
TRICIN: A Phase II Trial on the Efficacy of Topical TRIchloroacetic Acid in Patients with Cervical Intraepithelial Neoplasia

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistics
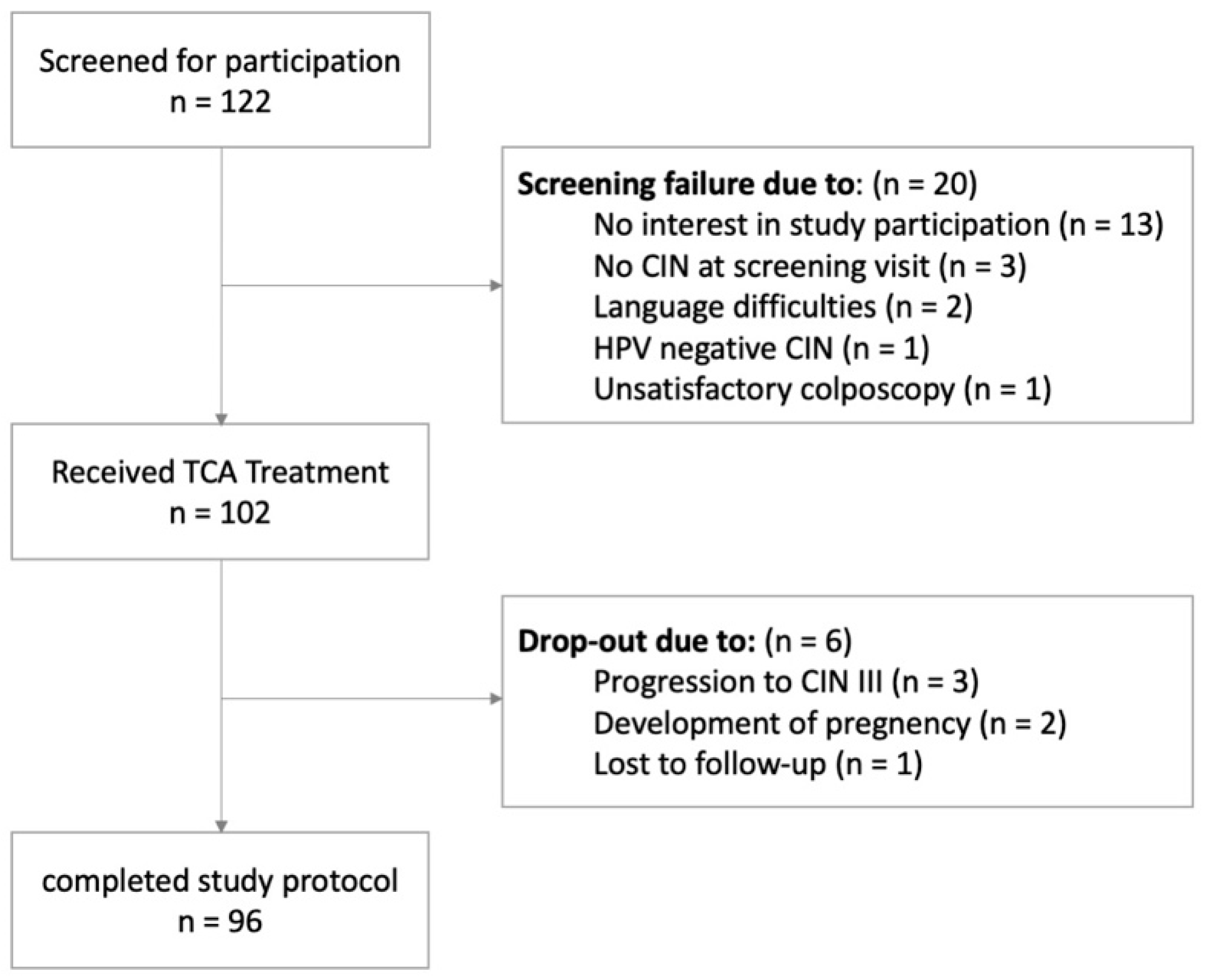
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Insinga, R.P.; Glass, A.G.; Rush, B.B. Diagnoses and outcomes in cervical cancer screening: A population-based study. Am. J. Obstet. Gynecol. 2004, 191, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Perkins, R.B.; Guido, R.S.; Castle, P.E.; Chelmow, D.; Einstein, M.H.; Garcia, F.; Huh, W.K.; Kim, J.J.; Moscicki, A.-B.; Nayar, R.; et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J. Low. Genit. Tract Dis. 2020, 24, 102–131. [Google Scholar] [CrossRef] [Green Version]
- Arbyn, M.; Kyrgiou, M.; Simoens, C.; Raifu, A.O.; Koliopoulos, G.; Martin-Hirsch, P.; Prendiville, W.; Paraskevaidis, E. Perinatal mortality and other severe adverse pregnancy outcomes associated with treatment of cervical intraepithelial neoplasia: Meta-analysis. BMJ 2008, 337, a1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekos, C.; Schwameis, R.; Heinze, G.; Garner, M.; Grimm, C.; Joura, E.; Horvat, R.; Polterauer, S.; Polterauer, M. Influence of age on histologic outcome of cervical intraepithelial neoplasia during observational management: Results from large cohort, systematic review, meta-analysis. Sci. Rep. 2018, 8, 6383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K.; Drake, P. Births: Final Data for 2017. National vital statistics reports: From the Centers for Disease Control and Prevention, National Center for Health Statistics. Natl. Vital Stat. Syst. 2018, 67, 1–50. [Google Scholar]
- Lin, C.; Franceschi, S.; Clifford, G.M. Human papillomavirus types from infection to cancer in the anus, according to sex and HIV status: A systematic review and meta-analysis. Lancet Infect. Dis. 2018, 18, 198–206. [Google Scholar] [CrossRef] [Green Version]
- Cranston, R.D.; Baker, J.R.; Liu, Y.; Wang, L.; Elishaev, E.; Ho, K.S. Topical application of trichloroacetic acid is efficacious for the treatment of internal anal high-grade squamous intraepithelial lesions in HIV-positive men. Sex. Transm. Dis. 2014, 41, 420–426. [Google Scholar] [CrossRef]
- Singh, J.C.; Kuohung, V.; Palefsky, J.M. Efficacy of trichloroacetic acid in the treatment of anal intraepithelial neoplasia in HIV-positive and HIV-negative men who have sex with men. J. Acquir. Immune Defic. Syndr. 2009, 52, 474–479. [Google Scholar]
