
Correlation between Tissue Cellularity and Metabolism Represented by Diffusion-Weighted Imaging (DWI) and 18F-FDG PET/MRI in Head and Neck Cancer (HNC)

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Demographics
2.2. PET/MRI Imaging
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PET/MRI | Positron Emission Tomography/Magnetic Resonance Imaging |
| SUV | Standardized Uptake Value |
| MTV | Metabolic Tumor Volume |
| TLG | Metabolic Tumor Volume |
| CRT | Chemo-Radiotherapy |
| HCC | Head and Neck Cancer |
| FDG | Fluorodeoxyglucose |
| AJCC | American Joint Committee on Cancer |
| (G) | Grade |
References
- Pace, L.S.M.; Nicolai, E.; Aiello, M.; Catalano, O.A. Whole-body PET/MRI in oncology: Current status and clinical applica-tions. Transl. Imaging 2013, 1, 31–44. [Google Scholar] [CrossRef]
- Queiroz, M.A.; Hüllner, M.; Kuhn, F.; Huber, G.; Meerwein, C.; Kollias, S.; Von Schulthess, G.; Veit-Haibach, P. Use of diffusion-weighted imaging (DWI) in PET/MRI for head and neck cancer evaluation. Eur. J. Pediatr. 2014, 41, 2212–2221. [Google Scholar] [CrossRef] [Green Version]
- Becker, M.; Zaidi, H. Imaging in head and neck squamous cell carcinoma: The potential role of PET/MRI. Br. J. Radiol. 2014, 87, 20130677. [Google Scholar] [CrossRef] [PubMed]
- Razek, A.A.K.A.; Kamal, E. Nasopharyngeal carcinoma: Correlation of apparent diffusion coeffecient value with prognostic parameters. Radiol. Med. 2013, 118, 534–539. [Google Scholar] [CrossRef]
- Surov, A.; Meyer, H.J.; Wienke, A. Correlation between apparent diffusion coefficient (ADC) and cellularity is different in several tumors: A meta-analysis. Oncotarget 2017, 8, 59492–59499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herneth, A.M.; Guccione, S.; Bednarski, M. Apparent Diffusion Coefficient: A quantitative parameter for in vivo tumor characterization. Eur. J. Radiol. 2003, 45, 208–213. [Google Scholar] [CrossRef]
- Jeh, S.K.; Kim, S.H.; Kim, H.S.; Kang, B.J.; Jeong, S.H.; Yim, H.W.; Song, B.J. Correlation of the apparent diffusion coefficient value and dynamic magnetic resonance imaging findings with prognostic factors in invasive ductal carcinoma. J. Magn. Reson. Imaging 2010, 33, 102–109. [Google Scholar] [CrossRef]
- Hayashida, Y.; Hirai, T.; Morishita, S.; Kitajima, M.; Murakami, R.; Korogi, Y.; Makino, K.; Nakamura, H.; Ikushima, I.; Yamura, M.; et al. Diffusion-weighted Imaging of Metastatic Brain Tumours: Comparison with Histologic Type and Tumour Cellularity. Am. J. Neuroradiol. 2006, 27, 1419–1425. Available online: http://www.ajnr.org/content/27/7/1419.abstract (accessed on 22 October 2021).
