
Hemodynamic, Surgical and Oncological Outcomes of 40 Distal Pancreatectomies with Celiac and Left Gastric Arteries Resection (DP CAR) without Arterial Reconstructions and Preoperative Embolization

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Surgery
2.2. Statistics
3. Results
3.1. Patient Characteristics and DP-CAR Outcomes
3.1.1. Postoperative Complications after DP CAR
3.1.2. Long-Term Outcomes after DP CAR and Perioperative Factors Affecting the Survival
3.2. Arterial Geometry Data before and after DP CAR
Analysis of Intraoperative and Ultrasound Data
4. Discussion
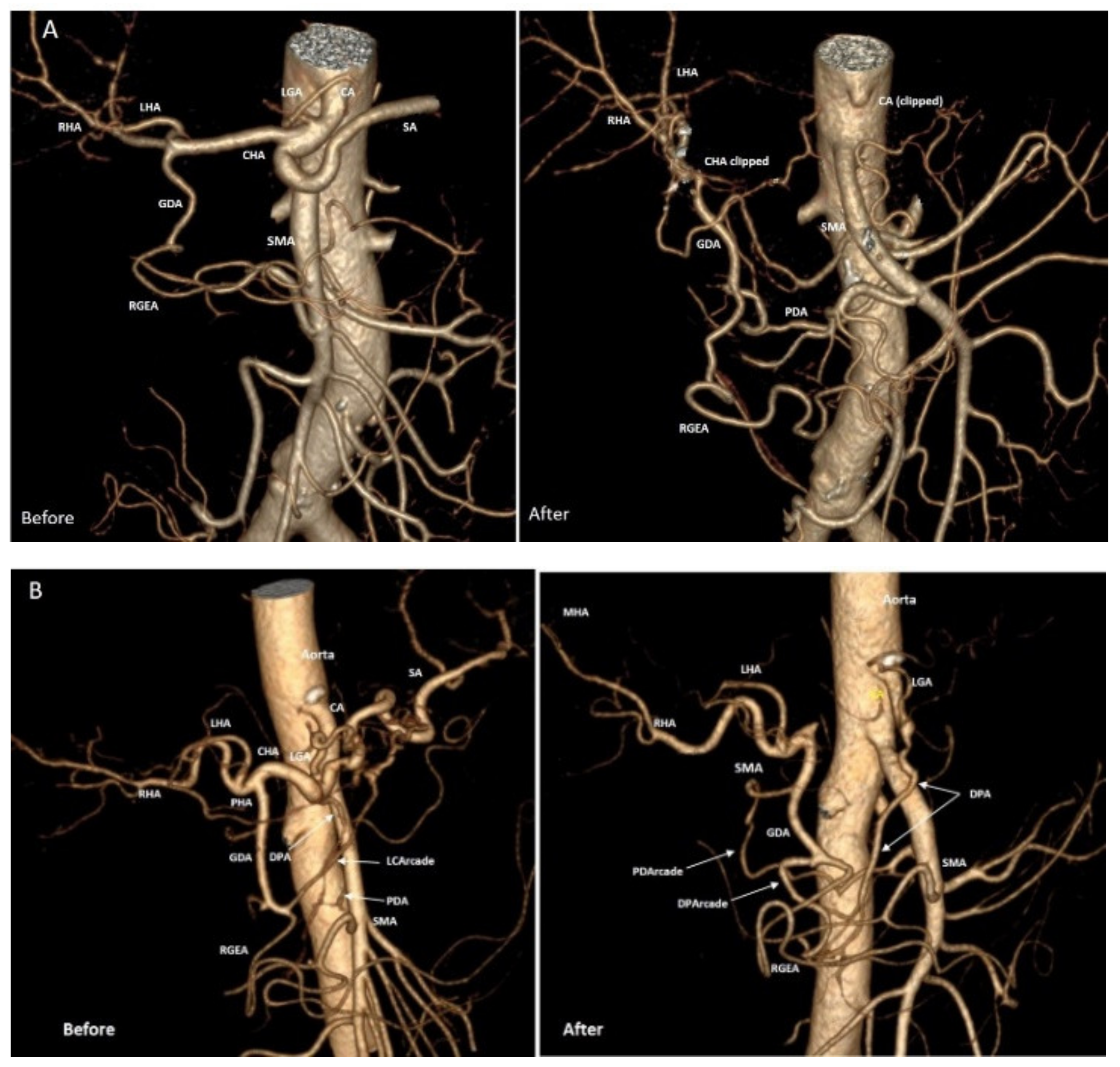
- Reduction of the GDA diameter (not dependent on surgical manipulations on GDA) against the background of enlargement of the PDA and other collaterals after acute celiac axis blockade was the first described phenomenon. Apparently, the narrowing of a certain segment of the arterial pathway with enlargement of the other parts may be an adaptive process. The latter would be energetically favorable for maintaining sufficient hepatic blood flow to meet the advanced energy requirements of the stomach. This phenomenon needs further research [60,61,62], considering its unpredictability for modeling [63]. At the same time, modeling of the celiac axis critical stenosis was able to predict the increase in diameter of some arteries of the pancreaticoduodenal arcade by more than 2–3 times [63], which is in line with our data.
