
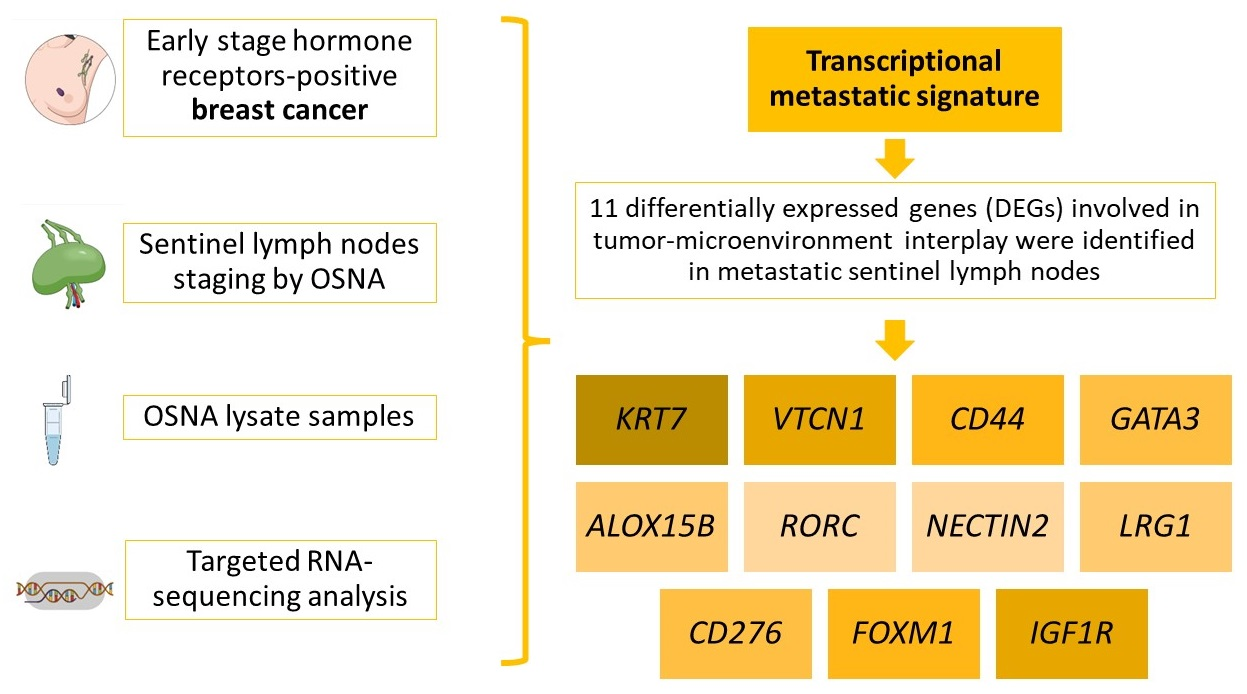
One Step Nucleic Acid Amplification (OSNA) Lysate Samples Are Suitable to Establish a Transcriptional Metastatic Signature in Patients with Early Stage Hormone Receptors-Positive Breast Cancer

 ,
,  , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. SLN Biopsy and OSNA Assay
2.3. ALND: Non-Sentinel LNs
2.4. Pathological Evaluation of the Tumor
2.5. RNA Sequencing
2.6. Statistical Analysis
3. Results
3.1. Clinicopathologic Results
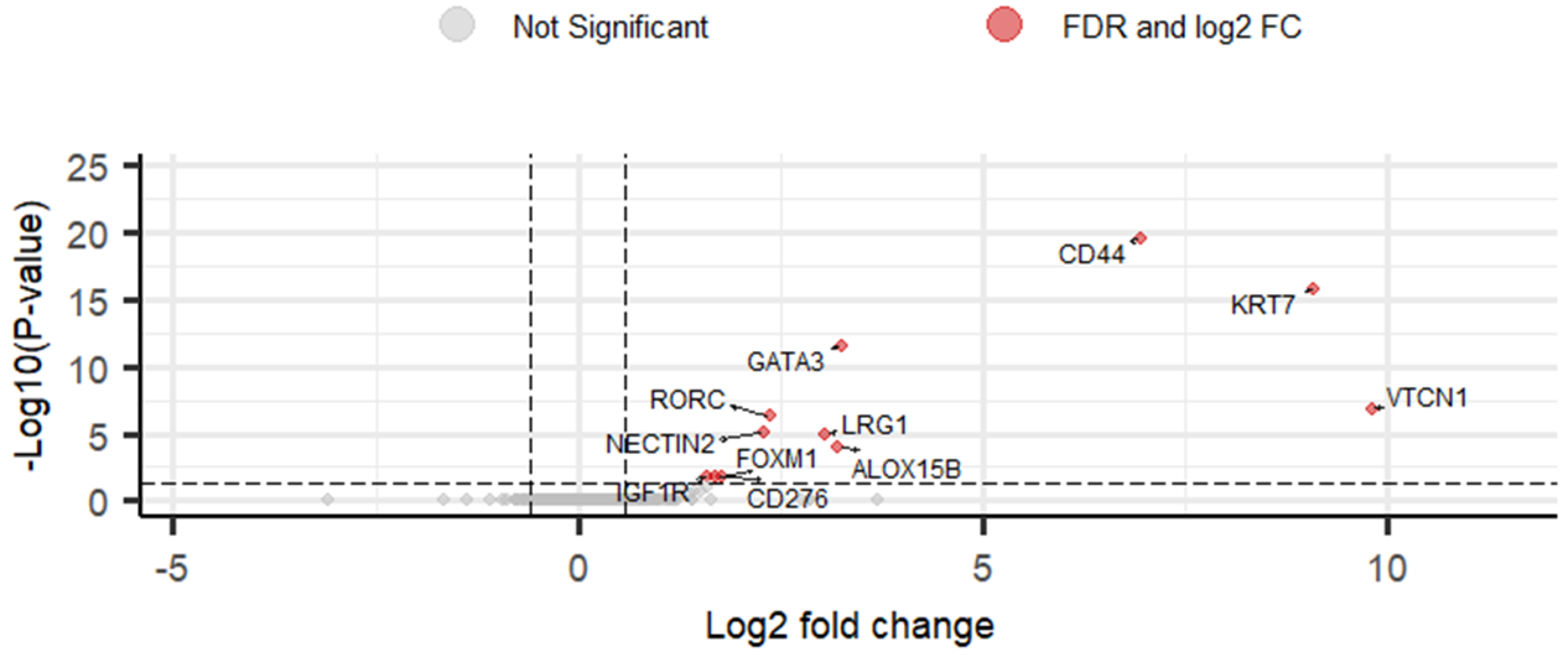
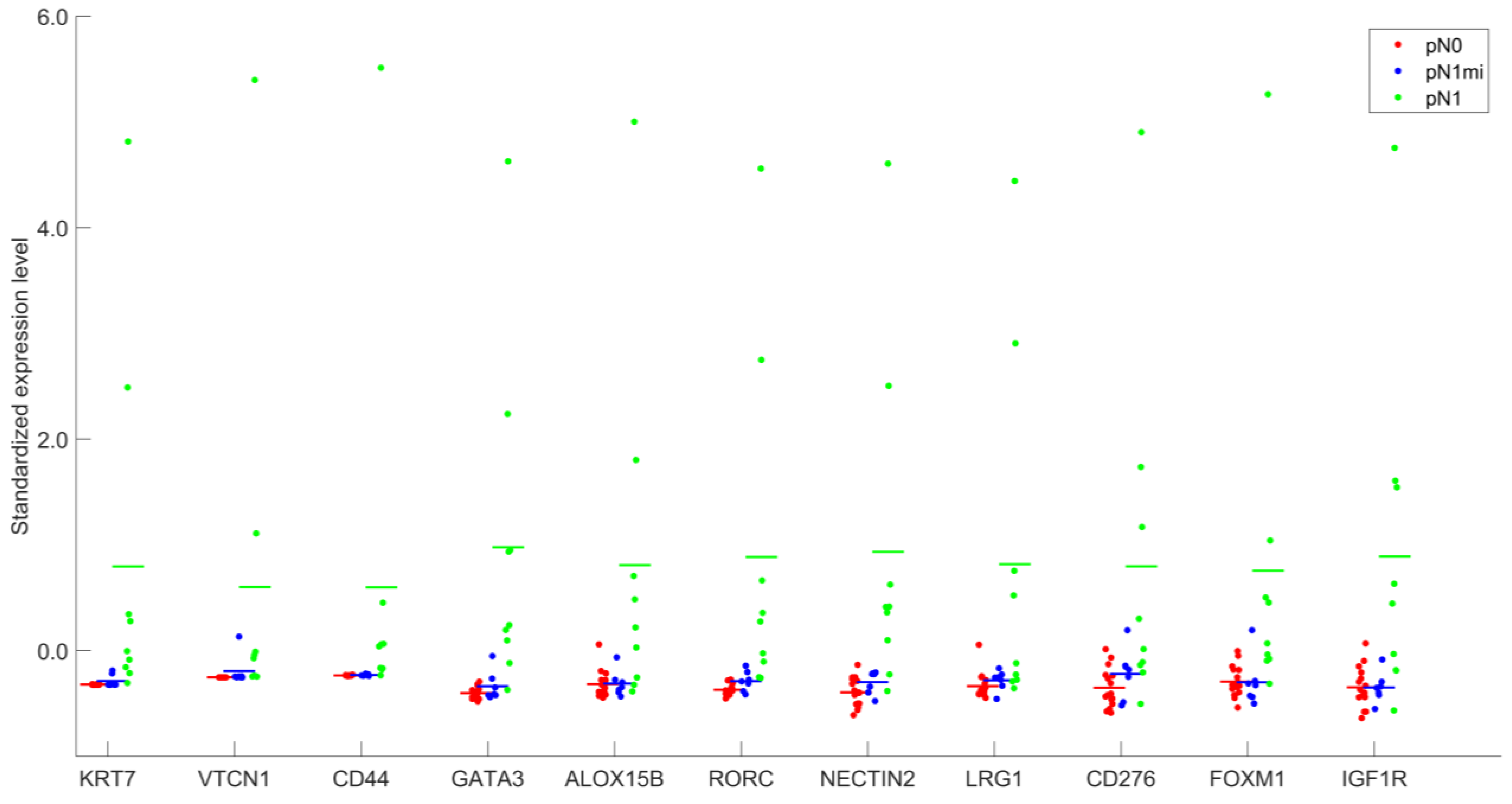
3.2. Gene Expression Analysis
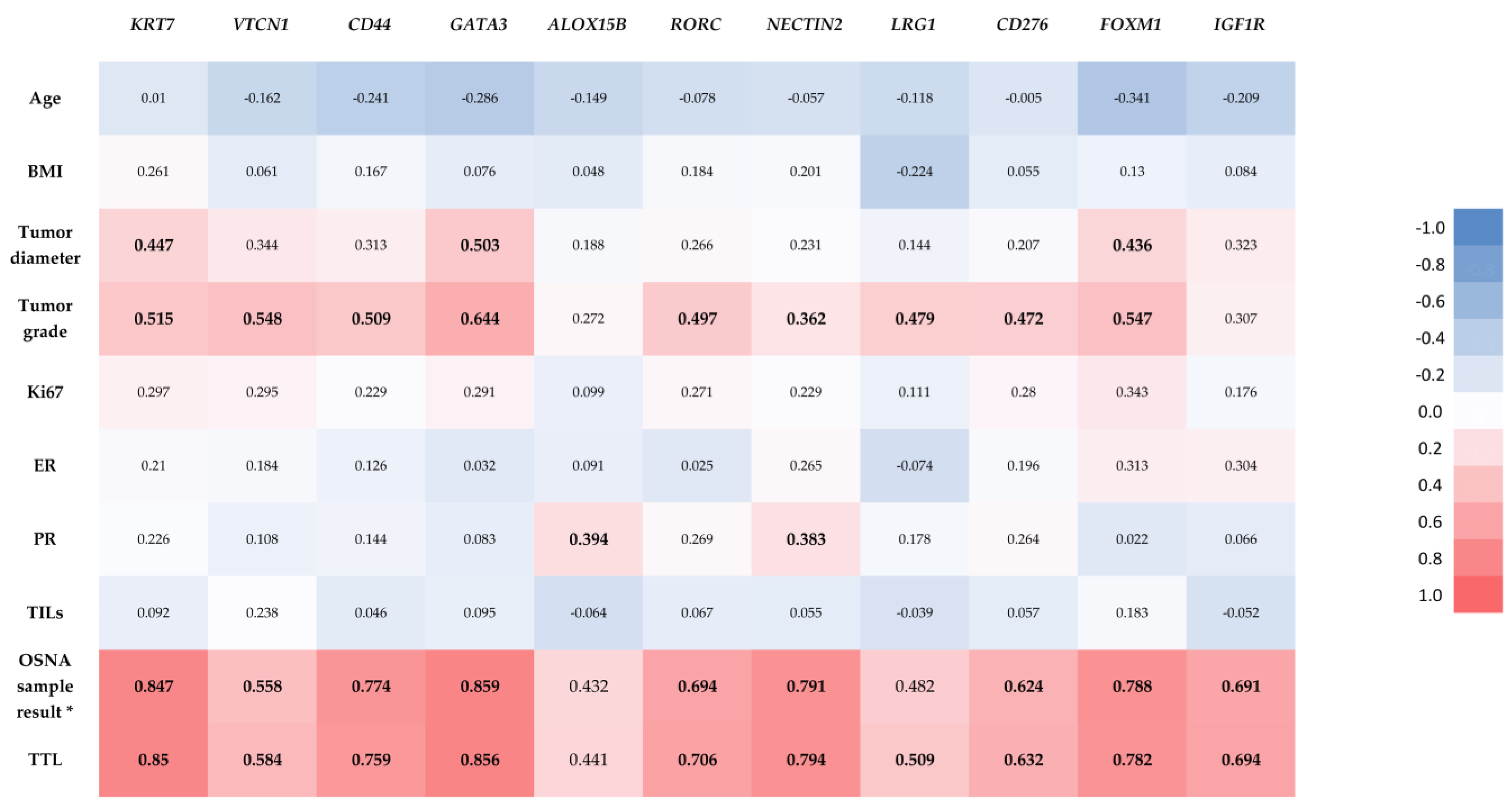
3.3. Statistical Analysis between DEGs and Relevant Clinicopathologic Parameters
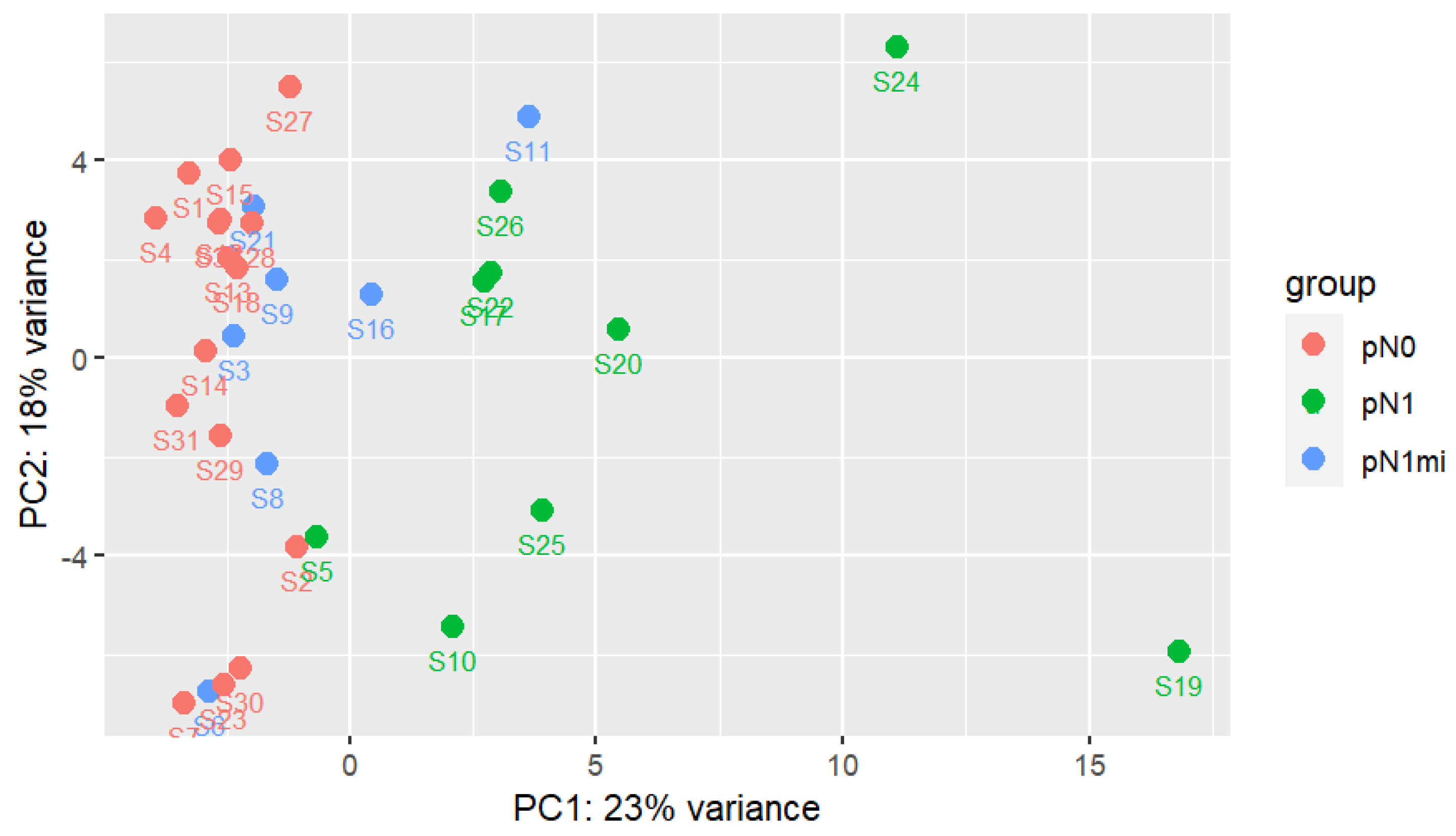
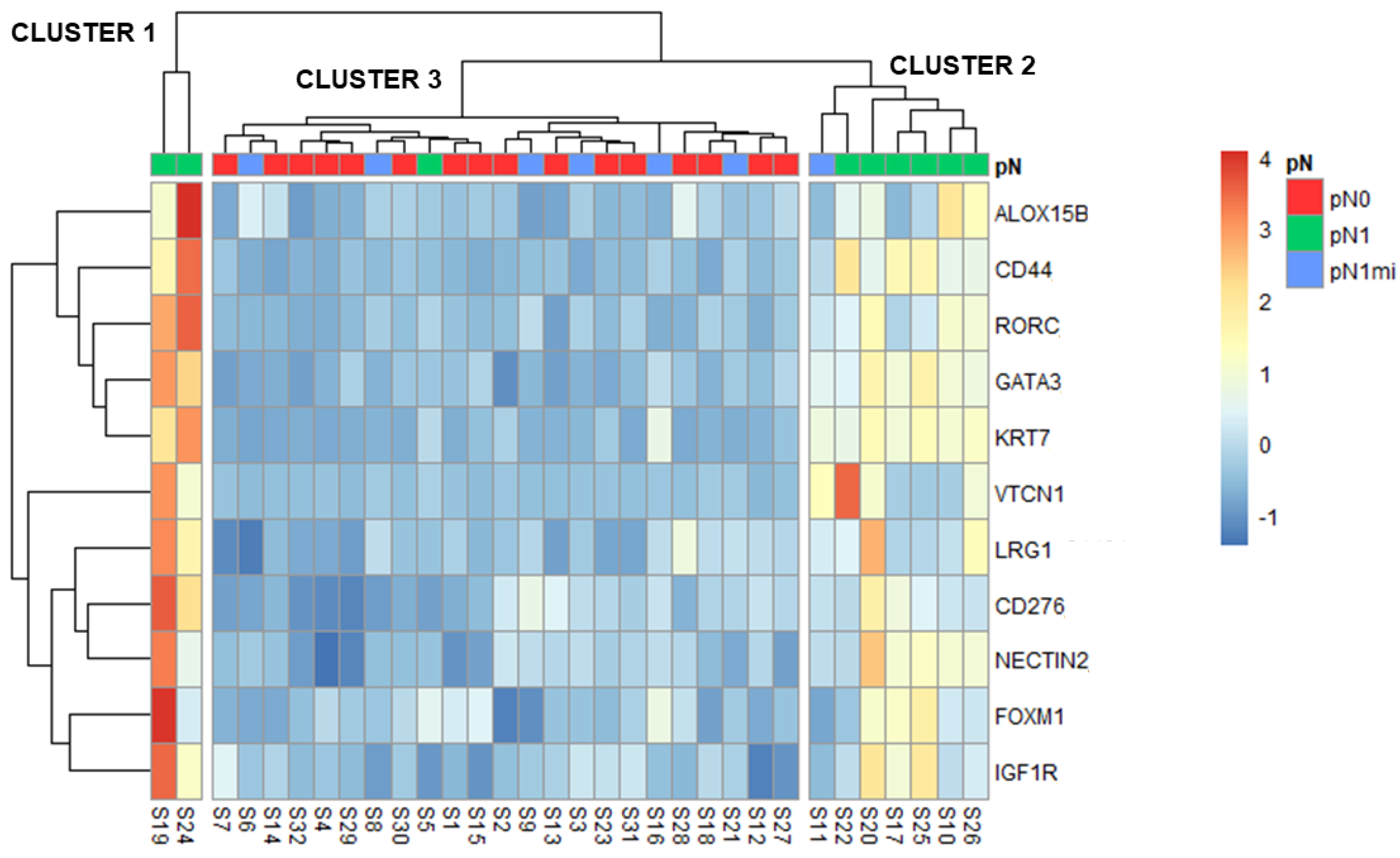
3.4. Clusters
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gibert-Ramos, A.; López, C.; Bosch, R.; Fontoura, L.; Bueno, G.; García-Rojo, M.; Berenguer, M.; Lejeune, M. Immune Response Profile of Primary Tumour, Sentinel and Non-Sentinel Axillary Lymph Nodes Related to Metastasis in Breast Cancer: An Immunohistochemical Point of View. Histochem. Cell Biol. 2019, 152, 177–193. [Google Scholar] [CrossRef]
- Lorusso, G.; Rüegg, C. New Insights into the Mechanisms of Organ-Specific Breast Cancer Metastasis. Semin. Cancer Biol. 2012, 22, 226–233. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burstein, H.J.; Curigliano, G.; Loibl, S.; Dubsky, P.; Gnant, M.; Poortmans, P.; Colleoni, M.; Denkert, C.; Piccart-Gebhart, M.; Regan, M.; et al. Estimating the Benefits of Therapy for Early-Stage Breast Cancer: The St. Gallen International Consensus Guidelines for the Primary Therapy of Early Breast Cancer 2019. Ann. Oncol. 2019, 30, 1541–1557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 691–722. [Google Scholar] [CrossRef] [PubMed]
- Burstein, H.J.; Curigliano, G.; Thürlimann, B.; Weber, W.P.; Poortmans, P.; Regan, M.M.; Senn, H.J.; Winer, E.P.; Gnant, M.; Aebi, S.; et al. Customizing Local and Systemic Therapies for Women with Early Breast Cancer: The St. Gallen International Consensus Guidelines for Treatment of Early Breast Cancer 2021. Ann. Oncol. 2021, 32, 1216–1235. [Google Scholar] [CrossRef]
- Lurie, R.H.; Anderson, B.O.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Blair, S.L.; Burstein, H.J.; Dang, C.; Elias, A.D.; et al. NCCN Guidelines Version 1.2020 Breast Cancer Risk Reduction. National Comprehensive Cancer Network. 2020. Available online: https://www.nccn.org/ (accessed on 29 February 2020).
