
Microwave Ablation for Colorectal Liver Metastases: A Systematic Review and Pooled Oncological Analyses

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Outcomes of Interest
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
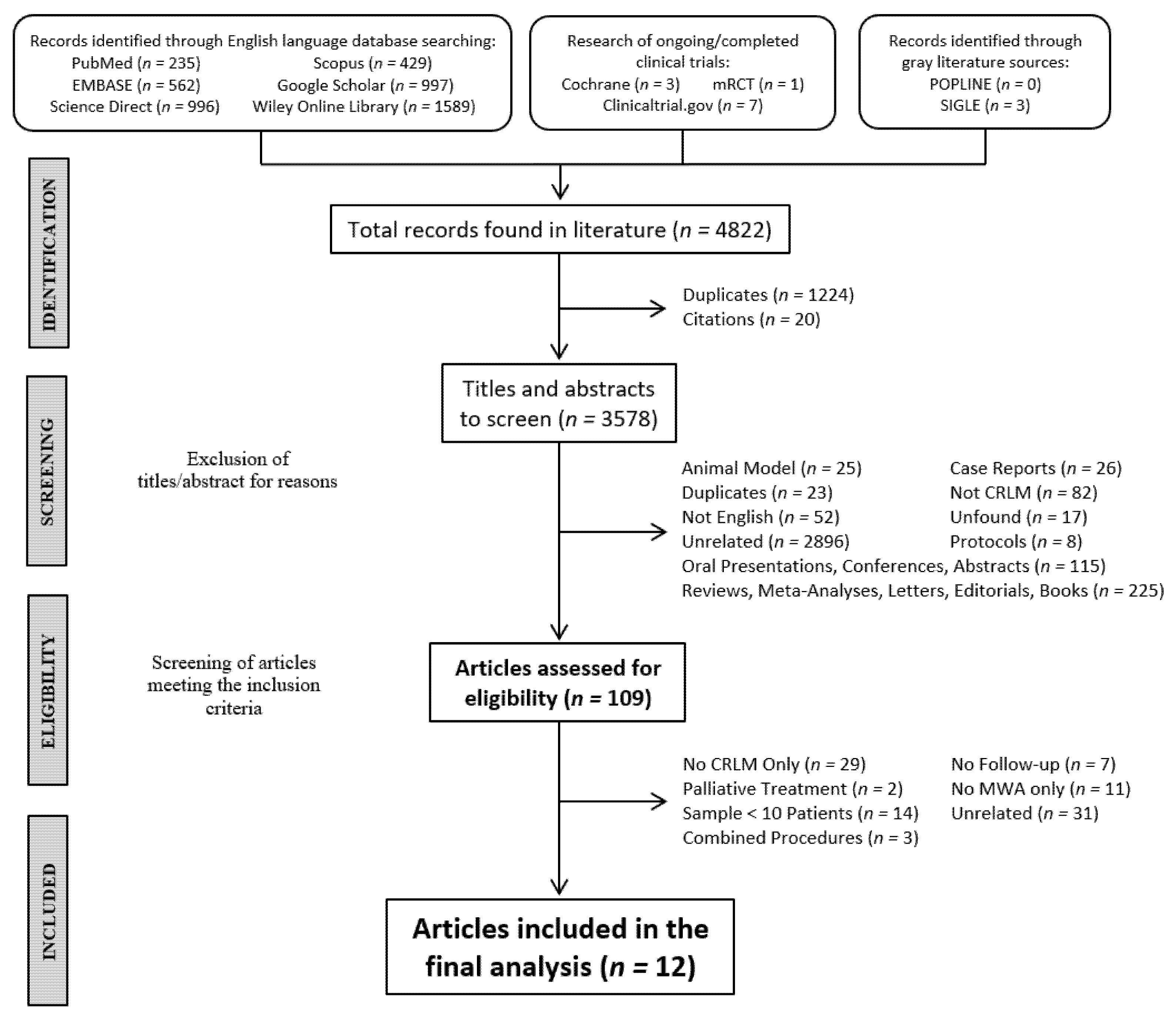
3.1. Literature Analysis
3.2. Study Characteristics
3.3. Subgroup Analysis
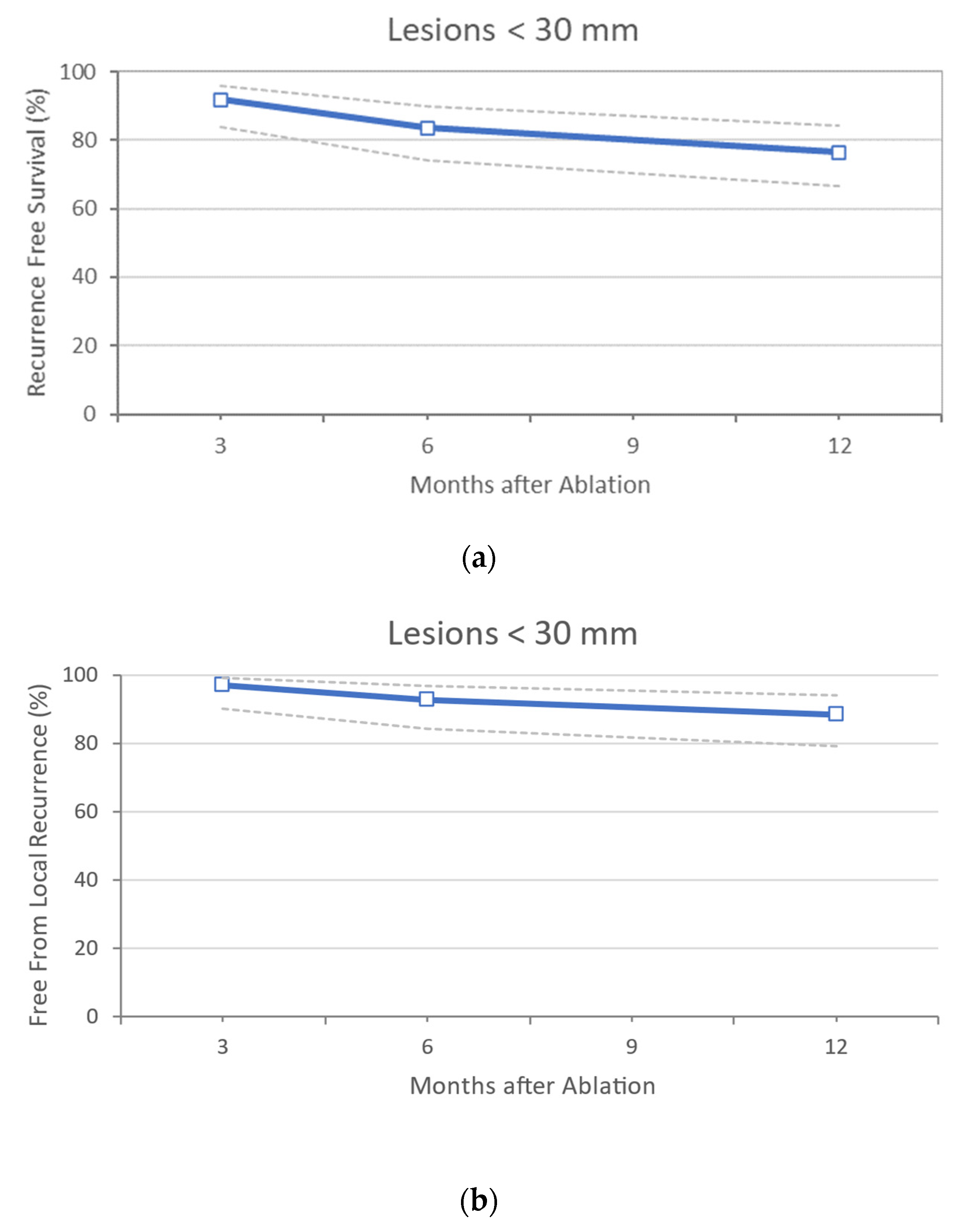
CRLM with a Diameter of ≤30 mm
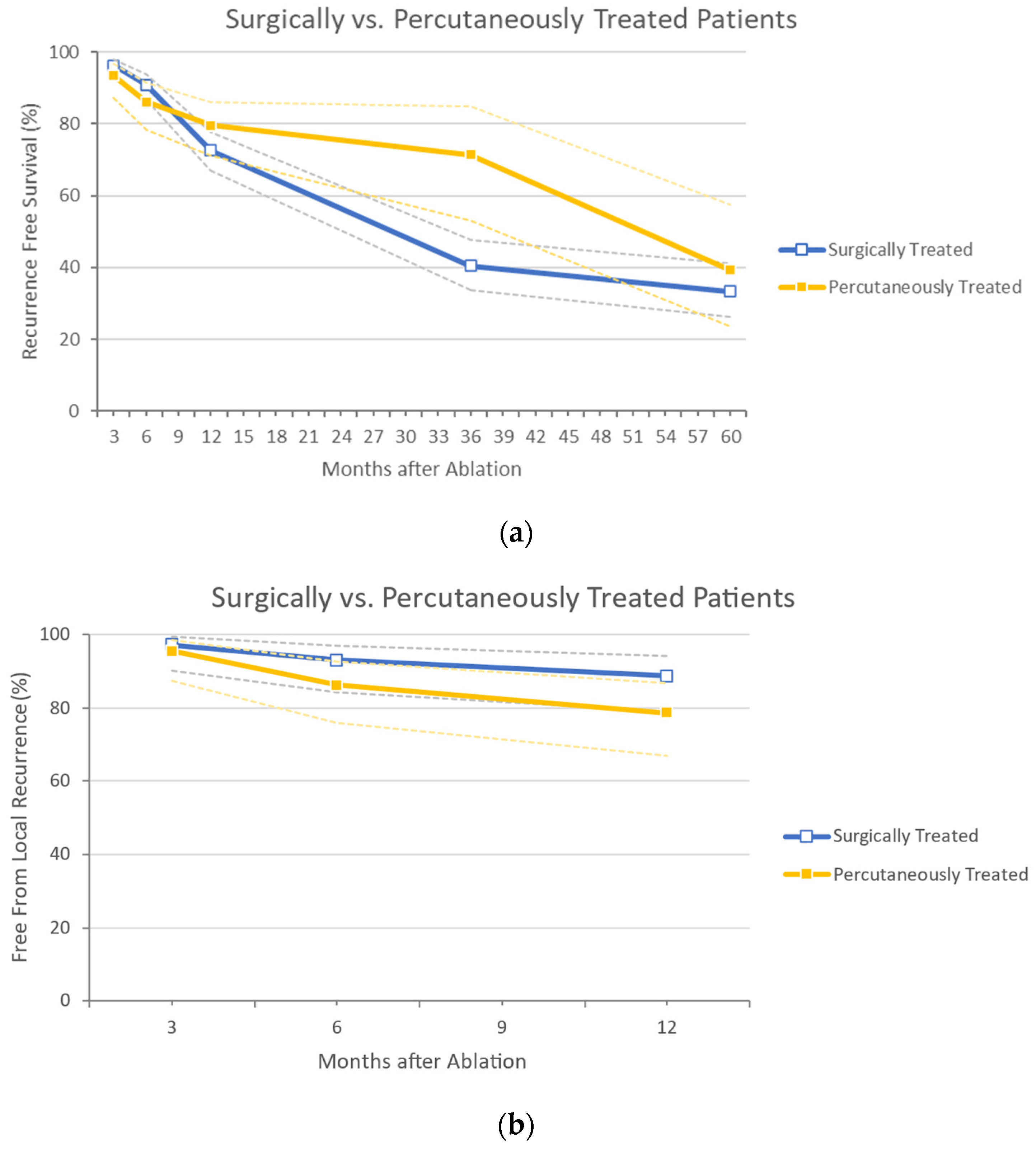
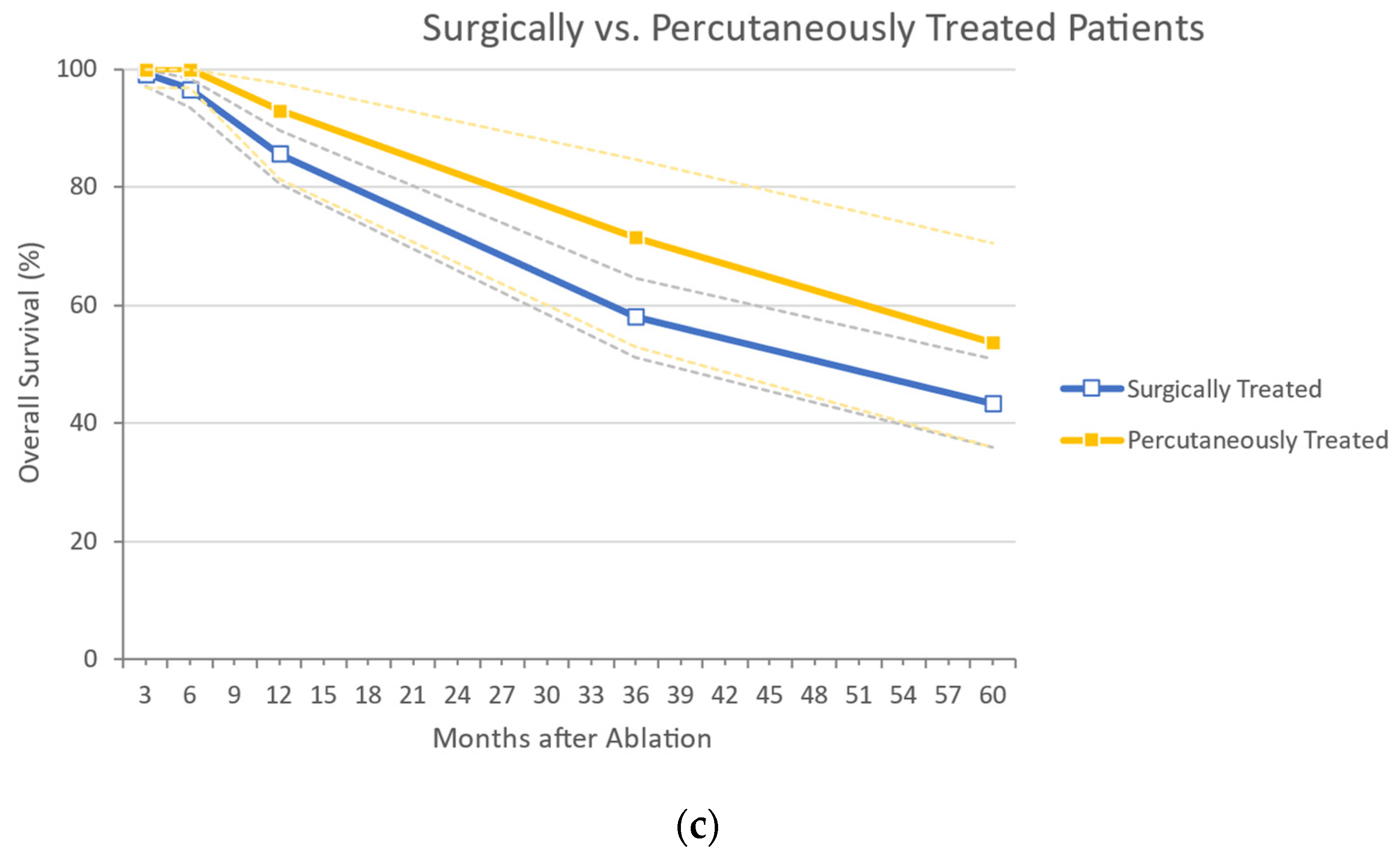
Surgical vs. Percutaneous MWA
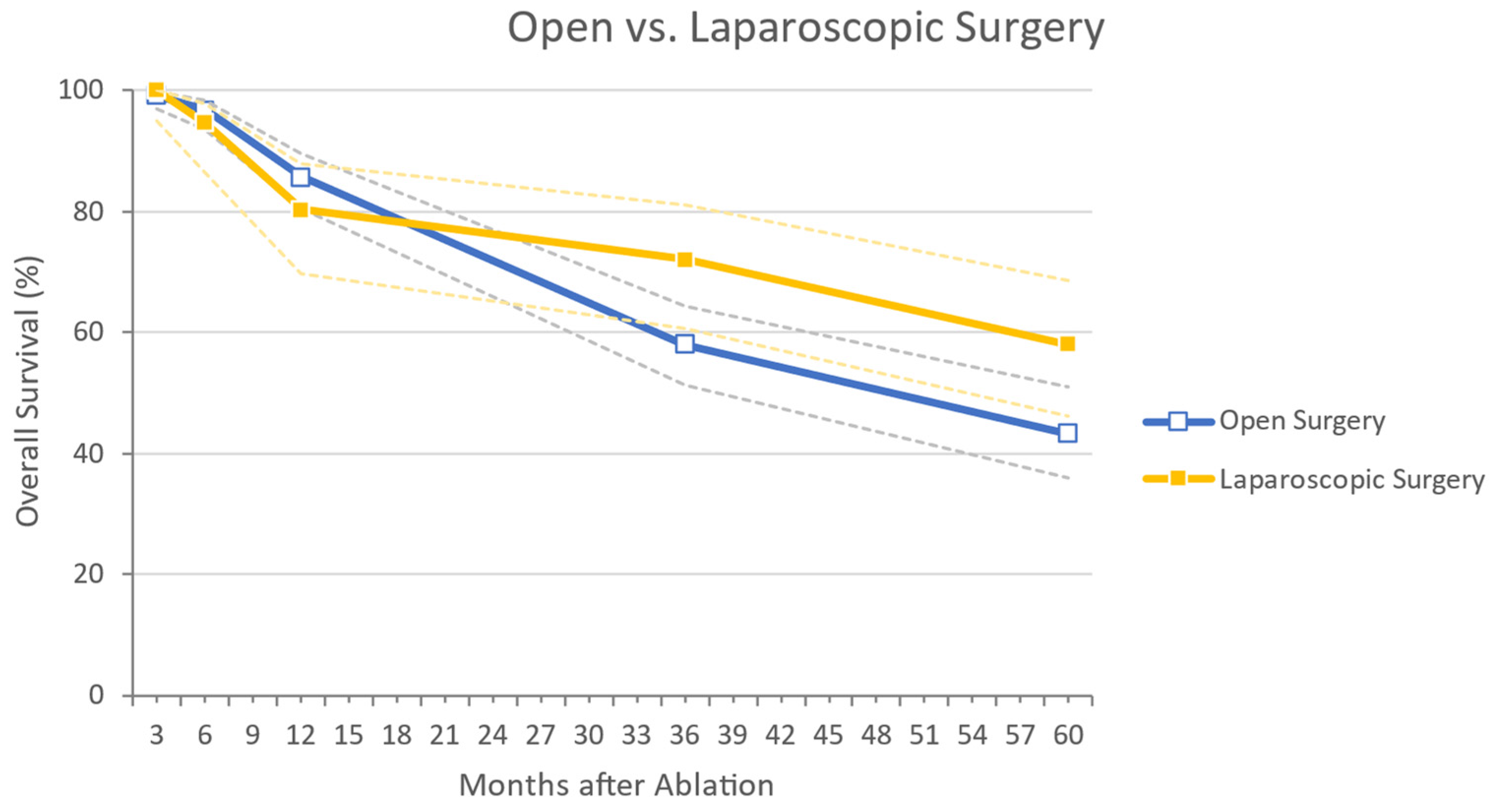
Surgical MWA: Open vs. Laparoscopic Approach
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Elferink, M.A.; de Jong, K.P.; Klaase, J.M.; Siemerink, E.J.; de Wilt, J.H. Metachronous metastases from colorectal cancer: A population-based study in North-East Netherlands. Int. J. Colorectal Dis. 2015, 30, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Engstrand, J.; Nilsson, H.; Stromberg, C.; Jonas, E.; Freedman, J. Colorectal cancer liver metastases—A population-based study on incidence, management and survival. BMC Cancer 2018, 18, 78. [Google Scholar] [CrossRef] [PubMed]
- Morris, E.J.; Forman, D.; Thomas, J.D.; Quirke, P.; Taylor, E.F.; Fairley, L.; Cottier, B.; Poston, G. Surgical management and outcomes of colorectal cancer liver metastases. Br. J. Surg. 2010, 97, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Hackl, C.; Neumann, P.; Gerken, M.; Loss, M.; Klinkhammer-Schalke, M.; Schlitt, H.J. Treatment of colorectal liver metastases in Germany: A ten-year population-based analysis of 5772 cases of primary colorectal adenocarcinoma. BMC Cancer 2014, 14, 810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, R.M. Therapy for metastatic colorectal cancer. Oncologist 2006, 11, 981–987. [Google Scholar] [CrossRef] [Green Version]
- Gillams, A.; Khan, Z.; Osborn, P.; Lees, W. Survival after radiofrequency ablation in 122 patients with inoperable colorectal lung metastases. Cardiovasc. Intervent. Radiol. 2013, 36, 724–730. [Google Scholar] [CrossRef]
- Tanaka, K.; Shimada, H.; Matsumoto, C.; Matsuo, K.; Takeda, K.; Nagano, Y.; Togo, S. Impact of the degree of liver resection on survival for patients with multiple liver metastases from colorectal cancer. World J. Surg. 2008, 32, 2057–2069. [Google Scholar] [CrossRef]
- Kingham, T.P.; Tanoue, M.; Eaton, A.; Rocha, F.G.; Do, R.; Allen, P.; De Matteo, R.P.; D’Angelica, M.; Fong, Y.; Jarnagin, W.R. Patterns of recurrence after ablation of colorectal cancer liver metastases. Ann. Surg. Oncol. 2012, 19, 834–841. [Google Scholar] [CrossRef]
- White, R.R.; Avital, I.; Sofocleous, C.T.; Brown, K.T.; Brody, L.A.; Covey, A.; Getrajdman, G.I.; Jarnagin, W.R.; Dematteo, R.P.; Fong, Y. Rates and patterns of recurrence for percutaneous radiofrequency ablation and open wedge resection for solitary colorectal liver metastasis. J. Gastrointest. Surg. 2007, 11, 256–263. [Google Scholar] [CrossRef]
- Otto, G.; Duber, C.; Hoppe-Lotichius, M.; Konig, J.; Heise, M.; Pitton, M.B. Radiofrequency ablation as first-line treatment in patients with early colorectal liver metastases amenable to surgery. Ann. Surg. 2010, 251, 796–803. [Google Scholar] [CrossRef]
- Adam, R.; Hagopian, E.J.; Linhares, M.; Krissat, J.; Savier, E.; Azoulay, D.; Kunstlinger, F.; Castaing, D.; Bismuth, H. A comparison of percutaneous cryosurgery and percutaneous radiofrequency for unresectable hepatic malignancies. Arch. Surg. 2002, 137, 1332–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillams, A.R.; Lees, W.R. Five-year survival in 309 patients with colorectal liver metastases treated with radiofrequency ablation. Eur. Radiol. 2009, 19, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Solbiati, L.; Ahmed, M.; Cova, L.; Ierace, T.; Brioschi, M.; Goldberg, S.N. Small liver colorectal metastases treated with percutaneous radiofrequency ablation: Local response rate and long-term survival with up to 10-year follow-up. Radiology 2012, 265, 958–968. [Google Scholar] [CrossRef] [PubMed]
