
Incidence and Risk Factors for Venous Thromboembolism in Female Patients Undergoing Breast Surgery

 ,
,  ,
,  , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Population Description
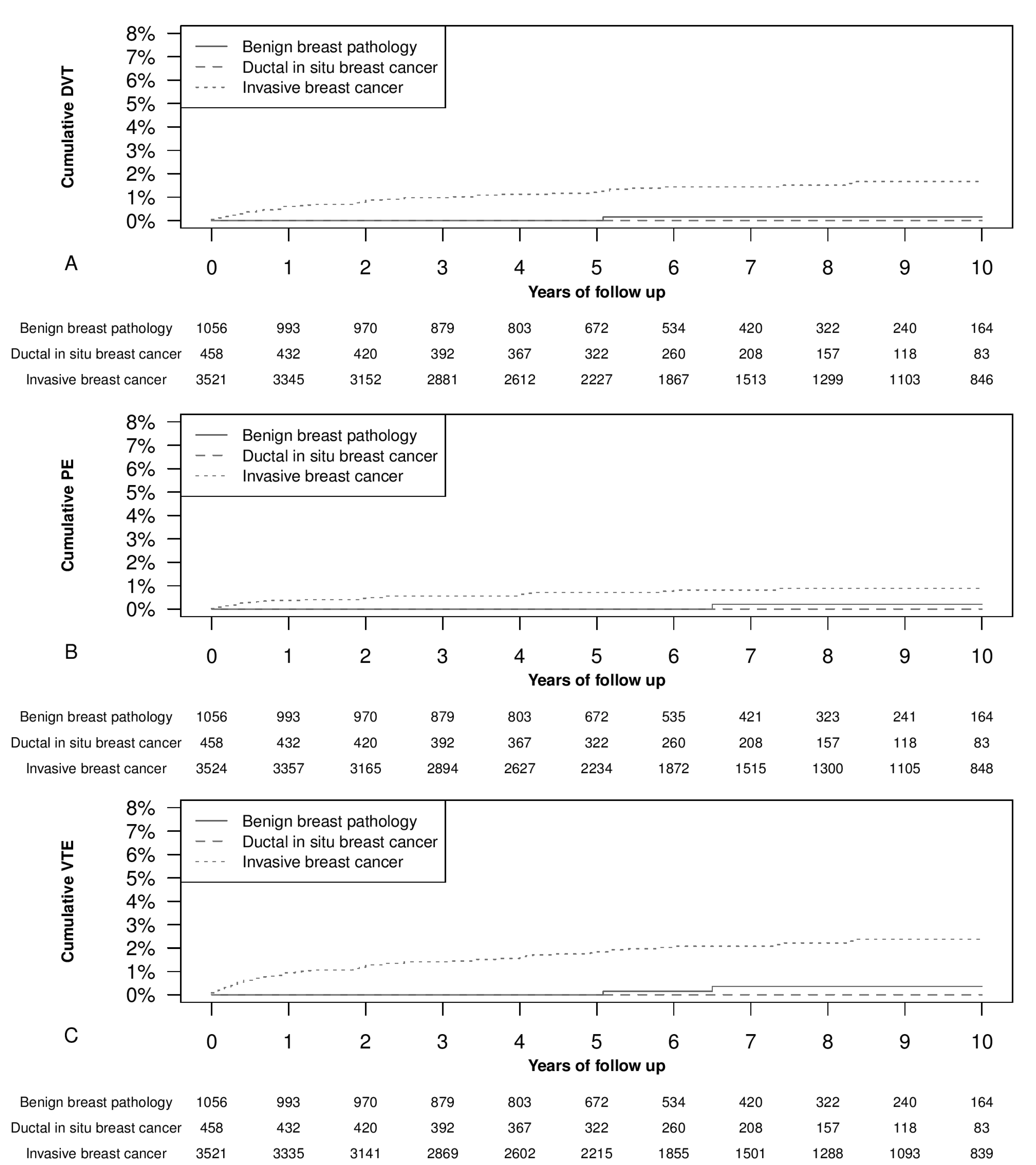
3.2. VENOUS Thromboembolism Occurrence
3.3. Factors Associated with Venous Thromboembolism Occurrence
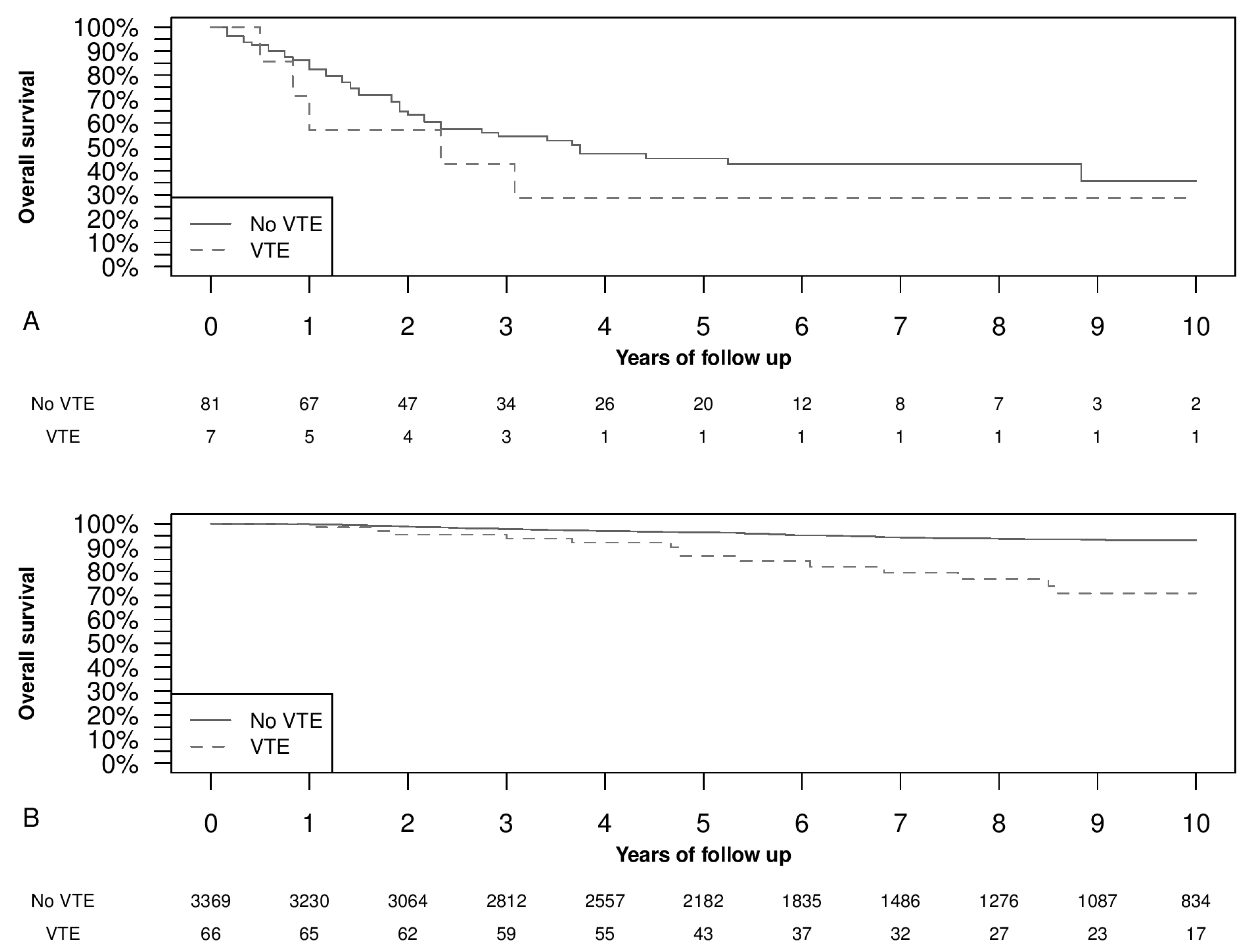
3.4. Overall Survival and Venous Thromboembolism Occurrence
4. Discussion
4.1. Venous Thromboembolism Occurrence
4.2. Factors Associated with VTE
4.3. Distant Metastases and Overall Survival
4.4. Strengths and Weaknesses
4.5. Generalisability
4.6. Relevance of the Findings and Unanswered Questions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Speed, V.; Roberts, L.N.; Patel, J.P.; Arya, R. Venous thromboembolism and women’s health. Br. J. Haematol. 2018, 183, 346–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tafur, A.J.; Fuentes, H.; Caprini, J.A.; Rivas, A.; Uresandi, F.; Duce, R.; López-Reyes, R.; Visonà, A.; Merah, A.; Monreal, M. Predictors of Early Mortality in Cancer-Associated Thrombosis: Analysis of the RIETE Database. TH Open 2018, 2, e158–e166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cedolini, C.; Bertozzi, S.; Londero, A.P.; Bernardi, S.; Seriau, L.; Concina, S.; Cattin, F.; Risaliti, A. Type of Breast Cancer Diagnosis, Screening, and Survival. Clin. Breast Cancer 2014, 14, 235–240. [Google Scholar] [CrossRef]
- Faiz, A.S.; Guo, S.; Kaveney, A.; Philipp, C.S. Risk of venous thromboembolism and endocrine therapy in older women with breast cancer in the United States. Blood Coagul. Fibrinolysis 2021, 32, 373–381. [Google Scholar] [CrossRef]
- Piccioli, A.; Prandoni, P.; Ewenstein, B.M.; Goldhaber, S.Z. Cancer and venous thromboembolism. Am. Heart J. 1996, 132, 850–855. [Google Scholar] [CrossRef]
- Kirwan, C.C.; Descamps, T.; Castle, J. Circulating tumour cells and hypercoagulability: A lethal relationship in metastatic breast cancer. Clin. Transl. Oncol. 2020, 22, 870–877. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, Y.; Wada, H.; Nomura, H.; Mizuno, T.; Saito, K.; Yamada, N.; Asanuma, K.; Usui, M.; Kamimoto, Y.; Matsumoto, T.; et al. Elevated Fibrin-related Markers in Patients with Malignant Diseases Frequently Associated with Disseminated Intravascular Coagulation and Venous Thromboembolism. Intern. Med. 2014, 53, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Vlenterie, M.; Desar, I.M.E.; Van Herpen, C.M.L.; Tol, J. Fatal microscopic pulmonary tumour embolisms in patients with breast cancer: Necessary knowledge for future medical practice. Neth. J. Med. 2014, 72, 28–31. [Google Scholar]
- Kyriazi, V. Breast Cancer as an Acquired Thrombophilic State. J. Breast Cancer 2012, 15, 148–156. [Google Scholar] [CrossRef] [Green Version]
- Momeni, A.; Fox, J.P. Venous Thromboembolism After Surgical Treatment of Breast Cancer. Ann. Plast. Surg. 2018, 80, 188–192. [Google Scholar] [CrossRef] [PubMed]
- von Tempelhoff, G.F.; Schönmann, N.; Heilmann, L. Thrombosis–a clue of poor prognosis in primary non-metastatic breast cancer? Breast Cancer Res. Treat. 2002, 73, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.J.; West, J.; Card, T.R.; Crooks, C.; Kirwan, C.C.; Grainge, M.J. When are breast cancer patients at highest risk of ve-nous thromboembolism? A cohort study using English health care data. Blood 2016, 127, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Khan, U.T.; Walker, A.J.; Baig, S.; Card, T.R.; Kirwan, C.C.; Grainge, M.J. Venous thromboembolism and mortality in breast can-cer: Cohort study with systematic review and meta-analysis. BMC Cancer 2017, 17, 747. [Google Scholar] [CrossRef] [Green Version]
