

Differences in Cancer-Specific Mortality after Trimodal Therapy for T2N0M0 Bladder Cancer according to Histological Subtype
 , ,
, ,  , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analyses
3. Results
3.1. Descriptive Characteristics of the Study Population
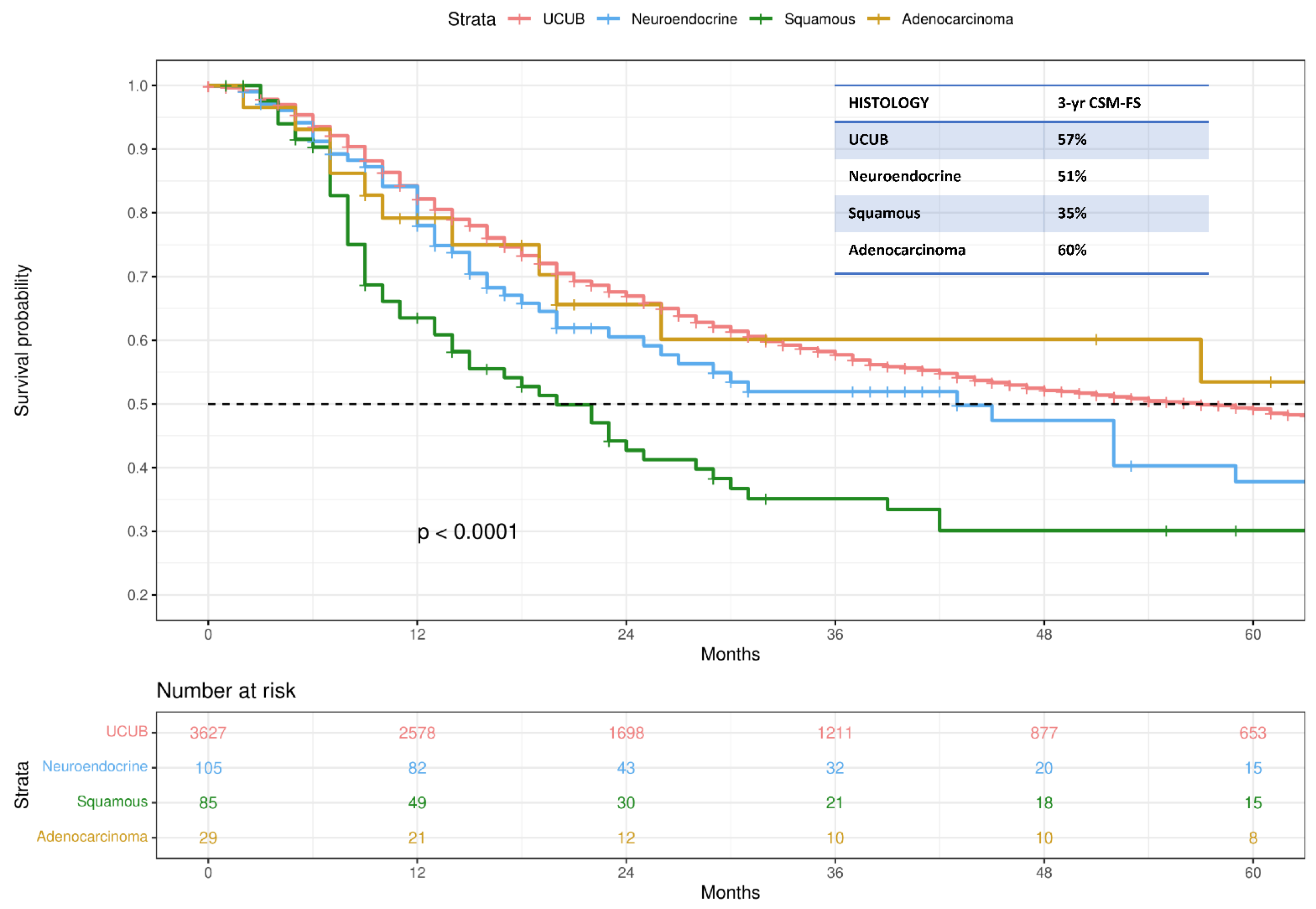
3.2. Kaplan–Meier Analyses Assessing CSM-Free Survival
3.3. Multivariable Cox Regression Models Predicting CSM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Witjes, C.A.; Bruins, H.M.; Cathomas, R. Guideline: Muscle-invasive and Metastatic Bladder Cancer. Eur. Assoc. Urol. 2016, 34, 1945–1952. [Google Scholar]
- Shipley, W.U.; Prout, G.R.; Einstein, A.B.; Coombs, L.J.; Wajsman, Z.; Soloway, M.S.; Englander, L.; Barton, B.A.; Hafermann, M.D. Treatment of Invasive Bladder Cancer by Cisplatin and Radiation in Patients Unsuited for Surgery. JAMA J. Am. Med. Assoc. 1987, 258, 931–935. [Google Scholar] [CrossRef]
- Kulkarni, G.S.; Hermanns, T.; Wei, Y.; Bhindi, B.; Satkunasivam, R.; Athanasopoulos, P.; Bostrom, P.J.; Kuk, C.; Li, K.; Templeton, A.J.; et al. Propensity score analysis of radical cystectomy versus bladder-sparing trimodal therapy in the setting of a multidisciplinary bladder cancer clinic. J. Clin. Oncol. 2017, 35, 2299–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, R.H.; Hunt, D.; Shipley, W.U.; Efstathiou, J.A.; Tester, W.J.; Hagan, M.P.; Kaufman, D.S.; Heney, N.M.; Zietman, A.L. Long-term outcomes in patients with muscle-invasive bladder cancer after selective bladder-preserving combined-modality therapy: A pooled analysis of radiation therapy oncology group protocols 8802, 8903, 9506, 9706, 9906, and 0233. J. Clin. Oncol. 2014, 32, 3801–3809. [Google Scholar] [CrossRef] [PubMed]
- James, N.D.; Hussain, S.A.; Hall, E.; Jenkins, P.; Tremlett, J.; Rawlings, C.; Crundwell, M.; Sizer, B.; Sreenivasan, T.; Hendron, C.; et al. Radiotherapy with or without Chemotherapy in Muscle-Invasive Bladder Cancer. N. Engl. J. Med. 2012, 366, 1477–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacalone, N.J.; Shipley, W.U.; Clayman, R.H.; Niemierko, A.; Drumm, M.; Heney, N.M.; Michaelson, M.D.; Lee, R.J.; Saylor, P.J.; Wszolek, M.F.; et al. Long-term Outcomes After Bladder-preserving Tri-modality Therapy for Patients with Muscle-invasive Bladder Cancer: An Updated Analysis of the Massachusetts General Hospital Experience. Eur. Urol. 2017, 71, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Alanee, S.; Alvarado-Cabrero, I.; Murugan, P.; Kumar, R.; Nepple, K.G.; Paner, G.P.; Patel, M.I.; Raspollini, M.R.; Lopez-Beltran, A.; Konety, B.R. Update of the International Consultation on Urological Diseases on bladder cancer 2018: Non-urothelial cancers of the urinary bladder. World J. Urol. 2019, 37, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Veskimäe, E.; Espinos, E.L.; Bruins, H.M.; Yuan, Y.; Sylvester, R.; Kamat, A.M.; Shariat, S.F.; Witjes, J.A.; Compérat, E.M. What Is the Prognostic and Clinical Importance of Urothelial and Nonurothelial Histological Variants of Bladder Cancer in Predicting Oncological Outcomes in Patients with Muscle-invasive and Metastatic Bladder Cancer? A European Association of Urology Mus. Eur. Urol. Oncol. 