- Van Tilborg, A.A.; Meijerink, M.R.; Sietses, C.; Van Waesberghe, J.H.; Mackintosh, M.O.; Meijer, S.; Van Kuijk, C.; Van Den Tol, P. Long-term results of radiofrequency ablation for unresectable colorectal liver metastases: A potentially curative intervention. Br. J. Radiol. 2011, 84, 556–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, J.; Liang, P.; Yu, X.; Liu, F.; Chen, L.; Wang, Y. A comparison of microwave ablation and bipolar radiofrequency ablation both with an internally cooled probe: Results in ex vivo and in vivo porcine livers. Eur. J. Radiol. 2011, 79, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Gravante, G.; Ong, S.L.; Metcalfe, M.S.; Strickland, A.; Dennison, A.R.; Lloyd, D.M. Hepatic microwave ablation: A review of the histological changes following thermal damage. Liver Int. 2008, 28, 911–921. [Google Scholar] [CrossRef]
- Wright, A.S.; Sampson, L.A.; Warner, T.F.; Mahvi, D.M.; Lee, F.T., Jr. Radiofrequency versus microwave ablation in a hepatic porcine model. Radiology 2005, 236, 132–139. [Google Scholar] [CrossRef]
- Dupuy, D.E. Microwave ablation compared with radiofrequency ablation in lung tissue-is microwave not just for popcorn anymore? Radiology 2009, 251, 617–618. [Google Scholar] [CrossRef] [Green Version]
- Simon, C.J.; Dupuy, D.E.; Mayo-Smith, W.W. Microwave ablation: Principles and applications. Radiographics 2005, 25 (Suppl. 1), S69–S83. [Google Scholar] [CrossRef]
- Rhaiem, R.; Kianmanesh, R.; Minon, M.; Tashkandi, A.; Aghaei, A.; Ledoux, G.; Hoeffel, C.; Bouche, O.; Sommacale, D.; Piardi, T. Microwave Thermoablation of Colorectal Liver Metastases Close to Large Hepatic Vessels Under Pringle Maneuver Minimizes the “Heat Sink Effect”. World J. Surg. 2020, 44, 1595–1603. [Google Scholar] [CrossRef]
- de Baere, T.; Deschamps, F.; Briggs, P.; Dromain, C.; Boige, V.; Hechelhammer, L.; Abdel-Rehim, M.; Auperin, A.; Goere, D.; Elias, D. Hepatic malignancies: Percutaneous radiofrequency ablation during percutaneous portal or hepatic vein occlusion. Radiology 2008, 248, 1056–1066. [Google Scholar] [CrossRef] [PubMed]
- Tombesi, P.; Di Vece, F.; Sartori, S. Radiofrequency, microwave, and laser ablation of liver tumors: Time to move toward a tailored ablation technique? Hepatoma Res. 2015, 1, 52–57. [Google Scholar]
- Correa-Gallego, C.; Fong, Y.; Gonen, M.; D’Angelica, M.I.; Allen, P.J.; DeMatteo, R.P.; Jarnagin, W.R.; Kingham, T.P. A retrospective comparison of microwave ablation vs. radiofrequency ablation for colorectal cancer hepatic metastases. Ann. Surg. Oncol. 2014, 21, 4278–4283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. PRISMA-S: An extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibanes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 3 May 2020).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Eng, O.S.; Tsang, A.T.; Moore, D.; Chen, C.; Narayanan, S.; Gannon, C.J.; August, D.A.; Carpizo, D.R.; Melstrom, L.G. Outcomes of microwave ablation for colorectal cancer liver metastases: A single center experience. J. Surg. Oncol. 2015, 111, 410–413. [Google Scholar] [CrossRef] [Green Version]
- Engstrand, J.; Nilsson, H.; Jansson, A.; Isaksson, B.; Freedman, J.; Lundell, L.; Jonas, E. A multiple microwave ablation strategy in patients with initially unresectable colorectal cancer liver metastases—A safety and feasibility study of a new concept. Eur. J. Surg. Oncol. 2014, 40, 1488–1493. [Google Scholar] [CrossRef]
- Ierardi, A.M.; Floridi, C.; Fontana, F.; Chini, C.; Giorlando, F.; Piacentino, F.; Brunese, L.; Pinotti, G.; Bacuzzi, A.; Carrafiello, G. Microwave ablation of liver metastases to overcome the limitations of radiofrequency ablation. Radiol. Med. 2013, 118, 949–961. [Google Scholar] [CrossRef]
- McEachron, K.R.; Ankeny, J.S.; Robbins, A.; Altman, A.M.; Marmor, S.; D’Souza, D.; Schat, R.; Spilseth, B.; Jensen, E.H. Surgical microwave ablation of otherwise non-resectable colorectal cancer liver metastases: Expanding opportunities for long term survival. Surg. Oncol. 2021, 36, 61–64. [Google Scholar] [CrossRef]
- Seki, T.; Wakabayashi, M.; Nakagawa, T.; Imamura, M.; Tamai, T.; Nishimura, A.; Yamashiki, N.; Inoue, K. Percutaneous microwave coagulation therapy for solitary metastatic liver tumors from colorectal cancer: A pilot clinical study. Am. J. Gastroenterol. 1999, 94, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Shady, W.; Petre, E.N.; Do, K.G.; Gonen, M.; Yarmohammadi, H.; Brown, K.T.; Kemeny, N.E.; D’Angelica, M.; Kingham, P.T.; Solomon, S.B.; et al. Percutaneous Microwave versus Radiofrequency Ablation of Colorectal Liver Metastases: Ablation with Clear Margins (A0) Provides the Best Local Tumor Control. J. Vasc. Interv. Radiol. 2018, 29, 268–275.e261. [Google Scholar] [CrossRef] [PubMed]