- Curigliano, G.; Burstein, H.J.; Winer, E.P.; Gnant, M.; Dubsky, P.; Loibl, S.; Colleoni, M.; Regan, M.M.; Piccart-Gebhart, M.; Senn, H.-J.; et al. De-Escalating and Escalating Treatments for Early-Stage Breast Cancer: The St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017. Ann. Oncol. 2017, 28, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Donker, M.; van Tienhoven, G.; Straver, M.E.; Meijnen, P.; van de Velde, C.J.H.; Mansel, R.E.; Cataliotti, L.; Westenberg, A.H.; Klinkenbijl, J.H.G.; Orzalesi, L.; et al. Radiotherapy or Surgery of the Axilla after a Positive Sentinel Node in Breast Cancer (EORTC 10981-22023 AMAROS): A Randomised, Multicentre, Open-Label, Phase 3 Non-Inferiority Trial. Lancet Oncol. 2014, 15, 1303–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuliano, A.E.; Ballman, K.V.; McCall, L.; Beitsch, P.D.; Brennan, M.B.; Kelemen, P.R.; Ollila, D.W.; Hansen, N.M.; Whitworth, P.W.; Blumencranz, P.W.; et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women with Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA 2017, 318, 918–926. [Google Scholar] [CrossRef] [Green Version]
- Andre, F.; Ismaila, N.; Allison, K.H.; Barlow, W.E.; Collyar, D.E.; Damodaran, S.; Henry, N.L.; Jhaveri, K.; Kalinsky, K.; Kuderer, N.M.; et al. Biomarkers for Adjuvant Endocrine and Chemotherapy in Early-Stage Breast Cancer: ASCO Guideline Update. J. Clin. Oncol. 2022, 40, 1816–1837. [Google Scholar] [CrossRef]
- Jimbo, K.; Kinoshita, T.; Suzuki, J.; Asaga, S.; Hojo, T.; Yoshida, M.; Tsuda, H. Sentinel and Nonsentinel Lymph Node Assessment Using a Combination of One-Step Nucleic Acid Amplification and Conventional Histological Examination. Breast 2013, 22, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- Fougo, J.L.; Amendoeira, I.; Brito, M.J.; Correia, A.P.; Gonçalves, A.; Honavar, M.; Machado, A.; Magalhães, A.; Marta, S.; Nogueira, M.; et al. Sentinel Node Total Tumour Load as a Predictive Factor for Non-Sentinel Node Status in Early Breast Cancer Patients—The Porttle Study. Surg. Oncol. 2020, 32, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, M.; Nakabayashi, K.; Yoshidome, K.; Kaneko, T.; Iwase, T.; Akiyama, F.; Kato, Y.; Tsuda, H.; Ueda, S.; Sato, K.; et al. One-Step Nucleic Acid Amplification for Intraoperative Detection of Lymph Node Metastasis in Breast Cancer Patients. Clin. Cancer Res. 2007, 13, 4807–4816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peg, V.; Sansano, I.; Vieites, B.; Bernet, L.; Cano, R.; Córdoba, A.; Sancho, M.; Martín, M.D.; Vilardell, F.; Cazorla, A.; et al. Role