
Quality of Life after Risk-Reducing Hysterectomy for Endometrial Cancer Prevention: A Systematic Review

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection (Inclusion Criteria)
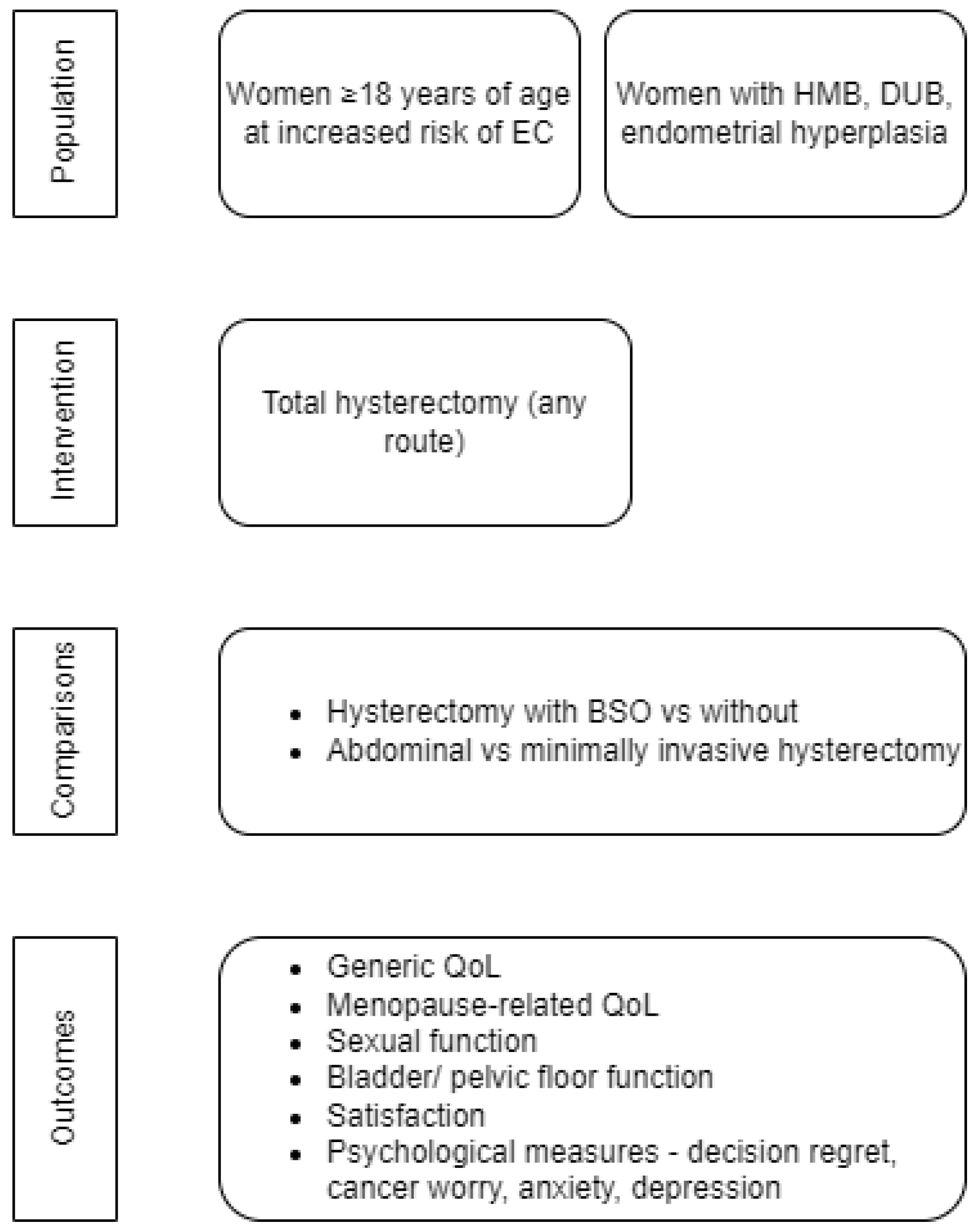
2.3. Using a Surrogate Population Model with Alternative Surgical Indication
2.4. Intervention
2.5. Comparators
2.6. Outcomes
2.7. Exclusion Criteria
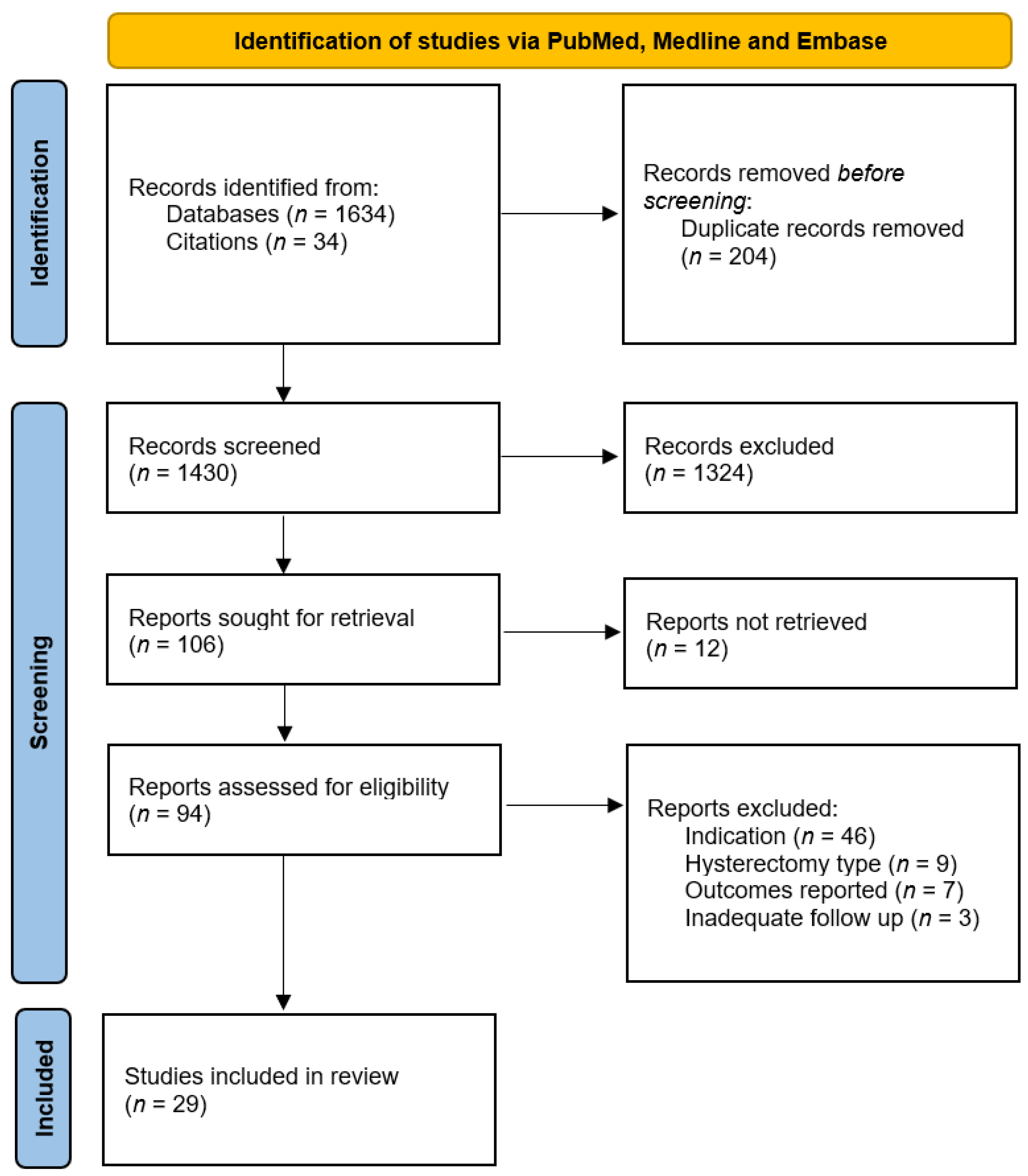
2.8. Screening of the Literature
2.9. Data Extraction
2.10. Quality Assessment
2.11. Analysis
2.12. Data accuracy and Availability
2.13. Ethical Approval
3. Results
3.1. Characteristics of Included Studies
3.2. Outcomes Reported
3.3. Quality Assessment
3.4. QoL following RRH
3.5. QoL following Hysterectomy as Treatment for Benign Disease
3.5.1. Hysterectomy Versus Hormonal Treatment
3.5.2. Comparison of Total vs. Subtotal Hysterectomy
3.5.3. Single Arm Cohort Studies
3.5.4. Hysterectomy Versus Endometrial Ablation or Resection
3.6. Comparison of Hysterectomy with BSO Versus without BSO
3.7. Comparison of Route of Hysterectomy
4. Discussion
4.1. Findings
4.2. Strengths and Weaknesses
4.3. Interpretation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Wehner, M.R.; Matrisian, L.M.; Nead, K.T. Estimated Projection of US Cancer Incidence and Death to 2040. JAMA Netw. Open 2021, 4, e214708. [Google Scholar] [CrossRef] [PubMed]
- Moller, P.; Seppala, T.T.; Bernstein, I.; Holinski-Feder, E.; Sala, P.; Gareth Evans, D.; Lindblom, A.; Macrae, F.; Blanco, I.; Sijmons, R.H.; et al. Cancer risk and survival in path_MMR carriers by gene and gender up to 75 years of age: A report from the Prospective Lynch Syndrome Database. Gut 2018, 67, 1306–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendricks, L.A.J.; Hoogerbrugge, N.; Schuurs-Hoeijmakers, J.H.M.; Vos, J.R. A review on age-related cancer risks in PTEN hamartoma tumor syndrome. Clin. Genet. 2021, 99, 219–225. [Google Scholar] [CrossRef]
- Johnatty, S.E.; Tan, Y.Y.; Buchanan, D.D.; Bowman, M.; Walters, R.J.; Obermair, A.; Quinn, M.A.; Blomfield, P.B.; Brand, A.; Leung, Y.; et al. Family history of cancer predicts endometrial cancer risk independently of Lynch Syndrome: Implications for genetic counselling. Gynecol. Oncol. 2017, 147, 381–387. [Google Scholar] [CrossRef]
- Bafligil, C.; Thompson, D.J.; Lophatananon, A.; Smith, M.J.; Ryan, N.A.; Naqvi, A.; Evans, D.G.; Crosbie, E.J. Association between genetic polymorphisms and endometrial cancer risk: A systematic review. J. Med. Genet. 2020, 57, 591–600. [Google Scholar] [CrossRef]
- Dalmartello, M.; Vermunt, J.; Negri, E.; Levi, F.; La Vecchia, C. Adult lifetime body mass index trajectories and endometrial cancer risk. BJOG 2021, 129, 1521–1529. [Google Scholar] [CrossRef]