- Kearon, C. Natural history of venous thromboembolism. Circulation 2003, 107, I22–I30. [Google Scholar] [CrossRef] [Green Version]
- Dentali, F.; Pegoraro, S.; Barco, S.; Di Minno, M.N.D.; Mastroiacovo, D.; Pomero, F.; Lodigiani, C.; Bagna, F.; Sartori, M.; Barillari, G.; et al. Clinical course of isolated distal deep vein thrombosis in patients with active cancer: A multicenter cohort study. J. Thromb. Haemost. 2017, 15, 1757–1763. [Google Scholar] [CrossRef] [Green Version]
- Londero, A.P.; Bernardi, S.; Bertozzi, S.; Angione, V.; Gentile, G.; Dri, C. Synchronous and metachronous breast malig-nancies: A cross-sectional retrospective study and review of the literature. Biomed. Res. Int. 2014, 2014, 250727. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Editorial Board. Breast Tumours, 5th ed.; World Health Organization: Geneva, Switzerland, 2019; pp. 181–185. [Google Scholar]
- Bertozzi, S.; Cedolini, C.; Londero, A.P.; Baita, B.; Giacomuzzi, F.; Capobianco, D.; Tortelli, M.; Uzzau, A.; Mariuzzi, L.; Risaliti, A.; et al. Sentinel lymph node biopsy in patients affected by breast ductal carcinoma in situ with and without microinvasion: Retrospective observational study. Medicine 2019, 98, e13831. [Google Scholar] [CrossRef]
- Cedolini, C.; Bertozzi, S.; Seriau, L.; Londero, A.P.; Concina, S.; Moretti, E.; Padovani, R.; Pasqualucci, A.; Ceschia, T.; Risaliti, A. Feasibility of concervative breast surgery and intraoperative radiation therapy for early breast cancer: A single-center, open, non-randomized, prospective pilot study. Oncol. Rep. 2014, 31, 1539–1546. [Google Scholar] [CrossRef] [Green Version]
- Bernardi, S.; Bertozzi, S.; Londero, A.P.; Gentile, G.; Angione, V.; Petri, R. Influence of Surgical Margins on the Outcome of Breast Cancer Patients: A Retrospective Analysis. World J. Surg. 2014, 38, 2279–2287. [Google Scholar] [CrossRef]
- Bertozzi, S.; Londero, A.P.; Giacomuzzi, F.; Angione, V.; Carbone, A.; Petri, R.; Bernardi, S. Applicability of two different validated models to predict axillary non-sentinel lymph node status by sentinel node biopsy in a single Italian center. Breast Cancer 2015, 22, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.J. A Class of K-Sample Tests for Comparing the Cumulative Incidence of a Competing Risk. Ann. Stat. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]
- Grambsch, P.M.; Therneau, T.M. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 1994, 81, 515–526. [Google Scholar] [CrossRef]
- Zammar, S.G.; Pockaj, B.A.; Stucky, C.C.; Wasif, N.; Gray, R.J. Is forgoing chemical venous thromboembolism prophylaxis for women undergoing breast-conserving surgery for breast cancer safe? Am. J. Surg. 2016, 212, 1162–1166. [Google Scholar] [CrossRef] [PubMed]
- Brand, J.S.; Hedayati, E.; Bhoo-Pathy, N.; Bergh, J.; Hall, P.; Humphreys, K.; Ludvigsson, J.F.; Czene, K. Time-dependent risk and predictors of ve-nous thromboembolism in breast cancer patients: A population-based cohort study. Cancer 2017, 123, 468–475. [Google Scholar] [CrossRef]
- Huang, L.; Li, J.; Jiang, Y. Association between hypertension and deep vein thrombosis after orthopedic surgery: A meta-analysis. Eur. J. Med. Res. 2016, 21, 13. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Yang, Y.; Chen, W.; Liang, L.; Zhai, Z.; Guo, L.; Wang, C.; Zhang, L.; China Venous Thromboembolism (VTE) Study Group. Hypertension associated with venous thromboembolism in patients with newly diagnosed lung cancer. Sci. Rep. 2016, 6, 19603. [Google Scholar] [CrossRef] [Green Version]