- Zhang, S.C.; Bao, Y.Y.; Zhou, S.H.; Shang, D.S. Application value of diffusion weighted magnetic resonance imag-ing in head and neck cancer. Int. J. Clin. Exp. Med. 2016, 9, 16747–16752. [Google Scholar]
- Srinivasan, A.; Dvorak, R.; Perni, K.; Rohrer, S.; Mukherji, S. Differentiation of Benign and Malignant Pathology in the Head and Neck Using 3T Apparent Diffusion Coefficient Values: Early Experience. Am. J. Neuroradiol. 2008, 29, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Freihat, O.; Tóth, Z.; Pintér, T.; Kedves, A.; Sipos, D.; Cselik, Z.; Lippai, N.; Repa, I.; Kovács, Á. Pre-treatment PET/MRI based FDG and DWI imaging parameters for predicting HPV status and tumor response to chemoradiotherapy in primary oropharyngeal squamous cell carcinoma (OPSCC). Oral Oncol. 2021, 116, 105239. [Google Scholar] [CrossRef] [PubMed]
- Kedves, A.; Tóth, Z.; Emri, M.; Fábián, K.; Sipos, D.; Freihat, O.; Tollár, J.; Cselik, Z.; Lakosi, F.; Bajzik, G.; et al. Predictive Value of Diffusion, Glucose Metabolism Parameters of PET/MR in Patients with Head and Neck Squamous Cell Carcinoma Treated with Chemoradiotherapy. Front. Oncol. 2020, 10, 1484. [Google Scholar] [CrossRef]
- Pak, K.; Cheon, G.J.; Nam, H.; Kim, S.; Kang, K.W.; Chung, J.; Kim, E.E.; Lee, D.S. Prognostic value of metabolic tumour volume and total lesion glycolysis in head and neck cancer: A systematic review and meta-analysis. J. Nucl. Med. 2014, 55, 884–890. Available online: http://www.academia.edu/download/46307953/Prognostic_Value_of_Metabolic_Tumour_Volu20160607-17979-obn7np.pdf (accessed on 23 September 2018). [CrossRef] [Green Version]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Vandecaveye, V.; De Keyzer, F.; Poorten, V.V.; Dirix, P.; Verbeken, E.; Nuyts, S.; Hermans, R. Head and Neck Squamous Cell Carcinoma: Value of Diffusion-weighted MR Imaging for Nodal Staging. Radiology 2009, 251, 134–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, S.; Wu, Z.; Wu, Y.; Zhang, W.; Li, J.; Dai, N.; Zhang, B.; Yan, J. Meta-analysis of the correlation between apparent diffusion coefficient and standardized uptake value in ma-lignant disease. Contrast Media Mol. Imaging 2017, 2017, 4729547. Available online: http://www.epistemonikos.org/documents/2ffc3010315c57bfa650e08188580270f3fc4105 (accessed on 16 January 2022). [CrossRef] [PubMed] [Green Version]
- Kim, Y.-I.; Paeng, J.C.; Cheon, G.J.; Suh, K.-S.; Lee, D.S.; Chung, J.-K.; Kang, K.W. Prediction of Posttransplantation Recurrence of Hepatocellular Carcinoma Using Metabolic and Volumetric Indices of 18F-FDG PET/CT. J. Nucl. Med. 2016, 57, 1045–1051. [Google Scholar] [CrossRef] [Green Version]