- Saed, L.; Varse, F.; Baradaran, H.R.; Moradi, Y.; Khateri, S.; Friberg, E.; Khazaei, Z.; Gharahjeh, S.; Tehrani, S.; Sioofy-Khojine, A.B.; et al. The effect of diabetes on the risk of endometrial Cancer: An updated a systematic review and meta-analysis. BMC Cancer 2019, 19, 527. [Google Scholar] [CrossRef] [Green Version]
- Dossus, L.; Allen, N.; Kaaks, R.; Bakken, K.; Lund, E.; Tjonneland, A.; Olsen, A.; Overvad, K.; Clavel-Chapelon, F.; Fournier, A.; et al. Reproductive risk factors and endometrial cancer: The European Prospective Investigation into Cancer and Nutrition. Int. J. Cancer 2010, 127, 442–451. [Google Scholar] [CrossRef]
- Alblas, M.; Velt, K.B.; Pashayan, N.; Widschwendter, M.; Steyerberg, E.W.; Vergouwe, Y. Prediction models for endometrial cancer for the general population or symptomatic women: A systematic review. Crit. Rev. Oncol. Hematol. 2018, 126, 92–99. [Google Scholar] [CrossRef]
- Kitson, S.J.; Evans, D.G.; Crosbie, E.J. Identifying High-Risk Women for Endometrial Cancer Prevention Strategies: Proposal of an Endometrial Cancer Risk Prediction Model. Cancer Prev. Res. 2017, 10, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Sroczynski, G.; Gogollari, A.; Conrads-Frank, A.; Hallsson, L.R.; Pashayan, N.; Widschwendter, M.; Siebert, U. Cost-Effectiveness of Early Detection and Prevention Strategies for Endometrial Cancer-A Systematic Review. Cancers 2020, 12, 1874. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.D.; Silver, E.R.; Tan, S.X.; Hur, C.; Kastrinos, F. Cost-effectiveness Analysis of Genotype-Specific Surveillance and Preventive Strategies for Gynecologic Cancers Among Women with Lynch Syndrome. JAMA Netw Open 2021, 4, e2123616. [Google Scholar] [CrossRef] [PubMed]
- Crosbie, E.J.; Ryan, N.A.J.; Arends, M.J.; Bosse, T.; Burn, J.; Cornes, J.M.; Crawford, R.; Eccles, D.; Frayling, I.M.; Ghaem-Maghami, S.; et al. The Manchester International Consensus Group recommendations for the management of gynecological cancers in Lynch syndrome. Genet. Med. 2019, 21, 2390–2400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmeler, K.M.; Lynch, H.T.; Chen, L.-m.; Munsell, M.F.; Soliman, P.T.; Clark, M.B.; Daniels, M.S.; White, K.G.; Boyd-Rogers, S.G.; Conrad, P.G.; et al. Prophylactic Surgery to Reduce the Risk of Gynecologic Cancers in the Lynch Syndrome. N. Eng. J. Med. 2006, 354, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moller, P. Prospective Lynch Syndrome Database (PLSD)—Cumulative Risk for Cancer by Age, Genetic Variant, and Gender. Available online: http://www.lscarisk.org/ (accessed on 13 April 2019).
