
Fluorescence Polarization Imaging of Methylene Blue Facilitates Quantitative Detection of Thyroid Cancer in Single Cells

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Samples
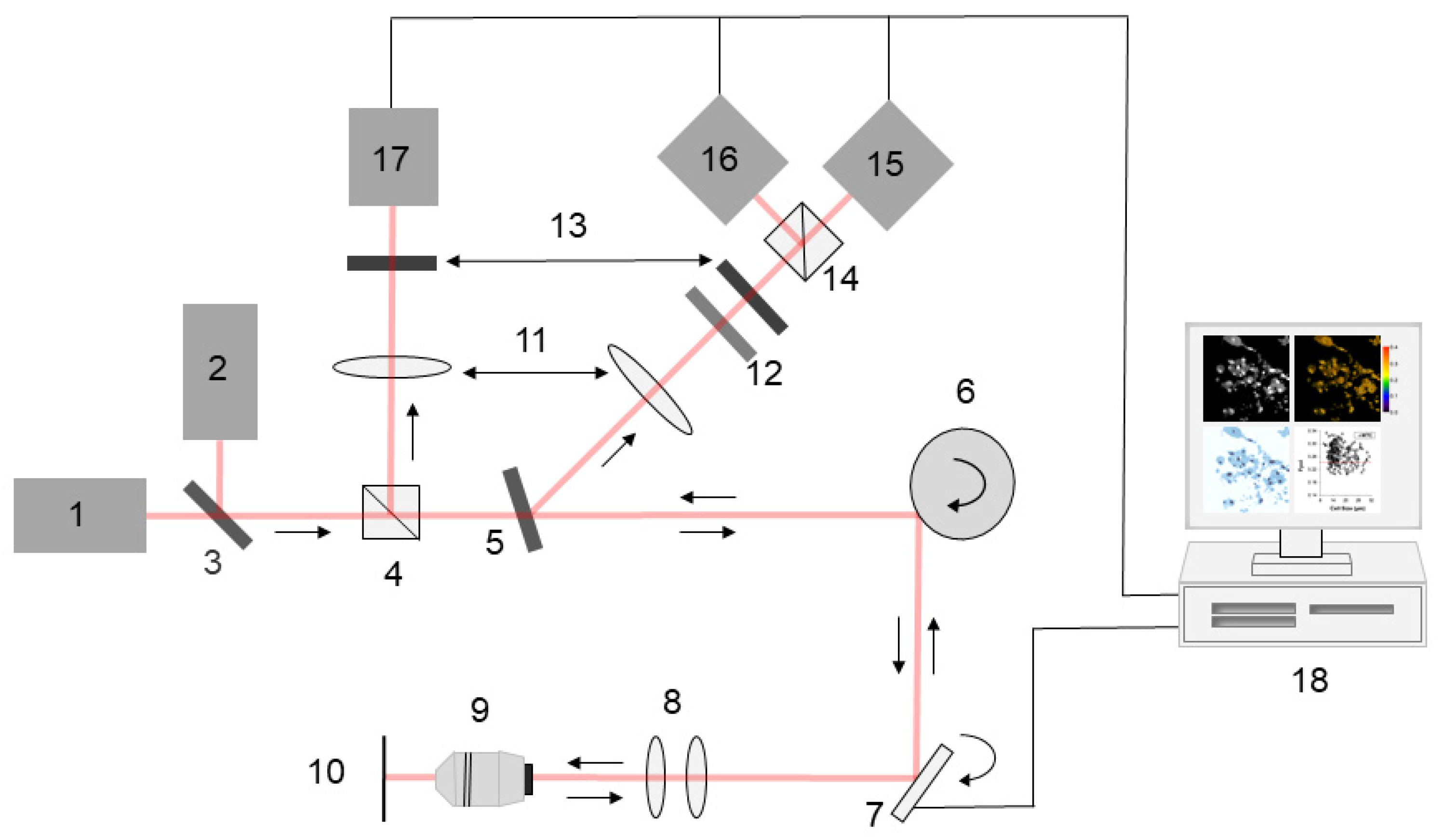
2.3. Multimodal Optical Imaging
2.4. Image Processing
2.5. Trypan Blue Exclusion Test
2.6. Statistical Analysis
3. Results
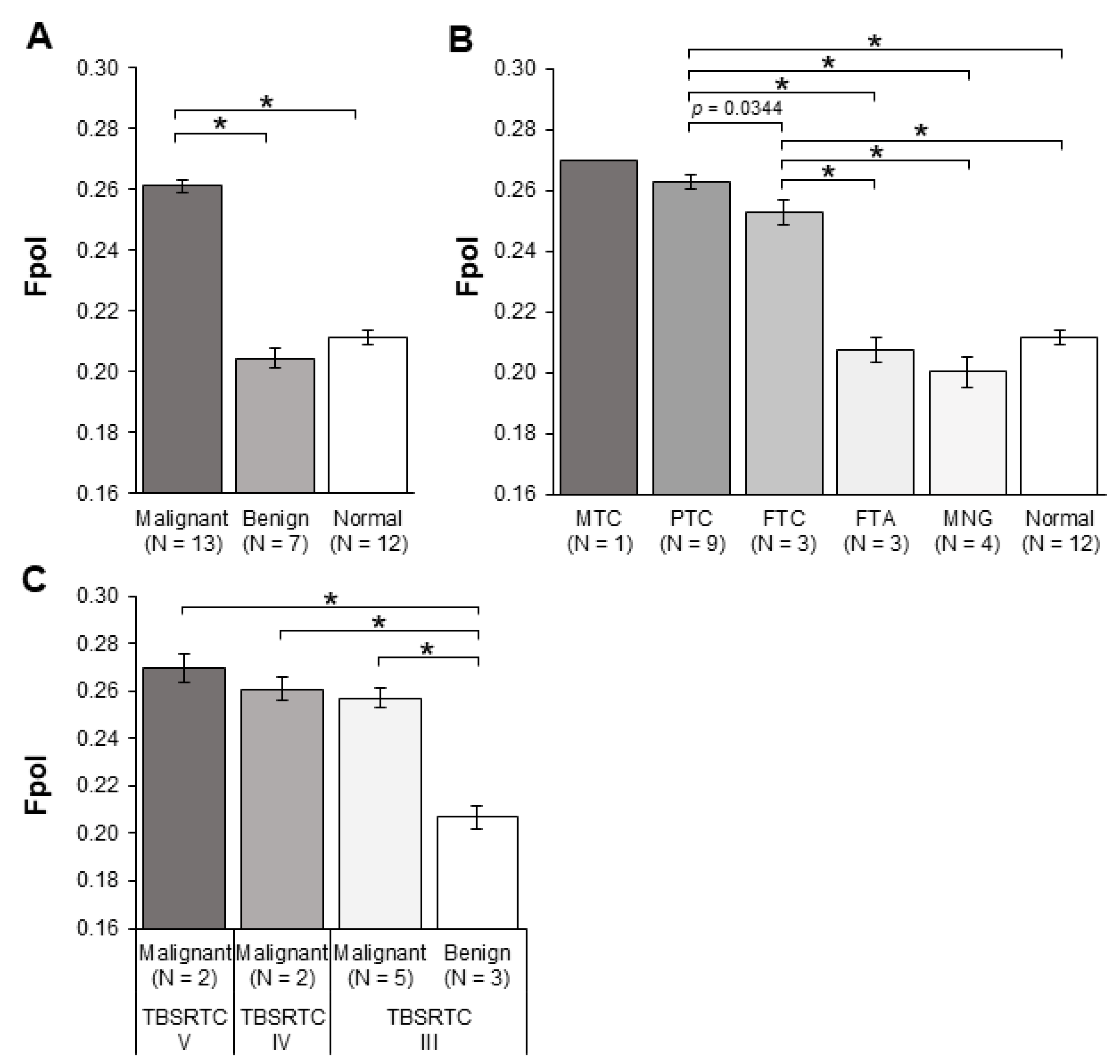
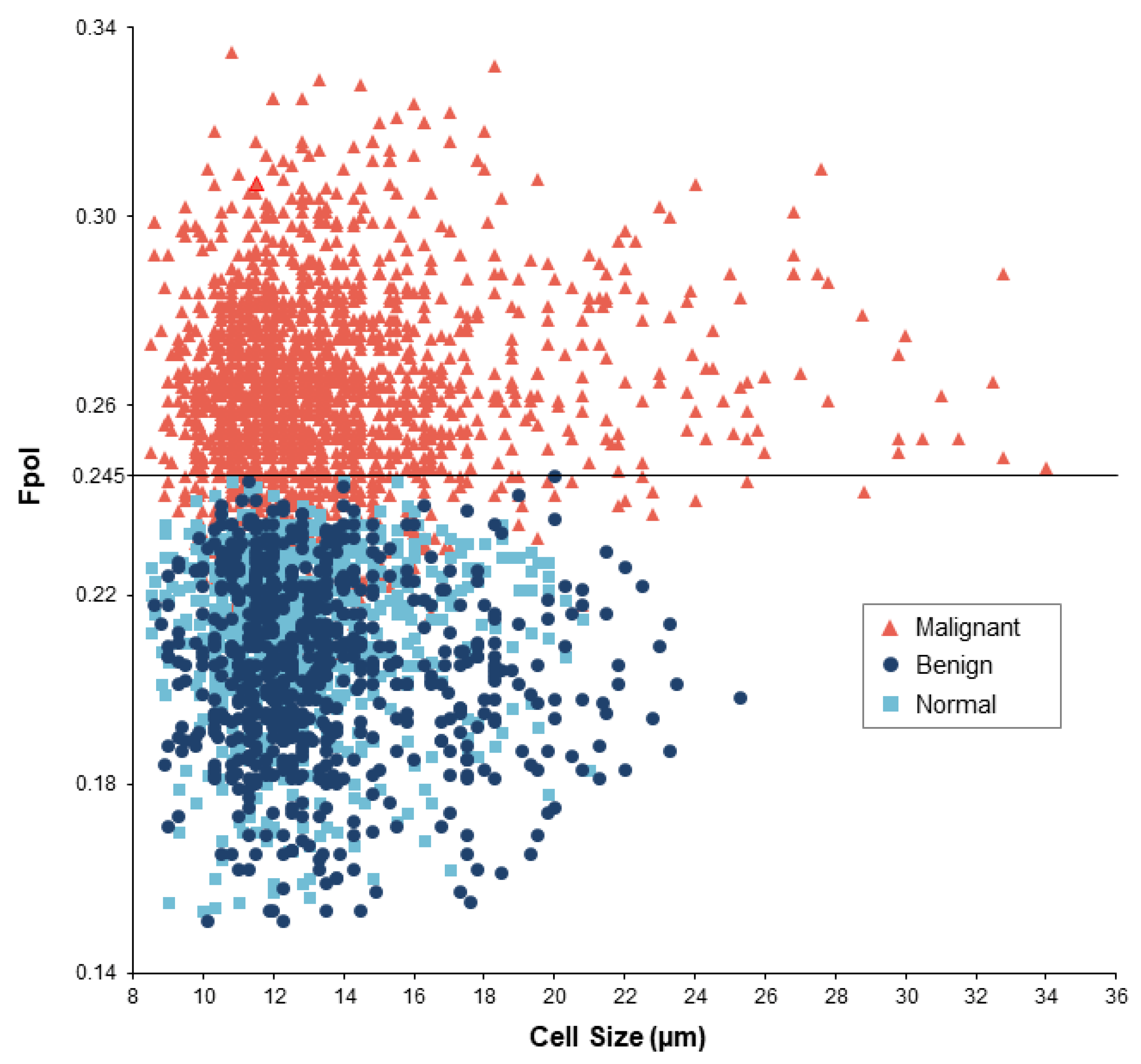
3.1. MB Fpol Is Significantly Elevated in Thyroid Cancer
3.2. MB Fpol Accurately Discriminates Cytologically Indeterminate Nodules
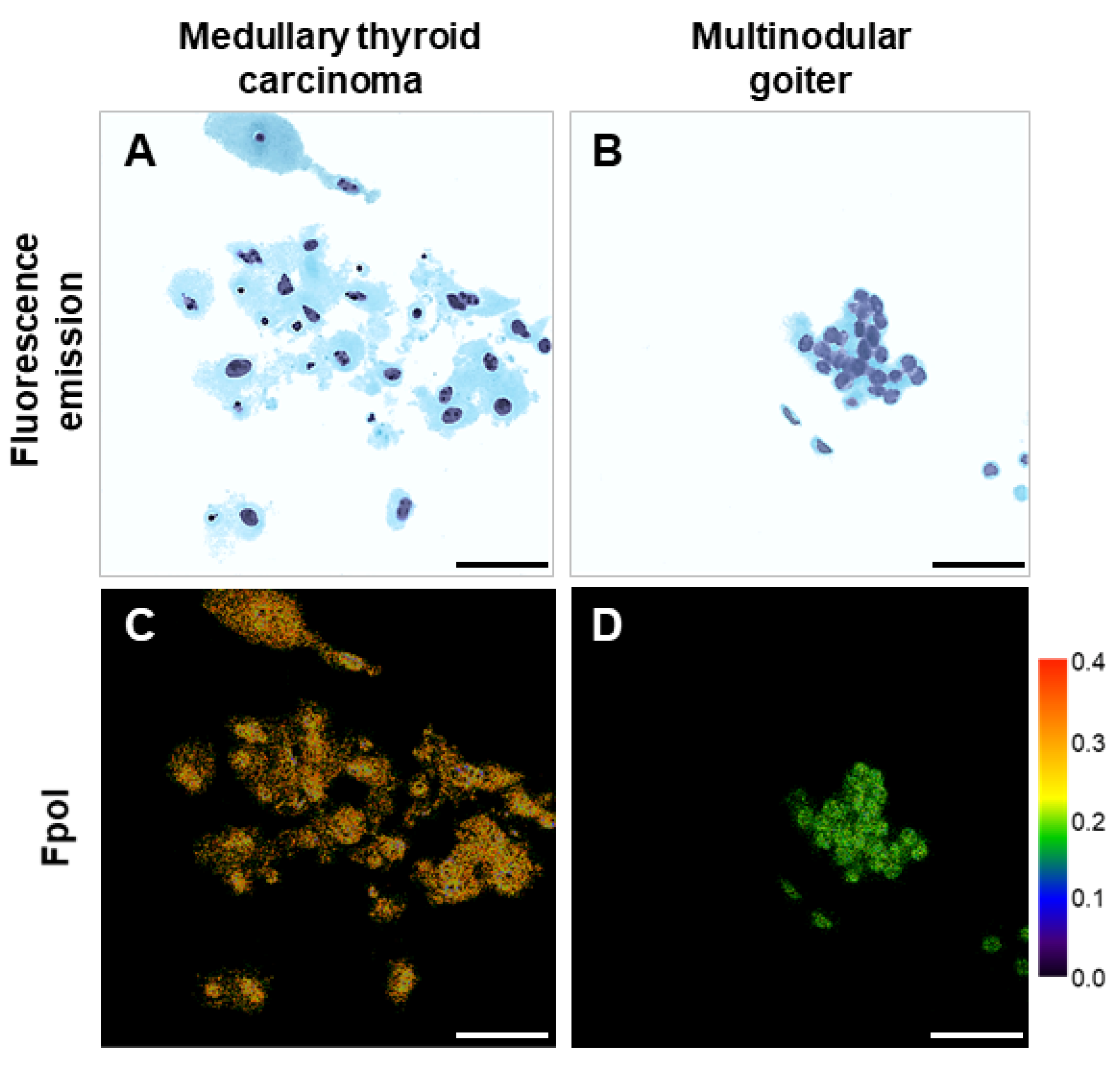
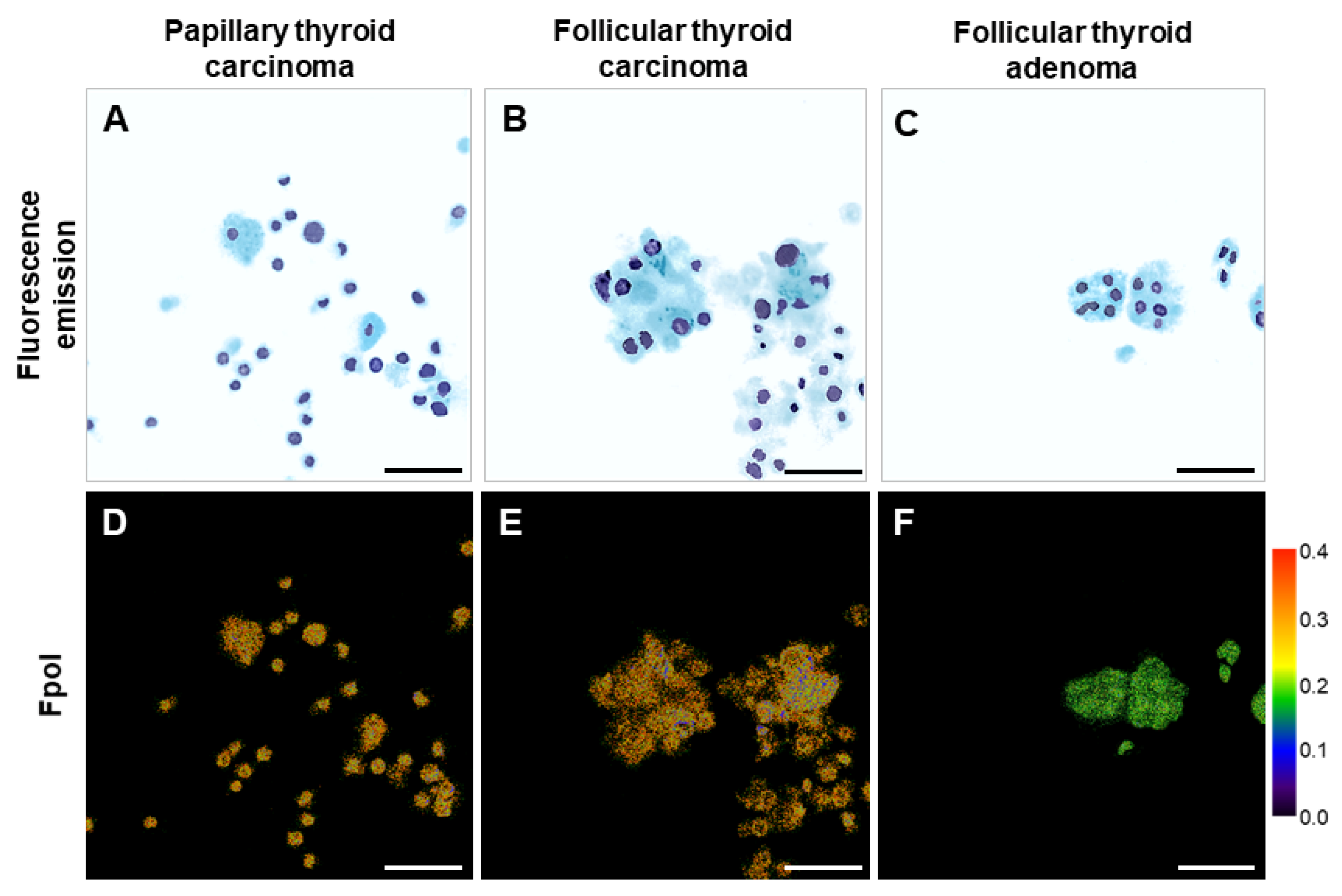
3.3. Fpol Images Provide Quantitative Cellular Level Contrast for Cancer Detection
3.4. Cellular MB Fpol Values Are Not Patient Specific
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vaccarella, S.; Franceschi, S.; Bray, F.; Wild, C.P.; Plummer, M.; Dal Maso, L. Worldwide Thyroid-Cancer Epidemic? The Increasing Impact of Overdiagnosis. N. Engl. J. Med. 2016, 375, 614–617. [Google Scholar] [CrossRef] [PubMed]
- Davies, L.; Welch, H.G. Current thyroid cancer trends in the United States. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabanillas, M.E.; McFadden, D.G.; Durante, C. Thyroid cancer. Lancet 2016, 388, 2783–2795. [Google Scholar] [CrossRef]
- Kitahara, C.M.; Sosa, J.A. The changing incidence of thyroid cancer. Nat. Rev. Endocrinol. 2016, 12, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Cancer Facts & Figures, 2021. The American Cancer Society. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf (accessed on 23 December 2021).
- Bomeli, S.R.; LeBeau, S.O.; Ferris, R.L. Evaluation of a thyroid nodule. Otolaryngol. Clin. N. Am. 2010, 43, 229–238. [Google Scholar] [CrossRef] [Green Version]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2017, 27, 1341–1346. [Google Scholar] [CrossRef] [PubMed]
