
Feasibility of a Multimodal Prehabilitation Programme in Patients Undergoing Cytoreductive Surgery for Advanced Ovarian Cancer: A Pilot Study

 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Enhanced Recovery after Surgery Program
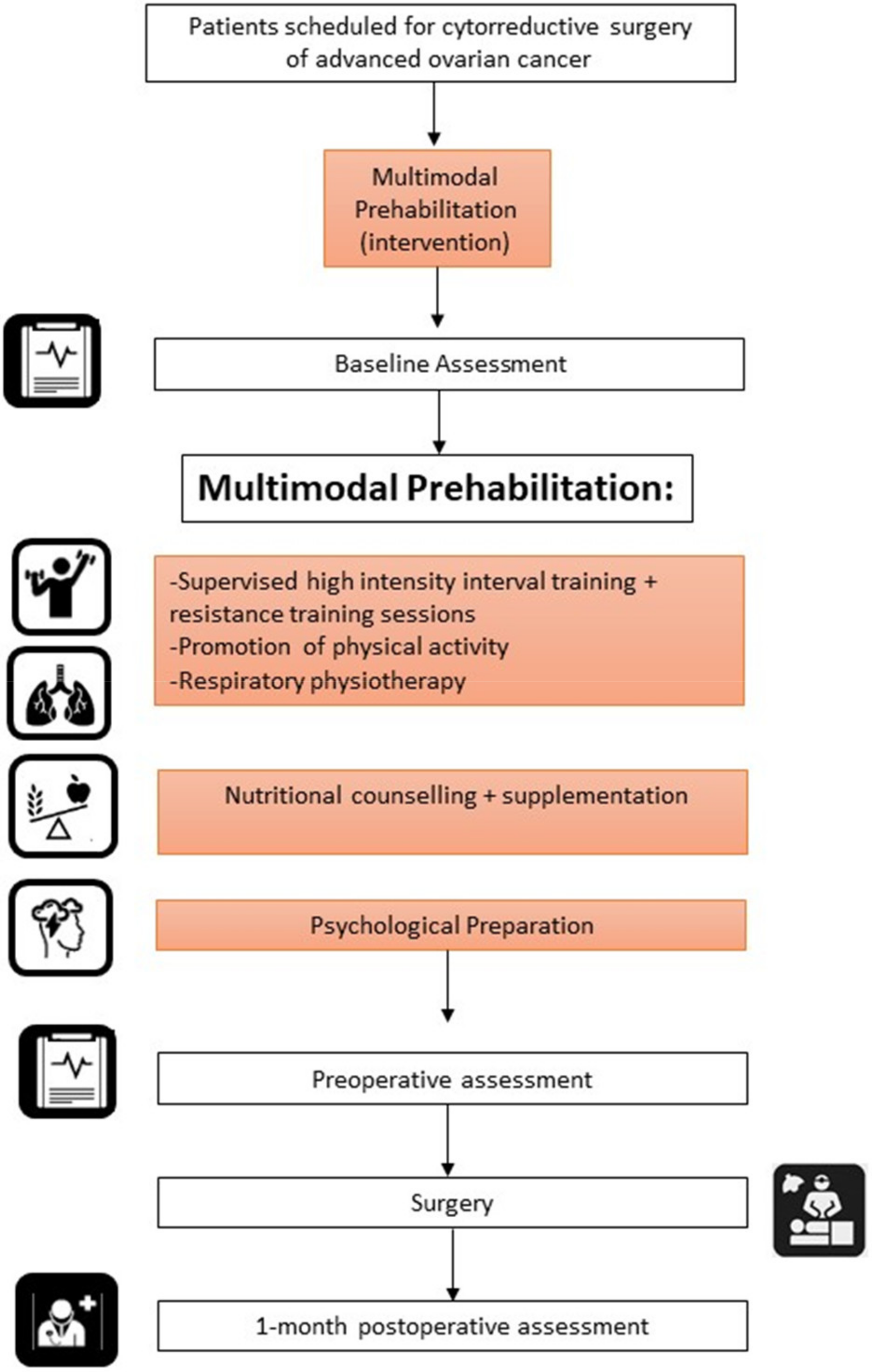
2.3. Prehabilitation Cohort: Multimodal Prehabilitation Programme
2.4. Control Cohort
2.5. Basal Health Status Assessment
2.6. Surgery and Postoperative Follow-Up Assessment
2.7. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Adherence to The Prehabilitation Program
3.3. Surgical Results
4. Discussion
4.1. Summary of Main Results
4.2. Results in the Context of Published Literature
4.3. Strengths and Weaknesses
4.4. Implications for Practice and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kehoe, S.; Hook, J.; Nankivell, M.; Jayson, G.C.; Kitchener, H.; Lopes, T.; Luesley, D.; Perren, T.; Bannoo, S.; Mascarenhas, M.; et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): An open-label, randomised, controlled, non-inferiority trial. Lancet 2015, 386, 249–257. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Janco, J.M.; Mariani, A.; Bakkum-Gamez, J.N.; Langstraat, C.L.; Weaver, A.L.; McGree, M.E.; Cliby, W.A. Risk-prediction model of severe postoperative complications after primary debulking surgery for advanced ovarian cancer. Gynecol. Oncol. 2016, 140, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Fagotti, A.; Ferrandina, G.; Vizzielli, G.; Fanfani, F.; Gallotta, V.; Chiantera, V.; Costantini, B.; Margariti, P.A.; Gueli Alletti, S.; Cosentino, F.; et al. Phase III randomised clinical trial comparing primary surgery versus neoadjuvant chemotherapy in advanced epithelial ovarian cancer with high tumour load (SCORPION trial): Final analysis of peri-operative outcome. Eur. J. Cancer 2016, 59, 22–33. [Google Scholar] [CrossRef]
- Vergote, I.; Tropé, C.G.; Amant, F.; Kristensen, G.B.; Ehlen, T.; Johnson, N.; Verheijen, R.H.; van der Burg, M.E.; Lacave, A.J.; Panici, P.B.; et al. Neoadjuvant Chemotherapy or Primary Surgery in Stage IIIC or IV Ovarian Cancer. N. Engl. J. Med. 2010, 363, 943–953. [Google Scholar] [CrossRef] [Green Version]
- Benedetti Panici, P.; Di Donato, V.; Fischetti, M.; Casorelli, A.; Perniola, G.; Musella, A.; Marchetti, C.; Palaia, I.; Berloco, P.; Muzii, L. Predictors of postoperative morbidity after cytoreduction for advanced ovarian cancer: Analysis and management of complications in upper abdominal surgery. Gynecol. Oncol. 2015, 137, 406–411. [Google Scholar] [CrossRef]
- Seagle, B.L.; Butler, S.K.; Strohl, A.E.; Nieves-Neira, W.; Shahabi, S. Gynecologic Oncology Chemotherapy delay after primary debulking surgery for ovarian cancer. Gynecol. Oncol. 2016, 144, 260–265. [Google Scholar] [CrossRef]