- Committee Opinion No 701: Choosing the Route of Hysterectomy for Benign Disease. Obstet Gynecol. 2017, 129, e155–e159. [CrossRef] [PubMed]
- Aarts, J.W.; Nieboer, T.E.; Johnson, N.; Tavender, E.; Garry, R.; Mol, B.W.; Kluivers, K.B. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst. Rev. 2015, 2015, CD003677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrison, J.; Balega, J.; Buckley, L.; Clamp, A.; Crosbie, E.; Drew, Y.; Durrant, L.; Forrest, J.; Fotopoulou, C.; Gajjar, K.; et al. British Gynaecological Cancer Society (BGCS) uterine cancer guidelines: Recommendations for practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 270, 50–89. [Google Scholar] [CrossRef] [PubMed]
- Madhvani, K.; Curnow, T.; Carpenter, T. Route of hysterectomy: A retrospective, cohort study in English NHS Hospitals from 2011 to 2017. BJOG 2019, 126, 795–802. [Google Scholar] [CrossRef]
- Clarke-Pearson, D.L.; Geller, E.J. Complications of hysterectomy. Obstet. Gynecol. 2013, 121, 654–673. [Google Scholar] [CrossRef]
- Fortin, C.; Hur, C.; Falcone, T. Impact of Laparoscopic Hysterectomy on Quality of Life. J. Minim. Invasive Gynecol. 2019, 26, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Hall, E.; Finch, A.; Jacobson, M.; Rosen, B.; Metcalfe, K.; Sun, P.; Narod, S.A.; Kotsopoulos, J. Effects of bilateral salpingo-oophorectomy on menopausal symptoms and sexual functioning among women with a BRCA1 or BRCA2 mutation. Gynecol. Oncol. 2019, 152, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Gaba, F.; Manchanda, R. Systematic review of acceptability, cardiovascular, neurological, bone health and HRT outcomes following risk reducing surgery in BRCA carriers. Best Pract. Res. Clin. Obstet. Gynaecol. 2020, 65, 46–65. [Google Scholar] [CrossRef] [PubMed]
- Manchanda, R.; Gaba, F.; Talaulikar, V.; Pundir, J.; Gessler, S.; Davies, M.; Menon, U.; Gynaecologists, R.C.o.O.a. Risk-Reducing Salpingo-Oophorectomy and the Use of Hormone Replacement Therapy Below the Age of Natural Menopause: Scientific Impact Paper No. 66. BJOG 2021, 129, e16–e34. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? Pharmacoeconomics 2016, 34, 645–649. [Google Scholar] [CrossRef]
- Rabin, R.; Charro, F.d. EQ-SD: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- NICE. NICE Health Technology Evaluations: The Manual; The National Institute for Health and Care Excellence: London, UK, 2022. [Google Scholar]
- Alblas, M.; Peterse, E.F.P.; Du, M.; Zauber, A.G.; Steyerberg, E.W.; van Leeuwen, N.; Lansdorp-Vogelaar, I. Cost-effectiveness of prophylactic hysterectomy in first-degree female relatives with Lynch syndrome of patients diagnosed with colorectal cancer in the United States: A microsimulation study. Cancer Med. 2021, 10, 6835–6844. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, R.; Keating, S.; Clancy, T. The impact of risk-reducing gynaecological surgery in premenopausal women at high risk of endometrial and ovarian cancer due to Lynch syndrome. Fam. Cancer 2015, 14, 51–60. [Google Scholar] [CrossRef]
- Etchegary, H.; Dicks, E.; Watkins, K.; Alani, S.; Dawson, L. Decisions about prophylactic gynecologic surgery: A qualitative study of the experience of female Lynch syndrome mutation carriers. Hered. Cancer Clin. Pract. 2015, 13, 10. [Google Scholar] [CrossRef]
- Etchegary, H.; Dicks, E.; Tamutis, L.; Dawson, L. Quality of life following prophylactic gynecological surgery: Experiences of female Lynch mutation carriers. Fam. Cancer 2018, 17, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Kalamo, M.H.; Mäenpää, J.U.; Seppälä, T.T.; Mecklin, J.P.; Huhtala, H.; Sorvettula, K.; Pylvänäinen, K.; Staff, S. Factors associated with decision-making on prophylactic hysterectomy and attitudes towards gynecological surveillance among women with Lynch syndrome (LS): A descriptive study. Fam. Cancer 2020, 19, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neis, K.J.; Zubke, W.; Fehr, M.; Römer, T.; Tamussino, K.; Nothacker, M. Hysterectomy for Benign Uterine Disease. Dtsch. Arztebl. Int. 2016, 113, 242–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ju, H.; Jones, M.; Mishra, G. The prevalence and risk factors of dysmenorrhea. Epidemiol. Rev. 2014, 36, 104–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitts, M.K.; Ferris, J.A.; Smith, A.M.; Shelley, J.M.; Richters, J. Prevalence and correlates of three types of pelvic pain in a nationally representative sample of Australian women. Med. J. Aust. 2008, 189, 138–143. [Google Scholar] [CrossRef]
- Santer, M.; Warner, P.; Wyke, S. A Scottish postal survey suggested that the prevailing clinical preoccupation with heavy periods does not reflect the epidemiology of reported symptoms and problems. J. Clin. Epidemiol. 2005, 58, 1206–1210. [Google Scholar] [CrossRef]
- Weissman, A.M.; Hartz, A.J.; Hansen, M.D.; Johnson, S.R. The natural history of primary dysmenorrhoea: A longitudinal study. BJOG 2004, 111, 345–352. [Google Scholar] [CrossRef]
- Abenhaim, H.A.; Harlow, B.L. Live births, cesarean sections and the development of menstrual abnormalities. Int. J. Gynaecol. Obstet. 2006, 92, 111–116. [Google Scholar] [CrossRef]
- Raffone, A.; Seracchioli, R.; Raimondo, D.; Maletta, M.; Travaglino, A.; Raimondo, I.; Giaquinto, I.; Orsini, B.; Insabato, L.; Pellicano, M.; et al. Prevalence of adenomyosis in endometrial cancer patients: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2021, 303, 47–53. [Google Scholar] [CrossRef]
- Rowlands, I.J.; Abbott, J.A.; Montgomery, G.W.; Hockey, R.; Rogers, P.; Mishra, G.D. Prevalence and incidence of endometriosis in Australian women: A data linkage cohort study. BJOG 2021, 128, 657–665. [Google Scholar] [CrossRef]
- Sanjida, S.; Obermair, A.; Gebski, V.; Armfield, N.; Janda, M. Long-term quality of life outcomes of women treated for early-stage endometrial cancer. Int. J. Gynecol. Cancer 2021, 31, 530–536. [Google Scholar] [CrossRef] [PubMed]
- NICE. Quality Appraisal Checklist—Qualitative Studies. Available online: https://www.nice.org.uk/process/pmg4/chapter/appendix-h-quality-appraisal-checklist-qualitative-studies (accessed on 23 August 2022).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 23 August 2022).