- Shibata, T.; Niinobu, T.; Ogata, N.; Takami, M. Microwave coagulation therapy for multiple hepatic metastases from colorectal carcinoma. Cancer 2000, 89, 276–284. [Google Scholar] [CrossRef]
- Song, P.; Sheng, L.; Sun, Y.; An, Y.; Guo, Y.; Zhang, Y. The clinical utility and outcomes of microwave ablation for colorectal cancer liver metastases. Oncotarget. 2017, 8, 51792–51799. [Google Scholar] [CrossRef] [Green Version]
- Stattner, S.; Jones, R.P.; Yip, V.S.; Buchanan, K.; Poston, G.J.; Malik, H.Z.; Fenwick, S.W. Microwave ablation with or without resection for colorectal liver metastases. Eur. J. Surg. Oncol. 2013, 39, 844–849. [Google Scholar] [CrossRef]
- Takahashi, H.; Kahramangil, B.; Kose, E.; Berber, E. A comparison of microwave thermosphere versus radiofrequency thermal ablation in the treatment of colorectal liver metastases. HPB 2018, 20, 1157–1162. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.; Li, Y. A comparative study of laparoscopic microwave ablation with laparoscopic radiofrequency ablation for colorectal liver metastasis. J. BUON 2017, 22, 667–672. [Google Scholar]
- Evrard, S.; Torzilli, G.; Caballero, C.; Bonhomme, B. Parenchymal sparing surgery brings treatment of colorectal liver metastases into the precision medicine era. Eur. J. Cancer 2018, 104, 195–200. [Google Scholar] [CrossRef]
- Moris, D.; Ronnekleiv-Kelly, S.; Rahnemai-Azar, A.A.; Felekouras, E.; Dillhoff, M.; Schmidt, C.; Pawlik, T.M. Parenchymal-Sparing Versus Anatomic Liver Resection for Colorectal Liver Metastases: A Systematic Review. J. Gastrointest. Surg. 2017, 21, 1076–1085. [Google Scholar] [CrossRef]
- Meijerink, M.R.; Puijk, R.S.; van Tilborg, A.; Henningsen, K.H.; Fernandez, L.G.; Neyt, M.; Heymans, J.; Frankema, J.S.; de Jong, K.P.; Richel, D.J.; et al. Radiofrequency and Microwave Ablation Compared to Systemic Chemotherapy and to Partial Hepatectomy in the Treatment of Colorectal Liver Metastases: A Systematic Review and Meta-Analysis. Cardiovasc. Intervent. Radiol. 2018, 41, 1189–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, H.; Berber, E. Role of thermal ablation in the management of colorectal liver metastasis. Hepatobiliary Surg. Nutr. 2020, 9, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Tabuse, K. A new operative procedure of hepatic surgery using a microwave tissue coagulator. Nihon Geka Hokan 1979, 48, 160–172. [Google Scholar] [PubMed]
- Zhao, Q.; Cheng, Z.; Han, Z.; Liu, F.; Yu, X.; Tan, X.; Han, B.; Dou, J.; Yu, J.; Liang, P. Percutaneous Microwave Ablation Versus Open Surgical Resection for Colorectal Cancer Liver Metastasis. Front. Oncol. 2021, 11, 638165. [Google Scholar] [CrossRef]
- Kim, S.K.; Rhim, H.; Kim, Y.S.; Koh, B.H.; Cho, O.K.; Seo, H.S.; Kim, Y. Radiofrequency thermal ablation of hepatic tumors: Pitfalls and challenges. Abdom Imaging 2005, 30, 727–733. [Google Scholar] [CrossRef]
- van Duijnhoven, F.H.; Jansen, M.C.; Junggeburt, J.M.; van Hillegersberg, R.; Rijken, A.M.; van Coevorden, F.; van der Sijp, J.R.; van Gulik, T.M.; Slooter, G.D.; Klaase, J.M.; et al. Factors influencing the local failure rate of radiofrequency ablation of colorectal liver metastases. Ann. Surg. Oncol. 2006, 13, 651–658. [Google Scholar] [CrossRef]
- Tinguely, P.; Dal, G.; Bottai, M.; Nilsson, H.; Freedman, J.; Engstrand, J. Microwave ablation versus resection for colorectal cancer liver metastases—A propensity score analysis from a population-based nationwide registry. Eur. J. Surg. Oncol. 2020, 46, 476–485. [Google Scholar] [CrossRef]
- Di Martino, M.; Rompianesi, G.; Mora-Guzman, I.; Martin-Perez, E.; Montalti, R.; Troisi, R.I. Systematic review and meta-analysis of local ablative therapies for resectable colorectal liver metastases. Eur. J. Surg. Oncol. 2020, 46, 772–781. [Google Scholar] [CrossRef]
- Della Corte, A.; Ratti, F.; Monfardini, L.; Marra, P.; Gusmini, S.; Salvioni, M.; Venturini, M.; Cipriani, F.; Aldrighetti, L.; De Cobelli, F. Comparison between percutaneous and laparoscopic microwave ablation of hepatocellular carcinoma. Int. J. Hyperthermia 2020, 37, 542–548. [Google Scholar] [CrossRef]