- Naz, S.; Hashmi, A.A.; Khurshid, A.; Faridi, N.; Edhi, M.M.; Kamal, A.; Khan, M. Diagnostic accuracy of Bethesda system for reporting thyroid cytopathology: An institutional perspective. Int. Arch. Med. 2014, 7, 46. [Google Scholar] [CrossRef]
- Ugurluoglu, C.; Dobur, F.; Karabagli, P.; Celik, Z.E. Fine needle aspiration biopsy of thyroid nodules: Cytologic and histopathologic correlation of 1096 patients. Int. J. Clin. Exp. Pathol. 2015, 8, 14800–14805. [Google Scholar]
- Bongiovanni, M.; Spitale, A.; Faquin, W.C.; Mazzucchelli, L.; Baloch, Z.W. The Bethesda System for Reporting Thyroid Cytopathology: A meta-analysis. Acta Cytol. 2012, 56, 333–339. [Google Scholar] [CrossRef]
- Fulciniti, F.; Cipolletta Campanile, A.; Malzone, M.G.; Chiofalo, M.G.; Capiluongo, A.; Monaco, M.; Di Maio, N.; Sandomenico, F.; Botti, G.; Chiappetta, G.; et al. Impact of ultrasonographic features, cytomorphology and mutational testing on malignant and indeterminate thyroid nodules on diagnostic accuracy of fine needle cytology samples: A prospective analysis of 141 patients. Clin. Endocrinol. 2019, 91, 851–859. [Google Scholar] [CrossRef]
- Vargas-Salas, S.; Martínez, J.R.; Urra, S.; Domínguez, J.M.; Mena, N.; Uslar, T.; Lagos, M.; Henríquez, M.; González, H.E. Genetic testing for indeterminate thyroid cytology: Review and meta-analysis. Endocr. Relat. Cancer 2018, 25, R163–R177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baloch, Z.W.; Fleisher, S.; LiVolsi, V.A.; Gupta, P.K. Diagnosis of “follicular neoplasm”: A gray zone in thyroid fine-needle aspiration cytology. Diagn. Cytopathol. 