

Dual NGS Comparative Analysis of Liquid Biopsy (LB) and Formalin-Fixed Paraffin-Embedded (FFPE) Samples of Non-Small Cell Lung Carcinoma (NSCLC)

 ,
,  ,
,  ,
,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Immunohistochemistry Detection
2.3. Liquid Biopsy and the cfDNA NGS Panel
2.4. Tumor Tissue and gDNA NGS Panel
2.5. NGS and Sequence Analysis
2.6. Tumor Tissue and PCR Evaluation of EGFR Pathogenic Variants
2.7. Data Analysis
3. Results
3.1. NSCLC Patients Group Characteristics
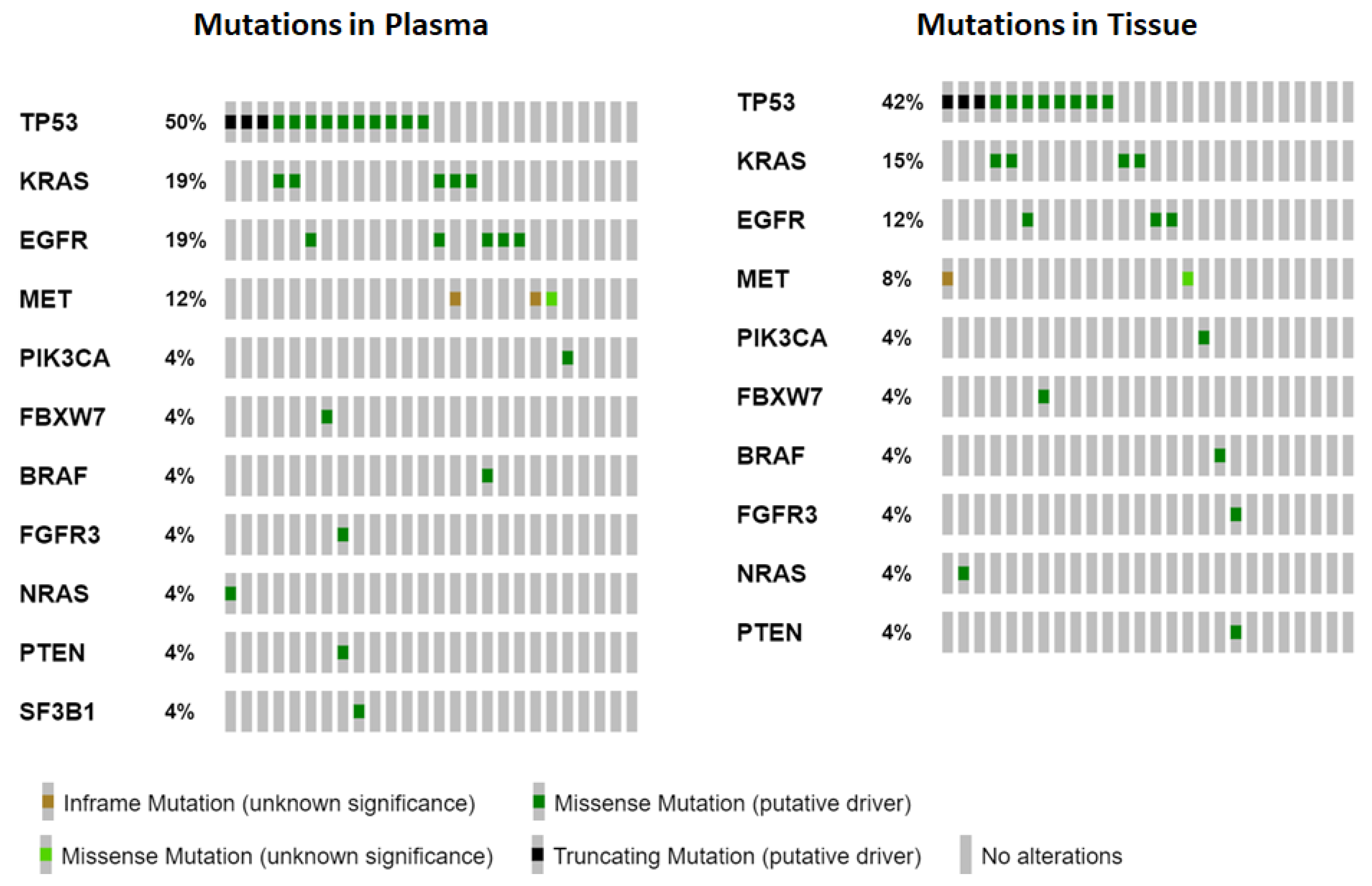
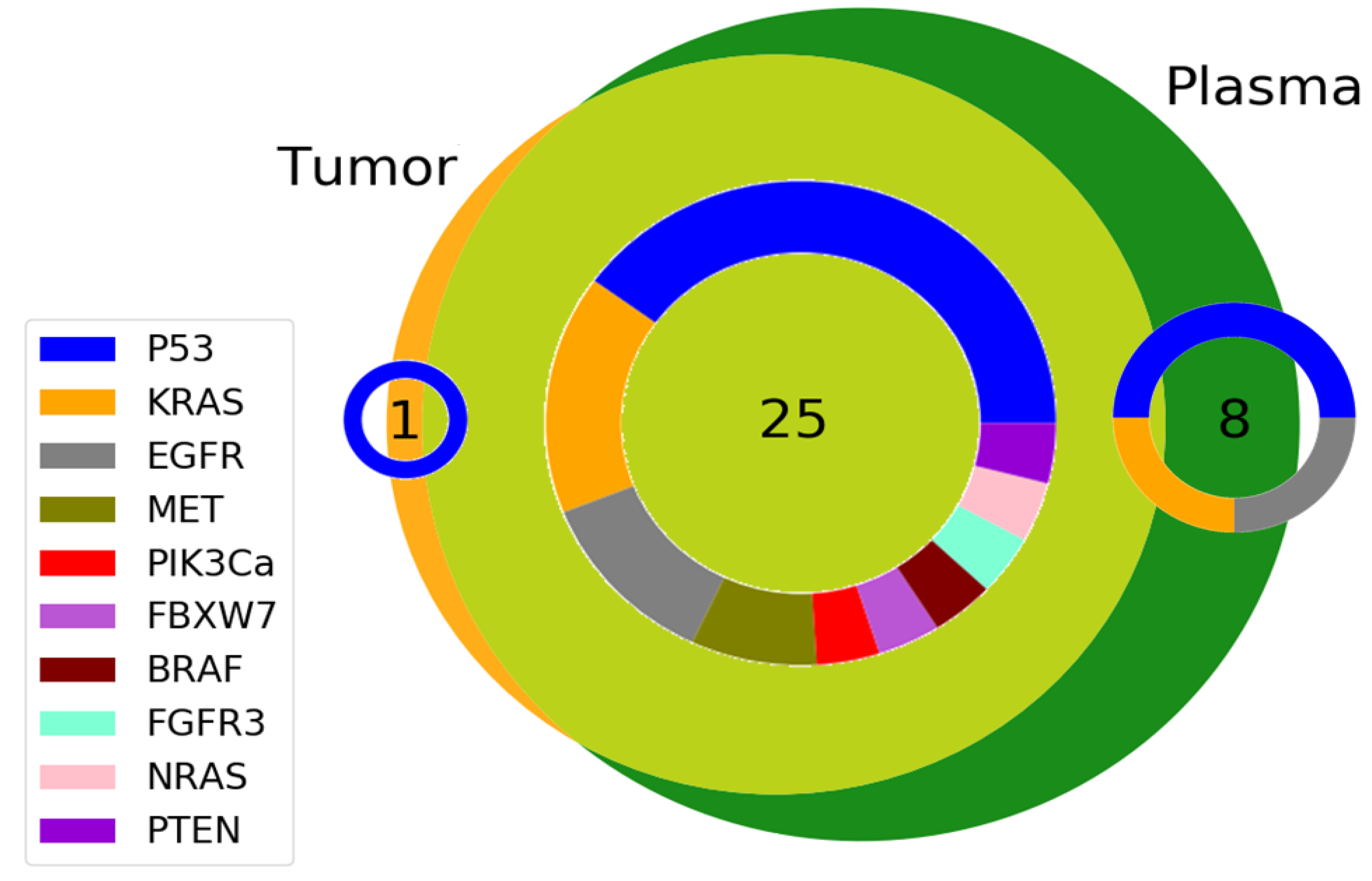
3.2. Gene Variants Detected
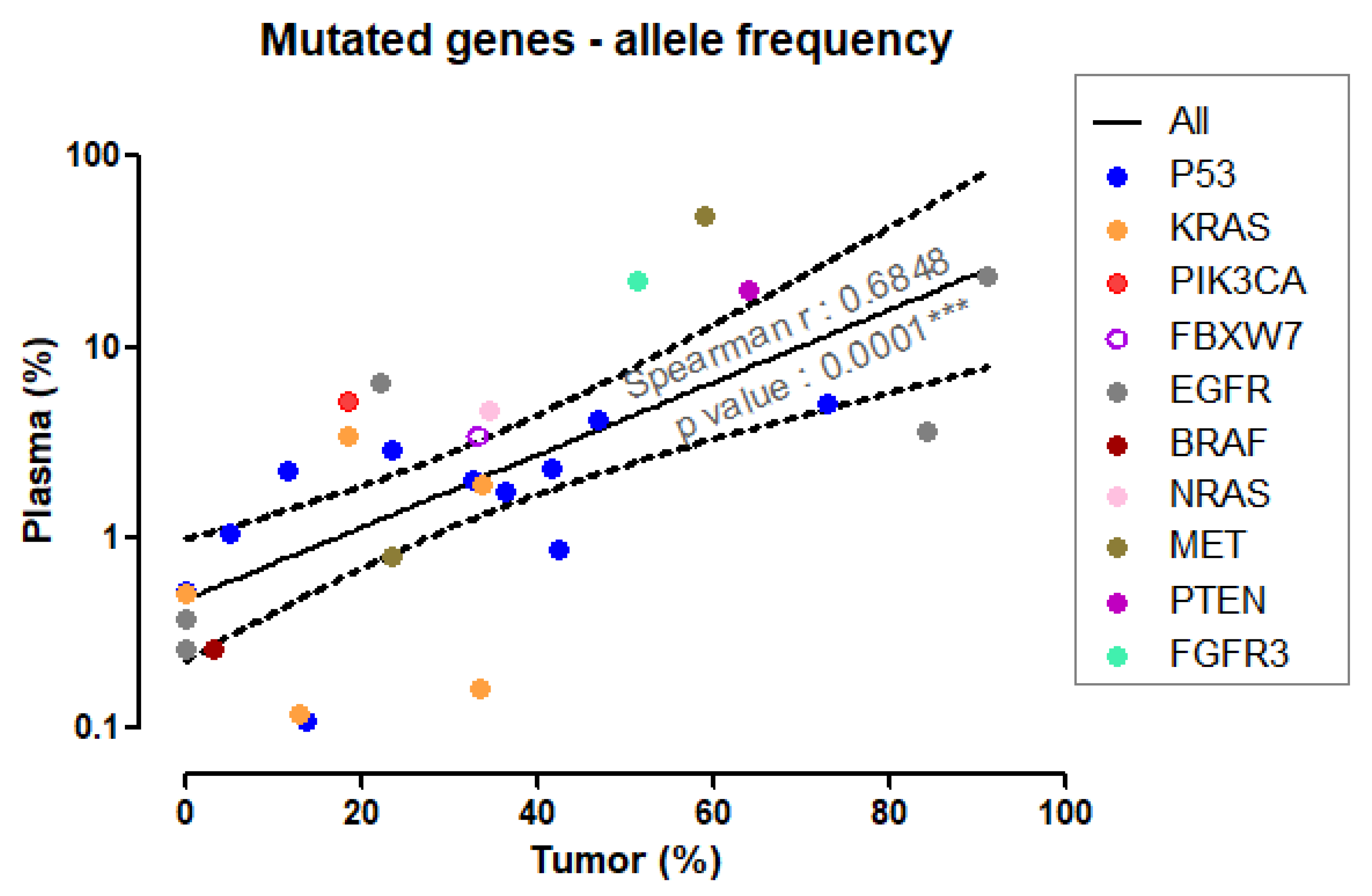
3.3. Variant Allelic Frequency for Different Genes in Plasma and Tumor Tissue
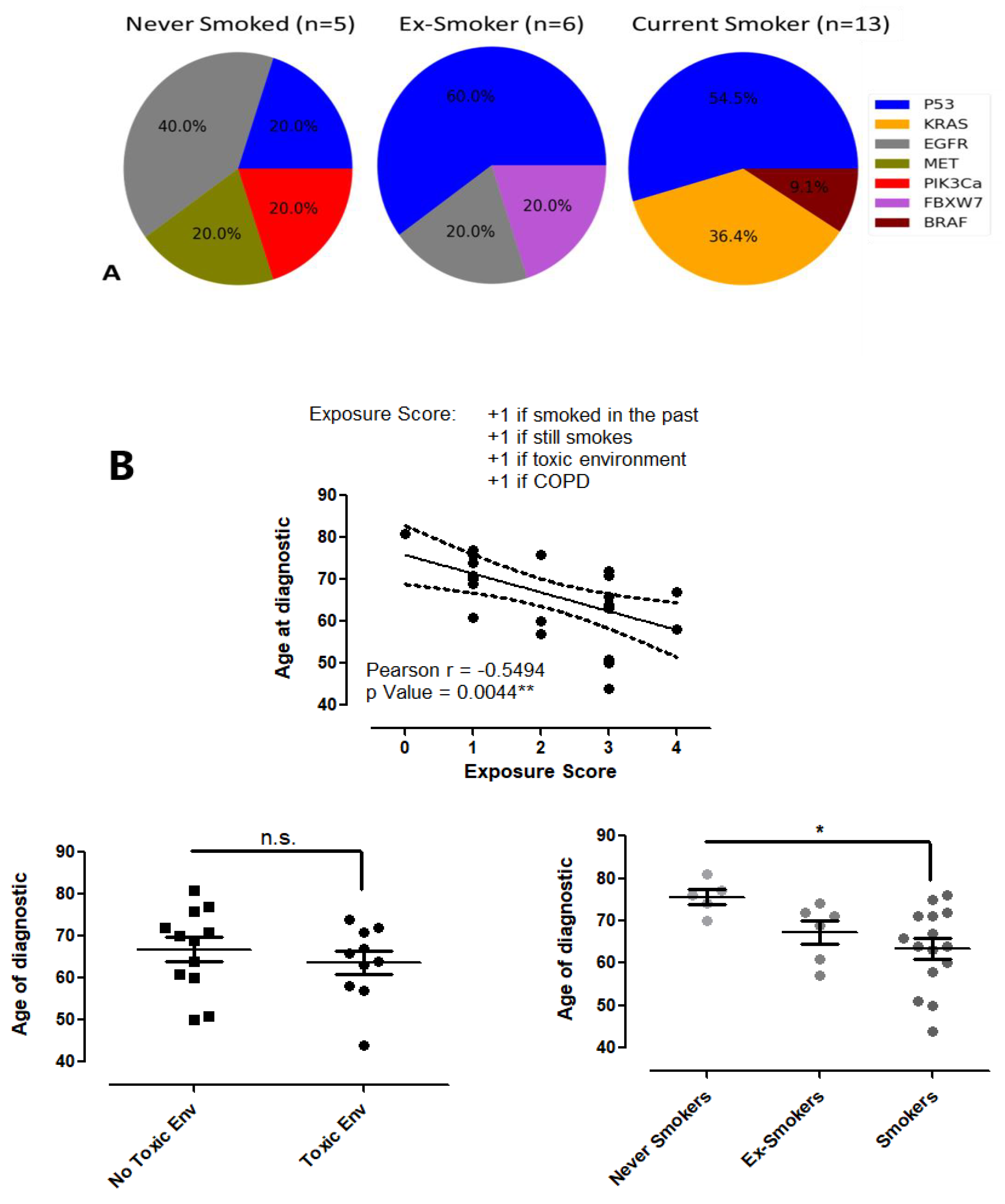
3.4. The Correlation between Risk Factors and Lung Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Alberg, A.J.; Brock, M.V.; Ford, J.G.; Samet, J.M.; Spivack, S.D. Epidemiology of Lung Cancer: Diagnosis and Management of Lung Cancer: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2013, 143, e1S–e29S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, R. Mapping of Global, Regional and National Incidence, Mortality and Mortality-to-Incidence Ratio of Lung Cancer in 2020 and 2050. Int. J. Clin. Oncol. 2022, 27, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Hecht, S.S. Progress and Challenges in Selected Areas of Tobacco Carcinogenesis. Chem. Res. Toxicol. 2008, 21, 160–171. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, K.; Gowers, K.H.; Lee-Six, H.; Chandrasekharan, D.P.; Coorens, T.; Maughan, E.F.; Beal, K.; Menzies, A.; Millar, F.R.; Anderson, E. Tobacco Smoking and Somatic Mutations in Human Bronchial Epithelium. Nature 2020, 578, 266–272. [Google Scholar] [CrossRef]
- Khoo, C.; Rogers, T.-M.; Fellowes, A.; Bell, A.; Fox, S. Molecular Methods for Somatic Mutation Testing in Lung Adenocarcinoma: EGFR and Beyond. Transl. Lung Cancer Res. 2015, 4, 126. [Google Scholar]
- Hussen, B.M.; Abdullah, S.T.; Salihi, A.; Sabir, D.K.; Sidiq, K.R.; Rasul, M.F.; Hidayat, H.J.; Ghafouri-Fard, S.; Taheri, M.; Jamali, E. The Emerging Roles of NGS in Clinical Oncology and Personalized Medicine. Pathol. Res. Pract. 2022, 230, 153760. [Google Scholar] [CrossRef]
- De Maglio, G.; Pasello, G.; Dono, M.; Fiorentino, M.; Follador, A.; Sciortino, M.; Malapelle, U.; Tiseo, M. The Storm of NGS in NSCLC Diagnostic-Therapeutic Pathway: How to Sun the Real Clinical Practice. Crit. Rev. Oncol. 2022, 169, 103561. [Google Scholar] [CrossRef]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; Hirsch, F.R.; Kerr, K. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors: Guideline from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. J. Thorac. Oncol. 2018, 13, 323–358. [Google Scholar]