- In contrast to the model [63], our data demonstrate that based on arterial geometry data acquired by CT before DP CAR, one cannot predict the disappearance of pulsation and linear blood velocity reduction in the arteries of hepatoduodenal ligament, as well as changes of diameters and volumetric flow rates in the arteries of pancreaticoduodenal arcade after surgery.
- The absence of a closed pancreaticoduodenal arcade is not a contraindication for DP CAR due to well-developed adaptive mechanisms in the arteries of the pancreaticoduodenal arcade. Arterial reconstructions in these patients seem unusual events.
- All cases of ischemic gastropathy developed in cases of small (>2 mm) or extremely small (#19, 1.1 mm) preoperative PDA diameters and were not accompanied by liver ischemia.
- The data obtained may demonstrate that the preoperative diameter of the PDA, a key vessel comprising the pancreatoduodenal arcade, is much more important for the stomach collateral supply than for the liver. Hence the quantification of the PDA diameter (>2 mm<) prior to surgery as a factor for the assessment of the gastric ischemia risk can be helpful
- a)
- before DPCAR and
- b)
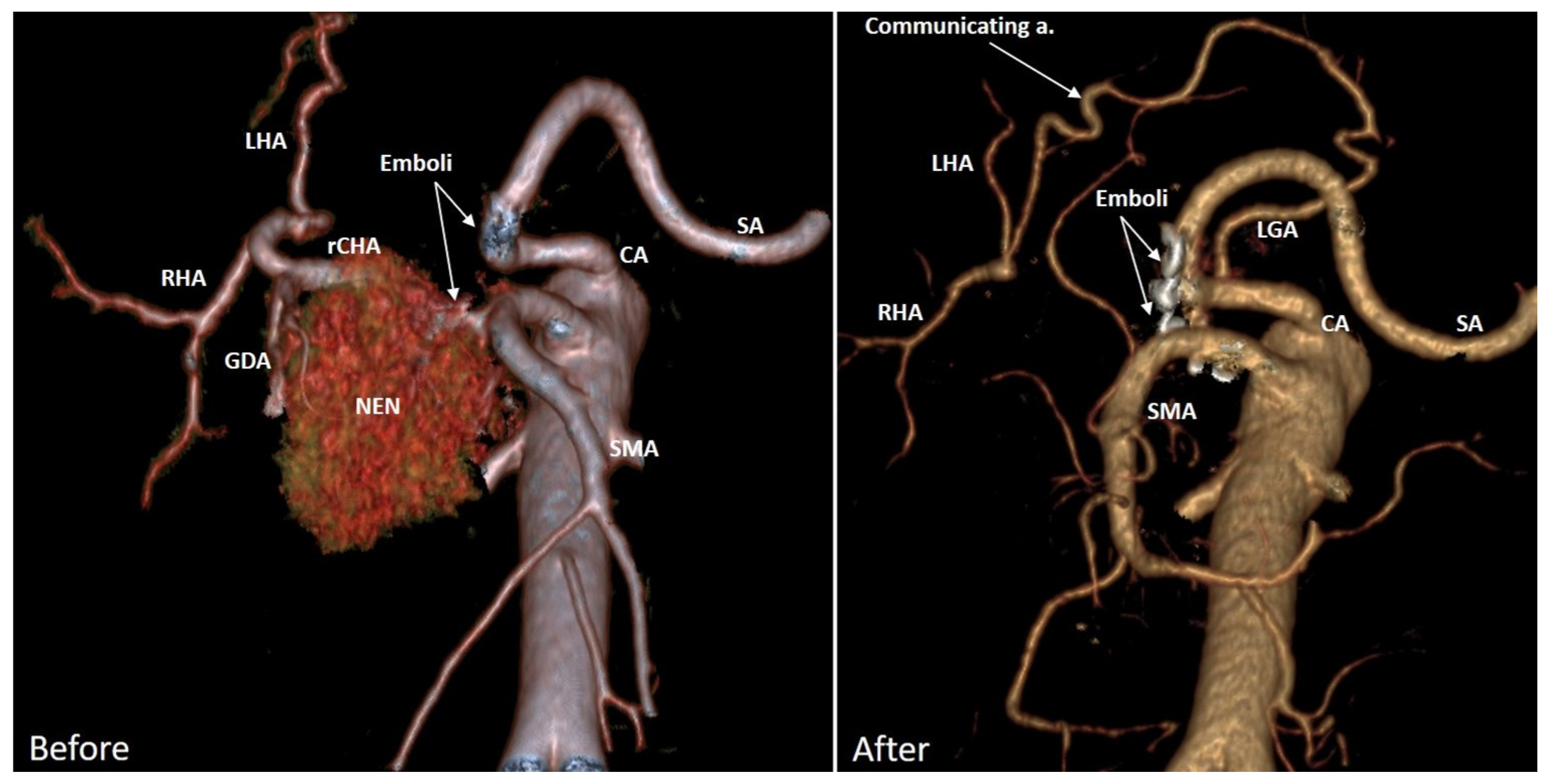
- after pre-DPCAR common hepatic artery embolization (COHE). COHE is done with the expectation of an increase in the PDA in diameter before DPCAR. However, this may not happen due to switching on the collaterals other than the desired PD arcade, and these alternative arcades can be sacrificed during PDAC. Two examples in Figure 5 and Figure 6 demonstrate this possibility, and clinical data [13,15,23,25] can be explained by these observations. It makes the necessity of CT-monitoring of the CHAE efficacy relevant.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Baxter, N.N.; Whitson, B.A.; Tuttle, T.M. Trends in the treatment and outcome of pancreatic cancer in the United States. Ann. Surg. Oncol. 2007, 14, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Iacobuzio-Donahue, C.A.; Fu, B.; Yachida, S.; Luo, M.; Abe, H.; Henderson, C.M.; Vilardel, F.; Wang, Z.; Keller, J.W.; Banerjee, P.; et al. DPC4 gene status of the primary carcinoma correlates with patterns of failure in patients with pancreatic cancer. J. Clin. Oncol. 2009, 27, 1806–1813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamisawa, T.; Isawa, T.; Koike, M.; Tsuruta, K.; Okamoto, A. Hematogenous metastases of pancreatic ductal carcinoma. Pancreas 1995, 11, 345–349. [Google Scholar] [CrossRef]
- Mao, C.; Domenico, D.R.; Kim, K.; Hanson, D.J.; Howard, J.M. Observations on the developmental patterns and the consequences of pancreatic exocrine adenocarcinoma. Findings of 154 autopsies. Arch. Surg. 1995, 30, 125–134. [Google Scholar] [CrossRef]
- Peixoto, R.D.; Speers, C.; McGahan, C.E.; Renouf, D.J.; Schaeffer, D.F.; Kennecke, H.F. Prognostic factors and sites of metastasis in unresectable locally advanced pancreatic cancer. Cancer Med. 2015, 4, 1171–1177. [Google Scholar] [CrossRef]
- Sugumar, K.; Hue, J.J.; Hardacre, J.M.; Ammori, J.B.; Rothermel, L.D.; Dorth, J.; Saltzman, J.; Mohamed, A.; Selfridge, J.E.; Bajor, D.; et al. Combined multiagent chemotherapy and radiotherapy is associated with prolonged overall survival in patients with non-operatively managed stage II-III pancreatic adenocarcinoma. HPB 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Bachellier, P.; Addeo, P.; Faitot, F.; Nappo, G.; Dufour, P. Pancreatectomy with arterial resection for pancreatic adenocarcinoma: How can it be done safely and with which outcomes? A single institution’s experience with 118 patients. Ann. Surg. 2020, 271, 932–940. [Google Scholar] [CrossRef] [PubMed]