2002, 26, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Howitt, B.E.; Chang, S.; Eszlinger, M.; Paschke, R.; Drage, M.G.; Krane, J.F.; Barletta, J.A. Fine-needle aspiration diagnoses of noninvasive follicular variant of papillary thyroid carcinoma. Am. J. Clin. Pathol. 2015, 144, 850–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misiakos, E.P.; Margari, N.; Meristoudis, C.; Machairas, N.; Schizas, D.; Petropoulos, K.; Spathis, A.; Karakitsos, P.; Machairas, A. Cytopathologic diagnosis of fine needle aspiration biopsies of thyroid nodules. World J. Clin. Cases 2016, 4, 38–48. [Google Scholar] [CrossRef]
- Valderrabano, P.; McIver, B. Evaluation and Management of Indeterminate Thyroid Nodules: The Revolution of Risk Stratification Beyond Cytological Diagnosis. Cancer Control 2017, 24, 1073274817729231. [Google Scholar] [CrossRef]
- Hannoush, Z.C.; Weiss, R.E. Thyroid Hormone Replacement in Patients Following Thyroidectomy for Thyroid Cancer. Rambam Maimonides Med. J. 2016, 7, e0002. [Google Scholar] [CrossRef]
- Zhang, M.; Lin, O. Molecular Testing of Thyroid Nodules: A Review of Current Available Tests for Fine-Needle Aspiration Specimens. Arch. Pathol. Lab. Med. 2016, 140, 1338–1344. [Google Scholar] [CrossRef] [Green Version]
- Poller, D.N.; Johnson, S.J. Recent Developments in the Pathology of Thyroid Cancer. Clin. Oncol. (R Coll. Radiol.) 2017, 29, 278–282. [Google Scholar] [CrossRef] [Green Version]
- Steward, D.L.; Kloos, R.T. Clinical diagnostic gene expression thyroid testing. Otolaryngol. Clin. N. Am. 2014, 47, 573–593. [Google Scholar] [CrossRef]
- Nikiforova, M.N.; Mercurio, S.; Wald, A.I.; Barbi de Moura, M.; Callenberg, K.; Santana-Santos, L.; Gooding, W.E.; Yip, L.; Ferris, R.L.; Nikiforov, Y.E. Analytical performance of the ThyroSeq v3 genomic classifier for cancer diagnosis in thyroid nodules. Cancer 2018, 124, 1682–1690. [Google Scholar] [CrossRef] [Green Version]
