
The Feasibility of Implementing Mainstream Germline Genetic Testing in Routine Cancer Care—A Systematic Review

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Databases
2.3. Data Collection
2.4. Outcomes
2.5. Critical Appraisal
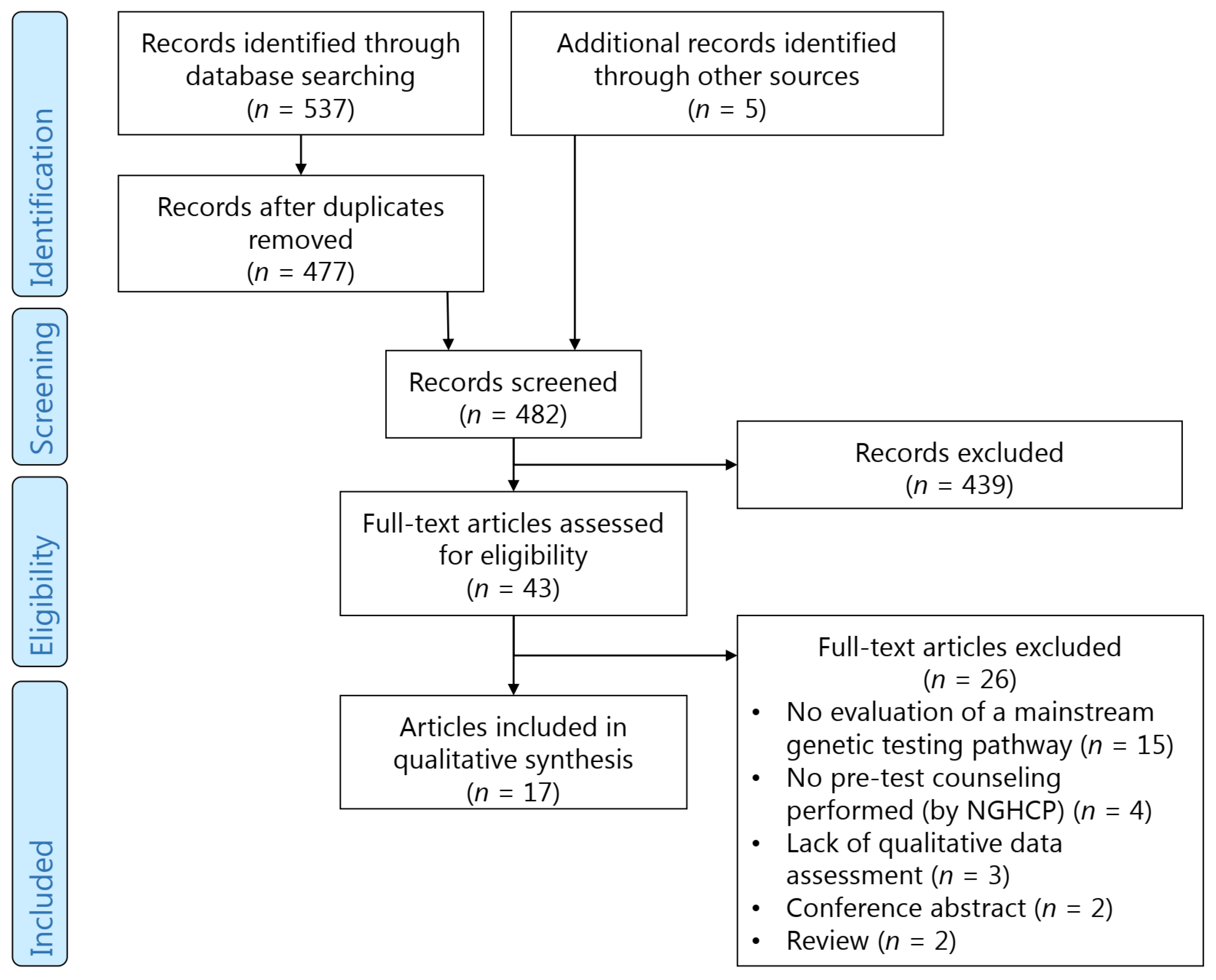
3. Results
3.1. Characteristics
3.2. Feasibility
3.2.1. Time Investment for NGHCPs
3.2.2. Barriers and Facilitators for NGHCPs
3.3. Quality of Care
3.3.1. Training of NGHCPs
3.3.2. Informed Consent
3.3.3. Genetic Counseling for Pathogenic Variants
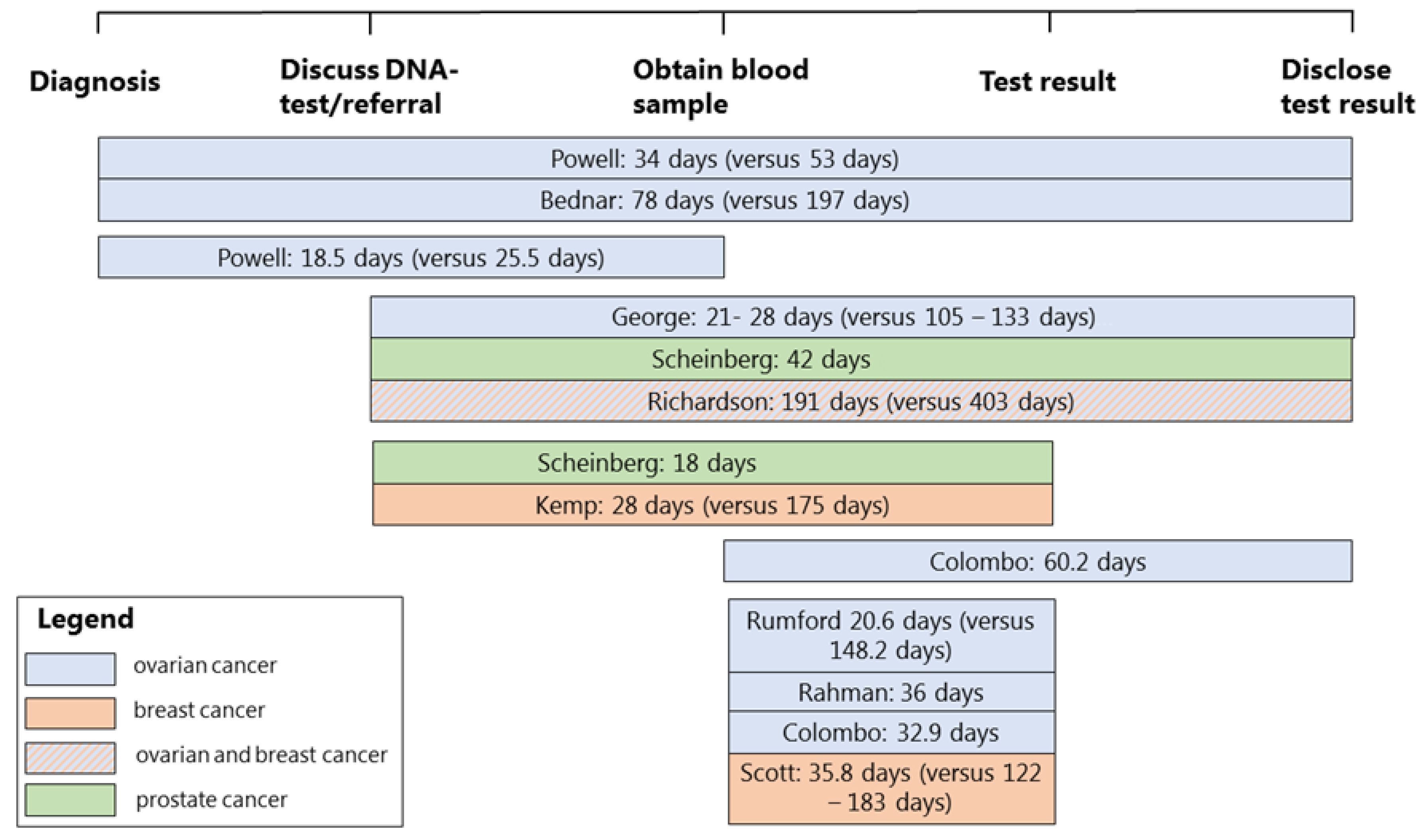
3.3.4. Turnaround Times
3.3.5. Adherence to Guidelines
3.3.6. Critical Appraisal
4. Discussion
4.1. Feasibility
4.1.1. Duration and Key Elements of Pre-Test Counseling
4.1.2. Barriers and Facilitators for Implementation of Mainstream Genetic Testing
4.2. Quality of Care
4.2.1. Training
4.2.2. Post-Test Counseling
4.2.3. Turnaround Time
4.2.4. Adherence to Guidelines
4.3. Limitations
4.4. Suggestions for the Implementation of Mainstream Genetic Testing
4.5. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Daly, M.B.; Pal, T.; Berry, M.P.; Buys, S.S.; Dickson, P.; Domchek, S.M.; Elkhanany, A.; Friedman, S.; Goggins, M.; Hutton, M.L.; et al. NCCN Clinical Practice Guideline in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 77–102. [Google Scholar] [CrossRef]
- Swisher, E.M. Usefulness of Multigene Testing: Catching the Train That’s Left the Station. JAMA Oncol. 2015, 1, 951–952. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Hu, C.; Hart, S.N.; Boddicker, N.; Polley, E.C.; Na, J.; Gnanaolivu, R.; Lee, K.Y.; Lindstrom, T.; Armasu, S.; et al. Evaluation of Germline Genetic Testing Criteria in a Hospital-Based Series of Women With Breast Cancer. J. Clin. Oncol. 2020, 38, 1409–1418. [Google Scholar] [CrossRef] [PubMed]
- De Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef] [PubMed]
- Tew, W.P.; Lacchetti, C.; Ellis, A.; Maxian, K.; Banerjee, S.; Bookman, M.; Jones, M.B.; Lee, J.M.; Lheureux, S.; Liu, J.F.; et al. PARP Inhibitors in the Management of Ovarian Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 38, 3468–3493. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.N.J.; Garber, J.E.; Kaufman, B.; Viale, G.; Fumagalli, D.; Rastogi, P.; Gelber, R.D.; de Azambuja, E.; Fielding, A.; Balmana, J.; et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N. Engl. J. Med. 2021, 384, 2394–2405. [Google Scholar] [CrossRef]
