
A Proposed Trial Design for the Treatment of Widely Metastatic Ewing Sarcoma Inspired by Evolutionary Dynamics

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
- -
- We are not “one drug away” from significantly improving outcomes for MES.
- -
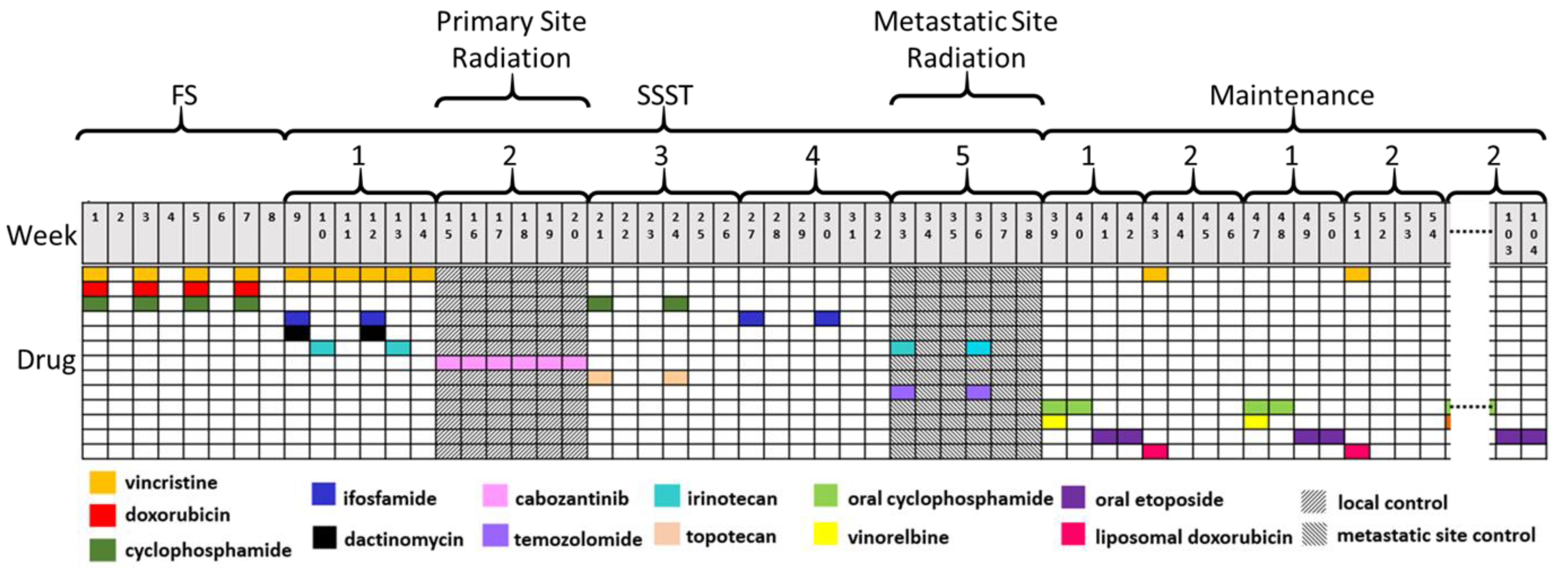
- After initial treatment (the “first-strike”; FS), therapy should be altered by changing agents and intensities at frequent intervals to affect small populations of resistant ES, here referred to as sequential second-strike therapies (SSST).
- -
- A prolonged and varied maintenance phase may be beneficial to drive the cancer cell population from a radiographic NED to below the MVP.