of Total Tumour Load of Sentinel Lymph Node on Survival in Early Breast Cancer Patients. Breast 2017, 33, 8–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertozzi, S.; Londero, A.P.; Bulfoni, M.; Seriau, L.; Agakiza, D.; Pasqualucci, A.; Andretta, M.; Orsaria, M.; Mariuzzi, L.; Cedolini, C. One-Step Nucleic Acid Amplification System in Comparison to the Intraoperative Frozen Section and Definitive Histological Examination Among Breast Cancer Patients: A Retrospective Survival Study. Front. Oncol. 2022, 12, 847858. [Google Scholar] [CrossRef] [PubMed]
- Shi, F.; Zhang, Q.; Liang, Z.; Zhang, M.; Liu, X. One-Step Nucleic Acid Amplification Assay Is an Accurate Technique for Sentinel Lymph Node Biopsy of Breast Cancer Patients: A Meta-Analysis. Br. J. Cancer 2017, 117, 1185–1191. [Google Scholar] [CrossRef] [Green Version]
- Peg, V.; Espinosa-Bravo, M.; Vieites, B.; Vilardell, F.; Antúnez, J.R.; De Salas, M.S.; Delgado-Sánchez, J.J.; Pinto, W.; Gozalbo, F.; Petit, A.; et al. Intraoperative Molecular Analysis of Total Tumor Load in Sentinel Lymph Node: A New Predictor of Axillary Status in Early Breast Cancer Patients. Breast Cancer Res. Treat. 2013, 139, 87–93. [Google Scholar] [CrossRef]
- Kenny, R.; Wong, G.; Gould, L.; Odofin, O.; Bowyer, R.; Sotheran, W. Can One-Step Nucleic Acid Amplification Assay Predict Four or More Positive Axillary Lymph Node Involvement in Breast Cancer Patients: A Single-Centre Retrospective Study. Ann. R. Coll. Surg. Engl. 2022, 104, 216–220. [Google Scholar] [CrossRef]
- Ohi, Y.; Umekita, Y.; Sagara, Y.; Rai, Y.; Yotsumoto, D.; Matsukata, A.; Baba, S.; Tamada, S.; Matsuyama, Y.; Ando, M.; et al. Whole Sentinel Lymph Node Analysis by a Molecular Assay Predicts Axillary Node Status in Breast Cancer. Br. J. Cancer 2012, 107, 1239–1243. [Google Scholar] [CrossRef] [Green Version]
- Nabais, C.; Figueiredo, J.; Lopes, P.; Martins, M.; Araújo, A. Total Tumor Load Assessed by One-Step Nucleic Acid Amplification Assay as an Intraoperative Predictor for Non-Sentinel Lymph Node Metastasis in Breast Cancer. Breast 2017, 32, 33–36. [Google Scholar] [CrossRef]
- Pina, H.; Salleron, J.; Gilson, P.; Husson, M.; Rouyer, M.; Leroux, A.; Rauch, P.; Marchal, F.; Käppeli, M.; Merlin, J.L.; et al. Intraoperative Prediction of Non-Sentinel Lymph Node Metastases in Breast Cancer Using Cytokeratin 19 MRNA Copy Number: A Retrospective Analysis. Mol. Clin. Oncol. 2022, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Riedel, A.; Shorthouse, D.; Haas, L.; Hall, B.A.; Shields, J. Tumor-Induced Stromal Reprogramming Drives Lymph Node Transformation. Nat. Immunol. 