- Rolfo, C.; Mack, P.C.; Scagliotti, G.V.; Baas, P.; Barlesi, F.; Bivona, T.G.; Herbst, R.S.; Mok, T.S.; Peled, N.; Pirker, R. Liquid Biopsy for Advanced Non-Small Cell Lung Cancer (NSCLC): A Statement Paper from the IASLC. J. Thorac. Oncol. 2018, 13, 1248–1268. [Google Scholar] [CrossRef] [Green Version]
- Tan, A.C. The Role of Liquid Biopsy in the Diagnostic Testing Algorithm for Advanced Lung Cancer. Onco 2022, 2, 181–185. [Google Scholar] [CrossRef]
- Robinson, J.T.; Thorvaldsdóttir, H.; Wenger, A.M.; Zehir, A.; Mesirov, J.P. Variant Review with the Integrative Genomics Viewer. Cancer Res. 2017, 77, e31–e34. [Google Scholar] [CrossRef] [PubMed]
- Karlovich, C.; Goldman, J.W.; Sun, J.-M.; Mann, E.; Sequist, L.V.; Konopa, K.; Wen, W.; Angenendt, P.; Horn, L.; Spigel, D. Assessment of EGFR Mutation Status in Matched Plasma and Tumor Tissue of NSCLC Patients from a Phase I Study of Rociletinib (CO-1686) Plasma/Tissue EGFR Analysis from a Phase I Rociletinib Study. Clin. Cancer Res. 2016, 22, 2386–2395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirtavoos-Mahyari, H.; Ghafouri-Fard, S.; Khosravi, A.; Motevaseli, E.; Esfahani-Monfared, Z.; Seifi, S.; Salimi, B.; Oskooei, V.K.; Ghadami, M.; Modarressi, M.H. Circulating Free DNA Concentration as a Marker of Disease Recurrence and Metastatic Potential in Lung Cancer. Clin. Transl. Med. 2019, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Razavi, P.; Li, B.T.; Brown, D.N.; Jung, B.; Hubbell, E.; Shen, R.; Abida, W.; Juluru, K.; De Bruijn, I.; Hou, C. High-Intensity Sequencing Reveals the Sources of Plasma Circulating Cell-Free DNA Variants. Nat. Med. 2019, 25, 1928–1937. [Google Scholar] [CrossRef]
- Spoor, J.; Eyck, B.M.; Atmodimedjo, P.N.; Jansen, M.P.; Helmijr, J.C.; Martens, J.W.; van der Wilk, B.J.; van Lanschot, J.J.B.; Dinjens, W.N. Liquid Biopsy in Esophageal Cancer: A Case Report of False-Positive Circulating Tumor DNA Detection Due to Clonal Hematopoiesis. Ann. Transl. Med. 2021, 9, 1264. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A. Non–Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 497–530. [Google Scholar] [CrossRef]
- Pereira, B.; Chen, C.T.; Goyal, L.; Walmsley, C.; Pinto, C.J.; Baiev, I.; Allen, R.; Henderson, L.; Saha, S.; Reyes, S. Cell-Free DNA Captures Tumor Heterogeneity and Driver Alterations in Rapid Autopsies with Pre-Treated Metastatic Cancer. Nat. Commun. 2021, 12, 1–13. [Google Scholar] [CrossRef]