- -
- We should incorporate biological and radiomic correlates over time, including circulating tumor cells and DNA (CTC and ctDNA) prior to every change in systemic therapy.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cangir, A.; Vietti, T.J.; Gehan, E.A.; Burgert, E.O.; Thomas, P.; Tefft, M.; Nesbit, M.E.; Kissane, J.; Pritchard, D. Ewing’s sarcoma metastatic at diagnosis. Results and comparisons of two intergroup Ewing’s sarcoma studies. Cancer 1990, 66, 887–893. [Google Scholar] [CrossRef]
- Gatenby, R.A.; Brown, J.S. Integrating evolutionary dynamics into cancer therapy. Nat. Rev. Clin. Oncol. 2020, 17, 675–686. [Google Scholar] [CrossRef]
- Reed, D.R.; Metts, J.; Pressley, M.; Fridley, B.L.; Hayashi, M.; Isakoff, M.S.; Loeb, D.M.; Makanji, R.; Roberts, R.D.; Trucco, M.; et al. An evolutionary framework for treating pediatric sarcomas. Cancer 2020, 126, 2577–2587. [Google Scholar] [CrossRef]
- Ye, J.C.; Horne, S.; Zhang, J.Z.; Jackson, L.; Heng, H.H. Therapy Induced Genome Chaos: A Novel Mechanism of Rapid Cancer Drug Resistance. Front. Cell Dev. Biol. 2021, 9, 1–6. [Google Scholar] [CrossRef]
- Grier, H.E.; Krailo, M.D.; Tarbell, N.J.; Link, M.P.; Fryer, C.J.; Pritchard, D.J.; Gebhardt, M.C.; Dickman, P.S.; Perlman, E.J.; Meyers, P.A.; et al. Addition of ifosfamide and etoposide to standard chemotherapy for Ewing’s sarcoma and primitive neuroectodermal tumor of bone. N. Engl. J. Med. 2003, 348, 694–701. [Google Scholar] [CrossRef] [Green Version]
- Felgenhauer, J.L.; Nieder, M.L.; Krailo, M.D.; Bernstein, M.L.; Henry, D.W.; Malkin, D.; Baruchel, S.; Chuba, P.J.; Sailer, S.L.; Brown, K.; et al. A pilot study of low-dose anti-angiogenic chemotherapy in combination with standard multiagent chemotherapy for patients with newly diagnosed metastatic Ewing sarcoma family of tumors: A Children’s Oncology Group (COG) Phase II study NCT00061893. Pediatr. Blood Cancer 2013, 60, 409–414. [Google Scholar] [CrossRef] [Green Version]
- Dubois, S.; Glade-Bender, J.; Buxton, A.; Laack, N.; Randall, L.; Chen, H.; Seibel, N.; Terezakis, S.; Hill-Kayser, C.; Hayes-Jordan, A.; et al. Randomized Phase 3 Trial of Ganitumab Added to Intervel Compressed Chemotherapy for Patients with Newly Diagnosed Metastatic Ewing Sarcoma: A Report from Children’s Oncology Group (COG). In Proceedings of the CTOS 2019 Annual Meeting, Tokyo, Japan, 13–16 November 2019; Available online: https://www.ctos.org/Portals/0/PDF/2019%20CTOS%20Final%20Program.pdf (accessed on 5 January 2022).
- Ladenstein, R.; Potschger, U.; Le Deley, M.C.; Whelan, J.; Paulussen, M.; Oberlin, O.; van den Berg, H.; Dirksen, U.; Hjorth, L.; Michon, J.; et al. Primary disseminated multifocal Ewing sarcoma: Results of the Euro-EWING 99 trial. J. Clin. Oncol. 2010, 28, 3284–3291. [Google Scholar] [CrossRef]
- Dirksen, U.; Brennan, B.; Le Deley, M.C.; Cozic, N.; van den Berg, H.; Bhadri, V.; Brichard, B.; Claude, L.; Craft, A.; Amler, S.; et al. High-Dose Chemotherapy Compared With Standard Chemotherapy and Lung Radiation in Ewing Sarcoma With Pulmonary Metastases: Results of the European Ewing Tumour Working Initiative of National Groups, 99 Trial and EWING 2008. J. Clin. Oncol. 2019, 37, 3192. [Google Scholar] [CrossRef]
- Hunold, A.; Weddeling, N.; Paulussen, M.; Ranft, A.; Liebscher, C.; Jurgens, H. Topotecan and cyclophosphamide in patients with refractory or relapsed Ewing tumors. Pediatr. Blood Cancer 2006, 47, 795–800. [Google Scholar] [CrossRef]