2016, 17, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- López, C.; Bosch, R.; Orero, G.; Korzynska, A.; García-Rojo, M.; Bueno, G.; Fernández-Carrobles, M.d.M.; Gibert-Ramos, A.; Roszkowiak, L.; Callau, C.; et al. The Immune Response in Nonmetastatic Axillary Lymph Nodes Is Associated with the Presence of Axillary Metastasis and Breast Cancer Patient Outcome. Am. J. Pathol. 2020, 190, 660–673. [Google Scholar] [CrossRef]
- Kim, R.; Emi, M.; Tanabe, K.; Arihiro, K. Immunobiology of the Sentinel Lymph Node and Its Potential Role for Antitumour Immunity. Lancet Oncol. 2006, 7, 1006–1016. [Google Scholar] [CrossRef] [PubMed]
- Grigoriadis, A.; Gazinska, P.; Pai, T.; Irhsad, S.; Wu, Y.; Millis, R.; Naidoo, K.; Owen, J.; Gillett, C.E.; Tutt, A.; et al. Histological Scoring of Immune and Stromal Features in Breast and Axillary Lymph Nodes Is Prognostic for Distant Metastasis in Lymph Node-Positive Breast Cancers. J. Pathol. Clin. Res. 2018, 4, 39–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadeghalvad, M.; Mohammadi-Motlagh, H.R.; Rezaei, N. Immune Microenvironment in Different Molecular Subtypes of Ductal Breast Carcinoma. Breast Cancer Res. Treat. 2021, 185, 261–279. [Google Scholar] [CrossRef]
- Howlader, N.; Cronin, K.A.; Kurian, A.W.; Andridge, R. Differences in Breast Cancer Survival by Molecular Subtypes in the United States. Cancer Epidemiol. Biomark. Prev. 2018, 27, 619–626. [Google Scholar] [CrossRef] [Green Version]
- El Bairi, K.; Haynes, H.R.; Blackley, E.; Fineberg, S.; Shear, J.; Turner, S.; de Freitas, J.R.; Sur, D.; Amendola, L.C.; Gharib, M.; et al. The Tale of TILs in Breast Cancer: A Report from The International Immuno-Oncology Biomarker Working Group. NPJ Breast Cancer 2021, 7, 1–17. [Google Scholar] [CrossRef]
- Dodson, A.; Parry, S.; Ibrahim, M.; Bartlett, J.M.S.; Pinder, S.; Dowsett, M.; Miller, K. Breast Cancer Biomarkers in Clinical Testing: Analysis of a UK National External Quality Assessment Scheme for Immunocytochemistry and in Situ Hybridisation Database Containing Results from 199 300 Patients. J. Pathol. Clin. Res. 2018, 4, 262–273. [Google Scholar] [CrossRef]
- Ribeiro, C.; Gante, I.; Dias, M.F.; Gomes, A.; Silva, H.C. A New Application to One-Step Nucleic Acid Amplification-Discarded Sample in Breast Cancer: Preliminary Results. Mol. Clin. Oncol. 2021, 15, 1–5. [Google Scholar] [CrossRef]