- Wilson, R.J.T.; Davies, S.; Yates, D.; Redman, J.; Stone, M. Impaired functional capacity is associated with all-cause mortality after major elective intra-abdominal surgery. Br. J. Anaesth. 2010, 105, 297–303. [Google Scholar] [CrossRef] [Green Version]
- Gillis, C.; Carli, F. Promoting perioperative metabolic and nutritional care. Anesthesiology 2015, 123, 1455–1472. [Google Scholar] [CrossRef] [Green Version]
- Nelson, G.; Bakkum-gamez, J.; Kalogera, E.; Glaser, G.; Altman, A.; Meyer, L.A.; Taylor, J.S.; Iniesta, M.; Lasala, J.; Mena, G.; et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery ( ERAS ) Society recommendations—2019 update. Int. J. Gynecol. Cancer 2019, 29, 651–668. [Google Scholar] [CrossRef]
- Luther, A.; Gabriel, J.; Watson, R.P.; Francis, N.K. The Impact of Total Body Prehabilitation on Post-Operative Outcomes After Major Abdominal Surgery: A Systematic Review. World J. Surg. 2018, 42, 2781–2791. [Google Scholar] [CrossRef] [PubMed]
- Moran, J.; Guinan, E.; McCormick, P.; Larkin, J.; Mockler, D.; Hussey, J.; Moriarty, J.; Wilson, F. The ability of prehabilitation to influence postoperative outcome after intra-abdominal operation: A systematic review and meta-analysis. Surgery 2016, 160, 1189–1201. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.J.; Hackney, R.J.; Lamb, P.J.; Wigmore, S.J.; Deans, D.A.C.; Skipworth, R.J.E. Prehabilitation Before Major Abdominal Surgery: A Systematic Review and Meta-analysis. World J. Surg. 2019, 43, 1661–1668. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; Tahir, M.R.; Bongers, B.C.; Kallen, V.L.; Slooter, G.D.; van Meeteren, N.L. Prehabilitation before major intra-abdominal cancer surgery: A systematic review of randomised controlled trials. Eur. J. Anaesthesiol. 2019, 36, 933–945. [Google Scholar] [CrossRef]
- Schneider, S.; Armbrust, R.; Spies, C.; du Bois, A.; Sehouli, J. Prehabilitation programs and ERAS protocols in gynecological oncology: A comprehensive review. Arch. Gynecol. Obstet. 2020, 301, 315–326. [Google Scholar] [CrossRef]
- Carli, F.; Brown, R. Prehabilitation to enhance postoperative recovery for an octogenarian following robotic-assisted hysterectomy with endometrial cancer. Can. J. Anaesth. 2012, 59, 779–784. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sport Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Keller, H.; de van der Schueren, M.A.E.; Jensen, G.L.; Barazzoni, R.; Compher, C.; Correia, M.I.T.D.; Gonzalez, M.C.; Jager-Wittenaar, H.; Pirlich, M.; Steiber, A.; et al. Global Leadership Initiative on Malnutrition (GLIM): Guidance on Validation of the Operational Criteria for the Diagnosis of Protein-Energy Malnutrition in Adults. J. Parenter Enter Nutr. 2020, 44, 992–1003. [Google Scholar] [CrossRef]