- Bofill Rodriguez, M.; Lethaby, A.; Fergusson, R.J. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2021, 2, CD000329. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, R.J.; Bofill Rodriguez, M.; Lethaby, A.; Farquhar, C. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2019, 8, CD000329. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, R.J.; Lethaby, A.; Shepperd, S.; Farquhar, C. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2013, CD000329. [Google Scholar] [CrossRef] [PubMed]
- Hidlebaugh, D.A. Cost and quality-of-life issues associated with different surgical therapies for the treatment of abnormal uterine bleeding. Obstet. Gynecol. Clin. N. Am. 2000, 27, 451–465. [Google Scholar] [CrossRef] [PubMed]
- Kershaw, V.; Hickey, I.; Wyld, L.; Jha, S. The impact of risk reducing bilateral salpingo-oophorectomy on sexual function in BRCA1/2 mutation carriers and women with Lynch syndrome: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reproduct. Biol. 2021, 265, 7–17. [Google Scholar] [CrossRef]
- Kluivers, K.B.; Johnson, N.P.; Chien, P.; Vierhout, M.E.; Bongers, M.; Mol, B.W. Comparison of laparoscopic and abdominal hysterectomy in terms of quality of life: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 136, 3–8. [Google Scholar] [CrossRef]
- Lethaby, A.; Ivanova, V.; Johnson, N.P. Total versus subtotal hysterectomy for benign gynaecological conditions. Cochrane Database Syst. Rev. 2006, 16, Cd004993. [Google Scholar] [CrossRef] [Green Version]
- Lethaby, A.; Shepperd, S.; Cooke, I.; Farquhar, C. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2000, 2, CD000329. [Google Scholar] [CrossRef]
- Marjoribanks, J.; Lethaby, A.; Farquhar, C. Surgery versus medical therapy for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2003, 2, Cd003855. [Google Scholar] [CrossRef]
- Marjoribanks, J.; Lethaby, A.; Farquhar, C. Surgery versus medical therapy for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2006, CD003855. [Google Scholar] [CrossRef]
- Marjoribanks, J.; Lethaby, A.; Farquhar, C. Surgery versus medical therapy for heavy menstrual bleeding. Cochrane Database Syst. Rev. 2016, 2016, CD003855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meston, C.M.; Bradford, A. A brief review of the factors influencing sexuality after hysterectomy. Sex. Relationsh. Ther. 2004, 19, 5–14. [Google Scholar] [CrossRef]
- Middleton, L.J.; Champaneria, R.; Daniels, J.P.; Bhattacharya, S.; Cooper, K.G.; Hilken, N.H.; O’Donovan, P.; Gannon, M.; Gray, R.; Khan, K.S.; et al. Hysterectomy, endometrial destruction, and levonorgestrel releasing intrauterine system (Mirena) for heavy menstrual bleeding: Systematic review and meta-analysis of data from individual patients. BMJ 2010, 341, c3929. [Google Scholar] [CrossRef] [Green Version]
- Pynnä, K.; Vuorela, P.; Lodenius, L.; Paavonen, J.; Roine, R.P.; Räsänen, P. Cost-effectiveness of hysterectomy for benign gynecological conditions: A systematic review. Acta Obstet. Gynecol. Scand. 2014, 93, 225–232. [Google Scholar] [CrossRef]
- van der Kooij, S.M.; Bipat, S.; Hehenkamp, W.J.; Ankum, W.M.; Reekers, J.A. Uterine artery embolization versus surgery in the treatment of symptomatic fibroids: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2011, 205, 317.e1–317.e18. [Google Scholar] [CrossRef]
- Vitale, S.G.; Ferrero, S.; Ciebiera, M.; Barra, F.; Török, P.; Tesarik, J.; Vilos, G.A.; Cianci, A. Hysteroscopic endometrial resection vs. hysterectomy for abnormal uterine bleeding: Impact on quality of life and sexuality. Evidence from a systematic review of randomized controlled trials. Curr. Opin. Obstet. Gynecol. 2020, 32, 159–165. [Google Scholar] [CrossRef]
- Hurskainen, R.; Teperi, J.; Rissanen, P.; Aalto, A.M.; Grenman, S.; Kivelä, A.; Kujansuu, E.; Vuorma, S.; Yliskoski, M.; Paavonen, J. Quality of life and cost-effectiveness of levonorgestrel-releasing intrauterine system versus hysterectomy for treatment of menorrhagia: A randomised trial. Lancet 2001, 357, 273–277. [Google Scholar] [CrossRef]
- Hurskainen, R.; Teperi, J.; Rissanen, P.; Aalto, A.M.; Grenman, S.; Kivelä, A.; Kujansuu, E.; Vuorma, S.; Yliskoski, M.; Paavonen, J. Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: Randomized trial 5-year follow-up. JAMA 2004, 291, 1456–1463. [Google Scholar] [CrossRef]
- Halmesmäki, K.; Hurskainen, R.; Tiitinen, A.; Teperi, J.; Grenman, S.; Kivelä, A.; Kujansuu, E.; Yliskoski, M.; Paavonen, J. A randomized controlled trial of hysterectomy or levonorgestrel-releasing intrauterine system in the treatment of menorrhagia-effect on FSH levels and menopausal symptoms. Hum. Reprod. 2004, 19, 378–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halmesmäki, K.; Hurskainen, R.; Teperi, J.; Grenman, S.; Kivelä, A.; Kujansuu, E.; Tuppurainen, M.; Yliskoski, M.; Vuorma, S.; Paavonen, J. The effect of hysterectomy or levonorgestrel-releasing intrauterine system on sexual functioning among women with menorrhagia: A 5-year randomised controlled trial. BJOG 2007, 114, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Heliövaara-Peippo, S.; Hurskainen, R.; Teperi, J.; Aalto, A.M.; Grénman, S.; Halmesmäki, K.; Jokela, M.; Kivelä, A.; Tomás, E.; Tuppurainen, M.; et al. Quality of life and costs of levonorgestrel-releasing intrauterine system or hysterectomy in the treatment of menorrhagia: A 10-year randomized controlled trial. Am. J. Obstet. Gynecol. 2013, 209, 535.e1–535.e14. [Google Scholar] [CrossRef] [PubMed]