- Sridhar, P.; Mercier, G.; Tan, J.; Truong, M.T.; Daly, B.; Subramaniam, R.M. FDG PET metabolic tumour volume seg- mentation and pathologic volume of pri-mary human solid tumours. AJR Am. J. Roentgenol. 2014, 202, 1114–1119. [Google Scholar] [CrossRef]
- Bos, R.; Van Der Hoeven, J.J.; Van Der Wall, E.; Van Der Groep, P.; Van Diest, P.J.; Comans, E.F.; Joshi, U.; Semenza, G.L.; Hoekstra, O.S.; Lammertsma, A.A.; et al. Biologic Correlates of 18Fluorodeoxyglucose Uptake in Human Breast Cancer Measured by Positron Emission Tomography. J. Clin. Oncol. 2002, 20, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Kato, T.; Ohta, T.; Tadokoro, M.; Yamada, T.; Ikeda, M.; Nishino, M.; Ishigaki, T.; Ito, K.; Gambhir, S. Fluorine-18 fluoro-2-deoxyglucose positron emission tomography in recurrent rectal cancer: Relation to tumour size and cellularity. Eur. J. Pediatr. 1996, 23, 1372–1377. [Google Scholar] [CrossRef]
- Freihat, O.; Pinter, T.; Kedves, A.; Sipos, D.; Cselik, Z.; Repa, I.; Kovács, Á. Diffusion-Weighted Imaging (DWI) derived from PET/MRI for lymph node assessment in patients with Head and Neck Squamous Cell Carcinoma (HNSCC). Cancer Imaging 2020, 20, 56. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.H.; Cho, I.H.; Chun, K.A.; Kong, E.J.; Kwon, S.D.; Kim, J.H. Correlation Between Apparent Diffusion Coefficients and Standardized Uptake Values in Hybrid 18F-FDG PET/MR: Preliminary Results in Rectal Cancer. Nucl. Med. Mol. Imaging 2016, 50, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Min, M.; Lee, M.T.; Lin, P.; Holloway, L.; Wijesekera, D.; Gooneratne, D.; Rai, R.; Xuan, W.; Fowler, A.; Forstner, D.; et al. Assessment of serial multi-parametric functional MRI (diffusion-weighted imaging and R2*) with18F-FDG-PET in patients with head and neck cancer treated with radiation therapy. Br. J. Radiol. 2016, 89, 20150530. [Google Scholar] [CrossRef] [Green Version]
- Fruehwald-Pallamar, J.; Czerny, C.; Mayerhoefer, M.E.; Halpern, B.S.; Eder-Czembirek, C.; Brunner, M.; Schuetz, M.; Weber, M.; Fruehwald, L.; Herneth, A.M. Functional imaging in head and neck squamous cell carcinoma: Correlation of PET/CT and diffusion-weighted imaging at 3 Tesla. Eur. J. Pediatr. 2011, 38, 1009–1019. [Google Scholar] [CrossRef]
- Rasmussen, J.H.; Nørgaard, M.; Hansen, A.E.; Vogelius, I.R.; Aznar, M.C.; Johannesen, H.H.; Costa, J.; Engberg, A.M.; Kjaer, A.; Specht, L.; et al. Feasibility of Multiparametric Imaging with PET/MR in Head and Neck Squamous Cell Carcinoma. J. Nucl. Med. 2017, 58, 69–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varoquaux, A.; Rager, O.; Lovblad, K.-O.; Masterson, K.; Dulguerov, P.; Ratib, O.; Becker, C.D.; Becker, M. Functional imaging of head and neck squamous cell carcinoma with diffusion-weighted MRI and FDG PET/CT: Quantitative analysis of ADC and SUV. Eur. J. Pediatr. 2013, 40, 842–852. [Google Scholar] [CrossRef] [Green Version]
