
Systemic Treatments for Advanced Small Bowel Adenocarcinoma: A Systematic Review

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
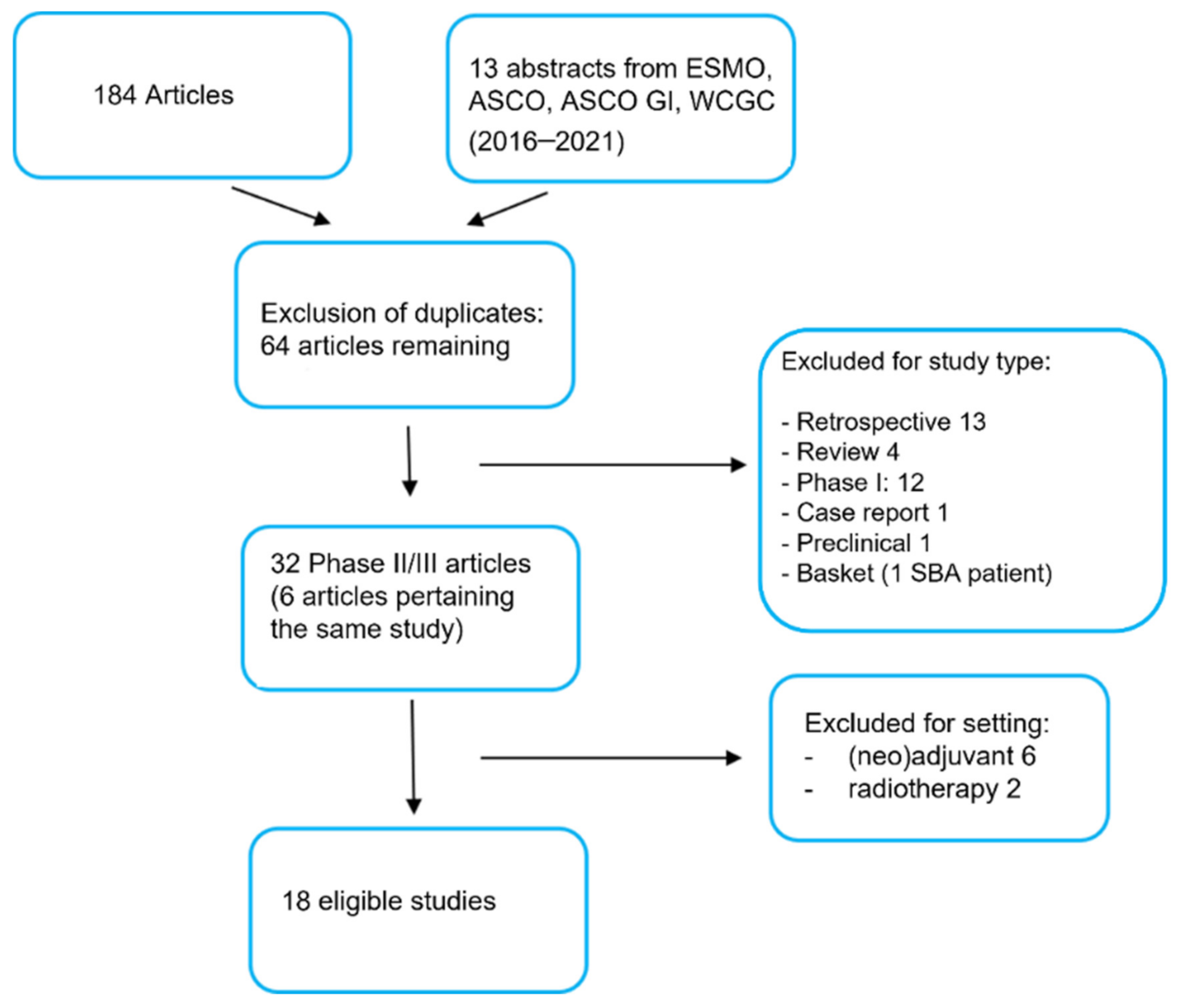
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- Population: patients affected by unresectable or metastatic small bowel adenocarcinoma; any age, any gender and any performance status, enrolled in phase II/III clinical trials.