- Kuppermann, M.; Varner, R.E.; Summitt, R.L.; Learman, L.A.; Ireland, C.; Vittinghoff, E.; Stewart, A.L.; Lin, F.; Richter, H.E.; Showstack, J.; et al. Effect of hysterectomy vs. medical treatment on health-related quality of life and sexual functioning: The medicine or surgery (Ms) randomized trial. JAMA 2004, 291, 1447–1455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adigüzel, C.; Seyfettinoğlu, S.; Aka Satar, D.; Arlier, S.; Eskimez, E.; Kaya, F.; Nazik, H. Evaluation of quality of life and cost-effectiveness of definitive surgery and the levonorgestrel intrauterine system as treatment options for heavy menstrual bleeding. Turk. J. Med. Sci. 2017, 47, 789–794. [Google Scholar] [CrossRef]
- Learman, L.A.; Summitt, R.L.; Varner, R.E.; McNeeley, S.G.; Goodman-Gruen, D.; Richter, H.E.; Lin, F.; Showstack, J.; Ireland, C.C.; Vittinghoff, E.; et al. A randomized comparison of total or supracervical hysterectomy: Surgical complications and clinical outcomes. Obstet. Gynecol. 2003, 102, 453–462. [Google Scholar] [CrossRef]
- Kuppermann, M.; Summitt, R.L.; Varner, R.E.; McNeeley, S.G.; Goodman-Gruen, D.; Learman, L.A.; Ireland, C.C.; Vittinghoff, E.; Lin, F.; Richter, H.E.; et al. Sexual functioning after total compared with supracervical hysterectomy: A randomized trial. Obstet. Gynecol. 2005, 105, 1309–1318. [Google Scholar] [CrossRef]
- Roberts, R.N.; Norman, B.P.; Harrison, C.G.; Heaton, N.R.; Law, J.K.; Wadehra, V.; Younger, H.M.; West, C.P. A medical audit and patient survey of hysterectomies performed for menstrual disorders. Scott. Med. J. 1996, 41, 44–46. [Google Scholar] [CrossRef]
- Brandsborg, B.; Dueholm, M.; Nikolajsen, L.; Kehlet, H.; Jensen, T.S. A prospective study of risk factors for pain persisting 4 months after hysterectomy. Clin. J. Pain 2009, 25, 263–268. [Google Scholar] [CrossRef]
- Till, S.R.; Schrepf, A.; Pierce, J.; Moser, S.; Kolarik, E.; Brummett, C.; As-Sanie, S. Sexual function after hysterectomy according to surgical indication: A prospective cohort study. Sex Health 2022, 19, 46–54. [Google Scholar] [CrossRef]
- Dwyer, N.; Hutton, J.; Stirrat, G.M. Randomised controlled trial comparing endometrial resection with abdominal hysterectomy for the surgical treatment of menorrhagia. Br. J. Obstet. Gynaecol. 1993, 100, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Sculpher, M.J.; Dwyer, N.; Byford, S.; Stirrat, G.M. Randomised trial comparing hysterectomy and transcervical endometrial resection: Effect on health related quality of life and costs two years after surgery. Br. J. Obstet. Gynaecol. 1996, 103, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Pinion, S.B.; Parkin, D.E.; Abramovich, D.R.; Naji, A.; Alexander, D.A.; Russell, I.T.; Kitchener, H.C. Randomised trial of hysterectomy, endometrial laser ablation, and transcervical endometrial resection for dysfunctional uterine bleeding. BMJ 1994, 309, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Alexander, D.A.; Naji, A.A.; Pinion, S.B.; Mollison, J.; Kitchener, H.C.; Parkin, D.E.; Abramovich, D.R.; Russell, I.T. Randomised trial comparing hysterectomy with endometrial ablation for dysfunctional uterine bleeding: Psychiatric and psychosocial aspects. BMJ 1996, 312, 280–284. [Google Scholar] [CrossRef] [Green Version]
- Aberdeen Endometrial Ablation Trials Group. A randomised trial of endometrial ablation versus hysterectomy for the treatment of dysfunctional uterine bleeding: Outcome at four years. Br. J. Obstet Gynaecol 1999, 106, 360–366. [Google Scholar] [CrossRef]
- O’Connor, H.; Broadbent, J.A.; Magos, A.L.; McPherson, K. Medical Research Council randomised trial of endometrial resection versus hysterectomy in management of menorrhagia. Lancet 1997, 349, 897–901. [Google Scholar] [CrossRef]
- Crosignani, P.G.; Vercellini, P.; Apolone, G.; De Giorgi, O.; Cortesi, I.; Meschia, M. Endometrial resection versus vaginal hysterectomy for menorrhagia: Long-term clinical and quality-of-life outcomes. Am. J. Obstet. Gynecol. 1997, 177, 95–101. [Google Scholar] [CrossRef]
- Tapper, A.M.; Heinonen, P.K. Comparison of hysteroscopic endometrial resection and laparoscopic assisted vaginal hysterectomy for the treatment of menorrhagia. Acta Obstet. Gynecol. Scand. 1998, 77, 78–82. [Google Scholar] [CrossRef]
- Tjarks, M.; Van Voorhis, B.J. Treatment of endometrial polyps. Obstet. Gynecol. 2000, 96, 886–889. [Google Scholar] [CrossRef]
- Mousa, H.A.; Abou El Senoun, G.M.; Mahmood, T.A. Medium-term clinical outcome of women with menorrhagia treated by rollerball endometrial ablation versus abdominal hysterectomy with conservation of at least one ovary. Acta Obstet. Gynecol. Scand. 2001, 80, 442–446. [Google Scholar] [CrossRef]
- Dickersin, K.; Munro, M.G.; Clark, M.; Langenberg, P.; Scherer, R.; Frick, K.; Zhu, Q.; Hallock, L.; Nichols, J.; Yalcinkaya, T.M.; et al. Hysterectomy compared with endometrial ablation for dysfunctional uterine bleeding: A randomized controlled trial. Obstet. Gynecol. 2007, 110, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Rajaram, S.; Gupta, B.; Goel, N.; Srivastava, H. Randomized controlled trial of thermal balloon ablation versus vaginal hysterectomy for leiomyoma-induced heavy menstrual bleeding. Int. J. Gynaecol. Obstet. 2016, 135, 140–144. [Google Scholar] [CrossRef]
- Selvanathan, S.; Acharya, N.; Singhal, S. Quality of Life after Hysterectomy and Uterus-Sparing Hysteroscopic Management of Abnormal Uterine Bleeding or Heavy Menstrual Bleeding. J. Midlife Health 2019, 10, 63–69. [Google Scholar] [CrossRef]
- Papaioannou, D.; Brazier, J.E.; Paisley, S. NICE DSU Technical Support Document 9: The Identification, Review and Synthesis of Health State Utility Values from the Literature; National Institute for Health and Care Excellence: London, UK, 2011. [Google Scholar]