- Yun, D.; Kim, S.; Song, I.; Chun, K. Comparative analysis of Laparoscopic versus open surgical radiofrequency ablation for malignant liver tumors. Korean J. Hepatobiliary Pancreat. Surg. 2014, 18, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Puijk, R.S.; Ruarus, A.H.; Vroomen, L.; van Tilborg, A.; Scheffer, H.J.; Nielsen, K.; de Jong, M.C.; de Vries, J.J.J.; Zonderhuis, B.M.; Eker, H.H.; et al. Colorectal liver metastases: Surgery versus thermal ablation (COLLISION)—A phase III single-blind prospective randomized controlled trial. BMC Cancer 2018, 18, 821. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| MWA only | Combined procedures (i.e., RFA) |
| MWA + resections of other liver portions | MWA and subsequent resection of the same target |
| CRLM (+ mixed studies with identifiable results for CRLM only) | No adenocarcinoma CRLM |
| No lesions’ dimensional limits | Palliative treatment |
| Patients aged above 18 years old | Pregnant women |
| Sample > 10 Patients | Case reports and sample < 10 patients |
| Regardless neoadjuvant CT | |
| Recurrences | |
| Treated surgically and percutaneously |
| Study ID | Year | Country | Study Type | Rand. | Study Design | Period | N-O QAS | Sample Size, n | CRLM Patients, n | MWA-Treated Patients, n | Ablations, n | Age, Mean ° (SD °) | Sex M/F |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| McEachron | 2021 | USA | Retrospective | No | Cohort | 2009–2018 | Fair | 36 | 36 | 36 | 40 ** | 52 (±12.75) | 21/15 |
| Rhaiem | 2020 | France | Prospective | No | Cohort | November 2017– December 2018 | Poor | 19 | 19 | 19 | 23 | 67 (±10.5) | 8/11 |
| Takahashi | 2018 | USA | Retrospective | No | Case–Control | 2014–2018 | Good | 105 | 105 | 51 | 121 | NA | 33/18 |
| Shady | 2017 | USA | Retrospective | No | Case–Control | November 2019– April 2015 | Good | 110 | 110 | 48 | 72 | NA | 35/13 |
| Yang | 2017 | China | Retrospective | No | Case–Control | January 2010– January 2016 | Fair | 179 | 179 | 71 | 121 | 51 (±5.33) | 49/22 |
| Song | 2016 | China | Retrospective | No | Case–Control | January 2012– January 2014 | Good | 62 | 62 | 28 | NA | NA | 15/13 |
| Eng | 2015 | USA | Retrospective | No | Cohort | January 2009– April 2013 | Poor | 33 | 33 | 33 | 49 | 61 (±11.75) | 24/9 |
| Engstrand | 2014 | Sweden | Retrospective | No | Case–Control | October 2009– September 2012 | Fair | 81 | 81 | 20 | 7 * (4–22 *) | 63.5 (±9.5) | 9/11 |
| Ierardi | 2013 | Italy | Prospective | No | Case–Control | May 2008– September 2011 | Poor | 25 | 17 | 17 | 23 | 65.75 (±7.75) | 13/4 |
| Stattner | 2013 | UK | Retrospective | No | Cohort | May 2005– December 2012 | Good | 43 | 43 | 43 | 95 | 64.5 (±11) | 32/11 |
| Shibata | 2000 | Japan | Prospective | Yes | Case–Control | December 1990– August 1887 | Good | 30 | 30 | 14 | 58 | 61.5 (±11.26) | 8/6 |
| Seki | 1999 | Japan | Prospective | No | Cohort | January 1994– May 1997 | Poor | 15 | 15 | 15 | 32 | 66 (±5.76) | 10/5 |
| Total | - | - | - | - | - | - | 741 | 730 | 395 | - | 58.92 (±9.19) | 257/138 |
| Study ID | MWA-Treated Patients/ Lesions, n | Dimensions, Mean (SD), mm | Lesions < 30 mm, n (%) | Percutaneous/ Surgical Treatment, pt n (%) | Surgical Open/Lap, pt n (%) | Single/Multiple Lesions, pt n (%) | Synch, pt n (%)/ Meta, pt n (%) | Neoadj, n (%)/ Adj, n (%) Treatment |
|---|---|---|---|---|---|---|---|---|
| McEachron 2021 | 36/135 | 19 ° (±19.5 °) | 132 (97.8%) | 0/ 36 (100%) | 13 * (32.5% *)/ 27 * (67.5% *) | NA/NA | 13 (36.1%)/NA | 36 (100%)/NA |
| Rhaiem 2020 | 19/23 | 15.25 ° (±2.75°) | 23 (100%) | 0/ 19 (100%) | 15 (78.9%)/ 4 (21.1%) | 15 (78.9%)/ 4 (21.1%) | 8 (42.1%)/ 11 (57.9%) | 17 (89%)/ 19 (100%) |
| Takahashi 2018 | 51/121 | 21.25 ° (±2.83 °) | 121 (100%) | 0/ 51 (100%) | 0/ 51 (100%) | 0/ 51 (100%) | NA/NA | 28 (54.9%)/NA |
| Shady 2017 | 48/60 | 17 ° (±7.5 °) | 56 (93.3%) | 48 (100%)/ 0 | 0/0 | 40 (83.3%)/ 8 (17.7%) | NA/NA | NA/NA |
| Yang 2017 | 71/121 | 3 ° (±0.67°) | NA | 0/ 71 (100%) | 0/ 71 (100%) | 33 (46.5%)/ 38 (53.5%) | NA/NA | NA/NA |
| Song 2016 | 28/NA | NA | NA | 28 (100%)/ 0 | 0/0 | 18 (64.3%)/ 10 (35.7%) | 10 (35.7%)/ 18 (64.3%) | NA/NA |