- Leavey, P.J.; Laack, N.N.; Krailo, M.D.; Buxton, A.; Randall, R.L.; DuBois, S.G.; Reed, D.R.; Grier, H.E.; Hawkins, D.S.; Pawel, B.; et al. Phase III Trial Adding Vincristine-Topotecan-Cyclophosphamide to the Initial Treatment of Patients With Nonmetastatic Ewing Sarcoma: A Children’s Oncology Group Report. J. Clin. Oncol. 2021, 39, 4029–4038. [Google Scholar] [CrossRef]
- Amin, H.M.; Morani, A.C.; Daw, N.C.; Lamhamedi-Cherradi, S.E.; Subbiah, V.; Menegaz, B.A.; Vishwamitra, D.; Eskandari, G.; George, B.; Benjamin, R.S.; et al. IGF-1R/mTOR Targeted Therapy for Ewing Sarcoma: A Meta-Analysis of Five IGF-1R-Related Trials Matched to Proteomic and Radiologic Predictive Biomarkers. Cancers 2020, 12, 1768. [Google Scholar] [CrossRef]
- Hunger, S.P.; Mullighan, C.G. Acute Lymphoblastic Leukemia in Children. N. Engl. J. Med. 2015, 373, 1541–1552. [Google Scholar] [CrossRef] [Green Version]
- Palmerini, E.; Righi, A.; Staals, E.L. Rare Primary Malignant Bone Sarcomas. Cancers 2020, 12, 3092. [Google Scholar] [CrossRef]
- Bisogno, G.; Ferrari, A.; Tagarelli, A.; Sorbara, S.; Chiaravalli, S.; Poli, E.; Scarzello, G.; De Corti, F.; Casanova, M.; Affinita, M.C. Integrating irinotecan in standard chemotherapy: A novel dose-density combination for high-risk pediatric sarcomas. Pediatr. Blood Cancer 2021, 68, e28951. [Google Scholar] [CrossRef]
- Ferrari, A.; Bergamaschi, L.; Chiaravalli, S.; Pecori, E.; Diletto, B.; Alessandro, O.; Giandini, T.; Livellara, V.; Sironi, G.; Casanova, M. Multiagent chemotherapy including IrIVA regimen and maintenance therapy in the treatment of desmoplastic small round cell tumor. Tumori. J. 2021, 0300891621995250. [Google Scholar] [CrossRef]
- Gatenby, R.A.; Artzy-Randrup, Y.; Epstein, T.; Reed, D.R.; Brown, J.S. Eradicating Metastatic Cancer and the Eco-Evolutionary Dynamics of Anthropocene Extinctions. Cancer Res. 2020, 80, 613–623. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.A.; Ludmir, E.B.; Liao, K.P.; McAleer, M.F.; Grosshans, D.R.; McGovern, S.L.; Bishop, A.J.; Woodhouse, K.D.; Paulino, A.C.; Yeboa, D.N. Timing of Local Therapy Affects Survival in Ewing Sarcoma. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 127–136. [Google Scholar] [CrossRef]
- Italiano, A.; Mir, O.; Mathoulin-Pelissier, S.; Penel, N.; Piperno-Neumann, S.; Bompas, E.; Chevreau, C.; Duffaud, F.; Entz-Werle, N.; Saada, E.; et al. Cabozantinib in patients with advanced Ewing sarcoma or osteosarcoma (CABONE): A multicentre, single-arm, phase 2 trial. Lancet Oncol. 2020, 21, 446–455. [Google Scholar] [CrossRef]
- Schiff, D.; Desjardins, A.; Cloughesy, T.; Mikkelsen, T.; Glantz, M.; Chamberlain, M.C.; Reardon, D.A.; Wen, P.Y. Phase 1 dose escalation trial of the safety and pharmacokinetics of cabozantinib concurrent with temozolomide and radiotherapy or temozolomide after radiotherapy in newly diagnosed patients with high-grade gliomas. Cancer 2016, 122, 582–587. [Google Scholar] [CrossRef]
- Saylors, R.L.; Stine, K.C.; Sullivan, J.; Kepner, J.L.; Wall, D.A.; Bernstein, M.L.; Harris, M.B.; Hayashi, R.; Vietti, T.J. Pediatric Oncology Group Cyclophosphamide plus topotecan in children with recurrent or refractory solid tumors: A Pediatric Oncology Group phase II study. J. Clin. Oncol. 2001, 19, 3463–3469. [Google Scholar] [CrossRef]
- McCabe, M.; Kirton, L.; Khan, M.; Fenwick, N.; Dirksen, U.; Gaspar, N.; Kanerva, J.; Kuehne, T.; Longhi, A.; Luksch, R.; et al. Results of the Second Interim Assessment of rEECur, an International Randomized Controlled Trial of Chemotherapy for the Treatment of Recurrent and Primary Refractory Ewing Sarcoma (RR-ES). 2020. Available online: https://ascopubs.org/doi/10.1200/JCO.2020.38.15_suppl.11502 (accessed on 5 January 2022).