- George, A.; Riddell, D.; Seal, S.; Talukdar, S.; Mahamdallie, S.; Ruark, E.; Cloke, V.; Slade, I.; Kemp, Z.; Gore, M.; et al. Implementing rapid, robust, cost-effective, patient-centred, routine genetic testing in ovarian cancer patients. Sci. Rep. 2016, 6, 29506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemp, Z.; Turnbull, A.; Yost, S.; Seal, S.; Mahamdallie, S.; Poyastro-Pearson, E.; Warren-Perry, M.; Eccleston, A.; Tan, M.M.; Teo, S.H.; et al. Evaluation of Cancer-Based Criteria for Use in Mainstream BRCA1 and BRCA2 Genetic Testing in Patients With Breast Cancer. JAMA Netw. Open 2019, 2, e194428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, N.A.; Donnelly, L.; Stocking, K.; Evans, D.G.; Crosbie, E.J. Feasibility of Gynaecologist Led Lynch Syndrome Testing in Women with Endometrial Cancer. J. Clin. Med. 2020, 9, 1842. [Google Scholar] [CrossRef] [PubMed]
- Ryan, N.A.J.; McMahon, R.; Tobi, S.; Snowsill, T.; Esquibel, S.; Wallace, A.J.; Bunstone, S.; Bowers, N.; Mosneag, I.E.; Kitson, S.J.; et al. The proportion of endometrial tumours associated with Lynch syndrome (PETALS): A prospective cross-sectional study. PLoS Med. 2020, 17, e1003263. [Google Scholar] [CrossRef]
- Scheinberg, T.; Goodwin, A.; Ip, E.; Linton, A.; Mak, B.; Smith, D.P.; Stockler, M.R.; Strach, M.C.; Tran, B.; Young, A.L.; et al. Evaluation of a Mainstream Model of Genetic Testing for Men With Prostate Cancer. JCO Oncol. Pract. 2021, 17, e204–e216. [Google Scholar] [CrossRef] [PubMed]
- Scheinberg, T.; Young, A.; Woo, H.; Goodwin, A.; Mahon, K.L.; Horvath, L.G. Mainstream consent programs for genetic counseling in cancer patients: A systematic review. Asia Pac. J. Clin. Oncol. 2020, 17, 163–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hempel, S.; Shekelle, P.G.; Liu, J.L.; Sherwood Danz, M.; Foy, R.; Lim, Y.W.; Motala, A.; Rubenstein, L.V. Development of the Quality Improvement Minimum Quality Criteria Set (QI-MQCS): A tool for critical appraisal of quality improvement intervention publications. BMJ Qual. Saf. 2015, 24, 796–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grindedal, E.M.; Jorgensen, K.; Olsson, P.; Gravdehaug, B.; Luras, H.; Schlichting, E.; Vamre, T.; Wangensteen, T.; Heramb, C.; Maehle, L. Mainstreamed genetic testing of breast cancer patients in two hospitals in South Eastern Norway. Fam. Cancer 2020, 19, 133–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, N.; Huang, G.; Scambia, G.; Chalas, E.; Pignata, S.; Fiorica, J.; Van Le, L.; Ghamande, S.; Gonzalez-Santiago, S.; Bover, I.; et al. Evaluation of a Streamlined Oncologist-Led BRCA Mutation Testing and Counseling Model for Patients With Ovarian Cancer. J. Clin. Oncol. 2018, 36, 1300–1307. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; Kentwell, M.; Meiser, B.; Do, J.; Nevin, S.; Taylor, N.; Barlow-Stewart, K.; Kirk, J.; James, P.; Scott, C.L.; et al. The development and evaluation of a nationwide training program for oncology health professionals in the provision of genetic testing for ovarian cancer patients. Gynecol. Oncol. 2020, 158, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Percival, N.; George, A.; Gyertson, J.; Hamill, M.; Fernandes, A.; Davies, E.; Rahman, N.; Banerjee, S. The integration of BRCA testing into oncology clinics. Br. J. Nurs. 2016, 25, 690–694. [Google Scholar] [CrossRef] [PubMed]