- Truty, M.; Kendrick, M.; Nagorney, D.; Smoot, R.; Cleary, S.; Graham, R.; Goenka, A.; Hallemeier, C.; Haddock, M.; Harmsen, W.; et al. Factors predicting response, perioperative outcomes, and survival following total neoadjuvant therapy for borderline/locally advanced pancreatic cancer. Ann. Surg. 2021, 273, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Cloyd, J.M.; Katz, M.H.; Prakash, L.; Varadhachary, G.R.; Wolff, R.A.; Shroff, R.T.; Javle, M.; Fogelman, D.; Overman, M.; Crane, C.H.; et al. Preoperative therapy and pancreatoduodenectomy for pancreatic ductal adenocarcinoma: A 25-year single-institution experience. J. Gastrointest. Surg. 2017, 21, 164–174. [Google Scholar] [CrossRef]
- Schmocker, R.K.; Wright, M.J.; Ding, D.; Beckman, M.l.J.; Javed, A.A.; Cameron, J.L.; Lafaro, K.J.; Burns, W.R.; Weiss, M.J.; He, J.; et al. An aggressive approach to locally confined pancreatic cancer: Defining surgical and oncologic outcomes unique to pancreatectomy with celiac axis resection (DP-CAR). Ann. Surg. Oncol. 2021, 28, 3125–3134. [Google Scholar] [CrossRef]
- Ocuin, L.M.; Miller-Ocuin, J.L.; Novak, S.M.; Bartlett, D.L.; Marsh, J.W.; Tsung, A.; Lee, K.K.; Hogg, M.E.; Zeh, H.J.; Zureikat, A.H. Robotic and open distal pancreatectomy with celiac axis resection for locallyadvanced pancreatic body tumors: A single institutional assessment of perioperative outcomes and survival. HPB 2016, 18, 835–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, T.; Hirano, S.; Noji, T.; Asano, T.; Okamura, K.; Tsuchikawa, T.; Murakami, S.; Kurashima, Y.; Ebihara, Y.; Nakanishi, Y.; et al. Distal pancreatectomy with en bloc celiac axis resection (modified Appleby procedure) for locally advanced pancreatic body cancer: A single-center review of 80 consecutive patients. Ann. Surg. Oncol. 2016, 23, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Yoshitomi, H.; Sakai, N.; Kagawa, S.; Takano, S.; Ueda, A.; Kato, A.; Furukawa, K.; Takayashiki, T.; Kuboki, S.; Miyzaki, M.; et al. Feasibility and safety of distal pancreatectomy with en bloc celiac axis resection (DP-CAR) combined with neoadjuvant therapy for borderline resectable and unresectable pancreatic body/tail cancer. Langenbecks Arch. Surg. 2019, 404, 451–458. [Google Scholar] [CrossRef]
- Truty, M.J.; Colglazier, J.J.; Mendes, B.C.; Nagorney, D.M.; Bower, T.C.; Smoot, R.L.; DeMartino, R.R.; Cleary, S.P.; Oderich, G.S.; Kendrick, M.L. En bloc celiac axis resection for pancreatic cancer: Classification of anatomical variants based on tumor extent. J. Am. Coll. Surg. 2020, 231, 8–29. [Google Scholar] [CrossRef]
- Appleby, L.H. The coeliac axis in the expansion of the operation for gastric carcinoma. Cancer 1953, 6, 704–707. [Google Scholar] [CrossRef]
- Nimura, Y.; Hattori, T.; Miura, K. A case of advanced carcinoma of the body and tail of the pancreas resected by the Appleby operation. Shujutu 1976, 30, 885–889. (In Japanese) [Google Scholar]
- Hishinuma, S.; Ogata, Y.; Tomikawa, M.; Ozawa, I. Stomach-preserving distal pancreatectomy with combined resection of the celiac artery: Radical procedure for locally advanced cancer of the pancreatic body. J. Gastrointest. Surg. 2007, 11, 743–749. [Google Scholar] [CrossRef]
- Michels, N.A. Collateral arterial pathways to the liver after ligation of the hepatic artery and removal of the celiac axis. Cancer 1953, 6, 708–724. [Google Scholar] [CrossRef]