- Bertozzi, S.; Londero, A.P.; Bernardi, S.; Cedolini, C. Applicability of the Notthingham Prognostic Index for predicting the survival of triple-negative invasive breast cancer in a single Italian center. Eur. J. Gynaecol. Oncol. 2019, 40, 787–790. [Google Scholar]
- Bertozzi, S.; Londero, A.P.; Cedolini, C.; Uzzau, A.; Seriau, L.; Bernardi, S.; Bacchetti, S.; Pasqual, E.M.; Risaliti, A. Prevalence, risk factors, and prognosis of per-itoneal metastasis from breast cancer. Springerplus 2015, 4, 688. [Google Scholar] [CrossRef] [Green Version]
- Ording, A.G.; Horváth-Puhó, E.; Garne, J.P.; Nyström, P.W.; Vyberg, M.; Sørensen, H.T.; Lash, T.L. Impact of comorbidity on risk of venous thromboembolism in patients with breast cancer: A Danish population-based cohort study. BMJ Open 2014, 4, e005082. [Google Scholar] [CrossRef] [Green Version]
- Nazarzadeh, M.; Pinho-Gomes, A.; Mohseni, H.; Byrne, K.; Bidel, Z.; Dehghan, A.; Canoy, D.; Tran, J.; Raimondi, F.; Solares, R.A.; et al. Blood pressure and risk of venous thromboembolism: A large-scale prospective cohort analysis and a mendelian randomisation study. J. Hypertension. 2019, 37, e95. [Google Scholar] [CrossRef]
- Mandalà, M.; Tondini, C.A. Adjuvant therapy in breast cancer and venous thromboembolism. Thromb. Res. 2012, 130, S66–S70. [Google Scholar] [CrossRef] [PubMed]
- Xing, L.; Adhikari, V.P.; Liu, H.; Kong, L.Q.; Liu, S.C.; Li, H.Y.; Ren, G.S.; Luo, F.; Wu, K.N. Diagnosis prevention and treatment for PICC-related up-per extremity deep vein thrombosis in breast cancer patients. Asia Pac. J. Clin. Oncol. 2012, 8, e12–e16. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.H.; Nguyen, T.J.; Hwang, B.H.; Vidar, E.N.; Davis, G.B.; Chan, L.S.; Woo, K.; Wong, A.K. Risk factors associated with venous thrombo-embolism in 49,028 mastectomy patients. Breast 2013, 22, 444–448. [Google Scholar] [CrossRef]
- Brand, J.S.; Hedayati, E.; Humphreys, K.; Ludvigsson, J.F.; Johansson, A.; Bergh, J.; Hall, P.; Czene, K. Chemotherapy, Genetic Susceptibility, and Risk of Venous Thromboembolism in Breast Cancer Patients. Clin. Cancer Res. 2016, 22, 5249–5255. [Google Scholar] [CrossRef] [Green Version]
- Narod, S.; Nazarali, S. Tamoxifen for women at high risk of breast cancer. Breast Cancer Targets Ther. 2014, 6, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Onitilo, A.A.; Doi, S.A.R.; Engel, J.M.; Glurich, I.; Johnson, J.; Berg, R. Clustering of venous thrombosis events at the start of ta-moxifen therapy in breast cancer: A population-based experience. Thromb. Res. 2012, 130, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Jokuszies, A.; Radtke, C.; Betzler, C.; Branski, L.; Krämer, R.; Vogt, P.M. Is tamoxifen associated with an increased risk for thromboembolic complications in patients undergoing microvascular breast reconstruction? Ger. Med. Sci. 2013, 11, Doc05. [Google Scholar]
- Carr, D.F.; Turner, R.M.; Pirmohamed, M. Pharmacogenomics of anticancer drugs: Personalising the choice and dose to manage drug response. Br. J. Clin. Pharmacol. 2020, 87, 237–255. [Google Scholar] [CrossRef]
- Giaccherini, C.; Marchetti, M.; Masci, G.; Verzeroli, C.; Russo, L.; Celio, L.; Sarmiento, R.; Gamba, S.; Tartari, C.J.; Diani, E.; et al. Thrombotic biomarkers for risk prediction of malignant disease recurrence in patients with early stage breast cancer. Haematologica 2019, 105, 1704–1711. [Google Scholar] [CrossRef] [Green Version]