| Eng 2015 | 33/49 | NA | 42 (85.7%) | 0/ 33 (100%) | NA/NA | NA/NA | NA/NA | 32 (96.9%)/ 30 (90.9%) |
| Engstrand 2014 | 20/NA | NA | NA | 0/ 20 (100%) | 20 (100%)/ 0 | 0/ 20 (100%) | 18 (90%)/ 2 (10%) | 9 (45%)/ 13 (65%) |
| Ierardi 2013 | 17/23 | 34.52 ° (±13.25 °) | 1 (4.8%) | 17 (100%)/ 0 | 0/0 | 14 (82.4%)/ 3 (17.6%) | NA/NA | NA/17 (100%) |
| Stattner 2013 | 43/95 | 20.25 ° (±5.83 °) | NA | 0/ 43 (100%) | 43 (100%)/ 0 | NA/NA | 27 (62.8%)/ 16 (37.2%) | 31 (72.1%)/NA |
| Shibata 2000 | 14/58 | 27 ° (±11 °) | NA | 0/ 14 (100%) | 14 (100%)/ 0 | 0/ 14 (100%) | NA/NA | NA/NA |
| Seki 1999 | 15/15 | 21.4 ° (±3.73 °) | 15 (100%) | 15 (100%)/ 0 | 0/0 | 15 (100%)/ 0 | 0/ 15 (100%) | 0/ 15 (100%) |
| Total | 395/700 | 17.62 ° (±7.87 °) | 390 (91.6%) {88.5–93.8%} | 108 (32.3%)/ 287 (85.9%) {27.5–37.5%}/ {81.8–89.2%} | 92 (34.7%)/ 126 (47.5%) {29.2–40.6%}/ {41.6–53.5%} | 135 (47.7%)/ 148 (52.3%) {41.9–53.5%}/ {46.5–58.1%} | 76 (47.2%)/ 62 (49.6%) {39.7–54.9%}/ {40.9–58.3%} | 153 (70.5%)/ 94 (90.4%) {64.1–76.2%}/ {83.2–94.7%} |
| Study ID | Type of MWA Device | Type of MWA Needle | Ablation(s) Per Lesion | Average Ablation Time, min | Average Energy | Operation Time, min | Complica-tions n (%) | Complications Type, pt n | Clavien–Dindo ≥ 3, n (%) | Length of Stay, Days (Range) |
|---|---|---|---|---|---|---|---|---|---|---|
| McEachron 2021 | NeuWaveTM Microwave Ablation System, Ethicon, Madison, WI, USA | Certus 140, 2.45 GHz ablation system, Certus PR XT (20 cm), or LK Max XT 25 cm probes (single, double or three probes: lesion cutoff 1.5–2.5 cm) | Single | NA | NA | NA | 8 (22.2%) | Post-operative pain (3), tumor lysis syndrome (1) | 1 (2.8%) | 2.5 (0–28) |
| Rhaiem 2020 | EmPrintTM Ablation System, Medtronic, Dublin, Ireland | 2.45 GHz, 14 G probes with ThermosphereTM Technology | Single and multiple | 5 | 75 W § | NA | 6 (31.6%) | Evisceration (1), biliary fistula (1), peritonitis due to anastomotic leakage (1), heparin-induced thrombocytopenia (1), surgical site infection (1), MHV thrombosis (1) | 0 | NA |
| Takahashi 2018 | EmPrintTM Ablation System, Covidien, Boulder, CO, USA | 2.45 GHz, 14 Gauge antenna | NA | 2.5–15 | 100 W | 154 (±3 *) | 7(13.7%) | NA | NA | (1–4) |
| Shady 2017 | NeuWaveTM Microwave Ablation System; HS AMICATM; Microsulis (Angiodynamics, New York, NY, USA); and EmPrintTM Ablation System | NA | NA | NA | NA | NA | 19 (39.6%) | PNX (11), hepatic artery- portal venous fistula (1), bowel perforation (1), bilomas (2), left portal vein thrombosis (1), sub-scapular hematoma (1), subcutaneous emphysema (1), pleural effusion (1) | 6 (12.5%) | NA |
| Yang 2017 | NA | NA | Single | 70 (total) | NA | NA | 9 (12.7%) | Perihepatic fluid collection (3), ascites (3), UTI (2), pleural effusion (1) | 0 | 7 (5–19) |
| Song 2016 | KY-2000 Microwave Ablation System (Kangyou Medical, Nanjing, Jiangsu, China) | 2450 MHz antennae of three types (0.5, 0.7 and 1.1 cm tips Ø) | NA | NA | NA | NA | 3 (10.7%) | Pain (3) | 2 (7.1%) | 5.9 (±0.9 *) |
| Eng 2015 | ValleyLabTM Microwave Ablation Generator System, Covidien, Boulder, CO, USA | NA | NA | NA | NA | NA | 18 (54.5%) | Intra-abdominal abscess drained radiologically (4), respiratory distress (3), biliary fistula (1) | 8 (24.2%) | 6 (1–32) |
| Engstrand 2014 | Acculis® Microwave Tissue Ablation System, Angiodynamics, Latham, NY, USA | NA | NA | NA | NA | 235 (112–475) | 12 (60%) | Multiple liver abscesses drained percutaneously (1), pleural effusion drained percutaneously (1), severe respiratory distress (3) | 5 (25%) | 10 (2–24) |
| Ierardi 2013 | EvidentTM Microwave Ablation System, Covidien, USA | Straight 14.5-gauge antennas (12–17 cm of length), saline-perfused coaxial cable. Lesions of 3–4 cm Ø were treated with two antennas. Lesions of >4 cm Ø were treated with three antennas | Single | 10 | 45 W | NA | 4 (23.5%) | Abscess drained (1), pain (3), ascites (1) | 1 (5.9%) | NA |
| Stattner 2013 | Acculis® Microwave Tissue Ablation System (Microsulis Medical Ltd., Dublin, UK) | 2.65 GHz, shaft-cooled Accu2i pMTA antenna | NA | 1.5 | 100 W | NA | 15 (34.9%) | Re-intervention (3), death (1) | 4 (9.3%) | 7 (4–80) |
| Shibata 2000 | Microwave tissue coagulator HSD-20M (Azwell, Osaka, Japan) | For coagulation of superficial tumors: 2-cm-long electrode (0.7 mm Ø; TM-20; Azwell). For deep tumors: 20-cm-long electrode (1.6 mm Ø; TMD- 16CBL; Azwell) | NA | 2–20 | 60– 100 W | 180 (±20 *) | 2 (14.3%) | Hepatic abscess (1), bile duct fistula (1) | 2 (14.3%) | NA |