- Sciacchitano, S.; Lavra, L.; Ulivieri, A.; Magi, F.; De Francesco, G.P.; Bellotti, C.; Salehi, L.B.; Trovato, M.; Drago, C.; Bartolazzi, A. Comparative analysis of diagnostic performance, feasibility and cost of different test-methods for thyroid nodules with indeterminate cytology. Oncotarget 2017, 8, 49421–49442. [Google Scholar] [CrossRef] [PubMed]
- Valderrabano, P.; Hallanger-Johnson, J.E.; Thapa, R.; Wang, X.; McIver, B. Comparison of Postmarketing Findings vs the Initial Clinical Validation Findings of a Thyroid Nodule Gene Expression Classifier: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Marcadis, A.R.; Valderrabano, P.; Ho, A.S.; Tepe, J.; Swartzwelder, C.E.; Byrd, S.; Sacks, W.L.; Untch, B.R.; Shaha, A.R.; Xu, B.; et al. Interinstitutional variation in predictive value of the ThyroSeq v2 genomic classifier for cytologically indeterminate thyroid nodules. Surgery 2019, 165, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Riaz, A.; Shreedhar, B.; Kamboj, M.; Natarajan, S. Methylene blue as an early diagnostic marker for oral precancer and cancer. Springerplus 2013, 2, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R.; Khan, A.; Quinlan, R.; Yaroslavsky, A.N. Polarization-sensitive multimodal imaging for detecting breast cancer. Cancer Res. 2014, 74, 4685–4693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, R.S.P.; Liebelt, E.L. Methylene Blue: An Antidote for Methemoglobinemia and Beyond. Pediatr. Emerg. Care 2021, 37, 474–477. [Google Scholar] [CrossRef]