- Powell, C.B.; Laurent, C.; Ciaravino, G.; Garcia, C.; Han, L.; Hoodfar, E.; Karlea, A.; Kobelka, C.; Lee, J.; Littell, R.D.; et al. Streamlining genetic testing for women with ovarian cancer in a Northern California health care system. Gynecol. Oncol. 2020, 159, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Rahman, B.; Lanceley, A.; Kristeleit, R.S.; Ledermann, J.A.; Lockley, M.; McCormack, M.; Mould, T.; Side, L. Mainstreamed genetic testing for women with ovarian cancer: First-year experience. J. Med. Genet. 2019, 56, 195–198. [Google Scholar] [CrossRef]
- Bednar, E.M.; Oakley, H.D.; Sun, C.C.; Burke, C.C.; Munsell, M.F.; Westin, S.N.; Lu, K.H. A universal genetic testing initiative for patients with high-grade, non-mucinous epithelial ovarian cancer and the implications for cancer treatment. Gynecol. Oncol. 2017, 146, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Flaum, N.; Morgan, R.D.; Burghel, G.J.; Bulman, M.; Clamp, A.R.; Hasan, J.; Mitchell, C.L.; Badea, D.; Moon, S.; Hogg, M.; et al. Mainstreaming germline BRCA1/2 testing in non-mucinous epithelial ovarian cancer in the North West of England. Eur. J. Hum. Genet. 2020, 28, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- McLeavy, L.; Rahman, B.; Kristeleit, R.; Ledermann, J.; Lockley, M.; McCormack, M.; Mould, T.; Side, L.; Lanceley, A. Mainstreamed genetic testing in ovarian cancer: Patient experience of the testing process. Int. J. Gynecol. Cancer 2020, 30, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M.; Min, H.J.; Hong, Q.; Compton, K.; Mung, S.W.; Lohn, Z.; Nuk, J.; McCullum, M.; Portigal-Todd, C.; Karsan, A.; et al. Oncology Clinic-Based Hereditary Cancer Genetic Testing in a Population-Based Health Care System. Cancers 2020, 12, 338. [Google Scholar] [CrossRef]
- Rumford, M.; Lythgoe, M.; McNeish, I.; Gabra, H.; Tookman, L.; Rahman, N.; George, A.; Krell, J. Oncologist-led BRCA ‘mainstreaming’ in the ovarian cancer clinic: A study of 255 patients and its impact on their management. Sci. Rep. 2020, 10, 3390. [Google Scholar] [CrossRef] [Green Version]
- Scott, N.; O’Sullivan, J.; Asgeirsson, K.; Macmillan, D.; Wilson, E. Changing practice: Moving to a specialist nurse-led service for BRCA gene testing. Br. J. Nurs. 2020, 29, S6–S13. [Google Scholar] [CrossRef] [PubMed]
- Taylor, N.; Parveen, S.; Robins, V.; Slater, B.; Lawton, R. Development and initial validation of the Influences on Patient Safety Behaviours Questionnaire. Implement Sci. 2013, 8, 81. [Google Scholar] [CrossRef] [Green Version]