- Klompmaker, S.; Peters, N.A.; Van Hilst, J.; Bassi, C.; Boggi, U.; Busch, O.R.; Niesen, W.; Van Glik, T.M.; Javed, A.A.; Kleeff, J. Outcomes and risk score for distal pancreatectomy with celiac axis resection (DPCAR): An international multicenter analysis. Ann. Surg. Oncol. 2019, 26, 772–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, N.A.; Javed, A.A.; Cameron, J.L.; Makary, M.A.; Hirose, K.; Pawlik, T.M.; He, J.; Wolfgang, C.L.; Weiss, M.J. Modified Appleby procedure for pancreatic adenocarcinoma: Does improved neoadjuvant therapy warrant such an aggressive approach? Ann. Surg. Oncol. 2016, 23, 3757–3764. [Google Scholar] [CrossRef]
- Nigri, G.; Petrucciani, N.; Belloni, E.; Lucarini, A.; Aurello, P.; D’Angelo, F.; Di Saverio, S.; Fancellu, A.; Ramacciato, G. Distal pancreatectomy with celiac axis resection: Systematic review and meta-analysis. Cancers 2021, 13, 1967. [Google Scholar] [CrossRef]
- Klompmaker, S.; Van Hilst, J.; Gerritsen, S.L.; Adham, M.; Teresa Albiol Quer, M.; Bassi, C.; Berrevoet, F.; Boggi, U.; Busch, O.R.; Cesaretti, M.; et al. E-AHPBA DP-CAR study group. Outcomes After Distal Pancreatectomy with Celiac Axis Resection for Pancreatic Cancer: A Pan-European Retrospective Cohort Study. Ann. Surg Oncol. 2018, 25, 1440–1447. [Google Scholar] [CrossRef] [Green Version]
- Denecke, T.; Andreou, A.; Podrabsky, P.; Grieser, C.; Warnick, P.; Bahra, M.; Klein, F.; Hamm, B.; Neuhaus, P.; Glanemann, M. Distal pancreatectomy with en bloc resection of the celiac trunk for extended pancreatic tumor disease: An interdisciplinary approach. Cardiovasc. Intervent. Radiol. 2011, 34, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Ueda, A.; Sakai, N.; Yoshitomi, H.; Furukawa, K.; Takayashiki, T.; Kuboki, S.; Takano, S.; Suzuki, D.; Kagawa, S.; Mishima, T.; et al. Is hepatic artery coil embolization useful in distal pancreatectomy with en bloc celiac axis resection for locally advanced pancreatic cancer? World J. Surg. Oncol. 2019, 17, 124. [Google Scholar] [CrossRef] [Green Version]
- Kondo, S.; Katoh, H.; Shimizu, T.; Omi, M.; Hirano, S.; Ambo, Y.; Okushiba, S.; Morikawa, T. Preoperative embolization of the common hepatic artery in preparation for radical pancreatectomy for pancreas body cancer. Hepatogastroenterology 2000, 47, 1447–1449. [Google Scholar] [PubMed]
- Abo, D.; Hasegawa, Y.; Sakuhara, Y.; Terae, S.; Shimizu, T.; Tha, K.K.; Tanaka, E.; Hirano, S.; Kondo, S.; Shirato, H. Feasibility of a dual microcatheter-dual interlocking detachable coil technique in preoperative embolization in preparation for distal pancreatectomy with en bloc celiac axis resection for locally advanced pancreatic body cancer. J. Hepatobiliary Pancreat. Sci. 2012, 19, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Hirai, I.; Kimura, W.; Kamiga, M.; Mizutani, M.; Takeshita, A.; Watanabe, T.; Fuse, A. The significance of intraoperative Doppler ultrasonography in evaluating hepatic arterial flow when assessing the indications for the Appleby procedure for pancreatic body cancer. J. Hepatobiliary Pancreat. Surg. 2005, 12, 55–60. [Google Scholar] [CrossRef]
- Yamagami, T.; Yoshimatsu, R.; Kajiwara, K.; Ishikawa, M.; Murakami, Y.; Uemura, K.; Awai, K. Arteriography after embolization before distal pancreatectomy with en bloc celiac axis resection. Minim. Invasive Ther. Allied Technol. 2015, 24, 350–355. [Google Scholar] [CrossRef]
- Miyakawa, S.; Horiguchi, A.; Hanai, T.; Mizuno, K.; Ishihara, S.; Niwamoto, N.; Iwase, Y.; Asano, Y.; Furusawa, K.; Miura, K.; et al. Monitoring hepatic venous hemoglobin oxygen saturtion during Appleby operation for pancreatic cancer. Hepatogastroenterology 2002, 49, 817–821. [Google Scholar]