- Intervention: Any type of treatment for advanced unresectable disease, including chemotherapy combinations, biological drugs (such as anti-vascular endothelial growth factor receptor biologics, tyrosine kinase inhibitors, anti-EGFR monoclonal antibodies) and immunotherapy.
- Comparison: This criterion did not apply to the aims of this systematic review.
- Outcomes of interest: Efficacy of treatments for advanced small bowel adenocarcinoma, including overall survival, progression free survival and overall response rate.
2.3. Exclusion Criteria
2.4. Data Collection
3. Results
3.1. Chemotherapy Combinations
3.2. Targeted Therapy
3.2.1. Anti-Vascular Treatment
3.2.2. Anti-EGFR Treatment
3.2.3. Anti-BRAF Treatment
3.2.4. Other Targeted Agents
3.3. Immunotherapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2016. CA A Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilimoria, K.Y.; Bentrem, D.J.; Wayne, J.D.; Ko, C.Y.; Bennett, C.L.; Talamonti, M.S. Small Bowel Cancer in the United States: Changes in Epidemiology, Treatment, and Survival over the Last 20 Years. Ann. Surg. 2009, 249, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Halfdanarson, T.R.; McWilliams, R.R.; Donohue, J.H.; Quevedo, J.F. A Single-Institution Experience with 491 Cases of Small Bowel Adenocarcinoma. Am. J. Surg. 2010, 199, 797–803. [Google Scholar] [CrossRef] [PubMed]
- Dabaja, B.S.; Suki, D.; Pro, B.; Bonnen, M.D.; Ajani, J. Adenocarcinoma of the Small Bowel: Presentation, Prognostic Factors, and Outcome of 217 Patients. Cancer 2004, 101, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Falcone, R.; Roberto, M.; Filetti, M.; Anselmi, E.; Marchetti, P. Anti Epidermal Growth Factor Receptor Therapy in Small Bowel Adenocarcinoma: Case Report and Literature Review. Medicine 2018, 97, e9672. [Google Scholar] [CrossRef]
- Williams, A.S.; Huang, W.-Y. The Analysis of Microsatellite Instability in Extracolonic Gastrointestinal Malignancy. Pathology 2013, 45, 540–552. [Google Scholar] [CrossRef]
- McWilliams, R.R.; Foster, N.R.; Mahoney, M.R.; Smyrk, T.C.; Murray, J.A.; Ames, M.M.; Horvath, L.E.; Schneider, D.J.; Hobday, T.J.; Jatoi, A.; et al. North Central Cancer Treatment Group N0543 (Alliance): A Phase 2 Trial of Pharmacogenetic-Based Dosing of Irinotecan, Oxaliplatin, and Capecitabine as First-Line Therapy for Patients with Advanced Small Bowel Adenocarcinoma. Cancer 2017, 123, 3494–3501. [Google Scholar] [CrossRef]
- Gibson, M.K.; Holcroft, C.A.; Kvols, L.K.; Haller, D. Phase II Study of 5-Fluorouracil, Doxorubicin, and Mitomycin C for Metastatic Small Bowel Adenocarcinoma. Oncologist 2005, 10, 132–137. [Google Scholar] [CrossRef] [Green Version]
- Overman, M.J.; Varadhachary, G.R.; Kopetz, S.; Adinin, R.; Lin, E.; Morris, J.S.; Eng, C.; Abbruzzese, J.L.; Wolff, R.A. Phase II Study of Capecitabine and Oxaliplatin for Advanced Adenocarcinoma of the Small Bowel and Ampulla of Vater. J. Clin. Oncol. 2009, 27, 2598–2603. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Shin, S.J.; Kim, J.