- Albada, A.; Ausems, M.G.; van Dulmen, S. Counselee participation in follow-up breast cancer genetic counselling visits and associations with achievement of the preferred role, cognitive outcomes, risk perception alignment and perceived personal control. Soc. Sci. Med. 2014, 116, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Eijzenga, W.; Aaronson, N.K.; Hahn, D.E.; Sidharta, G.N.; van der Kolk, L.E.; Velthuizen, M.E.; Ausems, M.G.; Bleiker, E.M. Effect of routine assessment of specific psychosocial problems on personalized communication, counselors’ awareness, and distress levels in cancer genetic counseling practice: A randomized controlled trial. J. Clin. Oncol. 2014, 32, 2998–3004. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.E.; Bradbury, A.R.; Arun, B.; Domchek, S.M.; Ford, J.M.; Hampel, H.L.; Lipkin, S.M.; Syngal, S.; Wollins, D.S.; Lindor, N.M. American Society of Clinical Oncology Policy Statement Update: Genetic and Genomic Testing for Cancer Susceptibility. J. Clin. Oncol. 2015, 33, 3660–3667. [Google Scholar] [CrossRef] [Green Version]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [Green Version]
- Page, E.C.; Bancroft, E.K.; Brook, M.N.; Assel, M.; Hassan Al Battat, M.; Thomas, S.; Taylor, N.; Chamberlain, A.; Pope, J.; Raghallaigh, H.N.; et al. Interim Results from the IMPACT Study: Evidence for Prostate-specific Antigen Screening in BRCA2 Mutation Carriers. Eur. Urol. 2019, 76, 831–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph-Williams, N.; Elwyn, G.; Edwards, A. Knowledge is not power for patients: A systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ. Couns. 2014, 94, 291–309. [Google Scholar] [CrossRef]
- Legare, F.; Ratte, S.; Gravel, K.; Graham, I.D. Barriers and facilitators to implementing shared decision-making in clinical practice: Update of a systematic review of health professionals’ perceptions. Patient Educ. Couns. 2008, 73, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Pieterse, A.H.; Stiggelbout, A.M.; Montori, V.M. Shared Decision Making and the Importance of Time. JAMA 2019, 322, 25–26. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, A.R.; Patrick-Miller, L.J.; Egleston, B.L.; DiGiovanni, L.; Brower, J.; Harris, D.; Stevens, E.M.; Maxwell, K.N.; Kulkarni, A.; Chavez, T.; et al. Patient feedback and early outcome data with a novel tiered-binned model for multiplex breast cancer susceptibility testing. Genet. Med. 2016, 18, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Underhill-Blazey, M.; Blonquist, T.; Chittenden, A.; Pozzar, R.; Nayak, M.; Lansang, K.; Hong, F.; Garber, J.; Stopfer, J.E. Informing models of cancer genetics care in the era of multigene panel testing with patient-led recommendations. J. Genet. Couns. 2021, 30, 268–282. [Google Scholar] [CrossRef]