| Seki 1999 | Microtaze OT-110 M, Nippon Shoji, Azwell Inc., Osaka, Japan | MW electrode of 2.0 mm Ø, 25 cm length (MD-20 CDL- 10/25) | Multiple | 1 | 80 W | NA | 1 (6.7%) | Pleural effusion (1) | 0 | 4 |
| Total | - | - | - | - | - | 184.16 ° (±26.45°) | 104 (26.3%) {22.2–30.9%} | - | 29 (8.4%) {5.9– 11.8%} | 5.43 (NA) |
| Study ID | Follow-Up Mean° (SD°), Months | 3 Months RF | 6 Months RF | 1 Year RF | 3 Years RF | 5 Years RF | Total RF | 3 Months FFLR | 6 Months FFLR | 1 Year FFLR |
|---|---|---|---|---|---|---|---|---|---|---|
| McEachron 2021 | NA | 100% | 100% | 100% | 54% | 54% | 50% | NA | NA | NA |
| Rhaiem 2020 | 11.75 (±2.25) | 90.3% | 61.9% | 47.6% | NA | NA | NA | 94.7% | 84.2% | 78.9% |
| Takahashi 2018 | 17 (±2.25) | 97.7% | 95.8% | 91.5% | NA | NA | NA | 97.7% | 95.8% | 91.5% |
| Shady 2017 | NA | 97% | 85.8% | 79% | NA | NA | 62% | 97% | 85.8% | 79% |
| Yang 2017 | NA | 100% | 94.3% | 80.3% | 56.2% | 39% | 39% | NA | NA | NA |
| Song 2016 | NA | 100% | 100% | 96.7% | 71.4% | 39.3% | 10% | NA | NA | NA |
| Eng 2015 | 17.46 (±11.51) | 96.9% | 87.9% | 66.7% | 19.3% | NA | 19.3% | NA | NA | NA |
| Engstrand 2014 | 28.25 (±11.25) | NA | NA | NA | NA | NA | 25% | NA | NA | NA |
| Ierardi 2013 | 15.77 (±8.25) | 88.2% | 82.3% | 70.6% | NA | NA | 64.7% | 88.2% | 88.2% | 76.5% |
| Stattner 2013 | 29.25 (±20.25) | 85.7% | 85.7% | 31% | 22% | 6% | 27.9% | NA | NA | NA |
| Shibata 2000 | NA | 100% | NA | 70% | NA | NA | 11.3% | NA | NA | NA |
| Seki 1999 | 21 (±8.09) | 73.4% | 66.7% | 60% | NA | NA | NA | NA | NA | NA |
| Total | 20.57 ° (±9.57°) | 95.5% {92.9– 97.2%} | 89.5% {85.9– 92.2%} | 65.1% {60.1– 69.7%} | 44.6% {38– 51.3%} | 34.3% {27.7– 41.5%} | 37.1% {31.9– 42.6%} | 96.3% {91.6– 98.4%} | 89.6% {83.3– 93.7%} | 83.7% {76.6– 88.9%} |
| Study ID | Hepatic Progression, ptn (%) | Extra-Hepatic Progression, pt n (%) | Overall Recurrence, pt n (%) | 3 Months OS | 6 Months OS | 1 Year OS | 3 Years OS | 5 Years OS | ||
| McEachron 2021 | 18 (50%) | 1 (2.8%) | 18 (50%) | 100% | 100% | 100% | 75% | 63% | ||
| Rhaiem 2020 | 7 (36.8%) | NA | 7 (36.8%) | 100% | 100% | 100% | NA | NA | ||
| Takahashi 2018 | NA | NA | 11 (21.6%) | NA | NA | NA | NA | NA | ||
| Shady 2017 | NA | NA | 23 (47.9%) | NA | NA | NA | NA | NA | ||
| Yang 2017 | NA | NA | 43 (60.6%) | 100% | 94.5% | 80.2% | 72% | 58% | ||
| Song 2016 | NA | NA | NA | 100% | 100% | 89.1% | 71.4% | 53.6% | ||
| Eng 2015 | 10 (30.3%) | 12 (36.4%) | 13 (39.4%) | 93.9% | 90.9% | 81.8% | 45.7% | NA | ||
| Engstrand 2014 | 17 (85%) | 11 (55%) | 15 (75%) | 100% | 100% | 90% | 41.5% | NA | ||
| Ierardi 2013 | 4 (23.5%) | 2 (11.8%) | 6 (35.3%) | 100% | 100% | NA | NA | NA | ||
| Stattner 2013 | 5 (11.6%) | 22 (51.2%) | 4 (9.3%) | 100% | 100% | 82% | 40% | 12% | ||
| Shibata 2000 | NA | NA | NA | 100% | 95% | 71% | 57% | 14% | ||
| Seki 1999 | 4 (26.6%) | 6 (40%) | 6 (40%) | 100% | 100% | 100% | NA | NA | ||
| Total | 65 (35.5%) {28.9–42.7%} | 54 (32.9%) {26.2–40.4%} | 146 (41.36%) {36.3–46.6%} | 99.3% {97.6– 99.8%} | 97.3% {94.8– 98.6%} | 86.7% {82.2– 90.2%} | 59.6% {53.3– 65.5%} | 44.8% {37.9– 51.8%} | ||
| Study ID | Patients/ Lesions Treated, n | Dimensi-ons, Mean (SD), mm | Percutaneous/ Surgical Treatment, pt n (%) | Surgical Open/Lap, pt n (%) | Single/ Multiple Lesions, pt n (%) | Synch, pt n (%)/Meta, pt n (%) | Neoadj, n (%) ±/ Adj, n (%) Treatment | Complica-tions n (% pt.) | CDs ≥3, n (%) |
|---|---|---|---|---|---|---|---|---|---|
| Rhaiem 2020 | 19/23 | 15.25 ° (±2.75 °) | 0±/ 19 (100%) | 15 (78.9%) ±/ 4 (21.1%) | 15 (78.9%) ±/ 4 (21.1%) | 8 (42.1%) ±/ 11 (57.9%) | 17 (89%) ±/ 19 (100%) | 6 (38%) | 0 |
| Takahashi 2018 | 51/121 | 21.25 ° (±2.83 °) | 0±/ 51 (100%) | 0±/ 51 (100%) | 0±/ 51 (100%) | NA/NA | 28 (54.9%)/NA | 7 (13.7%) | NA |
| Seki 1999 | 15/15 | 21.4 (±3.73 °) | 15 (100%) ±/ 0 | 0/0 | 15 (100%) ±/ 0 | 0±/ 15 (100%) | 0±/ 15 (100%) | 1 (6.7%) | 0 |
| Total | 85/159 | 20.39° (±2.90°) | 15 (17.6%)/ 70 (82.4%) {11–27.1%} ±/ {72.3–89%} | 15 (17.7%)/ 55 (64.7%) {11–27.1%} ±/ {54.1–74%} | 30 (35.3%)/ 55 (64.7%) {26.9–45.9%} ±/ {54.1–74%} | 8 (23.5%)/ 26 (76.5%) {12.4–40%} ±/ {60–87.6%} | 45 (52.9%)/ 34 (100%) {42.4–63.2%} ±/ {89.9–100%} | 14 (16.5%) {10.1–25.8%} | 0 (0%) {0–10.2%} |