- Martín-Sánchez, E.; Pernaut-Leza, E.; Mendaza, S.; Cordoba, A.; Vicente-Garcia, F.; Monreal-Santesteban, I.; Vizcaino, J.P.; De Cerio, M.J.D.; Perez-Janices, N.; Blanco-Luquin, I.; et al. Gene Promoter Hypermethylation Is Found in Sentinel Lymph Nodes of Breast Cancer Patients, in Samples Identified as Positive by One-Step Nucleic Acid Amplification of Cytokeratin 19 MRNA. Virchows Arch. 2016, 469, 51–59. [Google Scholar] [CrossRef]
- Kossai, M.; Radosevic-Robin, N.; Penault-Llorca, F. Refining Patient Selection for Breast Cancer Immunotherapy: Beyond PD-L1. ESMO Open. 2021, 6, 100257. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth Edition of the AJCC Cancer Staging Manual: Breast Cancer. Ann. Surg. Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef]
- Cykowska, A.; Marano, L.; D’Ignazio, A.; Marrelli, D.; Swierblewski, M.; Jaskiewicz, J.; Roviello, F.; Polom, K. New Technologies in Breast Cancer Sentinel Lymph Node Biopsy; from the Current Gold Standard to Artificial Intelligence. Surg. Oncol. 2020, 34, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Mathelin, C.; Lodi, M.; President, P.; Slnb, L. Narrative Review of Sentinel Lymph Node Biopsy in Breast Cancer: A Technique in Constant Evolution with Still Numerous Unresolved Questions. Chin. Clin. Oncol. 2021, 10, 20. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, Y.; Akiyama, F.; Iwase, T.; Kaneko, T.; Tsuda, H.; Sato, K.; Ueda, S.; Mano, M.; Masuda, N.; Takeda, M.; et al. Molecular Detection of Lymph Node Metastases in Breast Cancer Patients: Results of a Multicenter Trial Using the One-Step Nucleic Acid Amplification Assay. Clin. Cancer Res. 2009, 15, 2879–2884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basic Evaluation of the Automated Gene Amplification Detector RD-200 and LYNOAMP CK19 | Products & Solutions | Sysmex. Available online: https://www.sysmex.co.jp/en/products_solutions/library/journal/vol29_no1/summary03.html (accessed on 1 August 2022).
- Hortobagyi, G.N.; Connolly, J.L.; D’Orsi, C.J.; Edge, S.B.; Mittendorf, E.A.; Rugo, H.S.; Solin, L.J.; Weaver, D.L.; Winchester, D.J.; Giuliano, A. Breast. In AJCC Cancer Staging Manual; Springer International Publishing: Cham, Switzerland, 2017; pp. 589–636. [Google Scholar]
- WHO Classification of Tumours Editorial Board; International Agency for Research on Cancer; World Health Organization; WHO Classification of Tumours. Breast Tumours, 5th ed.; World Health Organization: Geneva, Switzerland, 2019; ISBN 9789283245001. [Google Scholar]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The Evaluation of Tumor-Infiltrating Lymphocytes (TILS) in Breast Cancer: Recommendations by an International TILS Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Honda, C.; Kurozumi, S.; Katayama, A.; Hanna-Khalil, B.; Masuda, K.; Nakazawa, Y.; Ogino, M.; Obayashi, S.; Yajima, R.; Makiguchi, T.; et al. Prognostic Value of Tumor-Infiltrating Lymphocytes in Estrogen Receptor-Positive and Human Epidermal Growth Factor Receptor 2-Negative Breast Cancer. Mol. Clin. Oncol. 