- Mego, M.; Zuo, Z.; Gao, H.; Cohen, E.N.; Giordano, A.; Tin, S.; Anfossi, S.; Jackson, S.; Woodward, W.; Ueno, N.T.; et al. Circulating tumour cells are linked to plasma D-dimer levels in patients with metastatic breast cancer. Thromb. Haemost. 2015, 113, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Prestidge, T.; Lee, S.; Harper, P.; Young, L.; Ockelford, P. Survival in patients with malignancy and venous thromboembo-lism by tumour subtype and thrombus location. Intern Med. J. 2012, 42, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Rosas, P.; Pesenti, M.; Verzeroli, C.; Giaccherini, C.; Russo, L.; Sarmiento, R.; Masci, G.; Celio, L.; Minelli, M.; Gamba, S.; et al. Validation of the Role of Thrombin Generation Potential by a Fully Automated System in the Identification of Breast Cancer Patients at High Risk of Disease Re-currence. TH Open. 2021, 5, e56–e65. [Google Scholar] [PubMed]
- Marchetti, M.; Giaccherini, C.; Masci, G.; Verzeroli, C.; Russo, L.; Celio, L.; Sarmiento, R.; Gamba, S.; Tartari, C.J.; Diani, E.; et al. Thrombin generation predicts early recur-rence in breast cancer patients. J. Thromb. Haemost. 2020, 18, 2220–2231. [Google Scholar] [CrossRef]
- Pather, K.; Dix-Peek, T.; Duarte, R.; Chetty, N.; Augustine, T. Breast cancer cell-induced platelet activation is compounded by tamoxifen and anastrozole in vitro. Thromb. Res. 2019, 177, 51–58. [Google Scholar] [CrossRef]
- Labelle, M.; Begum, S.; Hynes, R.O. Direct signaling between platelets and cancer cells induces an epithelial-mesenchymal-like transition and promotes metastasis. Cancer Cell 2011, 20, 576–590. [Google Scholar] [CrossRef] [Green Version]
- Riedl, J.; Hell, L.; Kaider, A.; Koder, S.; Marosi, C.; Zielinski, C.; Panzer, S.; Pabinger, I.; Ay, C. Association of platelet activation markers with cancer-associated venous thromboembolism. Platelets 2016, 27, 80–85. [Google Scholar] [CrossRef]
- Bambace, N.M.; Holmes, C.E. The platelet contribution to cancer progression. J. Thromb. Haemost. 2011, 9, 237–249. [Google Scholar] [CrossRef]
- van der Spuy, W.J.; Augustine, T.N. Ultrastructural investigation of the time-dependent relationship between breast cancer cells and thrombosis induction. BioMed Res. Int. 2016, 90, 59–63. [Google Scholar] [CrossRef]
- Nash, G.F.; Turner, L.F.; Scully, M.F.; Kakkar, A.K. Platelets and cancer. Lancet Oncol. 2002, 3, 425–430. [Google Scholar] [CrossRef]
- Mitrugno, A.; Williams, D.; Kerrigan, S.W.; Moran, N. A novel and essential role for FcγRIIa in cancer cell–induced platelet activation. Blood 2014, 123, 249–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwahara, M.; Sugimoto, M.; Tsuji, S.; Matsui, H.; Mizuno, T.; Miyata, S.; Yoshioka, A. Platelet Shape Changes and Adhesion Under High Shear Flow. Arter. Thromb. Vasc. Biol. 2002, 22, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Augustine, T.N.; van der Spuy, W.J.; Kaberry, L.L.; Shayi, M. Thrombin-Mediated Platelet Activation of Lysed Whole Blood and Platelet-Rich Plasma: A Comparison Between Platelet Activation Markers and Ultrastructural Alterations. Microsc. Microanal. 2016, 22, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Shirai, T.; Revenko, A.S.; Tibbitts, J.; Ngo, A.T.P.; Mitrugno, A.; Healy, L.D.; Johnson, J.; Tucker, E.I.; Hinds, M.T.; Coussens, L.M.; et al. Hepatic thrombopoietin gene silencing reduces platelet count and breast cancer progression in transgenic MMTV-PyMT mice. Blood Adv. 2019, 3, 3080–3091. [Google Scholar] [CrossRef] [Green Version]
- Mei, L.; Liu, Y.; Xia, C.; Zhou, Y.; Zhang, Z.; He, Q. Polymer–Drug Nanoparticles Combine Doxorubicin Carrier and Heparin Bioactivity Functionalities for Primary and Metastatic Cancer Treatment. Mol. Pharm. 2017, 14, 513–522. [Google Scholar] [CrossRef]