- Raut, V.; Takaori, K.; Kawaguchi, Y.; Mizumoto, M.; Kawaguchi, M.; Koizumi Kodama, S.; Kida, A.; Uemoto, S. Laparoscopic common hepatic artery ligation and staging followed by distal pancreatectomy with en blocresection of celiac artery for advanced pancreatic cancer. Asian J. Endosc. Surg. 2011, 4, 99–202. [Google Scholar] [CrossRef] [PubMed]
- Trabulsi, N.; Pelletier, J.S.; Abraham, C.; Vanounou, T. Preoperative diagnostic angiogram and endovascular aortic stent placement for appleby resection candidates: A novel surgical technique in the management of locally advanced pancreatic cancer. HPB Surg. 2015, 2015, 523273. [Google Scholar] [CrossRef] [Green Version]
- Miura, T.; Hirano, S.; Nakamura, T.; Tanaka, E.; Shichinohe, T.; Tsuchikawa, T.; Kato, K.; Matsumoto, J.; Kondo, S. A new preoperative prognostic scoring system to predict prognosis in patients with locally advanced pancreatic body cancer who undergo distal pancreatectomy with en bloc celiac axis resection: A retrospective cohort study. Surgery 2014, 155, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Sakamoto, Y.; Sano, T.; Kosuge, T. Prognostic factors after distal pancreatectomy with extended lymphadenectomy for invasive pancreatic adenocarcinoma of the body and tail. Surgery 2006, 139, 288–295. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Abu Hilal, M.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. International study group on pancreatic surgery (ISGPS). The 2016 update of the international study group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Wente, M.N.; Veit, J.A.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; et al. Postpancreatectomy hemorrhage (PPH)—An international study group of pancreatic surgery (ISGPS) definition. Surgery 2007, 142, 20–25. [Google Scholar] [CrossRef]
- Helliwell, T.; Woolgar, J.A. Standards and Minimum Datasets for Reporting Cancers; Minimum Dataset for the Histopathological Reporting of Pancreatic, Ampulla of Vater and Bile Duct Carcinoma; The Royal College of Pathologists: London, UK, 2002. [Google Scholar]
- Kakar, S.; Shi, C.; Adsay, V.; Bergsland, E.; Berlin, J.; Branton, P.; Fitzgibbons, P.; Wendy, L.; Frankel Klimstra, D.S.; Krasinskas, A.M.; et al. Gastrointestinal • Pancreas (Exocrine); Protocol for the examination of specimens from patients with carcinoma of the pancreas. Version: Pancreas Exocrine 4.0.0.1; College of American Pathologists: Chicago, IL, USA, 2017. [Google Scholar]
- Katz, M.H.; Shi, Q.; Ahmad, S.A.; Herman, J.M.; De Marsh, R.W.; Collisson, E.; Schwartz, L.; Frenkel, W.; Martin, R.; Conway, W.; et al. Preoperative modified FOLFIRINOX treatment followed by capecitabine-based chemoradiation for borderline resectable pancreatic cancer: Alliance for clinical trials in oncology trial A021101. JAMA Surg. 2016, 151, e161137. [Google Scholar] [CrossRef] [Green Version]
- Noda, Y.; Goshima, S.; Kawada, H.; Kawai, N.; Miyoshi, T.; Matsuo, M.; Bae, K.T. Modified national comprehensive cancer network criteria for assessing resectability of pancreatic ductal adenocarcinoma. AJR Am. J. Roentgenol. 2018, 210, 1252–1258. [Google Scholar] [CrossRef]
- Michels, N.A. Blood Supply and Anatomy of the Upper Abdominal Organs with a Descriptive Atlas; Lippincott: Philadelphia, PA, USA, 1955. [Google Scholar]