- Chen, A.Y.; Chen, P.M.; Chen, Y.J. DNA topoisomerase I drugs and radiotherapy for lung cancer. J. Thorac. Dis. 2012, 4, 390. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Takada, M.; Kawase, I.; Tada, T.; Kudoh, S.; Okishio, K.; Fukuoka, M.; Yamaoka, N.; Fujiwara, Y.; Yamakido, M. Enhancement of tumor radio-response by irinotecan in human lung tumor xenografts. Jpn. J. Cancer Res. 1997, 88, 218–223. [Google Scholar] [CrossRef]
- Chakravarti, A.; Erkkinen, M.G.; Nestler, U.; Stupp, R.; Mehta, M.; Aldape, K.; Gilbert, M.R.; Black, P.M.; Loeffler, J.S. Temozolomide-mediated radiation enhancement in glioblastoma: A report on underlying mechanisms. Clin. Cancer Res. 2006, 12, 4738–4746. [Google Scholar] [CrossRef] [Green Version]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Casey, D.A.; Wexler, L.H.; Merchant, M.S.; Chou, A.J.; Merola, P.R.; Price, A.P.; Meyers, P.A. Irinotecan and temozolomide for Ewing sarcoma: The Memorial Sloan-Kettering experience. Pediatr. Blood Cancer. 2009, 53, 1029–1034. [Google Scholar] [CrossRef]
- Green, D.M.; Nolan, V.G.; Goodman, P.J.; Whitton, J.A.; Srivastava, D.; Leisenring, W.M.; Neglia, J.P.; Sklar, C.A.; Kaste, S.C.; Hudson, M.M.; et al. The cyclophosphamide equivalent dose as an approach for quantifying alkylating agent exposure: A report from the Childhood Cancer Survivor Study. Pediatr. Blood Cancer 2014, 61, 53–67. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, M.; Chu, D.; Meyer, C.F.; Llosa, N.J.; McCarty, G.; Morris, C.D.; Levin, A.S.; Wolinsky, J.P.; Albert, C.M.; Steppan, D.A.; et al. Highly personalized detection of minimal Ewing sarcoma disease burden from plasma tumor DNA. Cancer 2016, 122, 3015–3023. [Google Scholar] [CrossRef]
- Hayashi, M.; Zhu, P.; McCarty, G.; Meyer, C.F.; Pratilas, C.A.; Levin, A.; Morris, C.D.; Albert, C.M.; Jackson, K.W.; Tang, C.M.; et al. Size-based detection of sarcoma circulating tumor cells and cell clusters. Oncotarget 2017, 8, 78965. [Google Scholar] [CrossRef] [Green Version]
- Klega, K.; Imamovic-Tuco, A.; Ha, G.; Clapp, A.N.; Meyer, S.; Ward, A.; Clinton, C.; Nag, A.; Van Allen, E.; Mullen, E.; et al. Detection of Somatic Structural Variants Enables Quantification and Characterization of Circulating Tumor DNA in Children With Solid Tumors. JCO Precis. Oncol. 2018, 2, 1–13. [Google Scholar] [CrossRef]
- Scarborough, J.A.; McClure, E.; Anderson, P.; Dhawan, A.; Durmaz, A.; Lessnick, S.L.; Hitomi, M.; Scott, J.G. Identifying States of Collateral Sensitivity during the Evolution of Therapeutic Resistance in Ewing’s Sarcoma. iScience 2020, 23, 101293. [Google Scholar] [CrossRef]