- Sun, H.; Cao, D.; Wu, H.; Liu, H.; Ke, X.; Ci, T. Development of low molecular weight heparin based nanoparticles for meta-static breast cancer therapy. Int. J. Biol. Macromol. 2018, 112, 343–355. [Google Scholar] [CrossRef]
- Serra, R.; Buffone, G.; Montemurro, R.; de Franciscis, S. Axillary vein thrombosis as the first clinical manifestation of inflammatory breast cancer: Report of a case. Surg. Today. 2013, 43, 100–102. [Google Scholar] [CrossRef]
- Ay, C.; Posch, F.; Kaider, A.; Zielinski, C.; Pabinger, I. Estimating risk of venous thromboembolism in patients with cancer in the presence of competing mortality. J. Thromb. Haemost. 2014, 13, 390–397. [Google Scholar] [CrossRef]
- Lévesque, L.E.; Hanley, J.A.; Kezouh, A.; Suissa, S. Problem of immortal time bias in cohort studies: Example using statins for preventing progression of diabetes. BMJ 2010, 340, b5087. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.-H.; Jhou, H.-J.; Chung, C.-H.; Lee, C.-H.; Wu, Y.-Y.; Chang, W.-C.; Chien, W.-C.; Chang, P.-Y. The Effect of Statins in Cancer Risk Reduction in Patients on Dialysis: A Population-Based Case-Control Study. J. Clin. Med. 2021, 10, 5602. [Google Scholar] [CrossRef]
- Inasu, M.; Feldt, M.; Jernström, H.; Borgquist, S.; Harborg, S. Statin use and patterns of breast cancer recurrence in the Malmö Diet and Cancer Study. Breast 2022, 61, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Zheng, H.; Xu, T.; Liu, X.; Liu, X.; Sun, L.; Pan, X.-F.; Mai, W.; Cai, X.; Huang, Y. Effects of statins in primary and secondary prevention for venous thromboembolism events: A meta analysis. Vasc. Pharmacol. 2021, 142, 106931. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sample | Variables | Values |
|---|---|---|
| (A) All the population | Woman age (years) | 57.72 (±14.27) |
| BMI (kg/m²) | 25.87 (±3.94) | |
| Tobacco smoke | 5.04% (254/5039) | |
| Familial history of cancer | 39.17% (378/965) | |
| Previous estrogen/progesterone use | 31.42% (224/713) | |
| Post-menopausal status | 73.09% (3681/5036) | |
| History of previous VTE | 1.61% (81/5039) | |
| Hypothyroidism | 11.33% (571/5039) | |
| Chronic hypertension | 26.35% (1328/5039) | |
| Chronic lung disease | 2.4% (121/5039) | |
| Chronic heart failure | 9.64% (486/5039) | |
| Breast surgery | ||
| Conservative | 61.38% (3093/5039) | |
| Mastectomy | 38.62% (1946/5039) | |
| Axilla surgery | 75.65% (3812/5039) | |
| Oncoplastic breast surgery | ||
| No plastic surgery | 76.38% (3849/5039) | |
| Immediate reconstruction | 12.24% (617/5039) | |
| Delayed reconstruction | 11.37% (573/5039) | |
| (B) Considering only breast invasive cancers | Non-surgical therapy | |
| Neoadjuvant chemotherapy | 5.48% (193/3524) | |
| Adjuvant radiotherapy | 54.57% (1923/3524) | |
| Adjuvant chemotherapy | 39.76% (1401/3524) | |
| Adjuvant hormonal therapy | 74.32% (2619/3524) | |
| Tumor characteristics | ||
| Comedo-like necrosis | 6.84% (241/3524) | |
| Multifocality/multicentricity | 17.93% (632/3524) | |
| EIC | 21.77% (767/3524) | |
| PVI | 14.25% (502/3524) | |
| Peritumoral inflammation | 2.47% (87/3524) | |
| Molecular subtype | ||
| Luminal A | 31.84% (1122/3524) | |
| Luminal B | 24.23% (854/3524) | |
| Luminal Her | 5.82% (205/3524) | |
| Her enriched | 4.37% (154/3524) | |
| Basal-like | 8.6% (303/3524) | |
| Unknown | 25.14% (886/3524) | |
| Lymph node characteristics | ||
| Isolated tumor cells | 2.21% (78/3524) | |
| Micrometastasis | 6.81% (240/3524) | |
| Extracapsular lymph node invasion | 8.97% (316/3524) | |
| Matted axilla lymph nodes | 3.18% (112/3524) | |
| Recurrences | ||
| Loco-regional | 5.7% (201/3524) | |
| Distant metastases | 7.01% (247/3524) |