- Parikh, A.R.; Leshchiner, I.; Elagina, L.; Goyal, L.; Levovitz, C.; Siravegna, G.; Livitz, D.; Rhrissorrakrai, K.; Martin, E.E.; Van Seventer, E.E. Liquid versus Tissue Biopsy for Detecting Acquired Resistance and Tumor Heterogeneity in Gastrointestinal Cancers. Nat. Med. 2019, 25, 1415–1421. [Google Scholar] [CrossRef]
- Chabon, J.J.; Simmons, A.D.; Lovejoy, A.F.; Esfahani, M.S.; Newman, A.M.; Haringsma, H.J.; Kurtz, D.M.; Stehr, H.; Scherer, F.; Karlovich, C.A. Circulating Tumour DNA Profiling Reveals Heterogeneity of EGFR Inhibitor Resistance Mechanisms in Lung Cancer Patients. Nat. Commun. 2016, 7, 1–15. [Google Scholar]
- Zhou, J.; Zhao, C.; Zhao, J.; Wang, Q.; Chu, X.; Li, J.; Zhou, F.; Ren, S.; Li, X.; Su, C. Re-biopsy and Liquid Biopsy for Patients with Non-small Cell Lung Cancer after EGFR-tyrosine Kinase Inhibitor Failure. Thorac. Cancer 2019, 10, 957–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavic, M.; Krivokuca, A.; Pavlovic, M.; Boljevic, I.; Rakobradovic, J.; Mihajlovic, M.; Tanic, M.; Damjanovic, A.; Malisic, E.; Jankovic, R. EGFR Mutation Testing from Liquid Biopsy of Non-Small Cell Lung Cancer at the Institute for Oncology and Radiology of Serbia. J. BUON 2020, 25, 2635–2642. [Google Scholar]
- Kim, C.H.; Kim, S.H.; Park, S.Y.; Yoo, J.; Kim, S.K.; Kim, H.K. Identification of EGFR Mutations by Immunohistochemistry with EGFR Mutation-Specific Antibodies in Biopsy and Resection Specimens from Pulmonary Adenocarcinoma. Cancer Res. Treat 2015, 47, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Yotsukura, M.; Yasuda, H.; Shigenobu, T.; Kaseda, K.; Masai, K.; Hayashi, Y.; Hishida, T.; Ohtsuka, T.; Naoki, K.; Soejima, K. Clinical and Pathological Characteristics of EGFR Mutation in Operable Early-Stage Lung Adenocarcinoma. Lung Cancer 2017, 109, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Kumari, N.; Singh, S.; Haloi, D.; Mishra, S.K.; Krishnani, N.; Nath, A.; Neyaz, Z. Epidermal Growth Factor Receptor Mutation Frequency in Squamous Cell Carcinoma and Its Diagnostic Performance in Cytological Samples: A Molecular and Immunohistochemical Study. World J. Oncol. 2019, 10, 142. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, E.; Sugita, M.; Furukawa, K.; Takahashi, H.; Uchida, O.; Kawaguchi, Y.; Ohira, T.; Matsubayashi, J.; Ikeda, N.; Hirsch, F.R. Frequency and Significance of Epidermal Growth Factor Receptor Mutations Detected by PCR Methods in Patients with Non-small Cell Lung Cancer. Oncol. Lett. 2019, 17, 5125–5131. [Google Scholar] [CrossRef] [Green Version]