- Snaith, R.P. The hospital anxiety and depression scale. Health Qual. Life Outcomes 2003, 1, 6–9. [Google Scholar] [CrossRef] [Green Version]
- Aletti, G.D.; Santillan, A.; Eisenhauer, E.L.; Hu, J.; Aletti, G.; Podratz, K.C.; Bristow, R.E.; Chi, D.S.; Cliby, W.A. A new frontier for quality of care in gynecologic oncology surgery: Multi-institutional assessment of short-term outcomes for ovarian cancer using a risk-adjusted model. Gynecol. Oncol. 2007, 107, 99–106. [Google Scholar] [CrossRef]
- European Society of Gynaecological Oncology. ESGO Ovarian Cancer OPERATIVE REPORT ESGO Guidelines. Available online: https://www.esgo.org/media/2016/10/ESGO-Operative-Report.pdf (accessed on 3 January 2022).
- Slankamenac, K.; Graf, R.; Barkun, J.; Clavien, P. The Comprehensive Complication Index. Ann. Surg. 2013, 258, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillis, C.; Li, C.; Lee, L.; Awasthi, R.; Augustin, B.; Gamsa, A.; Liberman, A.S.; Stein, B.; Charlebois, P.; Feldman, L.S.; et al. Prehabilitation versus Rehabilitation: A Randomized Control Trial in Patients Undergoing Colorectal Resection for Cancer. Anesthesiology 2014, 121, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Aida, M.; Federico, A.; Mathilde, M.; Carlos, D.; Gómez, M.; Daix, M.; Bétrian, S.; Gabiache, E.; Balagué, G.; Leclerc, S.; et al. Concordance of laparoscopic and laparotomic peritoneal cancer index using a two-step surgical protocol to select patients for cytoreductive surgery in advanced ovarian cancer. Arch. Gynecol. Obstet. 2021, 303, 1295–1304. [Google Scholar] [CrossRef]
- Jie, B.; Jiang, Z.M.; Nolan, M.T.; Zhu, S.N.; Yu, K.; Kondrup, J. Impact of preoperative nutritional support on clinical outcome in abdominal surgical patients at nutritional risk. Nutrition 2012, 28, 1022–1027. [Google Scholar] [CrossRef]
- Waitzberg, D.L.; Saito, H.; Plank, L.D.; Jamieson, G.G.; Jagannath, P.; Hwang, T.; Mijares, J.M.; Bihari, D. Postsurgical Infections are Reduced with Specialized Nutrition Support. World J. Surg. 2006, 30, 1592–1604. [Google Scholar] [CrossRef]
- Powell, R.; Scott, N.W.; Manyande, A.; Bruce, J.; Vögele, C.; Byrne-Davis, L.M.T.; Unsworth, M.; Osmer, C.; Johnston, M. Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. Cochrane Database Syst. Rev. 2016, 5, CD008646. [Google Scholar] [CrossRef]
- Carli, F.; Charlebois, P.; Stein, B.; Feldman, L.; Zavorsky, G.; Kim, D.J.; Scott, S.; Mayo, N.E. Randomized clinical trial of prehabilitation in colorectal surgery. Br. J. Surg. 2010, 97, 1187–1197. [Google Scholar] [CrossRef]
