
Patients with Positive Lymph Nodes after Radical Prostatectomy and Pelvic Lymphadenectomy—Do We Know the Proper Way of Management?

 ,
,  , ,
, , 
 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
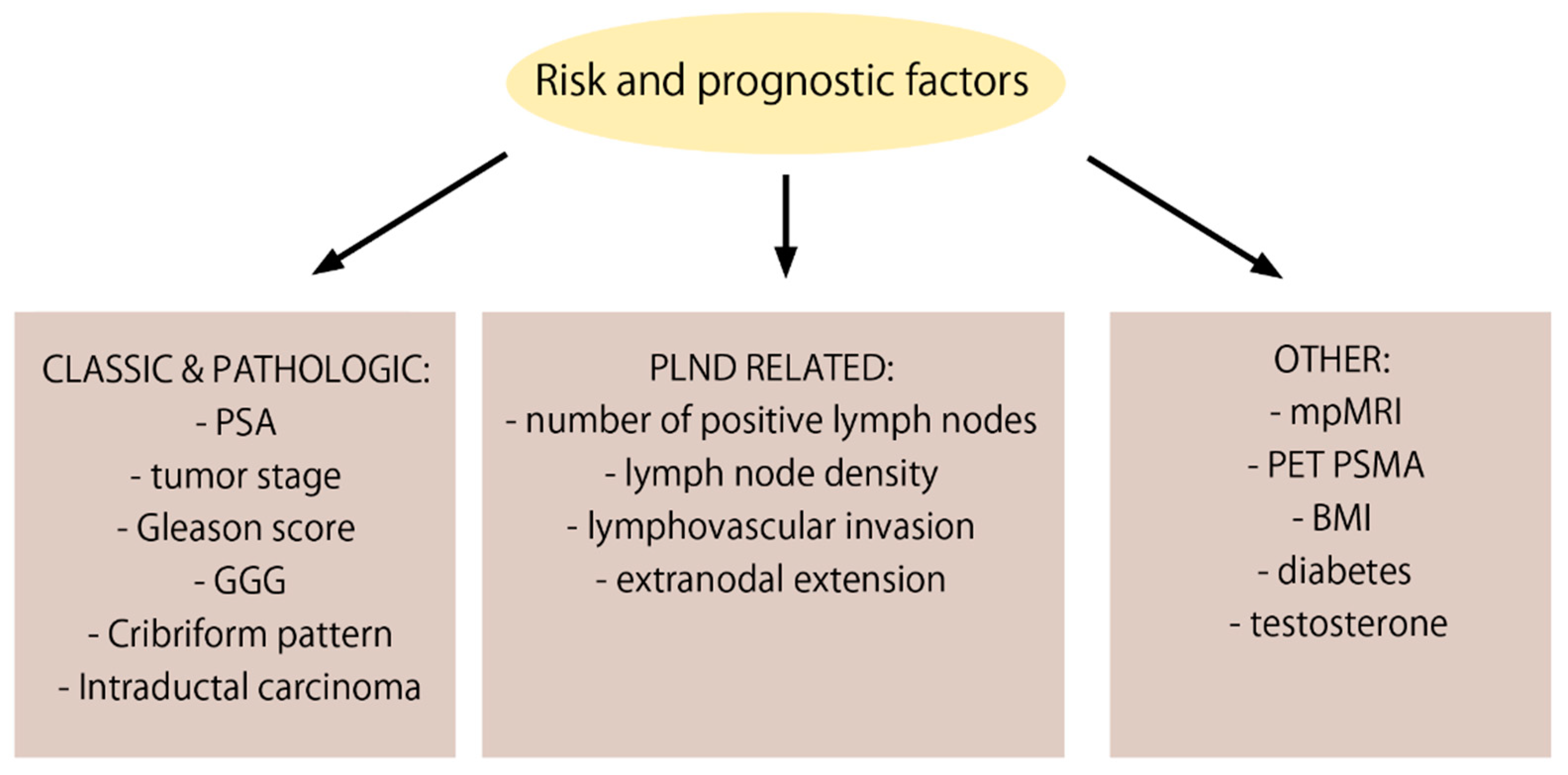
2. Risk and Prognostic Factors for Nodal Involvement
2.1. PSA
2.2. T—Tumor Stage
2.3. ECE—Extracapsular Extension
2.4. GS—Gleason SCORE
2.5. GGG—Gleason Grade Group
2.6. Cribriform Pattern
2.7. IDC—Intraductal Carcinoma
2.8. pN—Pathological Node Stage
2.9. LND—Lymph Node Density
2.10. LVI—Lymphovascular Invasion
2.11. ENE—Extranodal Extension
2.12. mpMRI
2.13. PSMA PET
2.14. Obesity—Higher Body Mass Index (BMI)
2.15. Diabetes
2.16. Testosterone
3. Impact of PLND
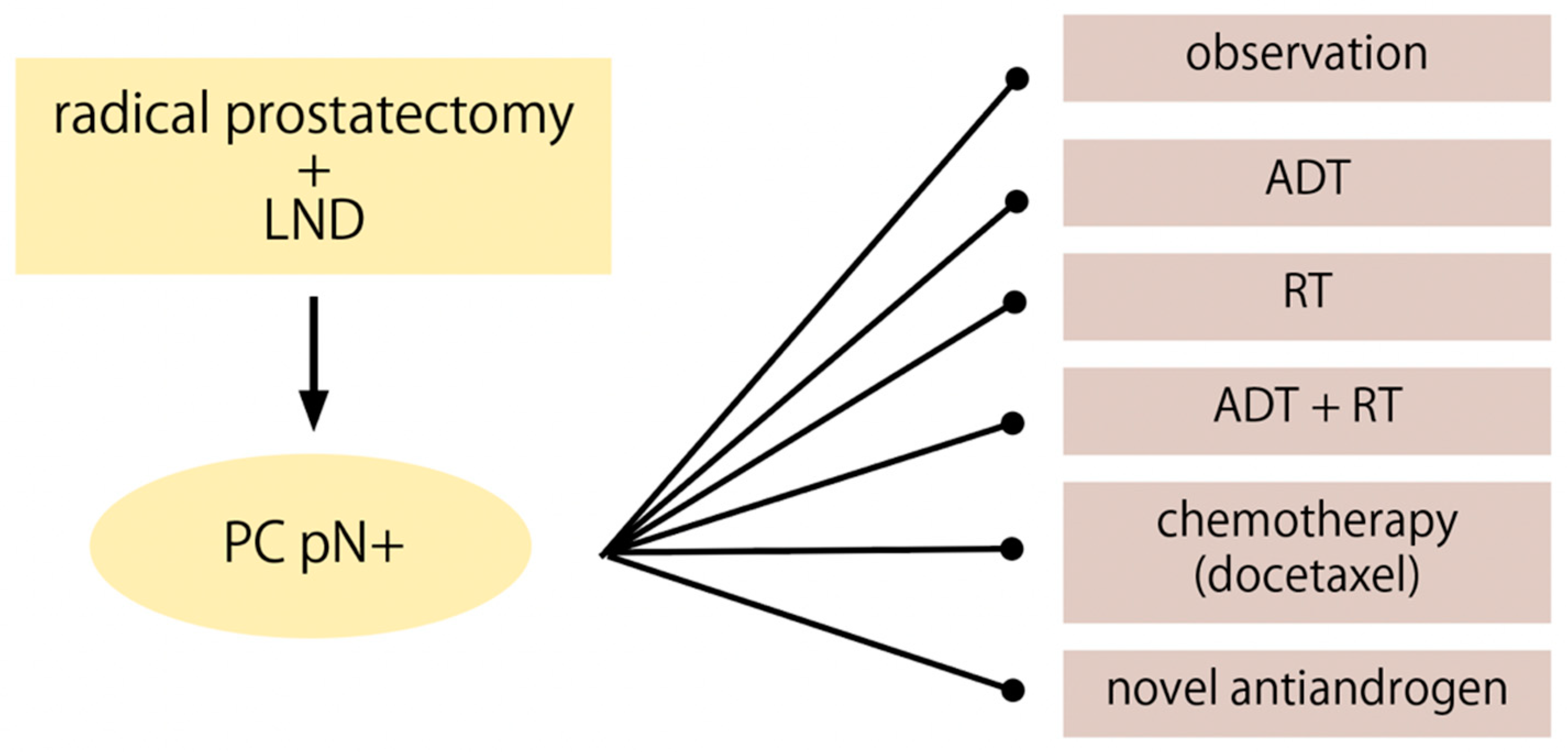
4. pN+ Management Options
4.1. Observation
4.2. ADT
4.3. RT and ADT
4.4. Docetaxel and New Antiandrogens (Abiraterone Acetate, Enzalutamide, Apalutamide)
5. Current Guidelines
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Engels, S.; Brautmeier, L.; Reinhardt, L.; Wasylow, C.; Hasselmann, F.; Henke, R.P.; Wawroschek, F.; Winter, A. Evaluation of Fast Molecular Detection of Lymph Node Metastases in Prostate Cancer Patients Using One-Step Nucleic Acid Amplification (Osna). Cancers 2021, 13, 1117. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.N.; Shoag, J.E.; Golan, R.; Halpern, J.A.; Schaeffer, E.M.; Hsu, W.C.; Nguyen, P.L.; Sedrakyan, A.; Chen, R.C.; Eggener, S.E.; et al. Contemporary Incidence and Outcomes of Prostate Cancer Lymph Node Metastases. J. Urol. 2018, 199, 1510–1517. [Google Scholar] [CrossRef] [PubMed]