- Varghese, P.; Abdel-Rahman, A.T.; Akberali, S.; Mostafa, A.; Gattuso, J.M.; Carpenter, R. Methylene blue dye--a safe and effective alternative for sentinel lymph node localization. Breast J. 2008, 14, 61–67. [Google Scholar] [CrossRef]
- Harari, A.; Sippel, R.S.; Goldstein, R.; Aziz, S.; Shen, W.; Gosnell, J.; Duh, Q.Y.; Clark, O.H. Successful localization of recurrent thyroid cancer in reoperative neck surgery using ultrasound-guided methylene blue dye injection. J. Am. Coll. Surg. 2012, 215, 555–561. [Google Scholar] [CrossRef]
- Ji, Y.B.; Lee, K.J.; Park, Y.S.; Hong, S.M.; Paik, S.S.; Tae, K. Clinical efficacy of sentinel lymph node biopsy using methylene blue dye in clinically node-negative papillary thyroid carcinoma. Ann. Surg. Oncol. 2012, 19, 1868–1873. [Google Scholar] [CrossRef]
- Santrac, N.; Markovic, I.; Medic Milijic, N.; Goran, M.; Buta, M.; Djurisic, I.; Dzodic, R. Sentinel lymph node biopsy in medullary thyroid microcarcinomas. Endocr. J. 2020, 67, 295–304. [Google Scholar] [CrossRef] [Green Version]
- Hillary, S.L.; Guillermet, S.; Brown, N.J.; Balasubramanian, S.P. Use of methylene blue and near-infrared fluorescence in thyroid and parathyroid surgery. Langenbecks Arch. Surg. 2018, 403, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaroslavsky, A.N.; Feng, X.; Muzikansky, A.; Hamblin, M.R. Fluorescence Polarization of Methylene Blue as a Quantitative Marker of Breast Cancer at the Cellular Level. Sci. Rep. 2019, 9, 940. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Muzikansky, A.; Ross, A.H.; Hamblin, M.R.; Jermain, P.R.; Yaroslavsky, A.N. Multimodal quantitative imaging of brain cancer in cultured cells. Biomed. Opt. Express 2019, 10, 4237–4248. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Jermain, P.; Feng, X.; Yaroslavsky, A.N. Multimodal optical imaging of renal cells. Opt. Eng. 2019, 58, 082415. [Google Scholar] [CrossRef]