- Kimura, H.; Ohira, T.; Uchida, O.; Matsubayashi, J.; Shimizu, S.; Nagao, T.; Ikeda, N.; Nishio, K. Analytical Performance of the Cobas EGFR Mutation Assay for Japanese Non-Small-Cell Lung Cancer. Lung Cancer 2014, 83, 329–333. [Google Scholar] [CrossRef]
- Choudhury, Y.; Tan, M.-H.; Shi, J.L.; Tee, A.; Ngeow, K.C.; Poh, J.; Goh, R.R.; Mong, J. Complementing Tissue Testing With Plasma Mutation Profiling Improves Therapeutic Decision-Making for Patients With Lung Cancer. Front. Med. 2022, 9, 758464. [Google Scholar] [CrossRef]
- Denis, M.G.; Lafourcade, M.-P.; Le Garff, G.; Dayen, C.; Falchero, L.; Thomas, P.; Locher, C.; Oliviero, G.; Licour, M.; Reck, M. Circulating Free Tumor-Derived DNA to Detect EGFR Mutations in Patients with Advanced NSCLC: French Subset Analysis of the ASSESS Study. J. Thorac. Dis. 2019, 11, 1370. [Google Scholar] [CrossRef]
- Mogi, A.; Kuwano, H. TP53 Mutations in Nonsmall Cell Lung Cancer. J. Biomed. Biotechnol. 2011, 583929. [Google Scholar] [CrossRef] [Green Version]
- Scoccianti, C.; Vesin, A.; Martel, G.; Olivier, M.; Brambilla, E.; Timsit, J.-F.; Tavecchio, L.; Brambilla, C.; Field, J.K.; Hainaut, P. Prognostic Value of TP53, KRAS and EGFR Mutations in Nonsmall Cell Lung Cancer: The EUELC Cohort. Eur. Respir. J. 2012, 40, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aisner, D.L.; Sholl, L.M.; Berry, L.D.; Rossi, M.R.; Chen, H.; Fujimoto, J.; Moreira, A.L.; Ramalingam, S.S.; Villaruz, L.C.; Otterson, G.A. The Impact of Smoking and TP53 Mutations in Lung Adenocarcinoma Patients with Targetable Mutations—The Lung Cancer Mutation Consortium (LCMC2) Multi-Institutional Profiling of Lung Adenocarcinomas. Clin. Cancer Res. 2018, 24, 1038–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbour, K.C.; Jordan, E.; Kim, H.R.; Dienstag, J.; Yu, H.A.; Sanchez-Vega, F.; Lito, P.; Berger, M.; Solit, D.B.; Hellmann, M. Effects of Co-Occurring Genomic Alterations on Outcomes in Patients with KRAS-Mutant Non–Small Cell Lung CancerCo-Occurring Genomic Alterations in KRAS-Mutant NSCLC. Clin. Cancer Res. 2018, 24, 334–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, K.; Hou, H.; Liang, Y.; Zhang, X. Prognostic Value of TP53 Concurrent Mutations for EGFR-TKIs and ALK-TKIs Based Targeted Therapy in Advanced Non-Small Cell Lung Cancer: A Meta-Analysis. BMC Cancer 2020, 20, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, I.; Zugazagoitia, J.; Herbertz, S.; John, W.; Paz-Ares, L.; Schmid-Bindert, G. KRAS-Mutant