- Covello, M.; Cavaliere, C.; Aiello, M.; Cianelli, M.; Mesolella, M.; Iorio, B.; Rossi, A.; Nicolai, E. Simultaneous PET/MR head–neck cancer imaging: Preliminary clinical experience and multiparametric evaluation. Eur. J. Radiol. 2015, 84, 1269–1276. [Google Scholar] [CrossRef]
- Núñez, D.A.; Medina, A.L.; Iglesias, M.M.; Gomez, F.S.; Dave, A.; Hatzoglou, V.; Paudyal, R.; Calzado, A.; Deasy, J.O.; Shukla-Dave, A.; et al. Multimodality functional imaging using DW-MRI and 18F-FDG-PET/CT during radiation therapy for human papillomavirus negative head and neck squamous cell carcinoma: Meixoeiro Hospital of Vigo Experience. World J. Radiol. 2017, 9, 17–26. [Google Scholar] [CrossRef]
- Nakajo, M.; Nakajo, M.; Kajiya, Y.; Tani, A.; Kamiyama, T.; Yonekura, R.; Fukukura, Y.; Matsuzaki, T.; Nishimoto, K.; Nomoto, M.; et al. FDG PET/CT and diffusion-weighted imaging of head and neck squamous cell carcinoma: Comparison of prognostic significance between primary tumour standardized uptake value and apparent diffusion coefficient. Clin. Nucl. Med. 2012, 37, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Kim, S.Y.; Lee, S.J.; Choi, J.W. The Correlations Between MRI Perfusion, Diffusion Parameters, and 18F-FDG PET Metabolic Parameters in Primary Head-and-Neck Cancer. Medicine 2015, 94, e2141. [Google Scholar] [CrossRef]
- Lambregts, D.M.J.; Beets, G.L.; Maas, M.; Curvo-Semedo, L.; Kessels, A.G.H.; Thywissen, T.; Beets-Tan, R.G.H. Tumour ADC measurements in rectal cancer: Effect of ROI methods on ADC values and interobserver variability. Eur. Radiol. 2011, 21, 2567–2574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miccò, M.; Vargas, H.A.; Burger, I.A.; Kollmeier, M.A.; Goldman, D.A.; Park, K.; Abu-Rustum, N.R.; Hricak, H.; Sala, E. Combined pre-treatment MRI and 18F-FDG PET/CT parameters as prognostic biomarkers in patients with cervical cancer. Eur. J. Radiol. 2014, 83, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Morand, G.B.; Vital, D.G.; Kudura, K.; Werner, J.; Stoeckli, S.J.; Huber, G.F.; Huellner, M.W. Maximum Standardized Uptake Value (SUVmax) of Primary Tumor Predicts Occult Neck Metastasis in Oral Cancer. Sci. Rep. 2018, 8, 11817. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.K.; Mak, H.K.; Huang, B.; Yeung, D.W.; Kwong, D.L.-W.; Khong, P.-L. Nasopharyngeal carcinoma: Relationship between 18F-FDG PET-CT maximum standardized uptake value, metabolic tumour volume and total lesion glycolysis and TNM classification. Nucl. Med. Commun. 2010, 31, 206–210. [Google Scholar] [CrossRef]
- Karan, B.; Pourbagher, A.; Torun, N. Diffusion-weighted imaging and18F-fluorodeoxyglucose positron emission tomography/computed tomography in breast cancer: Correlation of the apparent diffusion coefficient and maximum standardized uptake values with prognostic factors. J. Magn. Reson. Imaging 2015, 43, 1434–1444. [Google Scholar] [CrossRef]