- Jameson, D.M.; Ross, J.A. Fluorescence polarization/anisotropy in diagnostics and imaging. Chem. Rev. 2010, 110, 2685–2708. [Google Scholar] [CrossRef] [Green Version]
- Siegel, J.; Suhling, K.; Lévêque-Fort, S.; Sabharwal, Y.; Webb, S.E.D.; Davis, D.M.; Phillips, D.; French, P.M.W. Wide-field time-resolved fluorescence anisotropy imaging (TR-FAIM)–A novel approach to image the viscosity of a fluorophore environment. Rev. Sci. Instrum. 2003, 74, 182–190. [Google Scholar] [CrossRef] [Green Version]
- Strober, W. Trypan blue exclusion test of cell viability. Curr. Protoc. Immunol. 2001, 21, A3B. [Google Scholar] [CrossRef]
- Demidenko, E. Mixed Models: Theory and Applications with R; Wiley: New York, NY, USA, 2013. [Google Scholar]
- Khan, T.M.; Zeiger, M.A. Thyroid Nodule Molecular Testing: Is It Ready for Prime Time? Front. Endocrinol. 2020, 11, 590128. [Google Scholar] [CrossRef]
- Zhou, C.; Wang, Y.; Aguirre, A.D.; Tsai, T.H.; Cohen, D.W.; Connolly, J.L.; Fujimoto, J.G. Ex vivo imaging of human thyroid pathology using integrated optical coherence tomography and optical coherence microscopy. J. Biomed. Opt. 2010, 15, 016001. [Google Scholar] [CrossRef] [Green Version]
- Tokarz, D.; Cisek, R.; Joseph, A.; Asa, S.L.; Wilson, B.C.; Barzda, V. Characterization of pathological thyroid tissue using polarization-sensitive second harmonic generation microscopy. Lab. Investig. 2020, 100, 1280–1287. [Google Scholar] [CrossRef]
- Levi, J.; Kothapalli, S.R.; Bohndiek, S.; Yoon, J.K.; Dragulescu-Andrasi, A.; Nielsen, C.; Tisma, A.; Bodapati, S.; Gowrishankar, G.; Yan, X.; et al. Molecular photoacoustic imaging of follicular thyroid carcinoma. Clin. Cancer Res. 2013, 19, 1494–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouyang, Y.; Liu, Y.; Wang, Z.M.; Liu, Z.; Wu, M. FLIM as a Promising Tool for Cancer Diagnosis and Treatment Monitoring. Nanomicro. Lett. 2021, 13, 133. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.N.; Mochizuki, K.; Hashimoto, K.; Kumamoto, Y.; Harada, Y.; Fujita, K.; Komatsuzaki, T. High-Resolution Raman Microscopic Detection of Follicular Thyroid Cancer Cells with Unsupervised Machine Learning. J. Phys. Chem. B 2019, 123, 4358–4372. [Google Scholar] [CrossRef] [PubMed]
- Freeman, E.E.; Semeere, A.; Osman, H.; Peterson, G.; Rajadhyaksha, M.; González, S.; Martin, J.N.; Anderson, R.R.; Tearney, G.J.; Kang, D. Smartphone confocal microscopy for imaging cellular structures in human skin in vivo. Biomed. Opt. Express 2018, 9, 1906–1915. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Site | Diagnosis | TBSRTC Category | Tumor Sample | Normal Sample | ||
|---|---|---|---|---|---|---|---|
| Number of Cells | Mean Fpol ± SD | Number of Cells | Mean Fpol ± SD | ||||
| 1 | UMMC | MTC | VI | 247 | 0.270 ± 0.028 | 47 | 0.209 ± 0.014 |
| 2 | UMMC | PTC | VI | 137 | 0.253 ± 0.016 | 84 | 0.211 ± 0.015 |
| 3 | UMMC | PTC | VI | 79 | 0.263 ± 0.019 | 72 | 0.219 ± 0.012 |
| 4 | UMMC | PTC | VI | 103 | 0.257 ± 0.014 | 52 | 0.220 ± 0.012 |
| 5 | LGH | PTC | V | 57 | 0.263 ± 0.015 | 125 | 0.215 ± 0.018 |
| 6 | LGH | PTC | V | 204 | 0.276 ± 0.019 | - | - |
| 7 | LGH | PTC | IV | 84 | 0.260 ± 0.014 | - | - |
| 8 | LGH | PTC | III | 128 | 0.268 ± 0.019 | - | - |
| 9 | LGH | PTC | III | 210 | 0.259 ± 0.018 | - | - |
| 10 | LGH | PTC | III | 254 | 0.263 ± 0.016 | - | - |
| 11 | UMMC | FTC | IV | 89 | 0.262 ± 0.019 | 25 | 0.221 ± 0.024 |
| 12 | UMMC | FTC | III | 94 | 0.250 ± 0.015 | 59 | 0.210 ± 0.012 |