- Kondo, S.; Katoh, H.; Hirano, S.; Ambo, Y.; Tanaka, E.; Maeyama, Y.; Morikawa, T.; Okushiba, S. Ischemic Gastropathy After Distal Pancreatectomy with Celiac Axis Resection. Surg. Today 2004, 34, 337–340. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.D. The physiological principle of minimum work. I. The vascular system and the cost of blood volume. Proc. Natl. Acad. Sci. USA 1926, 12, 207–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamir, M. Shear forces and blood vessel radii in the cardiovascular system. J. Gen. Physiol. 1977, 69, 449–461. [Google Scholar] [CrossRef]
- Caselles, V.; Kimmel, R.; Sapiro, G. Geodesic active contours. Int. J. Comput. Vis. 1997, 22, 61–97. [Google Scholar] [CrossRef]
- Shang, Q. Separation and Segmentation of The Hepatic Vasculature in CT Images. Ph.D. Thesis, Faculty of the Graduate School of Vanderbilt University, Nashville, TN, USA, 2010; p. 113. [Google Scholar]
- Egorov, V.I.; Petrov, R.V.; Amosova, E.L.; Kharazov, A.F.; Petrov, K.S.; Yu, A.; Zhurina, E.V.; Kondratyev, P.M.; Zelter, S.O.; Dzigasov, M.V.; et al. Distal pancreatectomy with resection of the celiac trunk, right or left hepatic artery without arterial reconstruction (extended DP-CAR). Khirurgiia 2021, 10, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Mollberg, N.; Rahbari, N.N.; Koch, M.; Hartwig, W.; Hoeger, Y.; Buchler, M.W.; Weitz, J. Arterial resection during pancreatectomy for pancreatic cancer: A systematic review and meta-analysis. Ann. Surg. 2011, 254, 882–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperti, C.; Berselli, M.; Pedrazzoli, S. Distal pancreatectomy for body-tail pancreatic cancer: Is there a role for celiac axis resection? Pancreatology 2010, 10, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Cesaretti, M.; Abdel-Rehim, M.; Barbier, L.; Dokmak, S.; Hammel, P.; Sauvanet, A. Modified Appleby procedure for borderline resectable/locally advanced distal pancreatic adenocarcinoma: A major procedure for selected patients. J. Visc. Surg. 2016, 153, 173–181. [Google Scholar] [CrossRef]
- Malek, A.; Izumo, S. Physiological fluid shear stress causes downregulation of endothelin-1 mRNA in bovine aortic endothelium. Am. J. Physiol. 1992, 263, 389–396. [Google Scholar] [CrossRef]
- Langille, B.L.; Bendeck, M.P.; Keeley, F.W. Adaptations of carotid arteries of young and mature rabbits to reduced carotid blood flow. Am. J. Physiol. 1989, 256, H931–H939. [Google Scholar] [CrossRef]
- Humphrey, J.D. Vascular adaptation and mechanical homeostasis at tissue, cellular, and sub-cellular levels. Cell Biochem. Biophys. 2008, 50, 53–78. [Google Scholar] [CrossRef]
- Rosen, L.A.; Hollis, T.M.; Sharma, M.G. Alterations in bovine endothelial histidine decarboxylase activity following exposure to shear stress. Exp. Mol. Pathol. 1974, 20, 329–343. [Google Scholar] [CrossRef]
- Driss, A.B.; Benessiano, J.; Poitevin, P.; Levy, B.I.; Michael, J.-B. Arterial expansive remodeling induced by high flow rates. Am. J. Physiol. 1997, 272, H851–H858. [Google Scholar] [PubMed]
- Rudic, D.R.; Shesely, E.G.; Maeda, N.; Smithies, O.; Segal, S.S.; Sessa, W.C. Direct evidence for the importance of endothelium-derived nitric oxide in vascular remodeling. J. Clin. Investig. 1998, 101, 731–736. [Google Scholar] [CrossRef]
- Holzapfel, G.A.; Odgen, R.W. Mechanics of Biological Tissue; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Martinez-Lemus, L.A.; Hill, M.A.; Bolz, S.S.; Pohl, U.; Meininger, G.A. Acute mechanoadaptation of vascular smooth muscle cells in response to continuous arteriolar vasoconstriction: Implications for functional remodeling. FASEB J. 2004, 18, 708–710. [Google Scholar] [CrossRef]