{kind=link}
| FS | SSST | Maintenance | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | ||
| Regimen and Doses | Vincristine 1.5 mg/m2 Day 1 Cyclophosphamide 1200 mg/m2 Day 1 Doxorubicin 75 mg/m2 Day 1 | Ifosfamide 3 g/m2 Days 1,2 Vincristine 1.5 mg/m2 Days 1,8,15 Actinomycin 1.5 mg/m2 Day 1 Irinotecan 20 mg/m2 Days 8–12 | Cabozantinib 40 mg/m2/day (60 mg/day patients 16 years and older) | Topotecan 0.75 mg/m2 Days 1–5 Cyclophosphamide 250 mg/m2 Days 1–5 | Ifosfamide 3 g/m2, Days 1–5 | Irinotecan 50 mg/m2 Days 1–5 Temozolomide 100 mg/m2 Days 1–5 | Oral Cyclophosphamide 25 mg/m2 Days 1–14 Vinorelbine 25 mg/m2 Days 1 Oral Etoposide 40 mg/m2 Days 15–28 | Vincristine 1.5 mg/m2 Day 1 Liposomal Doxorubicin 30 mg/m2 Day 1 |
| Length of Therapy | 14-day cycles, Four cycles total | 21-day cycles Two cycles, total | 42-day cycle, One cycle total | 21-day cycles, Two cycles total | 21-day cycles, Two cycles total | 21-day cycles, Two cycles total | 28-day cycles, Alternating with Maintenance 2 until 2 years | 28-day cycles, Alternating with Maintenance 1 until 2 years |
| Cyclophosphamide | Ifosfamide | Doxorubicin | Etoposide | |
|---|---|---|---|---|
| AEWS0031, regimen B (over 29 weeks) | 8.4 g/m2 | 63 g/m2 | 375 mg/m2 | 3500 mg/m2 |
| Total CED: 23.8 g/m2 | ||||
| SSST Protocol (over 104 weeks) | 10.5 g/m2 (7.3 g/m2 IV, 3.2 g/m2 oral) | 42 g/m2 | 540 mg/m2 (Includes 240 mg/m2 Liposomal) | 2240 mg/m2 equivalent (4480 mg/m2 oral, 2:1 IV to oral equivalency) |
| Total CED: 20.8 g/m2 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Metts, J.; Russell, T.; Reed, D.; Trucco, M. A Proposed Trial Design for the Treatment of Widely Metastatic Ewing Sarcoma Inspired by Evolutionary Dynamics. Cancers 2022, 14, 736. https://doi.org/10.3390/cancers14030736
Metts J, Russell T, Reed D, Trucco M. A Proposed Trial Design for the Treatment of Widely Metastatic Ewing Sarcoma Inspired by Evolutionary Dynamics. Cancers. 2022; 14(3):736. https://doi.org/10.3390/cancers14030736
Chicago/Turabian StyleMetts, Jonathan, Thomas Russell, Damon Reed, and Matteo Trucco. 2022. "A Proposed Trial Design for the Treatment of Widely Metastatic Ewing Sarcoma Inspired by Evolutionary Dynamics" Cancers 14, no. 3: 736. https://doi.org/10.3390/cancers14030736
APA StyleMetts, J., Russell, T., Reed, D., & Trucco, M. (2022). A Proposed Trial Design for the Treatment of Widely Metastatic Ewing Sarcoma Inspired by Evolutionary Dynamics. Cancers, 14(3), 736. https://doi.org/10.3390/cancers14030736