| Variables | DVT | PE | VTE | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Woman’s age (years) | 1.04 (1.02–1.06) | <0.05 | 1.02 (0.99–1.05) | 0.214 | 1.03 (1.01–1.05) | <0.05 |
| BMI (kg/m²) | 1.08 (1.02–1.14) | <0.05 | 1.13 (1.06–1.2) | <0.05 | 1.1 (1.05–1.15) | <0.05 |
| Tobacco smoke | 1.24 (0.38–3.98) | 0.722 | 0.71 (0.1–5.2) | 0.733 | 0.83 (0.26–2.63) | 0.750 |
| Familial history of cancer | 0.44 (0.09–2.14) | 0.311 | 0.79 (0.07–8.69) | 0.846 | 0.52 (0.14–1.92) | 0.325 |
| Previous estrogen/progesterone use | 0.86 (0.17–4.45) | 0.861 | 1.43 (0.24–8.55) | 0.696 | 1.09 (0.33–3.6) | 0.894 |
| Post-menopausal status | 4.16 (1.49–11.57) | <0.05 | 3.01 (0.91–10) | 0.072 | 3.4 (1.56–7.43) | <0.05 |
| Diabetes mellitus | 0.81 (0.2–3.34) | 0.773 | 0.72 (0.1–5.31) | 0.748 | 0.84 (0.26–2.67) | 0.765 |
| Hypothyroidism | 1.28 (0.57–2.85) | 0.550 | 2.14 (0.86–5.3) | 0.101 | 1.55 (0.83–2.89) | 0.166 |
| Chronic hypertension | 3.78 (2.13–6.71) | <0.05 | 4.61 (2.11–10.07) | <0.05 | 4.33 (2.68–7.01) | <0.05 |
| Chronic lung disease | 0.89 (0.12–6.49) | 0.912 | 5.26 (1.58–17.46) | <0.05 | 1.9 (0.6–6.03) | 0.278 |
| Chronic heart failure | 1.62 (0.73–3.62) | 0.236 | 2.17 (0.82–5.73) | 0.118 | 1.97 (1.06–3.67) | <0.05 |
| Breast surgery | ||||||
| Conservative | Reference | --- | Reference | --- | Reference | --- |
| Mastectomy | 1.39 (0.79–2.45) | 0.256 | 2.06 (0.97–4.41) | 0.062 | 1.56 (0.97–2.49) | 0.065 |
| Axilla surgery | ||||||
| No axilla surgery | 0.08 (0.01–0.57) | <0.05 | 0.17 (0.02–1.37) | 0.097 | 0.12 (0.03–0.5) | <0.05 |
| SLNB | Reference | --- | Reference | --- | Reference | --- |
| CALND | 1.26 (0.7–2.28) | 0.438 | 1.78 (0.77–4.1) | 0.175 | 1.54 (0.93–2.55) | 0.092 |
| Oncoplastic breast surgery | ||||||
| No plastic surgery | Reference | --- | Reference | --- | Reference | --- |
| Immediate reconstruction | 1.45 (0.67–3.14) | 0.340 | 0.28 (0.04–2.09) | 0.215 | 1.05 (0.52–2.13) | 0.892 |
| Delayed reconstruction | 1.13 (0.47–2.69) | 0.785 | 1.17 (0.4–3.4) | 0.769 | 0.97 (0.46–2.04) | 0.932 |
| History of previous VTE | 1.31 (0.18–9.5) | 0.789 | 2.37 (0.32–17.45) | 0.398 | 1.82 (0.45–7.45) | 0.402 |
| Histology | ||||||
| Negative | Reference | --- | Reference | --- | Reference | --- |
| Ductal in situ carcinoma | 0 (0–Inf) (*) | 0.996 | 0 (0–Inf) (*) | 0.997 | 0 (0–Inf) (*) | 0.995 |
| Invasive carcinoma non-special type | 13.77 (1.89–100.49) | <0.05 | 7.47 (1–55.82) | <0.05 | 9.87 (2.4–40.56) | <0.05 |
| Lobular invasive carcinoma | 14.2 (1.71–117.92) | <0.05 | 4.71 (0.43–51.99) | 0.206 | 9.47 (2.01–44.61) | <0.05 |
| Ductal and lobular invasive carcinoma | 8.45 (0.77–93.21) | 0.081 | 4.29 (0.27–68.69) | 0.303 | 6.38 (1.07–38.21) | <0.05 |
| Other type of invasive carcinoma | 28.1 (3.14–251.38) | <0.05 | 28.58 (3.19–255.73) | <0.05 | 24.98 (5.19–120.25) | <0.05 |
| Variables | DVT | PE | VTE | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| All breast surgery cohort (*) | ||||||
| Woman’s age (years) | 1.02 (1–1.05) | 0.080 | ||||
| BMI (kg/m²) | 1.06 (1–1.12) | <0.05 | 1.10 (1.03–1.17) | <0.05 | 1.07 (1.02–1.11) | <0.05 |
| Chronic hypertension | 2.10 (1.13–3.89) | <0.05 | 2.84 (1.26–6.39) | <0.05 | 2.83 (1.72–4.65) | <0.05 |
| Invasive breast cancer | 13.55 (1.84–99.54) | <0.05 | 8.03 (1.07–60.15) | <0.05 | 10.71 (2.6–44.11) | <0.05 |
| Variables | DVT | PE | VTE | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Woman’s age (years) | 1.03 (1.01–1.05) | <0.05 | 1 (0.98–1.03) | 0.785 | 1.02 (1–1.04) | 0.065 |
| BMI (kg/m²) | 1.07 (1.02–1.13) | <0.05 | 1.12 (1.05–1.2) | <0.05 | 1.09 (1.05–1.14) | <0.05 |