- Choi, B.B.; Kim, S.H.; Kang, B.J.; Lee, J.H.; Song, B.J.; Jeong, S.H.; Yim, H.W. Diffusion-weighted imaging and FDG PET/CT: Predicting the prognoses with apparent diffusion coefficient values and maximum standardized uptake values in patients with invasive ductal carcinoma. World J. Surg. Oncol. 2012, 10, 126. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Wu, J.R.; Wei, L.L.; Liao, G.X.; Yang, C.J.; Jin, G.Q.; Xiao, G.Y.; Su, D.K. High standardized uptake values of 18F-FDG PET/CT imaging but not MRI correlates to pathology find-ings in patients with cervical cancer. Hell. J. Nucl. Med. 2019, 22, 96–102. [Google Scholar] [CrossRef]
- Gong, J.; Wang, N.; Bian, L.; Wang, M.; Ye, M.; Wen, N.; Fu, M.; Fan, W.; Meng, Y. Cervical cancer evaluated with integrated 18F-FDG PET/MR. Oncol. Lett. 2019, 18, 1815–1823. [Google Scholar] [CrossRef]
- Yu, Y.Y.; Zhang, R.; Dong, R.T.; Hu, Q.Y.; Yu, T.; Liu, F.; Luo, Y.H.; Dong, Y. Feasibility of an ADC-based radiomics model for predicting pelvic lymph node metastases in patients with stage IB–IIA cervical squamous cell carcinoma. Br. J. Radiol. 2019, 92, 20180986. [Google Scholar] [CrossRef]
- Nerad, E.; Pizzi, A.D.; Lambregts, D.M.J.; Maas, M.; Wadhwani, S.; Bakers, F.C.H.; Bosch, H.C.M.V.D.; Beets-Tan, R.G.H.; Lahaye, M.J. The Apparent Diffusion Coefficient (ADC) is a useful biomarker in predicting metastatic colon cancer using the ADC-value of the primary tumor. PLoS ONE 2019, 14, e0211830. [Google Scholar] [CrossRef]
- Xu, C.; Li, H.; Seng, D.; Liu, F. Significance of SUV Max for Predicting Occult Lymph Node Metastasis and Prognosis in Early-Stage Tongue Squamous Cell Carcinoma. J. Oncol. 2020, 2020, 6241637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, F.; Kudo, K.; Yamashita, H.; Baba, M.; Shimizu, A.; Oyama-Manabe, N.; Kinoshita, R.; Li, R.; Shirato, H. Predicting metastasis in clinically negative axillary lymph nodes with minimum apparent diffusion coefficient value in luminal A-like breast cancer. Breast Cancer 2019, 26, 628–636. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 71 |
|---|---|
| Mean Age (y) | (61.6 ± 0.8) |
| Men | 49 (69.0%) |
| Women | 22 (31.0%) |
| Histologic Grade | |
| Grade 1 | 12 (16.9%) |
| Grade 2 | 41 (57.7%) |
| Grade 3 | 18 (20.4%) |
| Localization | |
| Pharyngeal | 32 (45.1%) |
| Laryngeal | 15 (21.1%) |
| Oral | 22 (33.8%) |
| T category | |
| T1 | 4 (5.6%) |
| T2 | 19 (26.8%) |
| T3 | 26 (36.6%) |
| T4 | 22 (31.0%) |
| N category | |
| N0 | 10 (14.1%) |
| N1 | 9 (12.7%) |
| N2 | 45(63.4%) |
| N3 | 7 (9.9%) |
| M Category | |
| M0 | 63 (88.7%) |
| M1 | 8 (11.3%) |
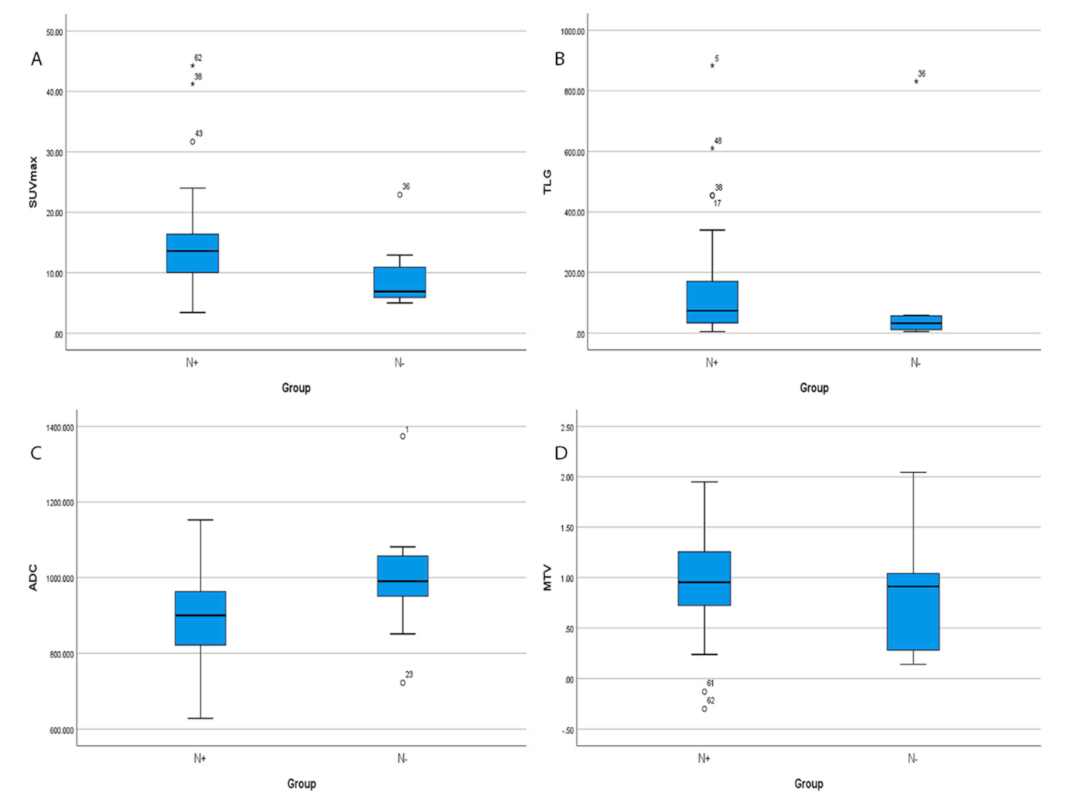
| N groups | |
| N+ | 61 (85.9%) |