-H.; Kim, H.; Choi, H.J. Better Outcome of XELOX Chemotherapy in Patients with Advanced Intestinal-Type Adenocarcinoma of the Ampulla of Vater. Tohoku J. Exp. Med. 2013, 231, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Horimatsu, T.; Nakayama, N.; Moriwaki, T.; Hirashima, Y.; Fujita, M.; Asayama, M.; Moriyama, I.; Nakashima, K.; Baba, E.; Kitamura, H.; et al. A Phase II Study of 5-Fluorouracil/L-Leucovorin/Oxaliplatin (MFOLFOX6) in Japanese Patients with Metastatic or Unresectable Small Bowel Adenocarcinoma. Int. J. Clin. Oncol. 2017, 22, 905–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiang, X.J.; Liu, Y.W.; Zhang, L.; Qiu, F.; Yu, F.; Zhan, Z.Y.; Feng, M.; Yan, J.; Zhao, J.G.; Xiong, J.P. A Phase II Study of Modified FOLFOX as First-Line Chemotherapy in Advanced Small Bowel Adenocarcinoma. Anti-Cancer Drugs 2012, 23, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Overman, M.; Adam, L.; Raghav, K.; Wang, J.; Kee, B.; Fogelman, D.; Eng, C.; Vilar, E.; Shroff, R.; Dasari, A.; et al. Phase II Study of Nab-Paclitaxel in Refractory Small Bowel Adenocarcinoma and CpG Island Methylator Phenotype (CIMP)-High Colorectal Cancer. Ann. Oncol. 2018, 29, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Gulhati, P.; Raghav, K.; Shroff, R.T.; Varadhachary, G.R.; Kopetz, S.; Javle, M.; Qiao, W.; Wang, H.; Morris, J.; Wolff, R.A.; et al. Bevacizumab Combined with Capecitabine and Oxaliplatin in Patients with Advanced Adenocarcinoma of the Small Bowel or Ampulla of Vater: A Single-Center, Open-Label, Phase 2 Study. Cancer 2017, 123, 1011–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramucirumab and Paclitaxel or FOLFIRI in Advanced Small Bowel Cancers-Full Text View-ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04205968 (accessed on 4 February 2022).
- Gulhati, P.; Raghav, K.; Shroff, R.; Varadhachary, G.; Javle, M.; Qiao, W.; Wang, H.; Morris, J.; Wolff, R.; Overman, M.J. Phase II Study of Panitumumab in RAS Wild-Type Metastatic Adenocarcinoma of Small Bowel or Ampulla of Vater. Oncologist 2018, 23, 277-e26. [Google Scholar] [CrossRef] [Green Version]
- Subbiah, V.; Bang, Y.-J.; Lassen, U.N.; Wainberg, Z.A.; Soria, J.-C.; Wen, P.Y.; Zenz, T.; Moreau, P.; Brunsvig, P.; De Braud, F.G.; et al. ROAR: A phase 2, open-label study in patients (pts) with BRAF V600E–mutated rare cancers to investigate the efficacy and safety of dabrafenib (D) and trametinib (T) combination therapy. J. Clin. Oncol. 2016, 34, TPS2604. [Google Scholar] [CrossRef]
- Hainsworth, J.D.; Meric-Bernstam, F.; Swanton, C.; Hurwitz, H.; Spigel, D.R.; Sweeney, C.; Burris, H.A.; Bose, R.; Yoo, B.; Stein, A.; et al. Targeted Therapy for Advanced Solid Tumors on the Basis of Molecular Profiles: Results From MyPathway, an Open-Label, Phase IIa Multiple Basket Study. J. Clin. Oncol. 2018, 36, 536–542. [Google Scholar] [CrossRef]