Non-Small Cell Lung Cancer: From Biology to Therapy. Lung Cancer 2018, 124, 53–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guibert, N.; Ilie, M.; Long, E.; Hofman, V.; Bouhlel, L.; Brest, P.; Mograbi, B.; Marquette, C.; Didier, A.; Mazieres, J. KRAS Mutations in Lung Adenocarcinoma: Molecular and Epidemiological Characteristics, Methods for Detection, and Therapeutic Strategy Perspectives. Curr. Mol. Med. 2015, 15, 418–432. [Google Scholar] [CrossRef]
- Lin, J.J.; Cardarella, S.; Lydon, C.A.; Dahlberg, S.E.; Jackman, D.M.; Jänne, P.A.; Johnson, B.E. Five-Year Survival in EGFR-Mutant Metastatic Lung Adenocarcinoma Treated with EGFR-TKIs. J. Thorac. Oncol. 2016, 11, 556–565. [Google Scholar] [CrossRef] [Green Version]
- Sakata, S.; Otsubo, K.; Yoshida, H.; Ito, K.; Nakamura, A.; Teraoka, S.; Matsumoto, N.; Shiraishi, Y.; Haratani, K.; Tamiya, M. Real-world Data on NGS Using the Oncomine DxTT for Detecting Genetic Alterations in Non-small-cell Lung Cancer: WJOG13019L. Cancer Sci. 2022, 113, 221. [Google Scholar] [CrossRef]
- Jin, R.; Peng, L.; Shou, J.; Wang, J.; Jin, Y.; Liang, F.; Zhao, J.; Wu, M.; Li, Q.; Zhang, B. EGFR-Mutated Squamous Cell Lung Cancer and Its Association with Outcomes. Front. Oncol. 2021, 11, 2262. [Google Scholar] [CrossRef]
- Gormally, E.; Vineis, P.; Matullo, G.; Veglia, F.; Caboux, E.; Le Roux, E.; Peluso, M.; Garte, S.; Guarrera, S.; Munnia, A. TP53 and KRAS2 Mutations in Plasma DNA of Healthy Subjects and Subsequent Cancer Occurrence: A Prospective Study. Cancer Res. 2006, 66, 6871–6876. [Google Scholar] [CrossRef] [Green Version]
- Husgafvel-Pursiainen, K.; Boffetta, P.; Kannio, A.; Nyberg, F.; Pershagen, G.; Mukeria, A.; Constantinescu, V.; Fortes, C.; Benhamou, S. P53 Mutations and Exposure to Environmental Tobacco Smoke in a Multicenter Study on Lung Cancer. Cancer Res. 2000, 60, 2906–2911. [Google Scholar] [PubMed]
- Halvorsen, A.R.; Silwal-Pandit, L.; Meza-Zepeda, L.A.; Vodak, D.; Vu, P.; Sagerup, C.; Hovig, E.; Myklebost, O.; Børresen-Dale, A.-L.; Brustugun, O.T. TP53 Mutation Spectrum in Smokers and Never Smoking Lung Cancer Patients. Front. Genet. 2016, 7, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, S.; Schiller, J.H.; Gazdar, A.F. Lung Cancer in Never Smokers—A Different Disease. Nat. Rev. Cancer 2007, 7, 778–790. [Google Scholar] [CrossRef]