| Tobacco smoke | 1.01 (0.93–1.1) | 0.751 | 0.75 (0.37–1.52) | 0.422 | 0.99 (0.91–1.07) | 0.754 |
| Familial history of cancer | 0.45 (0.09–2.16) | 0.319 | 0.79 (0.07–8.7) | 0.847 | 0.52 (0.14–1.93) | 0.332 |
| Previous estrogen/progesterone use | 1 (0.19–5.17) | 0.997 | 1.69 (0.28–10.14) | 0.564 | 1.27 (0.38–4.22) | 0.695 |
| Post-menopausal status | 2.78 (1–7.75) | 0.050 | 1.97 (0.59–6.56) | 0.269 | 2.25 (1.03–4.93) | <0.05 |
| Diabetes mellitus | 0.67 (0.16–2.77) | 0.583 | 0.61 (0.08–4.47) | 0.622 | 0.7 (0.22–2.22) | 0.545 |
| Hypothyroidism | 1.13 (0.5–2.51) | 0.771 | 1.94 (0.78–4.83) | 0.155 | 1.38 (0.74–2.58) | 0.308 |
| Chronic hypertension | 2.6 (1.46–4.63) | <0.05 | 3.65 (1.63–8.2) | <0.05 | 3.13 (1.92–5.11) | <0.05 |
| Chronic lung disease | 0.72 (0.1–5.22) | 0.745 | 4.3 (1.29–14.32) | <0.05 | 1.54 (0.48–4.89) | 0.467 |
| Chronic heart failure | 1.21 (0.54–2.7) | 0.640 | 1.65 (0.62–4.37) | 0.315 | 1.48 (0.8–2.77) | 0.215 |
| Breast surgery | ||||||
| Conservative | Reference | --- | Reference | --- | Reference | --- |
| Mastectomy | 0.98 (0.55–1.74) | 0.942 | 1.52 (0.7–3.32) | 0.288 | 1.11 (0.69–1.79) | 0.656 |
| Axilla surgery | ||||||
| SLNB | Reference | --- | Reference | --- | Reference | --- |
| CALND | 1.09 (0.6–1.96) | 0.775 | 1.55 (0.67–3.56) | 0.305 | 1.33 (0.81–2.2) | 0.264 |
| Oncoplastic breast surgery | ||||||
| No plastic surgery | Reference | --- | Reference | --- | Reference | --- |
| Immediate reconstruction | 1.07 (0.49–2.31) | 0.866 | 0.21 (0.03–1.56) | 0.128 | 0.78 (0.38–1.58) | 0.486 |
| Delayed reconstruction | 0.96 (0.4–2.3) | 0.930 | 1.02 (0.35–2.98) | 0.969 | 0.83 (0.4–1.76) | 0.631 |
| History of previous VTE | 1 (0.14–7.23) | 0.997 | 1.83 (0.25–13.48) | 0.555 | 1.4 (0.34–5.71) | 0.641 |
| Histology | ||||||
| Invasive carcinoma non-special type | Reference | --- | Reference | --- | Reference | --- |
| Lobular invasive carcinoma | 1.03 (0.43–2.45) | 0.946 | 0.63 (0.15–2.7) | 0.533 | 0.96 (0.45–2.02) | 0.912 |
| Ductal and lobular invasive carcinoma | 0.62 (0.15–2.56) | 0.504 | 0.58 (0.08–4.32) | 0.594 | 0.65 (0.2–2.08) | 0.468 |
| Other type of invasive carcinoma | 2.04 (0.72–5.74) | 0.177 | 3.8 (1.29–11.19) | <0.05 | 2.52 (1.14–5.57) | <0.05 |
| Variables | DVT | PE | VTE | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Tumor staging | ||||||
| Tumor size (T3 or T4) | 2.6 (1.03–6.58) | <0.05 | 3.9 (1.34–11.34) | <0.05 | 3.3 (1.63–6.66) | <0.05 |
| Nodal status (N2 or N3) | 3.59 (1.94–6.64) | <0.05 | 1.35 (0.46–3.93) | 0.580 | 2.94 (1.73–5) | <0.05 |
| Tumor grading (G3) | 1.63 (0.9–2.95) | 0.108 | 2.48 (1.15–5.35) | <0.05 | 1.9 (1.17–3.08) | <0.05 |
| TNM stage (III or IV) | 3.57 (1.98–6.44) | <0.05 | 2.06 (0.87–4.92) | 0.102 | 3.11 (1.89–5.12) | <0.05 |
| Tumor characteristics | ||||||
| Comedo-like necrosis | 0.6 (0.15–2.47) | 0.480 | 4.12 (1.65–10.26) | <0.05 | 1.57 (0.72–3.43) | 0.259 |
| Multifocality/multicentricity | 1.36 (0.69–2.68) | 0.370 | 1.66 (0.7–3.95) | 0.251 | 1.38 (0.79–2.42) | 0.259 |
| EIC | 0.67 (0.31–1.43) | 0.295 | 1.48 (0.64–3.41) | 0.356 | 0.93 (0.52–1.65) | 0.800 |
| PVI | 0.97 (0.41–2.29) | 0.950 | 1.18 (0.41–3.44) | 0.755 | 1.14 (0.58–2.23) | 0.708 |
| Peritumoral inflammation | 1.68 (0.41–6.94) | 0.471 | 0 (0–Inf) (*) | 0.997 | 1.15 (0.28–4.69) | 0.848 |
| Molecular subtype (Basal-like) | 3.15 (1.57–6.34) | <0.05 | 2.07 (0.71–6.02) | 0.180 | 2.47 (1.33–4.62) | <0.05 |
| Lymph nodes characteristics | ||||||
| Non axillary locoregional lymph nodes | 1.54 (0.21–11.19) | 0.668 | 0 (0–Inf) (*) | 0.996 | 1.06 (0.15–7.6) | 0.957 |
| Isolated tumor cells | 0 (0–Inf) (*) | 0.996 | 3.52 (0.83–14.89) | 0.087 | 1.27 (0.31–5.18) | 0.740 |