- Wiley, D.J.; Douglas, J.; Beutner, K.; Cox, T.; Fife, K.; Moscicki, A.B.; Fukumoto, L. External genital warts: Diagnosis, treatment, and prevention. Clin. Infect. Dis. 2002, 35 (Suppl. 2), S210–S224. [Google Scholar] [CrossRef] [Green Version]
- Workowski, K.A.; Bolan, G.A. Sexually transmitted diseases treatment guidelines, 2015. Morb. Mortal. Wkly. Rep. (MMWR) 2015, 64, 1–137. [Google Scholar]
- Geisler, S.; Speiser, S.; Speiser, L.; Heinze, G.; Rosenthal, A.; Speiser, P. Short-Term Efficacy of Trichloroacetic Acid in the Treatment of Cervical Intraepithelial Neoplasia. Obstet. Gynecol. 2016, 127, 353–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bansal, N.; Wright, J.D.; Cohen, C.J.; Herzog, T.J. Natural history of established low grade cervical intraepithelial (CIN 1) lesions. Anticancer Res. 2008, 28, 1763–1766. [Google Scholar] [PubMed]
- Grimm, C.; Polterauer, S.; Natter, C.; Rahhal, J.; Hefler, L.; Tempfer, C.B.; Heinze, G.; Stary, G.; Reinthaller, A.; Speiser, P. Treatment of cervical intraepithelial neoplasia with topical imiquimod: A randomized controlled trial. Obstet. Gynecol. 2012, 120, 152–159. [Google Scholar] [CrossRef]
- Holowaty, P.; Miller, A.B.; Rohan, T.; To, T. Natural history of dysplasia of the uterine cervix. J. Natl. Cancer Inst. 1999, 91, 252–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polterauer, S.; Reich, O.; Widschwendter, A.; Hadjari, L.; Bogner, G.; Reinthaller, A.; Joura, E.; Trutnovsky, G.; Ciresa-Koenig, A.; Ganhoer-Schimboeck, J.; et al. Topical imiquimod compared with conization to treat cervical high-grade squamous intraepithelial lesions: Multicenter, randomized controlled trial. Gynecol. Oncol. 2022, 165, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Cokan, A.; Pakiz, M.; Serdinsek, T.; Dovnik, A.; Kodric, T.; Repse Fokter, A.; Kavalar, R.; But, I. Comparison of Conservative Treatment of Cervical Intraepithelial Lesions with Imiquimod with Standard Excisional Technique Using LLETZ: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 5777. [Google Scholar] [CrossRef] [PubMed]
- Burgos, J.; Martin-Castillo, M.; Landolfi, S.; Dinares, M.C.; Villar, J.; Navarro, J.; Ribera, E.; Falcó, V.; Curran, A. Brief Report: Effectiveness of Trichloroacetic Acid vs. Electrocautery Ablation for the Treatment of Anal High-Grade Squamous Intraepithelial Lesion in HIV-Infected Patients. J. Acquir. Immune. Defic Syndr. 2018, 79, 612–616. [Google Scholar] [CrossRef]