- Dronkers, J.J.; Lamberts, H.; Reutelingsperger, I.M.; Naber, R.H.; Dronkers-Landman, C.M.; Veldman, A.; van Meeteren, N.L. Preoperative therapeutic programme for elderly patients scheduled for elective abdominal oncological surgery: A randomized controlled pilot study. Clin. Rehabil. 2010, 24, 614–622. [Google Scholar] [CrossRef]
- Barberan-Garcia, A.; Ubré, M.; Roca, J.; Lacy, A.M.; Burgos, F.; Risco, R.; Momblán, D.; Balust, J.; Blanco, I.; Martínez-Pallí, G. Personalised Prehabilitation in High-risk Patients Undergoing Elective Major Abdominal Surgery: A Randomized Blinded Controlled Trial. Ann. Surg. 2018, 267, 50–56. [Google Scholar] [CrossRef]
- Dholakia, J.; Cohn, D.E.; Straughn, J.M.; Dilley, S.E. Prehabilitation for medically frail patients undergoing surgery for epithelial ovarian cancer: A cost-effectiveness analysis. J. Gynecol. Oncol. 2021, 32, e92. [Google Scholar] [CrossRef]
- Heger, P.; Probst, P.; Wiskemann, J.; Steindorf, K.; Diener, M.K.; Mihaljevic, A.L. A Systematic Review and Meta-analysis of Physical Exercise Prehabilitation in Major Abdominal Surgery (PROSPERO 2017 CRD42017080366). J. Gastrointest Surg. 2020, 24, 1375–1385. [Google Scholar] [CrossRef] [PubMed]
- Mina, D.S.; Clarke, H.; Ritvo, P.; Leung, Y.W.; Matthew, A.G.; Katz, J.; Trachtenberg, J.; Alibhai, S.M. Effect of total-body prehabilitation on postoperative outcomes: A systematic review and meta-analysis. Physiotherapy 2014, 100, 196–207. [Google Scholar] [CrossRef] [PubMed]
- Mahner, S.; Eulenburg, C.; Staehle, A.; Wegscheider, K.; Reuss, A.; Pujade-Lauraine, E.; Harter, P.; Ray-Coquard, I.; Pfisterer, J.; du Bois, A. Prognostic impact of the time interval between surgery and chemotherapy in advanced ovarian cancer: Analysis of prospective randomised phase III trials. Eur. J. Cancer 2013, 49, 142–149. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Prehabilitation Cohort | Control Cohort | p-Value |
|---|---|---|---|
| n = 15 | n = 19 | ||
| Age (years), median [IQR] | 55 (52–69) | 60 (52–72) | 0.5 |
| Body mass index (kg/m2), median [IQR] | 25 (23–26) | 24 (24–26) | 0.36 |
| Charlson Comorbidity Index, median [IQR] | 4 (3–5) | 4 (3–6) | 0.8 |
| ECOG, n (%) | |||
| 0 | 10 | 6 | 0.08 |
| 1 | 5 | 13 | |
| CA 125, median [IQR] | 30 (16–166) | 76 (30–585) | 0.09 |
| Preoperative albumin (g/L), median [IQR] | 44 (43–46) | 44 (36–46) | 0.3 |
| FIGO staging, N (%) | 0.029 | ||
| III B | 1 (6.7) | 0 (0) | |
| III C | 5 (33.4) | 12 (63.2) | |
| IV A | 4 (26.7) | 0 (0) | |
| IVB | 5 (33.4) | 7 (36.8) | |
| Histology, n (%) | |||
| Low-grade serous carcinoma | 1 (6.7) | 2 (10.5) | |
| High-grade serous carcinoma | 12 (80) | 16 (84.2) | |