- Krawczyk, P.; Grzycka-Kowalczyk, L.; Błach, J.; Reszka, K.; Chmielewska, I.; Kieszko, R.; Wójcik-Superczyńska, M.; Szczyrek, M.; Jankowski, T.; Milanowski, J. The Efficacy of T790M Mutation Testing in Liquid Biopsy—Real Clinic Data. PLoS ONE 2022, 17, e0267846. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Naoki, K.; Manabe, T.; Masuzawa, K.; Hasegawa, H.; Yasuda, H.; Kawada, I.; Soejima, K.; Betsuyaku, T. Comparison of Detection Methods of EGFR T790M Mutations Using Plasma, Serum, and Tumor Tissue in EGFR-TKI-Resistant Non-Small Cell Lung Cancer. OncoTargets Ther. 2018, 11, 3335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Luca, G.; Lastraioli, S.; Conte, R.; Mora, M.; Genova, C.; Rossi, G.; Tagliamento, M.; Coco, S.; Dal Bello, M.G.; Zupo, S. Performance of the OncomineTM Lung CfDNA Assay for Liquid Biopsy by NGS of NSCLC Patients in Routine Laboratory Practice. Appl. Sci. 2020, 10, 2895. [Google Scholar] [CrossRef]
- Wolf, J.; Seto, T.; Han, J.-Y.; Reguart, N.; Garon, E.B.; Groen, H.J.; Tan, D.S.; Hida, T.; de Jonge, M.; Orlov, S.V. Capmatinib in MET Exon 14–Mutated or MET-Amplified Non–Small-Cell Lung Cancer. New Engl. J. Med. 2020, 383, 944–957. [Google Scholar] [CrossRef]
- Paik, P.K.; Felip, E.; Veillon, R.; Sakai, H.; Cortot, A.B.; Garassino, M.C.; Mazieres, J.; Viteri, S.; Senellart, H.; Van Meerbeeck, J. Tepotinib in Non–Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations. New Engl. J. Med. 2020, 383, 931–943. [Google Scholar] [CrossRef]
- Bauml, J.M.; Li, B.T.; Velcheti, V.; Govindan, R.; Curioni-Fontecedro, A.; Dooms, C.; Takahashi, T.; Duda, A.W.; Odegaard, J.I.; Cruz-Guilloty, F. Clinical Validation of Guardant360 CDx as a Blood-Based Companion Diagnostic for Sotorasib. Lung Cancer 2022, 166, 270–278. [Google Scholar] [CrossRef]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M. Detection of Circulating Tumor DNA in Early-and Late-Stage Human Malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, M.G.O.; Cruz-Martins, N.; Machado, J.C.; Costa, J.L.; Hespanhol, V. The Value of Cell-Free Circulating Tumour DNA Profiling in Advanced Non-Small Cell Lung Cancer (NSCLC) Management. Cancer Cell Int. 2021, 21, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, C.; Rolfo, C.D.; Oxnard, G.R.; Gray, J.E.; Sholl, L.M.; Gandara, D.R. Strategies for the Successful Implementation of Plasma-Based NSCLC Genotyping in Clinical Practice. Nat. Rev. Clin. Oncol. 2021, 18, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Leighl, N.B.; Page, R.D.; Raymond, V.M.; Daniel, D.B.; Divers, S.G.; Reckamp, K.L.; Villalona-Calero, M.A.; Dix, D.; Odegaard, J.I.; Lanman, R.B. Clinical Utility of Comprehensive Cell-Free DNA Analysis to Identify Genomic Biomarkers in Patients with Newly Diagnosed Metastatic Non–Small Cell Lung CancercfDNA Clinical Utility to Identify NSCLC Genomic Biomarkers. Clin. Cancer Res. 2019, 25, 4691–4700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rijavec, E.; Coco, S.; Genova, C.; Rossi, G.; Longo, L.; Grossi, F. Liquid Biopsy in Non-Small Cell Lung Cancer: Highlights and Challenges. Cancers 2019, 12, 17. [Google Scholar] [CrossRef] [PubMed]