- Yoon, S.Y.; Wong, S.W.; Lim, J.; Ahmad, S.; Mariapun, S.; Padmanabhan, H.; Hassan, N.T.; Lau, S.Y.; Ch’ng, G.S.; Haniffa, M.; et al. Oncologist-led BRCA counselling improves access to cancer genetic testing in middle-income Asian country, with no significant impact on psychosocial outcomes. J. Med. Genet. 2021, 59. [Google Scholar] [CrossRef]
- Medendorp, N.M.; van den Heuvel, L.M.; Han, P.K.J.; Hillen, M.A.; Smets, E.M.A. Communication skills training for healthcare professionals in providing genetic counseling: A scoping literature review. Patient Educ. Couns. 2021, 104, 20–32. [Google Scholar] [CrossRef]
- Starkings, R.; Shilling, V.; Jenkins, V.; Fallowfield, L. A systematic review of communication interventions to help healthcare professionals discuss genetic testing for breast cancer. Breast Cancer Res. Treat. 2020, 183, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Menko, F.H.; Ter Stege, J.A.; van der Kolk, L.E.; Jeanson, K.N.; Schats, W.; Moha, D.A.; Bleiker, E.M.A. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: A systematic review of the literature and implications for clinical practice. Fam. Cancer 2019, 18, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Clift, K.; Macklin, S.; Halverson, C.; McCormick, J.B.; Abu Dabrh, A.M.; Hines, S. Patients’ views on variants of uncertain significance across indications. J. Community Genet. 2020, 11, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Kurian, A.W.; Li, Y.; Hamilton, A.S.; Ward, K.C.; Hawley, S.T.; Morrow, M.; McLeod, M.C.; Jagsi, R.; Katz, S.J. Gaps in Incorporating Germline Genetic Testing Into Treatment Decision-Making for Early-Stage Breast Cancer. J. Clin. Oncol. 2017, 35, 2232–2239. [Google Scholar] [CrossRef]
- Macklin, S.K.; Jackson, J.L.; Atwal, P.S.; Hines, S.L. Physician interpretation of variants of uncertain significance. Fam. Cancer 2019, 18, 121–126. [Google Scholar] [CrossRef]
- Ghose, A.; Moschetta, M.; Pappas-Gogos, G.; Sheriff, M.; Boussios, S. Genetic Aberrations of DNA Repair Pathways in Prostate Cancer: Translation to the Clinic. Int. J. Mol. Sci. 2021, 22, 9783. [Google Scholar] [CrossRef]
- Hoskovec, J.M.; Bennett, R.L.; Carey, M.E.; DaVanzo, J.E.; Dougherty, M.; Hahn, S.E.; LeRoy, B.S.; O’Neal, S.; Richardson, J.G.; Wicklund, C.A. Projecting the Supply and Demand for Certified Genetic Counselors: A Workforce Study. J. Genet. Couns. 2018, 27, 16–20. [Google Scholar] [CrossRef]
- Cohen, S.A.; Nixon, D.M. A collaborative approach to cancer risk assessment services using genetic counselor extenders in a multi-system community hospital. Breast Cancer Res. Treat. 2016, 159, 527–534. [Google Scholar] [CrossRef]