| Micrometastasis | 0.94 (0.29–3.01) | 0.912 | 2.51 (0.86–7.27) | 0.091 | 1.59 (0.73–3.47) | 0.247 |
| Extracapsula invasion | 2.75 (1.33–5.7) | <0.05 | 2.07 (0.71–6.03) | 0.180 | 2.73 (1.49–5) | <0.05 |
| Matted axilla lymph nodes | 2.52 (0.78–8.14) | 0.121 | 6.56 (2.26–19.09) | <0.05 | 4.24 (1.94–9.28) | <0.05 |
| Recurrences | ||||||
| Locoregional recurrence | 1.01 (0.31–3.27) | 0.982 | 2.79 (0.96–8.1) | 0.060 | 1.73 (0.79–3.79) | 0.170 |
| Distant metastases | 6.98 (3.77–12.91) | <0.05 | 3.49 (1.31–9.27) | <0.05 | 5.79 (3.4–9.84) | <0.05 |
| Non-surgical therapies | ||||||
| Neoadjuvant chemotherapy | 0.76 (0.18–3.12) | 0.700 | 2.23 (0.67–7.45) | 0.190 | 1.35 (0.54–3.36) | 0.515 |
| Adjuvant radiotherapy | 1.71 (0.93–3.16) | 0.086 | 0.69 (0.32–1.48) | 0.337 | 1.29 (0.79–2.11) | 0.301 |
| Adjuvant chemotherapy | 2.41 (1.34–4.35) | <0.05 | 1.5 (0.7–3.24) | 0.299 | 2.02 (1.25–3.26) | <0.05 |
| Adjuvant hormonal therapy | 1.07 (0.54–2.1) | 0.847 | 0.62 (0.27–1.38) | 0.242 | 0.91 (0.53–1.56) | 0.729 |
| Tamoxifen | 0.76 (0.42–1.4) | 0.382 | 0.8 (0.36–1.8) | 0.589 | 0.76 (0.46–1.26) | 0.292 |
| Variables | DVT | PE | VTE | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Invasive breast cancer sub-cohort (†) | ||||||
| Woman’s age (years) | 1.04 (1.01–1.07) | <0.05 | ||||
| BMI (kg/m²) | 1.06 (1.01–1.12) | <0.05 | 1.10 (1.03–1.17) (¶) | <0.05 | 1.06 (1.00–1.12) (¶) | 0.054 |
| Chronic hypertension | 1.98 (1.07–3.63) | <0.05 | 2.99 (1.31–6.85) (¶) | <0.05 | 2.35 (1.3–4.24) (¶) | <0.05 |
| Chronic lung disease | 2.93 (0.87–9.90) (§) | 0.084 | ||||
| Other type of invasive carcinoma | 3.5 (1.18–10.39) (§) | <0.05 | 1.93 (0.69–5.4) (§) | 0.211 | ||
| TNM stage (III–IV) | 1.91 (1–3.65) | 0.050 | 3.63 (2.01–6.55) (§) | <0.05 | ||
| Comedo-like necrosis | 5.24 (2.08–13.19) (§) | <0.05 | 0.69 (0.17–2.86) (§) | 0.612 | ||
| Molecular subtype (basal-like) | 2.46 (1.19–5.08) | <0.05 | 3.56 (1.76–7.18) (§) | <0.05 | ||
| Matted axilla lymph nodes | 7.4 (2.53–21.69) (§) | <0.05 | ||||
| Locoregional recurrence | 0.44 (0.13–1.51) | 0.193 | 2.89 (0.99–8.42) (§) | 0.052 | ||
| Distant metastases diagnosed during follow-up | 4.42 (2.17–8.99) | <0.05 | 7.04 (3.8–13.04) (§) | <0.05 | ||
| Adjuvant radiotherapy | 1.74 (0.92–3.26) | 0.086 | ||||
| Adjuvant chemotherapy | 2.11 (1.02–4.37) | <0.05 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Londero, A.P.; Bertozzi, S.; Cedolini, C.; Neri, S.; Bulfoni, M.; Orsaria, M.; Mariuzzi, L.; Uzzau, A.; Risaliti, A.; Barillari, G. Incidence and Risk Factors for Venous Thromboembolism in Female Patients Undergoing Breast Surgery. Cancers 2022, 14, 988. https://doi.org/10.3390/cancers14040988
Londero AP, Bertozzi S, Cedolini C, Neri S, Bulfoni M, Orsaria M, Mariuzzi L, Uzzau A, Risaliti A, Barillari G. Incidence and Risk Factors for Venous Thromboembolism in Female Patients Undergoing Breast Surgery. Cancers. 2022; 14(4):988. https://doi.org/10.3390/cancers14040988
Chicago/Turabian StyleLondero, Ambrogio P., Serena Bertozzi, Carla Cedolini, Silvia Neri, Michela Bulfoni, Maria Orsaria, Laura Mariuzzi, Alessandro Uzzau, Andrea Risaliti, and Giovanni Barillari. 2022. "Incidence and Risk Factors for Venous Thromboembolism in Female Patients Undergoing Breast Surgery" Cancers 14, no. 4: 988. https://doi.org/10.3390/cancers14040988
APA StyleLondero, A. P., Bertozzi, S., Cedolini, C., Neri, S., Bulfoni, M., Orsaria, M., Mariuzzi, L., Uzzau, A., Risaliti, A., & Barillari, G. (2022). Incidence and Risk Factors for Venous Thromboembolism in Female Patients Undergoing Breast Surgery. Cancers, 14(4), 988. https://doi.org/10.3390/cancers14040988