| N− | 10 (14.1%) |
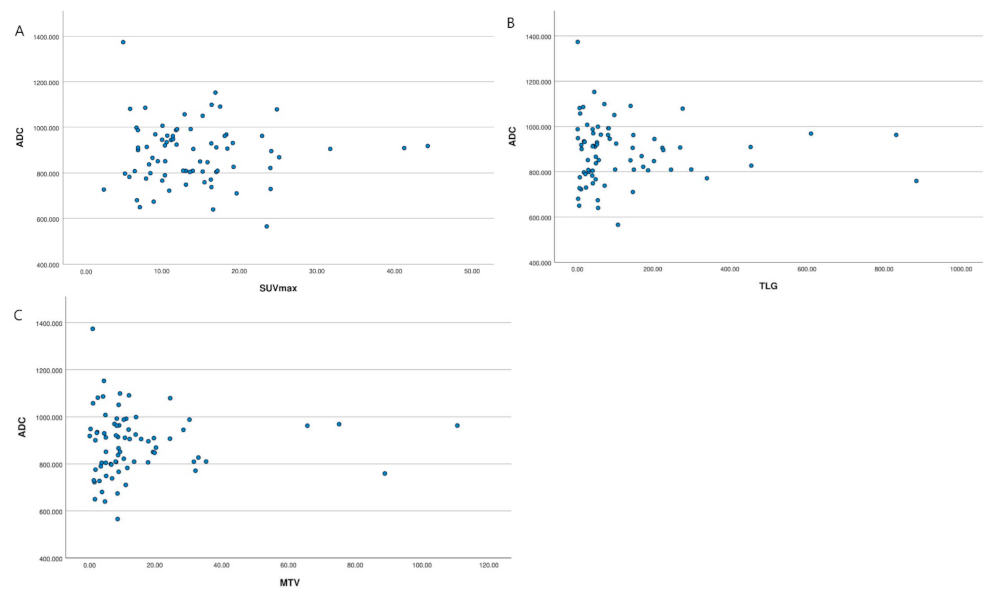
| Parameter | ADC | SUVmax | TLG | MTV | Tumor Size | |
|---|---|---|---|---|---|---|
| ADC | Spearman (rho) | −0.184 | −0.182 | −0.037 | −0.088 | |
| Sig. (2-tailed) | −0.125 | 0.129 | 0.756 | 0.464 | ||
| SUVmax | Spearman (rho) | 0.456 * | ||||
| Sig. (2-tailed) | 0.000 | |||||
| TLG | Spearman (rho) | 0.794 * | ||||
| Sig. (2-tailed) | 0.000 | |||||
| MTV | Spearman (rho) | 0.739 * | ||||
| Sig. (2-tailed) | 0.000 | |||||
| Grouping | SUVmax | TLG | MTV | ADC |
|---|---|---|---|---|
| SEX | p = 0.314 | p = 0.522 | p = 0.784 | p = 0.897 |
| T stages | p = 0.267 | p =0.006 | p= 0.001 | p = 0.880 |
| N stages | p =0.023 | p =0.033 | p = 0.605 | p = 0.092 |
| M stages | p = 0.283 | p = 0.785 | p = 0.913 | p = 0.347 |
| Grades | p = 0.233 | p = 0.310 | p = 0.713 | p =0.050 |
| Localization | p = 0.389 | p = 0.128 | p = 0.367 | p = 0.270 |
| Prognostic Factors | B | T | p Value |
|---|---|---|---|
| SUVmax | |||
| Tumor size | 0.409 | 3.333 | 0.001 * |
| T stages | N/A | N/A | N/A |
| N stages | 0.227 | 1.995 | 0.022 * |
| TLG | |||
| Tumor size | 0.767 | 8.988 | 0.000 * |
| T stages | −0.050 | −0.598 | 0.552 |
| N stages | 0.119 | 1.500 | 0.138 |
| MTV | |||
| Tumor size | 0.662 | 6.857 | 0.000 * |
| T stages | 0.140 | 1.473 | 0.146 |
| N stages | N/A | N/A | N/A |
| ADC | |||
| N stages | 0.043 | 2.042 | 0.069 |
| Tumor grades | −0.021 | −1.846 | 0.045 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freihat, O.; Zoltán, T.; Pinter, T.; Kedves, A.; Sipos, D.; Repa, I.; Kovács, Á.; Zsolt, C. Correlation between Tissue Cellularity and Metabolism Represented by Diffusion-Weighted Imaging (DWI) and 18F-FDG PET/MRI in Head and Neck Cancer (HNC). Cancers 2022, 14, 847. https://doi.org/10.3390/cancers14030847
Freihat O, Zoltán T, Pinter T, Kedves A, Sipos D, Repa I, Kovács Á, Zsolt C. Correlation between Tissue Cellularity and Metabolism Represented by Diffusion-Weighted Imaging (DWI) and 18F-FDG PET/MRI in Head and Neck Cancer (HNC). Cancers. 2022; 14(3):847. https://doi.org/10.3390/cancers14030847
Chicago/Turabian StyleFreihat, Omar, Tóth Zoltán, Tamas Pinter, András Kedves, Dávid Sipos, Imre Repa, Árpád Kovács, and Cselik Zsolt. 2022. "Correlation between Tissue Cellularity and Metabolism Represented by Diffusion-Weighted Imaging (DWI) and 18F-FDG PET/MRI in Head and Neck Cancer (HNC)" Cancers 14, no. 3: 847. https://doi.org/10.3390/cancers14030847
APA StyleFreihat, O., Zoltán, T., Pinter, T., Kedves, A., Sipos, D., Repa, I., Kovács, Á., & Zsolt, C. (2022). Correlation between Tissue Cellularity and Metabolism Represented by Diffusion-Weighted Imaging (DWI) and 18F-FDG PET/MRI in Head and Neck Cancer (HNC). Cancers, 14(3), 847. https://doi.org/10.3390/cancers14030847