 107 (39.3) | |
| 6–10 | 32 (18.2) | 9 (16.1) | 3 (7.5) | 44 (16.2) | |
| >10 | 59 (33.5) ⁑ | 13 (23.2) | 4 (10) | 76 (27.9) | |
| Synchronous disease | 150 (85.2) | 45 (80.4) | 28 (70.0) | 223 (82.0) | 0.073 |
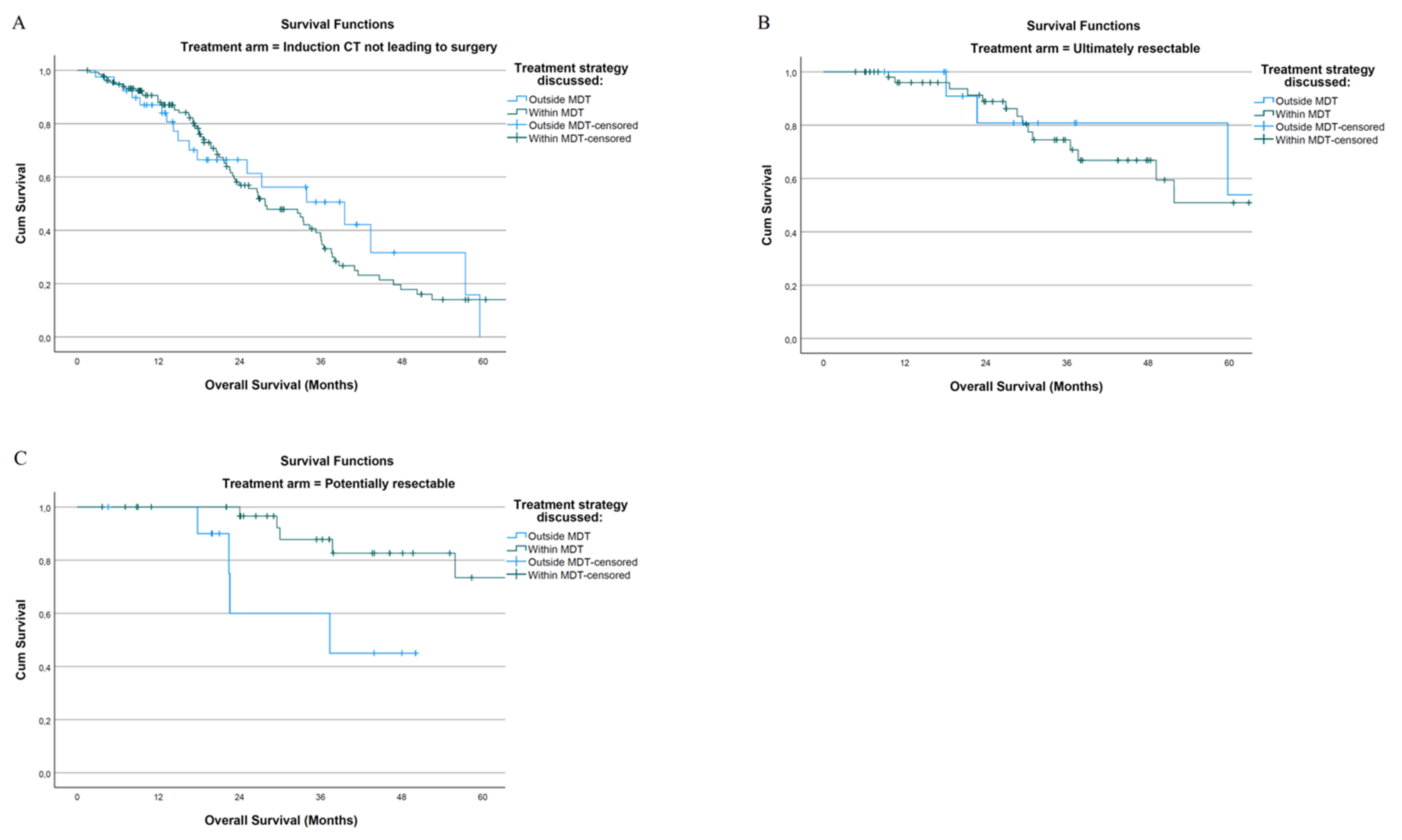
| Treatment approach discussed at MDT | 136 (77.3) | 43 (76.8) | 32 (80) | 211 (77.6) | 0.921 |
| ECOG 0 | 103 (58.5) | 40 (71.4) | 31 (32.3) | 171 (63.8) | 0.089 |
| CEA at baseline (>100 ng/mL) | 60 (37.5) ⁑ | 15 (30) | 4 (12.1) | 79 (32.5) | 0.016 |
| HER-2 status | 0.069 | ||||
| Not amplified | 25 (14.2) | 15 (27.8) | 3 (7.8) | 43 (16) | |
| Amplified | 3 (1.7) | 1 (1.9) | 0 | 4 (1.5) | |
| Not evaluated | 148 (84.1) | 38 (70.4) | 35 (92.1) | 221 (82.5) | |
| N° of criteria for biologically challenging disease (median/IQR) | 3 (2–3) | 2 (2–3) | 2 (2–3) | 2 (2–3) | 0.075 |
| Major liver resection | - | 30 (56.6) | 13 (34.2) | 43 (44.8) | 0.038 |
| R0 resection | - | 39 (78) | 34 (89.5) | 73 (76.0) | 0.293 |
| ST regimen | 0.49 | ||||
| FOLFIRI + Cetuximab | 71 (40.3) | 21 (37.5) | 20 (51.3) | 112 (41.5) | |
| FOLFOX + Cetuximab | 23 (13.1) | 5 (8.9) | 2 (5.1) | 30 (11.1) | |
| FOLFIRI + Panitumumab | 12 (6.8) | 3 (5.4) | 1 (2.6) | 16 (5.9) | |
| FOLFOX + Panitumumab | 70 (39.8) | 27 (48.2) | 15 (38.5) | 112 (41.5) | |
| Number of ST cycles administered before surgical resection (median/IQR) | 5 (1.5–10.5) | 8 (6–12) | 6 (0–8) | 7 (5–10) | 0.002 * |
| 3 months PFS | 167 (94.9) | 56 (100) | 40 (100) | 263 (96.7) | 0.083 |
| 6 months PFS | 138 (78.4) | 54 (98.2) † | 37 (97.4) ‡ | 229 (85.1) | <0.001 |