- Stoll, K.; Kubendran, S.; Cohen, S.A. The past, present and future of service delivery in genetic counseling: Keeping up in the era of precision medicine. Am. J. Med. Genet. C Semin. Med. Genet. 2018, 178, 24–37. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Norquist, B.; Lacchetti, C.; Armstrong, D.; Grisham, R.N.; Goodfellow, P.J.; Kohn, E.C.; Levine, D.A.; Liu, J.F.; Lu, K.H.; et al. Germline and Somatic Tumor Testing in Epithelial Ovarian Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 38, 1222–1245. [Google Scholar] [CrossRef]
- Sie, A.S.; van Zelst-Stams, W.A.; Spruijt, L.; Mensenkamp, A.R.; Ligtenberg, M.J.; Brunner, H.G.; Prins, J.B.; Hoogerbrugge, N. More breast cancer patients prefer BRCA-mutation testing without prior face-to-face genetic counseling. Fam. Cancer 2014, 13, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Hogarth, S.; Javitt, G.; Melzer, D. The current landscape for direct-to-consumer genetic testing: Legal, ethical, and policy issues. Annu. Rev. Genomics Hum. Genet. 2008, 9, 161–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frugtniet, B.; Morgan, S.; Murray, A.; Palmer-Smith, S.; White, R.; Jones, R.; Hanna, L.; Fuller, C.; Hudson, E.; Mullard, A.; et al. The detection of germline and somatic BRCA1/2 genetic variants through parallel testing of patients with high-grade serous ovarian cancer: A national retrospective audit. BJOG 2022, 129, 433–442. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| References | |
|---|---|
| Extra time to discuss genetic test | |
| No significant added time | [19] |
| 6–10 min (21/64 NGHCPs) and 11–20 min (17/64 NGHCPs) | [18] |
| 8 min | [9,20] |
| 10 min | [11] |
| 20 min | [17] |
| Extra time to disclose genetic test result | |
| 6–10 min (21/54 NGHCPs) and 4–5 min (8/54 NGHCPs) | [18] |
| 9 min | [11] |
| NGHCPs (strongly) agreed that discussing genetic testing was possible within the timeframe of a consultation | [7,8,11,17,20] |
| Workload increased slightly (24/46 NGHCPs) or did not increase (19/46 NGHCPs) | [18] |
| References | |
|---|---|
| Barriers | |
| Concerns about added time pressure | [11,19] |
| Inadequate knowledge about genetics | [11] |
| Lack of knowledge of VUSs | [11,21] |
| Lack of local infrastructure | [18] |
| Lack of human resources | [18] |
| Lack of funding/unwillingness to allocate funds | [18] |
| Facilitators | |
| Supporting materials (training and Frequently Asked Questions) | [7,8,17,20] |
| Approved clinical protocol | [7,8,17,20] |
| Information sheets to provide to patients | [7,8,17] |
| Assistance of a nurse consultant | [11] |
| Required written test packages | [11] |
| Education program | [11] |
| References | |
|---|---|