- Ayatollahi, H.; Ershadimoghaddam, S.; Naji, S.; Yekta, Z.; Jalali, Z. Comparison between Single Versus Twice Application of Topical 85% Trichloroacetic Acid in the Treatment of Cervical Intraepithelial Neoplasia; A Randomized Clinical Trial on Efficacy and Tolerability. Asian Pac. J. Cancer Prev. 2022, 23, 947–952. [Google Scholar] [CrossRef]
- Rajalingam, D.; Loftis, C.; Xu, J.J.; Kumar, T.K. Trichloroacetic acid-induced protein precipitation involves the reversible association of a stable partially structured intermediate. Protein Sci. 2009, 18, 980–993. [Google Scholar] [CrossRef] [Green Version]
- Melnikow, J.; Nuovo, J.; Willan, A.R.; Chan, B.K.; Howell, L.P. Natural history of cervical squamous intraepithelial lesions: A meta-analysis. Obstet. Gynecol. 1998, 92, 727–735. [Google Scholar] [CrossRef]
- Wright, T.C., Jr.; Massad, L.S.; Dunton, C.J.; Spitzer, M.; Wilkinson, E.J.; Solomon, D.; 2006 American Society for Colposcopy and Cervical Pathology-sponsored Consensus Conference. 2006 consensus guidelines for the management of women with cervical intraepithelial neoplasia or adenocarcinoma in situ. Am. J. Obstet. Gynecol. 2007, 197, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Redman, C.W.E.; Verdoodt, F.; Kyrgiou, M.; Tzafetas, M.; Ghaem-Maghami, S.; Petry, K.-U.; Leeson, S.; Bergeron, C.; Nieminen, P.; et al. Incomplete excision of cervical precancer as a predictor of treatment failure: A systematic review and meta-analysis. Lancet Oncol. 2017, 18, 1665–1679. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Patient’s age * | 26.6 (19.3–50.0) |
| Tobacco use | |
| non-smoker | 63 (61.8) |
| <5 cigarettes/day | 17 (16.7) |
| 5–9 cigarettes/day | 8 (7.8) |
| 10–19 cigarettes/day | 12 (11.8) |
| >20 cigarettes/day | 2 (2.0) |
| Body Mass Index (kg/m2) | 23.7 (4.8) |
| Number of previous sexual partners * | 7 (1–65) |
| Immunologic disorder | |
| None | 101 (99.0) |
| Crohn’s disease | 1 (1.0) |
| History of STD | |
| HPV infection | 92 (90.2) |
| Chlamydia infection | 5 (4.9) |
| Previous Treatment for CIN | 3 (2.9) |
| Condylomata accuminata | 2 (2.0) |
| Previous pregnancies * | 0 (0–4) |
| Previous deliveries * | 0 (0–3) |
| Days from last menstrual period * | 18.5 (10.0–27.75) |
| Current contraception method | |
| None | 11 (10.8) |
| Oral contraceptive | 45 (44.1) |
| Intravaginal ring | 3 (2.9) |
| Barrier method (condom) | 36 (35.3) |
| Cooper IUD | 5 (4.9) |
| Hormonal IUD | 1 (1.0) |
| Unknown | 1 (1.0) |
| CIN I (n/%) | CIN II (n/%) | |
|---|---|---|
| Number of patients | 76 (74.5) | 26 (25.5) |
| HPV 16 | 20 (26.3) | 14 (53.8) |
| HPV 18 | 12 (15.8) | 0 (0) |
| Other high-risk HPV | 63 (82.9) | 20 (76.9) |
| multiple HPV types | 17 (22.4) | 8 (30.8) |