- Bubien, V.; Bonnet, F.; Brouste, V.; Hoppe, S.; Barouk-Simonet, E.; David, A.; Edery, P.; Bottani, A.; Layet, V.; Caron, O.; et al. High cumulative risks of cancer in patients with PTEN hamartoma tumour syndrome. J. Med. Genet. 2013, 50, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, T.S.; Marions, L.B.; Edlund, M.G. Heavy menstrual bleeding significantly affects quality of life. Acta Obstet. Gynecol. Scand. 2014, 93, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Lukes, A.S.; Baker, J.; Eder, S.; Adomako, T.L. Daily menstrual blood loss and quality of life in women with heavy menstrual bleeding. Womens Health 2012, 8, 503–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimamoto, K.; Hirano, M.; Wada-Hiraike, O.; Goto, R.; Osuga, Y. Examining the association between menstrual symptoms and health-related quality of life among working women in Japan using the EQ-5D. BMC Womens Health 2021, 21, 325. [Google Scholar] [CrossRef] [PubMed]
- Hüsing, A.; Dossus, L.; Ferrari, P.; Tjønneland, A.; Hansen, L.; Fagherazzi, G.; Baglietto, L.; Schock, H.; Chang-Claude, J.; Boeing, H.; et al. An epidemiological model for prediction of endometrial cancer risk in Europe. Eur. J. Epidemiol. 2016, 31, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Fortner, R.T.; Hüsing, A.; Kühn, T.; Konar, M.; Overvad, K.; Tjønneland, A.; Hansen, L.; Boutron-Ruault, M.C.; Severi, G.; Fournier, A.; et al. Endometrial cancer risk prediction including serum-based biomarkers: Results from the EPIC cohort. Int. J. Cancer 2017, 140, 1317–1323. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.; Mavaddat, N.; Wilcox, A.N.; Cunningham, A.P.; Carver, T.; Hartley, S.; Babb de Villiers, C.; Izquierdo, A.; Simard, J.; Schmidt, M.K.; et al. BOADICEA: A comprehensive breast cancer risk prediction model incorporating genetic and nongenetic risk factors. Genet. Med. 2019, 21, 1708–1718. [Google Scholar] [CrossRef]
- Lee, A.; Yang, X.; Tyrer, J.; Gentry-Maharaj, A.; Ryan, A.; Mavaddat, N.; Cunningham, A.P.; Carver, T.; Archer, S.; Leslie, G.; et al. Comprehensive epithelial tubo-ovarian cancer risk prediction model incorporating genetic and epidemiological risk factors. J. Med. Genet. 2021, 59, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Siyam, T.; Ross, S.; Campbell, S.; Eurich, D.T.; Yuksel, N. The effect of hormone therapy on quality of life and breast cancer risk after risk-reducing salpingo-oophorectomy: A systematic review. BMC Women’s Health 2017, 17, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoll, J.; Rosenthal, E.; Cummings, S.; Willmott, J.; Bernhisel, R.; Kupfer, S.S. No evidence of increased risk of breast cancer in women with Lynch syndrome identified by multigene panel testing. JCO Precis. Oncol. 2020, 4, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Gaba, F.; Goyal, S.; Marks, D.; Chandrasekaran, D.; Evans, O.; Robbani, S.; Tyson, C.; Legood, R.; Saridogan, E.; McCluggage, W.G.; et al. Surgical decision making in premenopausal. J. Med. Genet. 2021, 59, 122–132. [Google Scholar] [CrossRef]
- Moorman, P.G.; Myers, E.R.; Schildkraut, J.M.; Iversen, E.S.; Wang, F.; Warren, N. Effect of hysterectomy with ovarian preservation on ovarian function. Obstet. Gynecol. 2011, 118, 1271–1279. [Google Scholar] [CrossRef]
- Trabuco, E.C.; Moorman, P.G.; Algeciras-Schimnich, A.; Weaver, A.L.; Cliby, W.A. Association of Ovary-Sparing Hysterectomy with Ovarian Reserve. Obstet. Gynecol. 2016, 127, 819–827. [Google Scholar] [CrossRef] [Green Version]
- Ahn, E.H.; Bai, S.W.; Song, C.H.; Kim, J.Y.; Jeong, K.A.; Kim, S.K.; Lee, J.S.; Kwon, J.Y.; Park, K.H. Effect of hysterectomy on conserved ovarian function. Yonsei Med. J. 2002, 43, 53–58. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Adamson, J.; Ebrahim, S. Lay perceptions of a ‘natural’ menopause. Cross sectional study of the British Women’s Heart and Health Study. BJOG 2002, 109, 1398–1400. [Google Scholar] [CrossRef]
- Farquhar, C.M.; Sadler, L.; Harvey, S.A.; Stewart, A.W. The association of hysterectomy and menopause: A prospective cohort study. BJOG 2005, 112, 956–962. [Google Scholar] [CrossRef]
- Thakar, R.; Ayers, S.; Clarkson, P.; Stanton, S.; Manyonda, I. Outcomes after total versus subtotal abdominal hysterectomy. N. Engl. J. Med. 2002, 347, 1318–1325. [Google Scholar] [CrossRef]
- Christiansen, U.J.; Hansen, M.J.; Lauszus, F.F. Hysterectomy is not associated with de-novo urinary incontinence: A ten-year cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 215, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Duru, C.; Jha, S.; Lashen, H. Urodynamic outcomes after hysterectomy for benign conditions: A systematic review and meta-analysis. Obstet. Gynecol. Surv. 2012, 67, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Heliövaara-Peippo, S.; Halmesmäki, K.; Hurskainen, R.; Teperi, J.; Grenman, S.; Kivelä, A.; Tomas, E.; Tuppurainen, M.; Paavonen, J. The effect of hysterectomy or levonorgestrel-releasing intrauterine system on lower urinary tract symptoms: A 10-year follow-up study of a randomised trial. BJOG 2010, 117, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.; Granath, F.; Cnattingius, S.; Falconer, C. Hysterectomy and risk of stress-urinary-incontinence surgery: Nationwide cohort study. Lancet 2007, 370, 1494–1499. [Google Scholar] [CrossRef] [PubMed]
- Forsgren, C.; Lundholm, C.; Johansson, A.L.; Cnattingius, S.; Zetterström, J.; Altman, D. Vaginal hysterectomy and risk of pelvic organ prolapse and stress urinary incontinence surgery. Int. Urogynecol. J. 2012, 23, 43–48. [Google Scholar] [CrossRef]
- Chan, J.L.; Senapati, S.; Johnson, L.N.C.; Digiovanni, L.; Voong, C.; Butts, S.F.; Domchek, S.M. Risk factors for sexual dysfunction in BRCA mutation carriers after risk-reducing salpingo-oophorectomy. Menopause 2019, 26, 132–139. [Google Scholar] [CrossRef]