| Topics for pre-test genetic counseling | |
| • Discussing the genes that are tested and their role in the development of cancer | [7,8,17,18,20,26] |
| • The possible implications of a genetic test for patients (mainly on treatment) and family members | [7,8,17,18,20,26] |
| • Possible outcomes of a genetic test (i.e., normal result, pathogenic or uncertain variant) | [17,20,26] |
| • Costs | [17,18,20] |
| • The possibility of additional pre-test counseling at a genetics department | [17,18] |
| Informed consent | |
| • Written informed consent | [7,8,9,11,18,19,20,24,25,26] |
| • Oral and/or written informed consent | [23] |
| • Informed consent obtained (not specified as verbal or written) | [17,21,22,27] |
| Patient information material a | |
| A summary of the information discussed and/or additional information was provided to the patient in an information sheet after discussing the genetic test | [7,8,9,11,16,17,18,19,20,26,27] |
| Include a training module with |
| - key topics for pre-test counseling |
| - an informed consent procedure |
| Provide clear instructions indicating when patients are eligible for genetic testing |
| Include FAQ forms and a clear protocol |
| Invite patients directly for post-test counseling in case a pathogenic variant is found (without the necessity of a referral by the NGHCP) |
| Close collaboration between genetic and non-genetic departments |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bokkers, K.; Vlaming, M.; Engelhardt, E.G.; Zweemer, R.P.; van Oort, I.M.; Kiemeney, L.A.L.M.; Bleiker, E.M.A.; Ausems, M.G.E.M. The Feasibility of Implementing Mainstream Germline Genetic Testing in Routine Cancer Care—A Systematic Review. Cancers 2022, 14, 1059. https://doi.org/10.3390/cancers14041059
Bokkers K, Vlaming M, Engelhardt EG, Zweemer RP, van Oort IM, Kiemeney LALM, Bleiker EMA, Ausems MGEM. The Feasibility of Implementing Mainstream Germline Genetic Testing in Routine Cancer Care—A Systematic Review. Cancers. 2022; 14(4):1059. https://doi.org/10.3390/cancers14041059
Chicago/Turabian StyleBokkers, Kyra, Michiel Vlaming, Ellen G. Engelhardt, Ronald P. Zweemer, Inge M. van Oort, Lambertus A. L. M. Kiemeney, Eveline M. A. Bleiker, and Margreet G. E. M. Ausems. 2022. "The Feasibility of Implementing Mainstream Germline Genetic Testing in Routine Cancer Care—A Systematic Review" Cancers 14, no. 4: 1059. https://doi.org/10.3390/cancers14041059
APA StyleBokkers, K., Vlaming, M., Engelhardt, E. G., Zweemer, R. P., van Oort, I. M., Kiemeney, L. A. L. M., Bleiker, E. M. A., & Ausems, M. G. E. M. (2022). The Feasibility of Implementing Mainstream Germline Genetic Testing in Routine Cancer Care—A Systematic Review. Cancers, 14(4), 1059. https://doi.org/10.3390/cancers14041059