| 3 Months (n/%) | 6 Months (n/%) | |||
|---|---|---|---|---|
| Lesion Grade at Study Inclusion | CIN I (n = 76) | CIN II (n = 26) | CIN I (n = 76) | CIN II (n = 26) |
| Remission | ||||
| No CIN | 56 (73.7) | 21 (80.8) | 60 (78.9) | 20 (76.9) |
| Regression | ||||
| CIN I | - | 3 (11.5) | - | 5 (19.2) |
| Persistence | ||||
| CIN II | - | 1 (3.8) | - | - |
| CIN I | 14 (18.4) | - | 8 (10.5) | - |
| Progression | ||||
| CIN III | 2 (2.6) | 1 (3.8) | - | - |
| CIN II | 1 (1.3) | - | 3 (4.2) | - |
| Drop out | 3 (3.9) | 5 (6.6) | 1 (3.8) | |
| 3 Months | 6 Months | |||||
|---|---|---|---|---|---|---|
| Lesion Grade | HPV Type 16 | HPV Type 18 | Other HR Types | HPV Type 16 | HPV Type 18 | Other HR Types |
| CIN II Clearance | 71.4% (41.9–91.6%) | - | 75.0% (50.9–91.3%) | 78.6% (49.2–95.3) | - | 75.0% (50.9–91.3%) |
| CIN I Clearance | 85.0% (62.1–96.8%) | 81.8% (48.2–97.7%) | 60.3% (47.2–72.4%) | 75.0% (50.9–91.3%) | 91.7% (61.5–99.8%) | 66.7% (53.7–78.0%) |
| Total Clearance | 79.4% (62.1–91.3%) | 81.8% (48.2–97.7%) | 63.9% (52.6–74.1%) | 76.5% (58.8–89.3%) | 91.7% (61.5–99.8%) | 68.7% (57.6–78.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwameis, R.; Ganhoer-Schimboeck, J.; Hadjari, V.L.; Hefler, L.; Bergmeister, B.; Küssel, T.; Gittler, G.; Steindl-Schoenhuber, T.; Grimm, C. TRICIN: A Phase II Trial on the Efficacy of Topical TRIchloroacetic Acid in Patients with Cervical Intraepithelial Neoplasia. Cancers 2022, 14, 5991. https://doi.org/10.3390/cancers14235991
Schwameis R, Ganhoer-Schimboeck J, Hadjari VL, Hefler L, Bergmeister B, Küssel T, Gittler G, Steindl-Schoenhuber T, Grimm C. TRICIN: A Phase II Trial on the Efficacy of Topical TRIchloroacetic Acid in Patients with Cervical Intraepithelial Neoplasia. Cancers. 2022; 14(23):5991. https://doi.org/10.3390/cancers14235991
Chicago/Turabian StyleSchwameis, Richard, Julia Ganhoer-Schimboeck, Victoria Laudia Hadjari, Lukas Hefler, Birgit Bergmeister, Tatjana Küssel, Gunda Gittler, Theodora Steindl-Schoenhuber, and Christoph Grimm. 2022. "TRICIN: A Phase II Trial on the Efficacy of Topical TRIchloroacetic Acid in Patients with Cervical Intraepithelial Neoplasia" Cancers 14, no. 23: 5991. https://doi.org/10.3390/cancers14235991
APA StyleSchwameis, R., Ganhoer-Schimboeck, J., Hadjari, V. L., Hefler, L., Bergmeister, B., Küssel, T., Gittler, G., Steindl-Schoenhuber, T., & Grimm, C. (2022). TRICIN: A Phase II Trial on the Efficacy of Topical TRIchloroacetic Acid in Patients with Cervical Intraepithelial Neoplasia. Cancers, 14(23), 5991. https://doi.org/10.3390/cancers14235991