- Fenizia, F.; Pasquale, R.; Roma, C.; Bergantino, F.; Iannaccone, A.; Normanno, N. Measuring Tumor Mutation Burden in Non-Small Cell Lung Cancer: Tissue versus Liquid Biopsy. Transl. Lung Cancer Res. 2018, 7, 668. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Antigen | Clone | Provider |
|---|---|---|---|
| 1 | TTF1 | SP141 | Ventana Medical Systems, Tucson, AZ, USA |
| 2 | CK7 | SP52 | |
| 3 | KI67 | 30-9 | |
| 4 | Synaptophysin | SP11 | |
| 5 | Vimentin | v9 | |
| 6 | CD5 | SP19 | |
| 7 | PD-L1 | SP263 | |
| 8 | ALK | D5F3 | |
| 9 | Calretinin | SP65 | |
| 10 | CK20 | SP33 | |
| 11 | PAX8 | MRQ-50 | |
| 12 | P63 | 7JUL | Leica Biosystems, Deer Park, IL, USA |
| 13 | Chromogranin A | 5H7 | |
| 14 | Wilms’ Tumor | WT49 | |
| 15 | CDX2 | EP25 | |
| 16 | CA19.9 | Syalyl Lewis C241:5:1:4 | |
| 17 | ER | 6F11 | |
| 18 | GATA3 | L50-823 | Bio SB, Santa Barbara, CA, USA |
| 19 | P40 | ZR8 | |
| 20 | PD-L1 | 22C3 | Agilent Technologies, Santa Clara, CA, USA |
| Never Smoked | Ex-Smokers | Current Smokers | All Patients | |
|---|---|---|---|---|
| Number | 5 | 6 | 13 | 26 |
| Age (mean ± SD) | 76 ± 3.6 years | 67 ± 6.2 years | 62 ± 8.9 years | 67 ± 9 years |
| Sex | ||||
| Female | 3 (60%) | 0 (0%) | 2 (15.4%) | 6 (23.08%) |
| Male | 2 (40%) | 6 (100%) | 11 (84.6%) | 20 (76.92%) |
| Differentiation degree | ||||
| Well differentiated (G1 and G1/G2) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Moderately differentiated (G2) | 1 (20%) | 1 (16.7%) | 2 (15.4%) | 4 (15.38%) |
| Poorly differentiated ( G3) | 2 (40%) | 4 (66.7%) | 10 (76.9%) | 18 (69.23%) |
| NA | 2 (40%) | 1 (16.7%) | 1 (7.7%) | 4 (15.38%) |
| TNM stage | ||||
| Stage I/II | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Stage III/IV | 5 (100%) | 6 (100%) | 13 (100%) | 26 (100%) |
| PATIENT No. | GENE | MUTATION | VAF % TUMOR | VAF% PLASMA |
|---|---|---|---|---|
| 1 | MET | T1010I | 58.89 | 49.53 |
| 2 | MET KRAS | c.3082 + 2T > C p.? G13D | - - | 0.81 0.51 |
| 3 | MET TP53 | exon 14 Skipping c.2942-11_2986del p.? R213 * V143M | - 23.31 1.40 - | - - 0.80 0.65 |
| 4 | SF3B1 TP53 | K700E G244D | - - | 0.25 0.52 |
| 5 | FBXW7 TP53 | R505S R248W | 33.1 73.01 | 3.46 5.07 |