| Study ID | 3 Months RF | 6 Months RF | 1 Year RF | 3 Months FFLR | 6 Months FFLR | 1 Year FFLR | Hepatic Progression, pt n (%) | Overall Recurrence, pt n (%) | 3 Months OS | 6 Months OS | 1 Year OS |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Rhaiem 2020 | 90.3% | 61.9% | 47.6% | 94.7% | 84.2% | 78.9% | 7 (36.84%) | 7 (36.8%) | 100% | 100% | 100% |
|
Takahashi 2018 | 97.7% | 95.8% | 91.5% | 97.7% | 95.8% | 91.5% | NA | 11 (21.6%) | NA | NA | NA |
|
Seki 1999 | 73.4% | 66.7% | 60% | NA | NA | NA | 4 (26.6%) | 6 (40%) | 100% | 100% | 100% |
| Total |
91.8% {83.9– 95.9%} |
83.5% {74.2– 89.9%} |
76.5% {66.4– 84.2%} |
97.1% {90.2– 99.2%} |
92.9% {84.3– 96.9%} |
88.6% {79– 94.1%} |
11 (32.4%) {19.1–49.1%} |
24 (28.2%) {19.8–38.6%} |
100% {89.9– 100%} |
100% {89.9– 100%} |
100% {89.9– 100%} |
| Study ID | Patients/ Lesions Treated, n | Dimensions, Mean (SD), mm | Lesions <30 mm, n (%) | Surgical Open/Lap, pt n (%) | Single/Multiple Lesions, pt n (%) | Synch, pt n (%)/Meta, pt n (%) | Complications n (%) | CDs ≥3, n (%) | |
|---|---|---|---|---|---|---|---|---|---|
| Surgical Approach |
McEachron 2021 | 36/135 | 19 ° (±19.5 °) | 132 (97.78%) | 13* (32.5% *)/ 27* (67.5% *) | NA | 13 (36.11%)/NA | 8 (22.2%) | 1 (2.8%) |
| Rhaiem 2020 | 19/23 | 15.25 ° (±2.75 °) | 23 (100%) | 15 (78.95%)/ 4 (21.05%) | 15 (78.95%)/ 4 (21.05%) | 8 (42,1%)/ 11 (57.89%) | 6 (38%) | 0 | |
| Takahashi 2018 | 51/121 | 21.25 ° (±2.83 °) | 121 (100%) | 0/ 51 (100%) | 0/ 51 (100%) | NA/NA | 7 (13.7%) | NA | |
|
Yang 2017 | 71/121 | 3 ° (±0.67°) | NA | 0/ 71 (100%) | 33 (46.48%)/ 38 (53.52%) | NA/NA | 9 (12.7%) | 0 | |
|
Eng 2015 | 33/49 | NA | 42 (85.71%) | NA | NA | NA/NA | 18 (54.5%) | 8 (24.2%) | |
|
Engstrand 2014 | 20/NA | NA | NA | 20 (100%)/ 0 | 0/ 20 (100%) | 18 (90%)/ 2 (10%) | 12 (60%) | 5 (25%) | |
| Stattner 2013 | 43/95 | 20.25 ° (±5.83°) | NA | 43 (100%)/ 0 | NA | 27 (62.8%)/ 16 (37.2%) | 15 | 4 | |
| Shibata 2000 | 14/58 | 27 (±11) | NA | 14 (100%)/ 0 | 0/ 14 (100%) | NA/NA | 2 | 2 | |
| Total | 287/602 |
15.51 ° (±7.16°) |
318 (96.9%) {94.5–98.3%} |
92 (42.2%)/ 126 (57.8%) {35.8–48.8%}/ {51.2–64.2%} |
48 (27.4%)/ 127 (72.6%) {21.4–34.5%}/ {65.5–78.6%} |
66 (55.9%)/ 29 (35.4%) {46.9–64.7%}/ {25.9–46.2%} |
77 (26.8%) {22–32.2%} |
20 (8.5%) {5.6–12.7%} | |
| Radiological Approach | Shady 2017 | 48/60 | 17 ° (±7.5 °) |
56 (93.33%) | − |
40 (83.3%)/ 8 (17.67%) | NA/NA | 19 | 6 (12%) |
| Song 2016 | 28/NA | NA | NA | − |
18 (64.3%)/ 10 (35.7%) |
10 (35.7%)/ 18 (64.3%) | 3 (10.7%) | 2 | |
| Ierardi 2013 | 17/23 | 34.52 (±13.25 °) |
1 (4.8%) | − |
14 (82.4%)/ 3 (17.6%) | NA/NA | 4 (23.5%) | 1 (5.9%) | |
| Seki 1999 | 15/15 | 21.4 (±3.73 °) |
15 (100%) | − |
15 (100%)/ 0 |
0/ 15 (100%) | 1 (6.7%) | 0 | |
| Total | 108/98 |
21.78 ° (±8.27°) |
72 (73.5%) {63.9–81.2%} | − |
87 (80.6%)/ 21 (19.4%) {72.1–86.9%}/ {13.1–27.9%} |
10 (23.3%)/ 33 (76.8%) {13.2–37.7%}/ {62.3–86.9%} |
27 (25%) {17.8–33.9%} |
9 (8.3%) {4.5–15.1%} |
|
Study ID | 3 Months RF | 6 Months RF | 1 Year RF | 3 Years RF | 5 Years RF | 3 Months FFLR | 6 Months FFLR | 1 year FFLR | Hepatic Progression pt n (%) | Overall Recurrence, pt n (%) | 3 Months OS | 6 Months OS | 1 Year OS | 3 Years OS | 5 Years OS | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Surgical Approach |
McEachron 2021 | 100% | 100% | 100% | 54% | 54% | NA | NA | NA | 18 (50%) | 18 (50%) | 100% | 100% | 100% | 75% | 63% |
| Rhaiem 2020 | 90.3% | 61.9% | 47.6% | NA | NA | 94.7% | 84.2% | 78.9% | 7 (36.8%) | 7 (36.8%) | 100% | 100% | 100% | NA | NA | |
| Takahashi 2018 | 97.7% | 95.8% | 91.5% | NA | NA | 97.7% | 95.8% | 91.5% | NA | 11 (21.6%) | NA | NA | NA | NA | NA | |
|
Yang 2017 | 100% | 94.3% | 80.3% | 56.2% | 39% | NA | NA | NA | NA | 43 (60.6%) | 100% | 94.5% | 80.2% | 72% | 58% | |
|
Eng 2015 | 96.9% | 87.9% | 66.7% | 19.3% | NA | NA | NA | NA | 10 (30.3%) | 13 (39.4%) | 93.9% | 90.9% | 81.8% | 45.7% | NA | |
|
Engstrand 2014 | NA | NA | NA | NA | NA | NA | NA | NA | 17 (85%) | 15 (75%) | 100% | 100% | 90% | 41.5% | NA | |
| Stattner 2013 | 85.7% | 85.7% | 31% | 22% | 6% | NA | NA | NA | 5 (11.63%) | 4 (9.3%) | 100% | 100% | 82% | 40% | 12% | |