| Endometrioid carcinoma | 1 (6.7) | 1 (5.3) | 0.87 |
| Granulosa cell tumour | 1(6.7) | 0 (0) | |
| Duration of surgery (min), median [IQR] | 320 (255–280) | 310 (270–260) | 0.4 |
| PCI, median [IQR] | 10 (8–14) | 10 (8–14) | 0.97 |
| Type of surgery, n (%) | |||
| Primary cytoreduction surgery | 1 (6.7) | 7 (36.8) | |
| Interval debulking surgery | 11 (73.3) | 11 (57.9) | 0.21 |
| Secondary or tertiary cytoreduction | 3 (0.2) | 1 (5.2) | |
| Procedure, n (%) | |||
| Hysterectomy + bilateral salpingo-oophorectomy | 11 (73.3) | 18 (94.73) | 0.14 |
| Pelvic peritonectomy | 6 (40) | 5 (26.31) | 0.475 |
| Intestinal resection | 7 (46.66) | 10 (52.63) | 1 |
| Colorectal resection | 5 | 3 | 1 |
| Large bowel resection | 3 | 5 | 1 |
| Small bowel resection | 3 | 5 | 0.69 |
| Appendectomy | 4 (26.67) | 6 (31.58) | 1 |
| Radical omentectomy | 12 (80) | 17 (89.47) | 0.63 |
| Partial hepatectomy | 1 (6.67) | 0 (0) | 0.44 |
| Splenectomy | 2 (13.3) | 1 (5.26) | 0.57 |
| Diaphragmatic stripping | 7 (46.67) | 4 (21.05) | 0.15 |
| HIPEC | 1 (7.14) | 1 (5.26) | 1 |
| Debulking of pelvic/paraaortic lymph nodes | 10 (66.67) | 14 (77.78) | 0.69 |
| Aletti Complexity Score, median [IQR] | 6 (4–8) | 7 (4–8) | 0.51 |
| Residual disease, n (%) | |||
| R0 | 13 (86) | 19 (100) | |
| R1 | 1 (6.7) | 0 (0) | 0.18 |
| R2 | 1 (6.7) | 0 (0) |
| Characteristics | Prehabilitation Cohort |
|---|---|
| Duration of programme (weeks), median weeks [IQR] | 2 (2,3) |
| Number of gym sessions, median [IQR] | 6 (4–8) |
| Adherence to gym sessions: Patients completing >2 sessions or >75% of scheduled sessions, n (%) | 13 (86.6) |
| Adherence (%), median [IQR] | 83 (60–100) |
| Adverse effects, n (%) | 3/15 (20) |
| Mild dizziness | 3/15 (20) |
| Adherence to nutrition intervention >75%, n (%) | 15 (100) |
| Adherence to psychological intervention ≥1 session, n (%) | 12 (80) |
| Characteristics | Prehabilitation Cohort | Control Cohort | p-Value |
|---|---|---|---|
| n = 15 | n = 19 | ||
| Hospital stay (days), median [IQR] | 5 (4–6) | 7 (5–9) | 0.041 |
| Intensive care unit stay, days (%) | |||
| 0 | 9 (60) | 9 (47.4) | |
| 1 | 5 (33.3) | 6 (31.6) | |
| 2 | 1 (6.7) | 3 (15.8) | 0.88 |
| 3 | 0 (0) | 1 (5.3) | |
| Preoperative prealbumin (g/L), median [IQR] | 0.235 (0.214–0.316) | 0.180 (0.13–0.23) | 0.007 |
| Intraoperative complications, n (%) | |||
| Intestinal injury | 0 (0) | 1 (5.3) | |
| Vascular injury | 0 (0) | 0 (0) | |
| Urological injury | 0 (0) | 0 (0) | 0.40 |
| Nerve injury | 0 (0) | 0 (0) | |
| Need for blood transfusion | 1 (6.7) | 5 (26.3) | |
| CCI, median [IQR] | 0 (0–20.9) | 8, 66 (0–33.5) | 0.20 |
| CCI Mean, SD | 9, 33 (12.1) | 16, 62 (16.9) | 0.08 |