2019, 2, 625–642. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.; Krapcho, M. Cancer Stat Rev n.d.:SEER Statistics. Available online: https://seer.cancer.gov/csr/1975_2018/ (accessed on 25 August 2022).
- Janopaul-Naylor, J.R.; Zhong, J.; Liu, Y.; Zhang, C.; Osunkoya, A.O.; Joshi, S.S.; Bilen, M.A.; Carthon, B.; Kucuk, O.; Hartsell, L.M.; et al. Clinical and Translational Radiation Oncology Bladder preserving chemoradiotherapy compared to surgery for variants of urothelial carcinoma and other tumors types involving the bladder: An analysis of the National Cancer Database. Clin. Transl. Radiat. Oncol. 2021, 26, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Fischer-Valuck, B.W.; Michalski, J.M.; Contreras, J.A.; Brenneman, R.; Christodouleas, J.P.; Abraham, C.D.; Kim, E.H.; Arora, V.K.; Bullock, A.D.; Carmona, R.; et al. Clinical and Translational Radiation Oncology Short Communication A propensity analysis comparing definitive chemo-radiotherapy for muscle-invasive squamous cell carcinoma of the bladder vs. urothelial carcinoma of the bladder using the National Cancer D. Clin. Transl. Radiat. Oncol. 2019, 15, 38–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krasnow, R.E.; Drumm, M.; Roberts, H.J.; Niemierko, A.; Wu, C.L.; Wu, S.; Zhang, J.; Heney, N.M.; Wszolek, M.F.; Blute, M.L.; et al. Clinical Outcomes of Patients with Histologic Variants of Urothelial Cancer Treated with Trimodality Bladder-sparing Therapy. Eur. Urol. 2017, 72, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Bandini, M.; Pederzoli, F.; Madison, R.; Briganti, A.; Ross, J.S.; Niegisch, G.; Yu, E.Y.; Bamias, A.; Agarwal, N.; Sridhar, S.S.; et al. Unfavorable Cancer-specific Survival After Neoadjuvant Chemotherapy and Radical Cystectomy in Patients With Bladder Cancer and Squamous Cell Variant: A Multi-institutional Study. Clin. Genitourin. Cancer 2020, 18, e543–e556. [Google Scholar] [CrossRef] [PubMed]
- Vetterlein, M.W.; Wankowicz, S.A.M.; Seisen, T.; Lander, R.; Löppenberg, B.; Chun, F.K.; Menon, M.; Sun, M.; Barletta, J.A.; Choueiri, T.K.; et al. Neoadjuvant chemotherapy prior to radical cystectomy for muscle-invasive bladder cancer with variant histology. Cancer 2017, 123, 4346–4355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Necchi, A.; Raggi, D.; Gallina, A.; Madison, R.; Colecchia, M.; Lucianò, R.; Montironi, R.; Giannatempo, P.; Farè, E.; Pederzoli, F.; et al. Updated Results of PURE-01 with Preliminary Activity of Neoadjuvant Pembrolizumab in Patients with Muscle-invasive Bladder Carcinoma with Variant Histologies. Eur. Urol. 2019, 77, 447–448. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Overall (n = 3846) |