| 13 | LGH | FTC | III | 191 | 0.246 ± 0.016 | - | - |
| 14 | UMMC | FTA | III | 134 | 0.215 ± 0.018 | 102 | 0.205 ± 0.021 |
| 15 | UMMC | FTA | III | 145 | 0.211 ± 0.021 | 90 | 0.216 ± 0.010 |
| 16 | LGH | FTA | III | 129 | 0.204 ± 0.025 | 86 | 0.219 ± 0.021 |
| 17 | UMMC | MNG | II | 70 | 0.207 ± 0.026 | - | - |
| 18-1 | UMMC | MNG | II | 50 | 0.196 ± 0.025 | - | - |
| 18-2 | UMMC | MNG | II | 51 | 0.210 ± 0.019 | - | - |
| 19 | LGH | MNG | II | 145 | 0.196 ± 0.015 | - | - |
| 20 | LGH | Normal | - | - | - | 100 | 0.221 ± 0.014 |
| 21 | LGH | Normal | - | - | - | 78 | 0.204 ± 0.043 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jermain, P.R.; Fischer, A.H.; Joseph, L.; Muzikansky, A.; Yaroslavsky, A.N. Fluorescence Polarization Imaging of Methylene Blue Facilitates Quantitative Detection of Thyroid Cancer in Single Cells. Cancers 2022, 14, 1339. https://doi.org/10.3390/cancers14051339
Jermain PR, Fischer AH, Joseph L, Muzikansky A, Yaroslavsky AN. Fluorescence Polarization Imaging of Methylene Blue Facilitates Quantitative Detection of Thyroid Cancer in Single Cells. Cancers. 2022; 14(5):1339. https://doi.org/10.3390/cancers14051339
Chicago/Turabian StyleJermain, Peter R., Andrew H. Fischer, Lija Joseph, Alona Muzikansky, and Anna N. Yaroslavsky. 2022. "Fluorescence Polarization Imaging of Methylene Blue Facilitates Quantitative Detection of Thyroid Cancer in Single Cells" Cancers 14, no. 5: 1339. https://doi.org/10.3390/cancers14051339
APA StyleJermain, P. R., Fischer, A. H., Joseph, L., Muzikansky, A., & Yaroslavsky, A. N. (2022). Fluorescence Polarization Imaging of Methylene Blue Facilitates Quantitative Detection of Thyroid Cancer in Single Cells. Cancers, 14(5), 1339. https://doi.org/10.3390/cancers14051339