| 10 months PFS | 95 (54.0) | 46 (83.6) † | 34 (89.5) ‡ | 175 (65.1) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granieri, S.; Cotsoglou, C.; Bonomi, A.; Salvatore, L.; Filippi, R.; Nigro, O.; Gelsomino, F.; Zurlo, I.V.; Depetris, I.; Giampieri, R.; et al. Conversion Strategy in Left-Sided RAS/BRAF Wild-Type Metastatic Colorectal Cancer Patients with Unresectable Liver-Limited Disease: A Multicenter Cohort Study. Cancers 2022, 14, 5513. https://doi.org/10.3390/cancers14225513
Granieri S, Cotsoglou C, Bonomi A, Salvatore L, Filippi R, Nigro O, Gelsomino F, Zurlo IV, Depetris I, Giampieri R, et al. Conversion Strategy in Left-Sided RAS/BRAF Wild-Type Metastatic Colorectal Cancer Patients with Unresectable Liver-Limited Disease: A Multicenter Cohort Study. Cancers. 2022; 14(22):5513. https://doi.org/10.3390/cancers14225513
Chicago/Turabian StyleGranieri, Stefano, Christian Cotsoglou, Alessandro Bonomi, Lisa Salvatore, Roberto Filippi, Olga Nigro, Fabio Gelsomino, Ina Valeria Zurlo, Ilaria Depetris, Riccardo Giampieri, and et al. 2022. "Conversion Strategy in Left-Sided RAS/BRAF Wild-Type Metastatic Colorectal Cancer Patients with Unresectable Liver-Limited Disease: A Multicenter Cohort Study" Cancers 14, no. 22: 5513. https://doi.org/10.3390/cancers14225513
APA StyleGranieri, S., Cotsoglou, C., Bonomi, A., Salvatore, L., Filippi, R., Nigro, O., Gelsomino, F., Zurlo, I. V., Depetris, I., Giampieri, R., Berardi, R., Morelli, C., De Tursi, M., Roberto, M., Gjoni, E., Germini, A., de Angelis, N., Memeo, R., Facciorusso, A., ... Parisi, A. (2022). Conversion Strategy in Left-Sided RAS/BRAF Wild-Type Metastatic Colorectal Cancer Patients with Unresectable Liver-Limited Disease: A Multicenter Cohort Study. Cancers, 14(22), 5513. https://doi.org/10.3390/cancers14225513