2021, 15, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Performance of the Oncomine Immune Response Research Assay—A Highly Sensitive and Robust Tool for Immune Response Research. Thermo Fisher Scientific. 2017. Available online: https://www.thermofisher.com/pt/en/home/life-science/cancer-research/immuno-oncology-research.html?icid=fl-bid-immuno-oncology (accessed on 26 May 2022).
- Love, M.I.; Huber, W.; Anders, S. Moderated Estimation of Fold Change and Dispersion for RNA-Seq Data with DESeq2. Genome Biol. 2014, 15, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, K.; Wang, R.; Xie, H.; Hu, L.; Wang, C.; Xu, J.; Zhu, C.; Liu, Y.; Gao, F.; Li, X.; et al. Single-Cell RNA Sequencing Reveals Cell Heterogeneity and Transcriptome Profile of Breast Cancer Lymph Node Metastasis. Oncogenesis 2021, 10, 1–12. [Google Scholar] [CrossRef]
- Chauvin, J.M.; Zarour, H.M. TIGIT in Cancer Immunotherapy. J. Immunother. Cancer 2020, 8, e000957. [Google Scholar] [CrossRef]
- Kovács, S.A.; Győrffy, B. Transcriptomic Datasets of Cancer Patients Treated with Immune-Checkpoint Inhibitors: A Systematic Review. J. Transl. Med. 2022, 20, 249. [Google Scholar] [CrossRef] [PubMed]
- Goode, E.F.; Roussos Torres, E.T.; Irshad, S. Lymph Node Immune Profiles as Predictive Biomarkers for Immune Checkpoint Inhibitor Response. Front. Mol. Biosci. 2021, 8, 382. [Google Scholar] [CrossRef] [PubMed]
- Masucci, G.V.; Cesano, A.; Hawtin, R.; Janetzki, S.; Zhang, J.; Kirsch, I.; Dobbin, K.K.; Alvarez, J.; Robbins, P.B.; Selvan, S.R.; et al. Validation of Biomarkers to Predict Response to Immunotherapy in Cancer: Volume I–Pre-Analytical and Analytical Validation. J. Immunother. Cancer 2016, 4, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajendran, B.K.; Deng, C.-X.; Kumar Rajendran, B.; Deng, C.-X. Characterization of Potential Driver Mutations Involved in Human Breast Cancer by Computational Approaches. Oncotarget 2017, 8, 50252–50272. [Google Scholar] [CrossRef] [Green Version]
- The Human Proteome in Lymphoid Tissue–The Human Protein Atlas. Available online: https://www.proteinatlas.org/humanproteome/tissue/lymphoid+tissue#lymph_node (accessed on 4 September 2022).