- Tournigand, C.; Flechon, A.; Oudard, S.; Saada-Bouzid, E.; Pouessel, D.; Le Tourneau, C.; Augereau, P.; Beylot-Barry, M.; Grob, J.; Chibaudel, B.; et al. High Level of Activity of Nivolumab Anti-PD-1 Immunotherapy and Favorable Outcome in Metastatic/Refractory MSI-H Non-Colorectal Cancer: Results of the MSI Cohort from the French AcSé Program. Ann. Oncol. 2019, 30, v506. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.-P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients with Noncolorectal High Microsatellite Instability/Mismatch Repair–Deficient Cancer: Results from the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch Repair Deficiency Predicts Response of Solid Tumors to PD-1 Blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, K.S.; Foster, N.R.; Overman, M.J.; Boland, P.M.; Kim, S.S.; Arrambide, K.A.; Jaszewski, B.L.; Bekaii-Saab, T.; Graham, R.P.; Welch, J.; et al. ZEBRA: A Multicenter Phase II Study of Pembrolizumab in Patients with Advanced Small-Bowel Adenocarcinoma. Clin. Cancer Res. 2021, 27, 3641–3648. [Google Scholar] [CrossRef] [PubMed]
- Cardin, D.B.; Whisenant, J.; Ayers, G.D.; Gilbert, J.; Dahlman, K.B.; Shi, C.; Berlin, J. Pilot study to test safety and efficacy of avelumab in small bowel adenocarcinoma (SBA). J. Clin. Oncol. 2020, 38, 797. [Google Scholar] [CrossRef]
- Patel, S.P.; Othus, M.; Chae, Y.K.; Giles, F.J.; Hansel, D.E.; Singh, P.P.; Fontaine, A.; Shah, M.H.; Kasi, A.; Al Baghdadi, T.; et al. A Phase II Basket Trial of Dual Anti–CTLA-4 and Anti–PD-1 Blockade in Rare Tumors (DART SWOG 1609) in Patients with Nonpancreatic Neuroendocrine Tumors. Clin. Cancer Res. 2020, 26, 2290–2296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, L.; Marabelle, A.; Kim, T.; Geva, R.; Van Cutsem, E.; André, T.; Ascierto, P.; Maio, M.; Delord, J.-P.; Gottfried, M.; et al. Efficacy of Pembrolizumab in Phase 2 KEYNOTE-164 and KEYNOTE-158 Studies of Microsatellite Instability High Cancers. Ann. Oncol. 2017, 28 (Suppl. S5), v128–v129. [Google Scholar] [CrossRef]
- Diaz, L.A.; Marabelle, A.; Delord, J.-P.; Shapira-Frommer, R.; Geva, R.; Peled, N.; Kim, T.W.; Andre, T.; Van Cutsem, E.; Guimbaud, R.; et al. Pembrolizumab therapy for microsatellite instability high (MSI-H) colorectal cancer (CRC) and non-CRC. J. Clin. Oncol. 2017, 35, 3071. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Kemberling, H.; Eyring, A.; Bartlett, B.; Goldberg, R.M.; Crocenzi, T.S.; Fisher, G.A.; Lee, J.J.; et al. PD-1 blockade in mismatch repair deficient non-colorectal gastrointestinal cancers. J. Clin. Oncol. 2016, 34, 195. [Google Scholar] [CrossRef]
- Diaz, L.A.; Uram, J.N.; Wang, H.; Bartlett, B.; Kemberling, H.; Eyring, A.; Azad, N.S.; Dauses, T.; Laheru, D.; Lee, J.J.; et al. Programmed death-1 blockade in mismatch repair deficient cancer independent of tumor histology. J. Clin. Oncol. 2016, 34, 3003. [Google Scholar] [CrossRef]


{kind=link}
| Year | N° pts | Study Type | Treatment | Setting | Primary Outcome | Other Outcomes | Reference | |
|---|---|---|---|---|---|---|---|---|
| Chemotherapy | ||||||||
| McWilliams R.R. et al. | 2017 | 33 | phase II | CAPIRINOX (dose on UGT1A1*28 genotype) | I line | ORR 37.5% (IC 95% n.r) | mOS 13.4 m mPFS 8.9 m | [7] |
| Gibson M.K. et al. | 2005 | 39 | phase II | Fluorouracil + Mitomycine C + Doxorubicine | I line/pretreated | ORR 18% (IC 95% 7.8–34.4) | mOS 8 m | [8] |
| Overman M.J. et al. | 2009 | 31 | phase II | CAPOX | I line | ORR 50% (IC 95% 31–69) | mTTP 9.4 m/ mOS 20.4 m | [9] |
| Kim H.S. et al. | 2013 | 21 | phase II | XELOX | I line | TTP 7.6 m (IC 95% 6.7–8.5) | mOS 19.7 m/ ORR 38% (2 CR) | [10] |