| Shibata 2000 | 100% | NA | 70% | NA | NA | NA | NA | NA | NA | NA | 100% | 95% | 71% | 57% | 14% | |
| Total | 96.3% {93.2– 97.9%} | 90.9% {86.7– 93.9%} | 72.7% {67– 77.7%} | 40.4% {33.6– 47.7%} | 33.3% {26.3– 41.2%} | 97.1% {90.2– 99.2%} | 92.9% {84.3– 96.9%} | 88.6% {79– 94.1%} | 57 (37.6%) {30.4–45.7%} | 111 (40.7%) {35–46.6%} | 99.2% {96.9– 99.7%} | 96.6% {93.5– 98.3%} | 85.6% {80.54– 89.50%} | 58.1% {51.1– 64.4%} | 43.3% {35.9– 50.9%} | |
| Radiological Approach | Shady 2017 | 97% | 85.8% | 79% | NA | NA | 97% | 85.8% | 79% | NA | 23 (47.9%) | NA | NA | NA | NA | NA |
| Song 2016 | 100% | 100% | 96.7% | 71.4% | 39.3% | NA | NA | NA | NA | NA | 100% | 100% | 89.1% | 71.4% | 53.6% | |
|
Ierardi 2013 | 88.2% | 82.4% | 70.6% | NA | NA | 88.2% | 88.2% | 76.5% | 4 (23.5%) | 6 (35.3%) | 100% | 100% | NA | NA | NA | |
| Seki 1999 | 73.4% | 66.7% | 60% | NA | NA | NA | NA | NA | 4 (26.6%) | 6 (40%) | 100% | 100% | 100% | NA | NA | |
| Total | 93.5% {87.2– 96.8%} | 86.1% {78.3– 91.4%} | 79.6% {71.1– 86.2%} | 71.4% {52.9– 84.8%} | 39.3% {23.6– 57.6%} | 95.4% {87.3– 98.4%} | 86.2% {75.7– 92.5%} | (78.5%) {67–86.7%} | 8 (25%) {13.3–42.1%} | 35 (43.8%) {33.4–54.7%} | 100% {93.9– 100%} | 100% {93.9– 100%} | 93% {81.4– 97.6%} | 71.4% {52.9– 84.8%} | 53.6% {35.8– 70.5%} |
| Study ID | Patients/ Lesions Treated, n | Dimensions, Mean (SD), mm | Single/Multiple Lesions, pt n (%) | Complications, n (%) | CDs ≥ 3, n (%) | |
|---|---|---|---|---|---|---|
| Open | Engstrand 2014 | 20/NA | NA | 0/ 20 (100%) | 12 (60%) | 5 (25%) |
| Stattner 2013 | 43/95 | 20.25 ° (±5.83 °) | NA | 15 | 4 | |
| Shibata 2000 | 14/58 | 27 (±11) | 0/ 14 (100%) | 2 | 2 | |
| Total | 77/153 | 22.81 ° (±7.79 °) |
0 (0%)/34 (100%) {0–10.2%}/{89.9–100%} | 29 (37.7%) {27.7–48.8%} | 11 (14.3%) {8.2–23.8%} | |
| Laparoscopic | Takahashi 2018 | 51/121 | 21.25 ° (±2.83 °) | 0 51 (100%) | 7 (13.7%) | NA |
|
Yang 2017 | 71/121 | 3 ° (±0.67 °) | 33 (46.5%)/ 38 (53.5%) |
9 (12.7%) | 0 | |
| Total | 122/242 | 10.63 ° (±1.57 °) | 33 (27.1%)/89 (73%) {19.9–35.5%}/{64.5–80%} | 16 (13.1%) {8.2–20.3%} | - |
| Study ID | 3 Months RF | 6 Months RF | 1 Year RF | Overall Recurrence, pt n (%) | 3 Months OS | 6 Months OS | 1 Year OS | 3 Years OS | 5 Years OS | |
|---|---|---|---|---|---|---|---|---|---|---|
| Open | Engstrand 2014 | NA | NA | NA | 15 (75%) | 100% | 100% | 90% | 41.5% | NA |
| Stattner 2013 | 85.7% | 85.7% | 31% | 4 (9.3%) | 100% | 100% | 82% | 40% | 12% | |
| Shibata 2000 | 100% | NA | 70% | NA | 100% | 95% | 71% | 57% | 14% | |
| Total | 89.5% {78.9– 95.1%} | - | 40.4% {28.6– 53.3%} | 19 (30.2%) {20.2–42.4%} | 100% {95.3– 100%} | 98.7% {93– 99.8%} | 81.8% {71.8– 88.9%} | 42.9% {32.4– 54%} | 12.3% {6.1– 23.3%} | |
| Laparoscopic | Takahashi 2018 | 97.7% | 95.8% | 91.5% | 11 (21.6%) | NA | NA | NA | NA | NA |
| Yang 2017 | 100% | 94.3% | 80.3% | 43 (60.6%) | 100% | 94.5% | 80.2% | 72% | 58% | |
| Total | 99.2% {95.5– 99.9%} | 95.1% {89.7– 97.7%} | 85.5% {77.9– 90.5%} | 54 (44.3%) {35.8–53.1%} | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mimmo, A.; Pegoraro, F.; Rhaiem, R.; Montalti, R.; Donadieu, A.; Tashkandi, A.; Al-Sadairi, A.R.; Kianmanesh, R.; Piardi, T. Microwave Ablation for Colorectal Liver Metastases: A Systematic Review and Pooled Oncological Analyses. Cancers 2022, 14, 1305. https://doi.org/10.3390/cancers14051305
Mimmo A, Pegoraro F, Rhaiem R, Montalti R, Donadieu A, Tashkandi A, Al-Sadairi AR, Kianmanesh R, Piardi T. Microwave Ablation for Colorectal Liver Metastases: A Systematic Review and Pooled Oncological Analyses. Cancers. 2022; 14(5):1305. https://doi.org/10.3390/cancers14051305
Chicago/Turabian StyleMimmo, Antonio, Francesca Pegoraro, Rami Rhaiem, Roberto Montalti, Alix Donadieu, Ahmad Tashkandi, Abdul Rahman Al-Sadairi, Reza Kianmanesh, and Tullio Piardi. 2022. "Microwave Ablation for Colorectal Liver Metastases: A Systematic Review and Pooled Oncological Analyses" Cancers 14, no. 5: 1305. https://doi.org/10.3390/cancers14051305
APA StyleMimmo, A., Pegoraro, F., Rhaiem, R., Montalti, R., Donadieu, A., Tashkandi, A., Al-Sadairi, A. R., Kianmanesh, R., & Piardi, T. (2022). Microwave Ablation for Colorectal Liver Metastases: A Systematic Review and Pooled Oncological Analyses. Cancers, 14(5), 1305. https://doi.org/10.3390/cancers14051305