- Rizwan, A.; Bulte, C.; Kalaichelvan, A.; Cheng, M.; Krishnamachary, B.; Bhujwalla, Z.M.; Jiang, L.; Glunde, K. Metastatic Breast Cancer Cells in Lymph Nodes Increase Nodal Collagen Density. Sci. Rep. 2015, 5, 10002. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, G.; Pai, T.; Hardiman, T.; Avery-Kiejda, K.; Scott, R.J.; Spencer, J.; Pinder, S.E.; Grigoriadis, A. Molecular Patterns of Cancer Colonisation in Lymph Nodes of Breast Cancer Patients. Breast Cancer Res. 2018, 20, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valente, A.L.; Kane, J.L.; Ellsworth, D.L.; Shriver, C.D.; Ellsworth, R.E. Molecular Response of the Axillary Lymph Node Microenvironment to Metastatic Colonization. Clin. Exp. Metastasis 2014, 31, 565–572. [Google Scholar] [CrossRef]
- Blackburn, H.L.; Ellsworth, D.L.; Shriver, C.D.; Ellsworth, R.E. Breast Cancer Metastasis to the Axillary Lymph Nodes: Are Changes to the Lymph Node “Soil” Localized or Systemic? Breast Cancer 2017, 11, 117822341769124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rye, I.H.; Huse, K.; Josefsson, S.E.; Kildal, W.; Danielsen, H.E.; Schlichting, E.; Garred, Ø.; Riis, M.L.; Osbreac; Lingjærde, O.C.; et al. Breast Cancer Metastasis: Immune Profiling of Lymph Nodes Reveals Exhaustion of Effector T Cells and Immunosuppression. Mol. Oncol. 2022, 16, 88–103. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Sahoo, S.; Brien, R.; Jung, S.; Humphries, B.; Lee, W.; Cheng, Y.H.; Zhang, Z.; Luker, K.E.; Wicha, M.S.; et al. Single-Cell RNA-Sequencing of Migratory Breast Cancer Cells: Discovering Genes Associated with Cancer Metastasis. Analyst 2019, 144, 7296–7309. [Google Scholar] [CrossRef] [PubMed]
- Núñez, N.G.; Tosello Boari, J.; Ramos, R.N.; Richer, W.; Cagnard, N.; Anderfuhren, C.D.; Niborski, L.L.; Bigot, J.; Meseure, D.; de La Rochere, P.; et al. Tumor Invasion in Draining Lymph Nodes Is Associated with Treg Accumulation in Breast Cancer Patients. Nat. Commun. 2020, 11, 3272. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Kong, X.; Liu, R.; Xu, F.; Liu, G.; Sun, C. Development of a Novel Immune-Related Gene Prognostic Index for Breast Cancer. Front. Immunol. 2022, 13, 845093. [Google Scholar] [CrossRef] [PubMed]
- Michelakos, T.; Kontos, F.; Barakat, O.; Maggs, L.; Schwab, J.H.; Ferrone, C.R.; Ferrone, S. B7-H3 Targeted Antibody-Based Immunotherapy of Malignant Diseases. Expert Biol. Ther. 2021, 21, 587–602. [Google Scholar] [CrossRef] [PubMed]
- Kontos, F.; Michelakos, T.; Kurokawa, T.; Sadagopan, A.; Schwab, J.H.; Ferrone, C.R.; Ferrone, S. B7-H3: An Attractive Target for Antibody-Based Immunotherapy. Clin. Cancer Res. 2021, 27, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.; Huang, C.; Li, Y.; Umbach, D.M.; Li, L. CDSeqR: Fast Complete Deconvolution for Gene Expression Data from Bulk Tissues. BMC Bioinform. 2021, 22, 1–12. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | OSNA Negative N = 16 | OSNA Positive N = 16 | p-Value |
|---|---|---|---|
| Age, years | |||
| Minimum | 48 | 43 | - |
| Maximum | 78 | 73 | - |
| Mean ± SD | 58.4 ± 7.8 | 58.1 ± 8.4 | 0.552 ¥ |
| BMI, kg/m2 | |||
| Minimum | 18.3 | 16.6 | - |
| Maximum | 33.7 | 36.3 | - |
| Mean ± SD | 25.5 ± 3.5 | 27.0 ± 4.5 | 0.148 ¥ |
| BMI ≥ 30 kg/m2 (%) | 6.3% (n = 1) | 18.8% (n = 3) | 0.300 Φ |
| Gravidity | |||
| Minimum | 0 | 0 | - |
| Maximum | 5 | 4 | - |
| Mean ± SD | 2.1 ± 1.5 | 2.0 ± 1.1 | 0.554 ¥ |
| Parity | |||
| Minimum | 0 | 0 | - |
| Maximum | 3 | 3 | - |
| Mean ± SD | 1.8 ± 1.1 | 1.7 ± 0.9 | 0.569 ¥ |
| Premenopausal status (%) | 12.5% (n = 2) | 18.7% (n = 3) | 0.500 Φ |
| Postmenopausal status (%) | 87.5% (n = 14) | 81.3% (n = 13) | |
| Age of menopause, years | |||
| Minimum | 45 | 45 | - |
| Maximum | 57 | 56 | - |
| Mean ± SD | 51.5 ±3.7 | 50.8 ± 3.5 | 0.705 ¥ |
| Smoker (%) | 18.8% (n = 3) | 13.2% (n = 2) | 0.532 Φ |
| Histological Characteristics of the Tumors | OSNA Negative N = 16 | OSNA Positive N = 16 | p-Value |
|---|---|---|---|
| Histologic type (%) | |||
| No special type (NST) | 75.0% (n = 12) | 93.8% (n = 15) | 0.311 Φ |
| Lobular | 18.8% (n = 3) | 6.3% (n = 1) | |
| Tubular | 6.3% (n = 1) | 0.0% (n = 0) | |
| Tumor diameter, mm | |||
| Minimum | 2.0 | 5.5 | - |
| Maximum | 25.0 | 35.0 | - |
| Mean ± SD | 14.1 ± 6.2 | 16.5 ± 7.6 | 0.173 ¥ |
| Multifocality or multicentricity (%) | 12.5% (n = 2) | 25.0% (n = 4) | 0.327 Φ |
| LVI (%) | 6.3% (n = 1) | 43.8% (n = 7) | 0.019 Φ |
| Grade | |||
| Grade 1 (%) | 75.0% (n = 12) | 31.3% (n = 5) | 0.020 Φ |
| Grade 2 (%) | 18.8% (n = 3) | 56.2% (n = 9) | |
| Grade 3 (%) | 0.0% (n = 0) | 12.5% (n = 2) | |
| Unknown | 6.3% (n = 1) | 0.0% (n = 0) | |
| Mean ± SD | 1.2 ± 0.4 | 1.8 ± 0.7 | 0.006 £ |
| ER, % | |||
| Minimum | 75 | 80 | - |
| Maximum | 100 | 100 | - |
| Mean ± SD | 91.6 ± 8.7 | 96.3 ± 6.5 | 0.081 £ |