- Lorenz, T.; McGregor, B.; Swisher, E. Relationship satisfaction predicts sexual activity following risk-reducing salpingo-oophorectomy. J. Psychosom. Obstet. Gynaecol. 2014, 35, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, F.; Alimoradi, Z.; Tavakolian, S. Effect of Hysterectomy due to Benign Diseases on Female Sexual Function: A Systematic Review and Meta-analysis. J. Minim. Invasive Gynecol. 2022, 29, 476–488. [Google Scholar] [CrossRef]
- Bradford, A.; Meston, C. Sexual outcomes and satisfaction with hysterectomy: Influence of patient education. J. Sex. Med. 2007, 4, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Lykke, R.; Løwenstein, E.; Blaakær, J.; Gimbel, H. Hysterectomy technique and risk of pelvic organ prolapse repair: A Danish nationwide cohort study. Arch. Gynecol. Obstet. 2017, 296, 527–531. [Google Scholar] [CrossRef]
- Billfeldt, N.K.; Borgfeldt, C.; Lindkvist, H.; Stjerndahl, J.H.; Ankardal, M. A Swedish population-based evaluation of benign hysterectomy, comparing minimally invasive and abdominal surgery. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 222, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Pitter, M.C.; Simmonds, C.; Seshadri-Kreaden, U.; Hubert, H.B. The impact of different surgical modalities for hysterectomy on satisfaction and patient reported outcomes. Interact. J. Med. Res. 2014, 3, e11. [Google Scholar] [CrossRef] [PubMed]
- Bartels, H.C.; Rogers, A.C.; Janda, M.; Obermair, A.; Brennan, D.J. Quality of life following minimally invasive hysterectomy compared to abdominal hysterectomy: A metanalysis. Eur. J. Obstet. Gynecol. Reprod. Biol 2020, 252, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Casarin, J.; Cromi, A.; Bogani, G.; Multinu, F.; Uccella, S.; Ghezzi, F. Surgical morbidity of total laparoscopic hysterectomy for benign disease: Predictors of major postoperative complications. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 263, 210–215. [Google Scholar] [CrossRef]
- Zimmermann, J.S.M.; Sima, R.M.; Radosa, M.P.; Radosa, C.G.; Ples, L.; Wagenpfeil, S.; Solomayer, E.F.; Radosa, J.C. Quality of life and sexual function in patients aged 35 years or younger undergoing hysterectomy for benign gynecologic conditions: A prospective cohort study. Int. J. Gynaecol. Obstet. 2022. ahead of print. [Google Scholar] [CrossRef]
- Matza, L.S.; Stewart, K.D.; Lloyd, A.J.; Rowen, D.; Brazier, J.E. Vignette-Based Utilities: Usefulness, Limitations, and Methodological Recommendations. Value Health 2021, 24, 812–821. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author, Year | Country | Study Design | Hysterectomy Sample Size at Follow-up (n) | Age of Hysterectomy Participants (Years) (mean ± SD Unless Specified) | Follow-up (Months) | Population/Indication | BSO | Route of Hysterectomy |
|---|---|---|---|---|---|---|---|---|
| Risk-reducing hysterectomy | ||||||||
| Moldovan 2015 [31] | UK | Qualitative and cohort | 14 (quantitative) 11 (qualitative) | 52.5 | 12–144 | Lynch Syndrome + family history | 11/14 (78.6%) | TAH |
| Etchegary 2015 [32] | Canada | Qualitative | 8 | 49 (range 33–64) | 1.5–96 (mean 42) | Lynch Syndrome | yes | LAVH (6), TAH (2) |
| Etchegary 2018 [33] | Canada | Qualitative | 8 | 49 (range 33–64) | 36–120 | Lynch Syndrome | yes | TAH and TLH |
| Kalamo 2020 [34] | Finland | Cohort | 42 | 56.9 (range 43–72) | 12–456 | Lynch Syndrome | not reported | not reported |
| Treatment of heavy menstrual bleeding | ||||||||
| Hysterectomy vs. hormonal treatment | ||||||||
| Hurskainen 2001 [63] | Finland | RCT: hysterectomy vs. LNG-IUS | 112 | 43.1 ± 3.5 | 12 | HMB | 5/112 (4.5%) | TAH 21, vaginal 30, TLH 56 |
| Hurskainen 2004 [64] | Finland | RCT: 5-year follow-up of Hurskainen 2001 | 115 | 43.1 ± 3.5 | 60 | HMB | 5/112 (4.5%) | TAH 21, vaginal 30, TLH 56 |
| Halmesmäki 2004 [65] | Finland | RCT: Menopausal impact of Hurskainen 2001 | 107 | 43.1 ± 3.5 | 12 | HMB | 5/112 (4.5%) | TAH 21, vaginal 30, TLH 56 |
| Halmesmäki 2007 [66] | Finland | RCT: 5-year follow-up of Hurskainen 2001 | 117 | 43.1 ± 3.5 | 60 | HMB | 5/112 (4.5%) | TAH 21, vaginal 30, TLH 56 |
| Heliövaara-Peippo 2013 [67] | Finland | RCT: 10-year follow-up of Hurskainen 2001 | 117 | 43.1 ± 3.5 | 120 | HMB | 5/112 (4.5%) | TAH 21, vaginal 30, TLH 56 |
| Kuppermann 2004 [68] | USA | RCT: hysterectomy vs. oral medical treatment | 28 | 42.0 ± 4.6 | 24 | DUB | “discouraged” but not reported | TAH or vaginal |
| Adigüzel 2017 [69] | Turkey | Cohort: TLH vs. TAH vs. LNG-IUS | 64 | 48.4 ± 4.4 | 6 | HMB | not reported | 29 TAH, 35 TLH |
| Comparison of total vs. subtotal | ||||||||
| Learman 2003 [70] | USA | RCT: total vs. subtotal | 64 | 41.8 ± 5.2 | 24 | DUB | not reported | TAH |
| Kuppermann 2005 [71] | USA | RCT: 2-year outcomes of Learman 2003 | 67 | 41.8 ± 5.2 | 24 | DUB | not reported | TAH |
| Cohort/other | ||||||||
| Roberts 1996 [72] | UK | Cohort | 192 | 43.0 (range 21–56) | 6–18 | DUB | not reported | 242 TAH, 5 vaginal, 17 LAVH |
| Brandsborg 2009 [73] | Denmark | Cohort | 90 | 46 (median) (range 32–71) | 4 | DUB/fibroids | not reported | TAH, vaginal, LAVH (numbers not reported) |
| Till 2022 [74] | USA | Cohort: different indications of hysterectomy | 37 | 44.2 ± 6.9 | 6 | DUB/HMB | not reported | TLH (70%), TAH (11%), vaginal (19%) |
| Hysterectomy vs. endometrial ablation/resection | ||||||||
| Dwyer 1993 [75] | UK | RCT: hysterectomy vs. TCRE | 95 | 40.6 | 4 | HMB | up to 14/95 (10.5%) | TAH |
| Sculpher 1996 [76] | UK | RCT: 2-year follow-up of Dwyer 1993 | 73 | 40.6 | 34 (mean) | HMB | up to 14/95 (10.5%) | TAH |
| Pinion 1994 [77] | UK | RCT: hysterectomy vs. TCRE vs. ablation | 95 | 40.3 ± 5.2 | 12 | DUB | 6/85 (7.1%) | 85 TAH 10 vaginal |
| Alexander 1996 [78] | UK | RCT: 1-year follow-up of Pinion 1994 | 85 | 40.3 ± 5.2 | 12 | DUB | 6/85 (7.1%) | 85 TAH 10 vaginal |
| Aberdeen Trials Group 1999 [79] | UK | RCT: 4-year follow-up of Pinion 1994 | 72 | 40.3 ± 5.2 | 48 | DUB | in 6/85 (7.1%) | 85 TAH 10 vaginal |