| Horimatsu T. et al. | 2017 | 24 | phase II | mFOLFOX | I line | 1y PFS 23.3% (IC 95% 8.6–44.2%) | mOS 17.3 m/ ORR 45%/ mPFS 5.9 m | [11] |
| Xiang X.J. et al. | 2012 | 33 | phase II | mFOLFOX | I line | ORR 48.5% (95% CI 31–67%) | mTTP 7.8 m/ mOS 15.2 m | [12] |
| Overman M.J. et al. | 2018 | 10 | phase II | Nab-paclitaxel | II line or later line | 2 PR (10 pts) | // | [13] |
| Biologics | ||||||||
| Gulathi P. et al. | 2017 | 30 | phase II | CAPOX + Bevacizumab | I line | PFS 8.7 m | mOS 12.9 m/ORR 43–50% | [14] |
| Overman et al. | 2019 | ongoing | phase II | Paclitaxel/Ramucirumab vs FOLFIRI | II line | PFS | OS, ORR, safety, CEA | [15] |
| Gulathi P. et al. | 2018 | 9 | phase II | Panitumumab single agent | pretreated | early stopped after 9 pts RR 0% | mPFS 2.4 m/mOS 5.7 m | [16] |
| Subbiah V. et al. | 2016 | ongoing | phase II basket | Dabrafenib + Trametinib for BRAF V600 mutant | pretreated | ORR | DOR, PFS, OS, safety | [17] |
| Hainsworth J.D. | 2018 | ongoing | phase IIa basket | Pertuzumab plus Trastuzumab, Erlotinib, Vemurafenib or Vismodegib (target-based) | pretreated | ORR 0% | [18] | |
| Immunotherapy | ||||||||
| Tournigand C. | 2019 | 50 MSI-H (7 SBA) | phase II | Nivolumab | All lines | ORR 38% (95% CI: 24.6% to 52.8%) | DCR 74%. 6 mo mPFS 58.9% | [19] |
| Marabelle A. | 2020 | 233 MSI-H non-CRC (19 SBA) | phase II | Pembrolizumab | pretreated | ORR 42.1% (95% CI: 20.3–66.5%). | mPFS 9.2 mo. mOS not reached 14.6% SAE | [20] |
| Dung T. Le | 2017 | 46 MMRd non-CRC (5 SBA) | phase II | Pembrolizumab | pretreated | ORR 54% (95% CI: 39–69%) | DCR 72% (95% CI: 57–84%) mPFS 18.1 mo 2 y OS 57% | [21] |
| Pedersen K. | 2021 | MSI tumors | phase II | Pembrolizumab | pretreated | ORR 8% | mOS 7.1 mo mPFS 2.8 mo sAE > G2 63% | [22] |
| Cardin D. et al. | 2020 | 8 | phase II | Avelumab | All lines | ORR 29% | DCR 71% mPFS 8.0 mo | [23] |
| Patel S.P. et al. | 2020 | 25 | phase II basket | Ipilimumab/Nivolumab | pretreated | ORR 8% | mPFS 2 mo 6 mo OS 48% mOS 6 mo | [24] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Nardo, P.; Garattini, S.K.; Torrisi, E.; Fanotto, V.; Miolo, G.; Buonadonna, A.; Puglisi, F. Systemic Treatments for Advanced Small Bowel Adenocarcinoma: A Systematic Review. Cancers 2022, 14, 1502. https://doi.org/10.3390/cancers14061502
Di Nardo P, Garattini SK, Torrisi E, Fanotto V, Miolo G, Buonadonna A, Puglisi F. Systemic Treatments for Advanced Small Bowel Adenocarcinoma: A Systematic Review. Cancers. 2022; 14(6):1502. https://doi.org/10.3390/cancers14061502
Chicago/Turabian StyleDi Nardo, Paola, Silvio Ken Garattini, Elena Torrisi, Valentina Fanotto, Gianmaria Miolo, Angela Buonadonna, and Fabio Puglisi. 2022. "Systemic Treatments for Advanced Small Bowel Adenocarcinoma: A Systematic Review" Cancers 14, no. 6: 1502. https://doi.org/10.3390/cancers14061502
APA StyleDi Nardo, P., Garattini, S. K., Torrisi, E., Fanotto, V., Miolo, G., Buonadonna, A., & Puglisi, F. (2022). Systemic Treatments for Advanced Small Bowel Adenocarcinoma: A Systematic Review. Cancers, 14(6), 1502. https://doi.org/10.3390/cancers14061502