| PR, % | |||
| Minimum | 20 | 25 | - |
| Maximum | 100 | 100 | - |
| Mean ± SD | 63.8 ± 26.8 | 75.0 ± 21.7 | 0.101 ¥ |
| Ki67, % | |||
| Minimum | 1 | 2 | - |
| Maximum | 18 | 18 | - |
| Mean ± SD | 7.3 ± 5.1 | 10.4 ± 4.0 | 0.034 ¥ |
| TILs, % | |||
| Low TILs (%) | 37.5% (n = 6) | 31.3% (n = 5) | 0.878 Φ |
| Intermediate TILs (%) | 31.3% (n = 5) | 25.0% (n = 4) | |
| High TILs (%) | 31.3% (n = 5) | 37.5% (n = 6) | |
| Unknown | 0.0% (n = 0) | 6.3% (n = 1) | |
| Mean ± SD | 29.4 ± 28.6 | 32.0 ± 17.6 | 0.647 £ |
| Characteristics of the SLNs | OSNA Negative N = 16 | OSNA Positive N = 16 | p-Value |
|---|---|---|---|
| Technique for SLNs detection (%) | |||
| Patent blue and radioisotope | 56.2% (n = 9) | 75.0% (n = 12) | 0.229 Φ |
| Superparamagnetic iron oxide | 43.8% (n = 7) | 25.0% (n = 4) | |
| Number of removed SLNs | |||
| Minimum | 1 | 1 | - |
| Maximum | 3 | 4 | - |
| Mean ± SD | 1.7 ± 0.8 | 1.8 ± 1.0 | 0.822 £ |
| Number of metastatic SLNs | |||
| 1 metastatic SLN (%) | - | 93.8% (n = 15) | - |
| 2 metastatic SLNs (%) | - | 6.2% (n = 1) | - |
| Mean ± SD | - | 1.1 ± 0.3 | - |
| OSNA result (%) | |||
| Negative (pN0) | 100% (n = 16) | - | - |
| Micrometastases (pN1mi) | - | 43.8% (n = 7) | - |
| Macrometastases (pN1) | - | 56.2% (n = 9) | - |
| OSNA selected sample result | |||
| Minimum | <160 | 280 | - |
| Maximum | <160 | 730,000 | - |
| Mean ± SD | - | 118,560 ± 211,763.5 | - |
| TTL | |||
| Minimum | - | 280 | - |
| Maximum | - | 730,000 | - |
| Mean ± SD | - | 121,238.1 ± 213,294.7 | - |
| Main Characteristics | Cluster 1 (N = 2) | Cluster 2 (N = 7) | Cluster 3 (N = 23) | p-Value |
|---|---|---|---|---|
| Age, years (mean ± SD) | 53.0 ± 7.1 | 56.3 ± 8.4 | 59.3 ± 7.9 | 0.443 Δ |
| BMI, kg/m2 (mean ± SD) | 28.6 ± 6.1 | 27.0 ± 2.3 | 25.8 ± 4.3 | 0.555 Δ |
| Tumor diameter, mm (mean ± SD) | 25.5 ± 13.4 *¥ | 19.1 ± 5.8 | 13.2 ± 5.6 *¥ | 0.009 Δ |
| Tumor grade (mean ± SD) | 2.5 ± 0.7 *£ | 1.7 ± 0.5 | 1.4 ± 0.6 *£ | 0.040 Ψ |
| ER, % (mean ± SD) | 100.0 ± 0.0 | 93.6 ± 7.5 | 93.5 ± 8.3 | 0.438 Ψ |
| PR, % (mean ± SD) | 95.0 ± 7.1 | 65.7 ± 24.1 | 68.3 ± 25.1 | 0.317 Δ |
| Ki67, % (mean ± SD) | 8.5 ± 4.9 | 10.6 ± 4.4 | 8.3 ± 4.9 | 0.571 Δ |
| Lymphovascular invasion (%) | 0.0% (n = 0) | 57.1% (n = 4) | 17.4% (n = 4) | 0.693 Φ |
| TILs, % (mean ± SD) | 20.0 ± 14.1 | 39.3 ± 25.9 | 28.9 ± 28.2 | 0.465 Ψ |
| OSNA sample result | ||||
| Minimum | 12,000 | 4500 | <160 | - |
| Maximum | 730,000 | 430,000 | 8200 | - |
| Mean ± SD | 371,000 ± 507,702.7 | 163,071.4 ± 172,381 | - | - |
| Number of metastatic SLNs (mean ± SD) | 1.0 ± 0.0 | 1.1 ± 0.4 *£ | 0.3 ± 0.5 **£ | <0.001 Ψ |
| TTL (mean ± SD) | 375,950 ± 500,702.3 | 167,778.6 ± 176,584.5 *£ | 1922 ± 2974.6 *£ | 0.005 Ψ |
| ALND (%) | 100.0% (n = 2) | 57.1% (n = 4) | 0.0% (n = 0) | <0.001 Φ |
| Number of non-sentinel LNs with metastases (mean ± SD) | 4 ± 2.8 | 0.5 ± 0.6 | - | 0.057 £ |
| Total number of LNs with metastases (mean ± SD) | 5.0 ± 2.8 *£ | 1.4 ± 0.5 *£ | 0.3 ± 0.5 **£ | <0.001 Ψ |
| Total number of LNs with macrometastases (mean ± SD) | 5.0 ± 2.8 *£ | 1.0 ± 0.6 **£ | 0.0 ± 0.2 **£ | <0.001 Ψ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gante, I.; Ribeiro, J.M.; Mendes, J.; Gomes, A.; Almeida, V.; Regateiro, F.S.; Caramelo, F.; Silva, H.C.; Figueiredo-Dias, M. One Step Nucleic Acid Amplification (OSNA) Lysate Samples Are Suitable to Establish a Transcriptional Metastatic Signature in Patients with Early Stage Hormone Receptors-Positive Breast Cancer. Cancers 2022, 14, 5855. https://doi.org/10.3390/cancers14235855
Gante I, Ribeiro JM, Mendes J, Gomes A, Almeida V, Regateiro FS, Caramelo F, Silva HC, Figueiredo-Dias M. One Step Nucleic Acid Amplification (OSNA) Lysate Samples Are Suitable to Establish a Transcriptional Metastatic Signature in Patients with Early Stage Hormone Receptors-Positive Breast Cancer. Cancers. 2022; 14(23):5855. https://doi.org/10.3390/cancers14235855
Chicago/Turabian StyleGante, Inês, Joana Martins Ribeiro, João Mendes, Ana Gomes, Vânia Almeida, Frederico Soares Regateiro, Francisco Caramelo, Henriqueta Coimbra Silva, and Margarida Figueiredo-Dias. 2022. "One Step Nucleic Acid Amplification (OSNA) Lysate Samples Are Suitable to Establish a Transcriptional Metastatic Signature in Patients with Early Stage Hormone Receptors-Positive Breast Cancer" Cancers 14, no. 23: 5855. https://doi.org/10.3390/cancers14235855
APA StyleGante, I., Ribeiro, J. M., Mendes, J., Gomes, A., Almeida, V., Regateiro, F. S., Caramelo, F., Silva, H. C., & Figueiredo-Dias, M. (2022). One Step Nucleic Acid Amplification (OSNA) Lysate Samples Are Suitable to Establish a Transcriptional Metastatic Signature in Patients with Early Stage Hormone Receptors-Positive Breast Cancer. Cancers, 14(23), 5855. https://doi.org/10.3390/cancers14235855