| O’Connor 1997 [80] | UK | RCT: hysterectomy vs. TCRE | 56 | 39.4 ± 4.8 | 12–36 | HMB | 0.04 | TAH/vaginal |
| Crosignani 1997 [81] | Italy | RCT: hysterectomy vs. TCRE | 39 | 45 (median) (IQR 42–48.5) | 24 | HMB | not reported | LAVH |
| Tapper 1998 [82] | Finland | Cohort: hysterectomy vs. TCRE | 40 | 43 ± 4.0 | 6–31 | HMB | not reported | TLH |
| Tjarks 2000 [83] | USA | Cohort: hysterectomy vs. polypectomy ± ablation vs. medical treatment | 7 | 49 (range 28–74) | 5–24 | DUB/HMB | not reported | not reported |
| Mousa 2001 [84] | UK | Cohort: hysterectomy vs. ablation | 40 | 41 (median) (range 30–48) | 32 (mean) (range 18–55) | HMB | no | TAH |
| Dickersin 2007 [85] | USA, Canada | RCT: hysterectomy vs. ablation | 107 | not reported | 24 | DUB | 18/114 (7.0%) | (TAH/vaginal/TLH-numbers not reported) |
| Jain 2016 [86] | India | RCT: hysterectomy vs. thermal balloon ablation | 20 | 44 ± 2.0 | 24 | DUB | not reported | vaginal |
| Selvanathan 2019 [87] | India | Cohort: hysterectomy vs. hysteroscopic surgery | 176 | 40.2 ± 4.3 | 48 | DUB/HMB | not reported | 116 TAH, 27 vaginal, 32 TLH |
| First Author, Year | Relevant Findings for Hysterectomy Group |
|---|---|
| Risk-reducing hysterectomy | |
| Moldovan 2015 [31] | No decision regret, reduced cancer worry. Few patients had menopausal symptoms impacting QoL, associated with poorer general health and psychological distress. |
| Etchegary 2015 [32] | Surgery alleviated cancer fear, no decision regret. Menopausal symptoms for women not on HRT |
| Etchegary 2018 [33] | High satisfaction in women who took HRT. Severe menopausal symptoms in those who did not take HRT. |
| Kalamo 2020 [34] | Generally satisfied with RRH. 45% still had a strong fear of cancer. |
| Treatment of heavy menstrual bleeding | |
| Hysterectomy vs. hormonal treatment | |
| Hurskainen 2001 [63] | Improved generic QoL, general health, reduced anxiety and depression, improved sexual satisfaction |
| Hurskainen 2004 [64] | Greater satisfaction, reduced anxiety/depression, better general health. Worse sexual satisfaction |
| Halmesmäki 2004 [65] | No signicant changes in overall menopausal index scores, although increase in vasomotor symptoms |
| Halmesmäki 2007 [66] | Increased self and partner sexual satisfaction, reduced sexual problems compared to baseline and to the Mirena |
| Heliövaara-Peippo 2013 [67] | Increase in overall QoL and sexual satisfaction until 5 years, decrease in QoL including sexual satisfaction between 5 to 10 years back to baseline |
| Kuppermann 2004 [68] | Improved QoL, satisfaction, symptom resolution, sexual desire and health distress. Improvements seen at 6 months, maintained at 2 years |
| Adigüzel 2017 [69] | Hysterectomy generally better health, social function better with TLH, no change in mental health parameters |
| Comparison of hysterectomy type | |
| Learman 2003 [70] | Improvement in pain and urinary symptoms |
| Kuppermann 2005 [71] | Improved sexual functioning, general QoL, and body image, no differences between groups |
| Cohort/other | |
| Roberts 1996 [72] | improved physical and mental health, majority had no change in sex life |
| Brandsborg 2009 [73] | Decrease in pain at 4 months. Those with low pre-operative QoL more likely to have ongoing post-operative pain |
| Till 2022 [74] | No significant change in sexual function (although a trend towards improved function) |
| Hysterectomy vs. endometrial ablation/resection | |
| Dwyer 1993 [75] | Higher satisfaction, fewer pre-menstrual symptoms |
| Sculpher 1996 [76] | Very high satisfaction. Evidence of improved QoL compared to resection |
| Pinion 1994 [77] | High satisfaction and improvement in symptoms |
| Alexander 1996 [78] | Reduced anxiety, depression and improved sexual relationships |
| Aberdeen Trials Group 1999 [79] | Generally better health, fewer pre-menstrual symptoms, high satisfaction |
| O’Connor 1997 [80] | Very high satisfaction, improvement in general quality of life and psychosocial functioning |
| Crosignani 1997 [81] | Greater satisfaction, greater social functioning and vitality, lower anxiety, similar sexual functioning |
| Tapper 1998 [82] | High satisfaction |
| Tjarks 2000 [83] | Hysterectomy had 100% satisfaction, greater than other treatment modalities |
| Mousa 2001 [84] | High satisfaction, improvement in general health inc sexual function, PMS |
| Dickersin 2007 [85] | Improved generic QoL, particularly reduced pain and fatigue compared to ablation |
| Jain 2016 [86] | Resolution of dysmenorrhea and pelvic pain, increase in generic QoL |
| Selvanathan 2019 [87] | Improvement in all QoL domains, greater in hysteroscopic group vs. hysterectomy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oxley, S.; Xiong, R.; Wei, X.; Kalra, A.; Sideris, M.; Legood, R.; Manchanda, R. Quality of Life after Risk-Reducing Hysterectomy for Endometrial Cancer Prevention: A Systematic Review. Cancers 2022, 14, 5832. https://doi.org/10.3390/cancers14235832
Oxley S, Xiong R, Wei X, Kalra A, Sideris M, Legood R, Manchanda R. Quality of Life after Risk-Reducing Hysterectomy for Endometrial Cancer Prevention: A Systematic Review. Cancers. 2022; 14(23):5832. https://doi.org/10.3390/cancers14235832
Chicago/Turabian StyleOxley, Samuel, Ran Xiong, Xia Wei, Ashwin Kalra, Michail Sideris, Rosa Legood, and Ranjit Manchanda. 2022. "Quality of Life after Risk-Reducing Hysterectomy for Endometrial Cancer Prevention: A Systematic Review" Cancers 14, no. 23: 5832. https://doi.org/10.3390/cancers14235832
APA StyleOxley, S., Xiong, R., Wei, X., Kalra, A., Sideris, M., Legood, R., & Manchanda, R. (2022). Quality of Life after Risk-Reducing Hysterectomy for Endometrial Cancer Prevention: A Systematic Review. Cancers, 14(23), 5832. https://doi.org/10.3390/cancers14235832