- Gerthoffer, W.T. Actin cytoskeletal dynamics in smooth muscle contraction. Can. J. Physiol. Pharmacol. 2005, 83, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Langille, B.L.; Dajnowiec, D. Cross-linking vasomotor tone and vascular remodeling. A novel function for tissue transglutaminase. Circ. Res. 2005, 96, 9–11. [Google Scholar] [CrossRef] [Green Version]
- Yuhn, C.; Hoshina, K.; Miyahara, K.; Oshima, M. Computational simulation of flow-induced arterial remodeling of the pancreaticoduodenal arcade associated with celiac artery stenosis. J. Biomech. 2019, 92, 146–154. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | 61.6 ± 7.9 (39–74) |
| Gender (m/f) | 21/19 (53%/47%) |
| Neoadjuvant chemotherapy (yes/no) | 21/19 (53%/47%) |
| Adjuvant chemotherapy (yes/no) | 34/3 (92%/8%) |
| CCI—2/3/4/5/6 (score) | 3/10/10/15/2 (7.5%/25%/25%/37.5%/5%) |
| OP time (min.) | 301 ± 53 (195–410) |
| Estimated blood loss (ml) | 274.5 ± 113.1 (100–650) |
| PV/SMV resection (yes/no) | 15/25 (38%/62%) |
| Gastrectomy/duodenectomy | 3/1 |
| Bile duct resection | 1 |
| Tumor size (mm) | 52.75 ± 16.6 (32–110) |
| PDAC/GC/NEN/lymphoma | 34/3/2/1 (85%/7.5%/5%/2.5%) |
| Contact with CHA or/and CA > 180° (yes/no) | 40/0 (100%/0%) |
| Arterial invasion at pathology (yes/no) | 31/9 (78%/22%) |
| Venous invasion (yes/no) | 37/3 (92.5%/7.5%) |
| Perineural invasion (yes/no) | 30/10 (75%/25%) |
| R0/R1-resection | 37/3 (92.5/7.5%) |
| Number of lymph nodes removed | 33 ± 11 (20–78) |
| >Additional resection of the right or left hepatic artery | 8 (20%) |
| Lymph nodes involvement, pN0/pN1/pN2 | 9/20/11 (22.5%/50%/27.5%) |
| Complications (C–D) 0,I,II/III,IV,V | 35/5 (87.5%/12.5%) |
| POPF No/Grade A/B/C | 23/6/9/2 (57.5%/15%/22.5%/5%) |
| Diarrhea (n) | 8 (20%) |
| Length of stay (days) | 14.3 ± 6.8 (8–44) |
| Lymphorrhea (n) | 4 (10%) |
| Mortality 30-/90-days | 2/1 (5%/2.5%) 7.5% |
| Ischemic gastropathy | 5 (12.5%) |
| Postpancreatectomy hemorrhage (n) | 2 (5%) |
| Reoperation (n) | 3 (7.5%) |
| Readmission (n) | 3 (7.5%) |
| Neoadjuvant Chemotherapy (NACHT) (n) | 20 |
| Adjuvant chemotherapy (ACHT) (n) | 30 |
| CA 19-9 before neoadjuvant chemotherapy (U/mL), n18 | 464 (234;665) |
| CA 19-9 after neoadjuvant chemotherapy (U/mL), n18 | 45 (19;68) |
| CA 19.9 before surgery | 65 (22;153) |
| CA 19-9 decreasing ratio after/before NACHT, n18 | 8.9 (5.0;15.9) |
| OP time (min) | 310 ± 49 (215–410) |
| Estimated blood loss (ml) | 280 ± 104 (140–650) |
| PV/SMV resection | 14 (41%) |
| Tumor size (mm) | 49 ± 12 (21–73) |
| Tumor grade 1/2/3 | 5/23/6 (15%/68%/17%) |
| Number of lymph nodes removed | 31 ± 5 (22–43) |
| Lymph nodes involvement pN0/pN1/pN2 | 7/18/9 (20.5%/53%/26.5%) |
| Invasion: artery/vein/perineural | 34 (100%)/34 (100%)/24 (70.5%) |
| R0/R1-resection | 34/3 (91.2%/8.8%) |
| Conversion of cT4 into pT3−2 | 8 (23.5%) |
| Tumor regression after NACHT, Score 1/2/3 n20 | 1/10/9 (5%/50%/45%) |
| Factor | Overall Survival (OS) | Progression-Free Survival (PFS) |
|---|---|---|
| p-Value | p-Value | |
| Gender | 0.739 | 0.597 |
| BMI | 0.642 | 0.895 |
| Additional hepatic artery resection | 0.866 | 0.130 |
| NACHT | 0.436 | 0.078 |
| ACHT | 0.643 | 0.489 |
| PV/SMV resection | 0.289 | 0.308 |
| Perineural invasion | 0.663 | 0.007 |
| R0- status | 0.359 | 0.857 |
| CA 19–9 before surgery, >66> | 0.198 | 0.038 |
| Tumor size | 0.721 | 0.715 |
| N+/N− | 0.023 | 0.003 |
| Tumor regression grade after NACHT | 0.678 | 0.044 |
| Site | n (%) |
|---|---|
| Local | 5 (16%) |
| Peritoneum | 8 (26%) |
| Liver | 6 (19%) |
| Lung | 2 (6.5%) |