| 6 | - | - | - | - |
| 7 | PIK3CA | E545K | 18.3 | 5.28 |
| 8 | TP53 | [E271D; V272L] V272L | 5.08 5.22 | 1.07 - |
| 9 | TP53 | R282G | 46.79 | 4.14 |
| 10 | FGFR3 PTEN TP53 | R248C D24Y C141W | 51.35 64.07 - | 22.61 20 16.24 |
| 11 | TP53 | C242Y | 36.3 | 1.74 |
| 12 | EGFR TP53 | L858R R248W V197M | 90.99 41.62 - | 23.62 2.33 0.26 |
| 13 | - | - | - | - |
| 14 | KRAS TP53 | G12C G245S R213P | 33.77 42.3 - | 1.89 0.88 1.26 |
| 15 | - | - | - | - |
| 16 | TP53 | S303Afs*42 | 32.71 | 2.02 |
| 17 | EGFR | L858R | 22.19 | 6.52 |
| 18 | EGFR | L858R | 84.25 | 3.61 |
| 19 | BRAF EGFR | V600E L858R | 3.06 - | 0.26 0.26 |
| 20 | KRAS | G12C | 33.46 | 0.16 |
| 21 | KRAS TP53 | G12V R213L | 18.36 11.61 | 3.40 2.23 |
| 22 | KRAS EGFR | G12D Q61H L858R | 12.81 - - | 0.12 0.57 0.37 |
| 23 | NRAS TP53 | Q61L G266 * R273H | 34.53 23.48 - | 4.72 2.89 0.82 |
| 24 | - | - | - | - |
| 25 | TP53 | S215I | 13.69 | 0.11 |
| 26 | MET | c.3082 + 1 G > C p.? | - | 11.68 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buburuzan, L.; Zamfir, M.-A.; Ardeleanu, C.M.; Muresan, A.H.; Vasilescu, F.; Hudita, A.; Costache, M.; Galateanu, B.; Puscasu, A.; Filippi, A.; et al. Dual NGS Comparative Analysis of Liquid Biopsy (LB) and Formalin-Fixed Paraffin-Embedded (FFPE) Samples of Non-Small Cell Lung Carcinoma (NSCLC). Cancers 2022, 14, 6084. https://doi.org/10.3390/cancers14246084
Buburuzan L, Zamfir M-A, Ardeleanu CM, Muresan AH, Vasilescu F, Hudita A, Costache M, Galateanu B, Puscasu A, Filippi A, et al. Dual NGS Comparative Analysis of Liquid Biopsy (LB) and Formalin-Fixed Paraffin-Embedded (FFPE) Samples of Non-Small Cell Lung Carcinoma (NSCLC). Cancers. 2022; 14(24):6084. https://doi.org/10.3390/cancers14246084
Chicago/Turabian StyleBuburuzan, Laura, Maria-Anca Zamfir (Irofei), Carmen Maria Ardeleanu, Alin Horatiu Muresan, Florina Vasilescu, Ariana Hudita, Marieta Costache, Bianca Galateanu, Alexandra Puscasu, Alexandru Filippi, and et al. 2022. "Dual NGS Comparative Analysis of Liquid Biopsy (LB) and Formalin-Fixed Paraffin-Embedded (FFPE) Samples of Non-Small Cell Lung Carcinoma (NSCLC)" Cancers 14, no. 24: 6084. https://doi.org/10.3390/cancers14246084
APA StyleBuburuzan, L., Zamfir, M. -A., Ardeleanu, C. M., Muresan, A. H., Vasilescu, F., Hudita, A., Costache, M., Galateanu, B., Puscasu, A., Filippi, A., & Motas, N. (2022). Dual NGS Comparative Analysis of Liquid Biopsy (LB) and Formalin-Fixed Paraffin-Embedded (FFPE) Samples of Non-Small Cell Lung Carcinoma (NSCLC). Cancers, 14(24), 6084. https://doi.org/10.3390/cancers14246084