|---|---|
| Age at diagnosis (years) | |
| Median | 77 |
| IQR | 70–83 |
| Histology | |
| Urothelial Carcinoma | 3627 (94.3) |
| Neuroendocrine Carcinoma | 105 (2.7) |
| Squamous Cell Carcinoma | 85 (2.2) |
| Adenocarcinoma | 29 (0.8) |
| Grade | |
| Low grade | 113 (3) |
| High grade | 3733 (97) |
| Sex | |
| Male | 2842 (74) |
| Female | 1004 (26) |
| Tumor Site | |
| Trigone | 293 (7.7) |
| Dome | 201 (5.2) |
| Lateral wall | 871 (22.6) |
| Anterior wall | 139 (3.6) |
| Posterior wall | 328 (8.5) |
| Bladder neck | 139 (3.6) |
| Ureteral orifice | 76 (2) |
| Lateral-posterior wall | 585 (15.2) |
| NOS | 1214 (31.6) |
| Follow-up (months) | |
| Median | 21 |
| IQR | 10–46 |
| Predictors | HR (95%CI) | p-Value |
|---|---|---|
| Histology | ||
| Urothelial Carcinoma | Ref. | - |
| Neuroendocrine Carcinoma | 1.28 (0.96–1.7) | 0.09 |
| Squamous Cell Carcinoma | 1.98 (1.5–2.61) | <0.001 |
| Adenocarcinoma | 1.02 (0.58–1.8) | 0.9 |
| Age at diagnosis (years) | 1.02 (1.02–1.03) | <0.001 |
| Sex | ||
| Female | Ref. | - |
| Male | 0.88 (0.78–0.97) | 0.02 |
| Grade | ||
| Low grade | Ref. | - |
| High grade | 1.08 (0.82–1.42) | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barletta, F.; Tappero, S.; Panunzio, A.; Incesu, R.-B.; Cano Garcia, C.; Piccinelli, M.L.; Tian, Z.; Gandaglia, G.; Moschini, M.; Terrone, C.; et al. Differences in Cancer-Specific Mortality after Trimodal Therapy for T2N0M0 Bladder Cancer according to Histological Subtype. Cancers 2022, 14, 5766. https://doi.org/10.3390/cancers14235766
Barletta F, Tappero S, Panunzio A, Incesu R-B, Cano Garcia C, Piccinelli ML, Tian Z, Gandaglia G, Moschini M, Terrone C, et al. Differences in Cancer-Specific Mortality after Trimodal Therapy for T2N0M0 Bladder Cancer according to Histological Subtype. Cancers. 2022; 14(23):5766. https://doi.org/10.3390/cancers14235766
Chicago/Turabian StyleBarletta, Francesco, Stefano Tappero, Andrea Panunzio, Reha-Baris Incesu, Cristina Cano Garcia, Mattia Luca Piccinelli, Zhe Tian, Giorgio Gandaglia, Marco Moschini, Carlo Terrone, and et al. 2022. "Differences in Cancer-Specific Mortality after Trimodal Therapy for T2N0M0 Bladder Cancer according to Histological Subtype" Cancers 14, no. 23: 5766. https://doi.org/10.3390/cancers14235766
APA StyleBarletta, F., Tappero, S., Panunzio, A., Incesu, R. -B., Cano Garcia, C., Piccinelli, M. L., Tian, Z., Gandaglia, G., Moschini, M., Terrone, C., Antonelli, A., Tilki, D., Chun, F. K. H., de Cobelli, O., Saad, F., Shariat, S. F., Montorsi, F., Briganti, A., & Karakiewicz, P. I. (2022). Differences in Cancer-Specific Mortality after Trimodal Therapy for T2N0M0 Bladder Cancer according to Histological Subtype. Cancers, 14(23), 5766. https://doi.org/10.3390/cancers14235766