| Clavien–Dindo classification <30 days, median [IQR] | |||
| Patients with ≥1 complication | 6 (40) | 12 (63.15) | |
| I | 4 (40) | 4 (23.5) | 0.30 |
| II | 6 (60) | 8 (47) | |
| III a | 0 (0) | 2 (11.8) | |
| III b | 0 (0) | 2 (11.8) | |
| IV a | 0 (0) | 1 (5.9) | |
| IV b | 0 (0) | 0 (0) | |
| V | 0 (0) | 0 (0) | |
| Major complications (Clavien–Dindo ≥ III), n (%) | |||
| No | 15 (100) | 14 (73.7) | 0.053 |
| Yes | 0 (0) | 5 (26.3) | |
| Type of complications, n (%) | |||
| Paralytic ileus/intestinal obstruction | 4 (40) | 1 (5.3) | |
| Cardiovascular complications | 0 (0) | 1(5.3) | |
| Pulmonary complications/DVT/PE | 0 (0) | 0 (0) | |
| Anastomotic leakage/peritonitis | 0 (0) | 0 (0) | |
| Infection/postsurgical abscess | 3 (30) | 5 (26.3) | 0.714 |
| Postsurgical bleeding/need for transfusion | 2 (20) | 9 (47.3) | |
| Lymphocele/lymphatic complications | 0 (0) | 3 (15.8) | |
| Time to starting chemotherapy (days), median [IQR] | 25 (23–35) | 35 (28–45) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz-Feijoo, B.; Agusti-Garcia, N.; Sebio, R.; López-Hernández, A.; Sisó, M.; Glickman, A.; Carreras-Dieguez, N.; Fuste, P.; Marina, T.; Martínez-Egea, J.; et al. Feasibility of a Multimodal Prehabilitation Programme in Patients Undergoing Cytoreductive Surgery for Advanced Ovarian Cancer: A Pilot Study. Cancers 2022, 14, 1635. https://doi.org/10.3390/cancers14071635
Diaz-Feijoo B, Agusti-Garcia N, Sebio R, López-Hernández A, Sisó M, Glickman A, Carreras-Dieguez N, Fuste P, Marina T, Martínez-Egea J, et al. Feasibility of a Multimodal Prehabilitation Programme in Patients Undergoing Cytoreductive Surgery for Advanced Ovarian Cancer: A Pilot Study. Cancers. 2022; 14(7):1635. https://doi.org/10.3390/cancers14071635
Chicago/Turabian StyleDiaz-Feijoo, Berta, Nuria Agusti-Garcia, Raquel Sebio, Antonio López-Hernández, Marina Sisó, Ariel Glickman, Nuria Carreras-Dieguez, Pere Fuste, Tiermes Marina, Judit Martínez-Egea, and et al. 2022. "Feasibility of a Multimodal Prehabilitation Programme in Patients Undergoing Cytoreductive Surgery for Advanced Ovarian Cancer: A Pilot Study" Cancers 14, no. 7: 1635. https://doi.org/10.3390/cancers14071635
APA StyleDiaz-Feijoo, B., Agusti-Garcia, N., Sebio, R., López-Hernández, A., Sisó, M., Glickman, A., Carreras-Dieguez, N., Fuste, P., Marina, T., Martínez-Egea, J., Aguilera, L., Perdomo, J., Pelaez, A., López-Baamonde, M., Navarro-Ripoll, R., Gimeno, E., Campero, B., Torné, A., Martinez-Palli, G., & Arguis, M. J. (2022). Feasibility of a Multimodal Prehabilitation Programme in Patients Undergoing Cytoreductive Surgery for Advanced Ovarian Cancer: A Pilot Study. Cancers, 14(7), 1635. https://doi.org/10.3390/cancers14071635