| Multiple | 2 (6.5%) |
| No | 8 (26%) |
| Indicator | Mean ± SD (min; max) | Me [q1; q3] |
|---|---|---|
| LBFV reduction on the HDL arteries, % | −2126 ± 19.34 (−66; 0) | −16 [−32,50; 7.00] |
| D1 GDA, mm | 3.73 ± 1.25 (1.82; 6.57) | 3.65 [2.70; 4.42] |
| D1 PDA, mm | 2.51 ± 0.83 (1.10; 5.76) | 2.31 [1.95; 2.91] |
| D1 PHA, mm | 3.86 ± 0.98 (2.0; 6.30) | 4.20 [2.90; 4.46] |
| D1 RGEA, mm | 2.53 ± 0.78 (1.20; 3.91) | 2.55 [1.93; 3.19] |
| D1 CHA/D1 GDA | 1.41 ± 0.53 (0.80; 3.08) | 1.26 [1.07; 1.79] |
| D1 CHA /D1 PDA | 2.11 ± 0.82 (0.83; 4.45) | 1.97 [1.38; 2.68] |
| Q2/Q1 for GDA | 2.37 ± 4.08 (0.16; 25.01) | 1.48 [0.78; 2.44] |
| Q2/Q1 for PDA | 7.33 ± 140.52 (0.91; 90.20) | 4.16 [2.17; 6.70] |
| Q2/Q1 for PHA | 1.19 ± 0.77 (0.27; 5.13) | 1.11 [0.84; 1.30] |
| Q2/Q1 for RGEA | 3.55 ± 4.0 (0.40; 18.84) | 2.35 [1.24; 3.50] |
| D2/D1 GDA | 1.11 ± 0.30 (0.63; 2.24) | 1.10 [0.94; 1.25] |
| D2/D1 PDA | 1.47 ± 0.39 (0.98; 3.08) | 1.43 [1.21; 1.61] |
| D2/D1 PHA | 1.00 ± 0.13 (0.66; 1.38) | 0,97 [0.93; 1.05] |
| D2/D1 RGEA | 1.27 ± 0.29 (0.80; 2.08) | 1.24 [1.06; 1.37] |
| ∆D GDA | 0.23 ± 0.93 (−2.30; 2.25) | 0.35 [−0.26; 0.81] |
| ∆D PDA | 0.98 ± 0.56 (−0.07; 2.29) | 0.95 [0.58; 1.44] |
| ∆D PHA | −0.01 ± 0.50 (−1.61; 1.30) | −0.11 [−0.25; 0.15] |
| ∆D RGEA | 0.55 ± 0.54 (−0.74; 1.82) | 0.50 [0.16; 0.91] |
| Blood Flow Parameters | D2/D1 GDA | D2/D1 PDA | D2/D1 PHA | D2/D1 RGEA |
|---|---|---|---|---|
| Pulse disappearance 1 | 0.87 | 0.66 | 0.80 | 1.00 |
| LBFV reduction 2, % | 0.09 | −0.11 | 0.14 | −0.06 |
| D2/D1 GDA | D2/D1 PDA | D2/D1 PHA | D1 CHA/ D1 GDA | D1 CHA/ D1 PDA | |
|---|---|---|---|---|---|
| D2/D1 PDA | −0.16 | ||||
| D2/D1 PHA | 0.15 | −0.11 | |||
| D2/D1 RGEA | −0.07 | 0.11 | 0.40 * | ||
| D1 CHA/ D1 GDA | 0.53 ** | −0.09 | 0.07 | −0.07 | |
| D1 CHA/ D1 PDA | −0.09 | 0.64 ** | 0.13 | −0.02 | 0.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Egorov, V.; Kim, P.; Kharazov, A.; Dzigasov, S.; Popov, P.; Rykova, S.; Zelter, P.; Demidova, A.; Kondratiev, E.; Grigorievsky, M.; et al. Hemodynamic, Surgical and Oncological Outcomes of 40 Distal Pancreatectomies with Celiac and Left Gastric Arteries Resection (DP CAR) without Arterial Reconstructions and Preoperative Embolization. Cancers 2022, 14, 1254. https://doi.org/10.3390/cancers14051254
Egorov V, Kim P, Kharazov A, Dzigasov S, Popov P, Rykova S, Zelter P, Demidova A, Kondratiev E, Grigorievsky M, et al. Hemodynamic, Surgical and Oncological Outcomes of 40 Distal Pancreatectomies with Celiac and Left Gastric Arteries Resection (DP CAR) without Arterial Reconstructions and Preoperative Embolization. Cancers. 2022; 14(5):1254. https://doi.org/10.3390/cancers14051254
Chicago/Turabian StyleEgorov, Viacheslav, Pavel Kim, Alexander Kharazov, Soslan Dzigasov, Pavel Popov, Sofia Rykova, Pavel Zelter, Anna Demidova, Eugeny Kondratiev, Maxim Grigorievsky, and et al. 2022. "Hemodynamic, Surgical and Oncological Outcomes of 40 Distal Pancreatectomies with Celiac and Left Gastric Arteries Resection (DP CAR) without Arterial Reconstructions and Preoperative Embolization" Cancers 14, no. 5: 1254. https://doi.org/10.3390/cancers14051254
APA StyleEgorov, V., Kim, P., Kharazov, A., Dzigasov, S., Popov, P., Rykova, S., Zelter, P., Demidova, A., Kondratiev, E., Grigorievsky, M., & Sorokin, A. (2022). Hemodynamic, Surgical and Oncological Outcomes of 40 Distal Pancreatectomies with Celiac and Left Gastric Arteries Resection (DP CAR) without Arterial Reconstructions and Preoperative Embolization. Cancers, 14(5), 1254. https://doi.org/10.3390/cancers14051254