- Touijer, K.A.; Mazzola, C.R.; Sjoberg, D.D.; Scardino, P.T.; Eastham, J.A. Long-Term Outcomes of Patients with Lymph Node Metastasis Treated with Radical Prostatectomy without Adjuvant Androgen-Deprivation Therapy. Eur. Urol. 2014, 65, 20–25. [Google Scholar] [CrossRef]
- Swanson, G.P.; Riggs, M.; Hermans, M. Pathologic Findings at Radical Prostatectomy: Risk Factors for Failure and Death. Urol. Oncol. Semin. Orig. Investig. 2007, 25, 110–114. [Google Scholar] [CrossRef]
- Gonzalez, C.M.; Roehl, K.A.; Antenor, J.V.; Blunt, L.W.; Han, M.; Catalona, W.J. Preoperative PSA Level Significantly Associated with Interval to Biochemical Progression after Radical Retropubic Prostatectomy. Urology 2004, 64, 723–728. [Google Scholar] [CrossRef]
- Briganti, A.; Larcher, A.; Abdollah, F.; Capitanio, U.; Gallina, A.; Suardi, N.; Bianchi, M.; Sun, M.; Freschi, M.; Salonia, A.; et al. Updated Nomogram Predicting Lymph Node Invasion in Patients with Prostate Cancer Undergoing Extended Pelvic Lymph Node Dissection: The Essential Importance of Percentage of Positive Cores. Eur. Urol. 2012, 61, 480–487. [Google Scholar] [CrossRef]
- Tosco, L.; Devos, G.; De Coster, G.; Roumeguère, T.; Everaerts, W.; Quackels, T.; Dekuyper, P.; Van Cleynenbreugel, B.; Van Damme, N.; Van Eycken, E.; et al. Development and External Validation of a Nomogram to Predict Lymph Node Invasion after Robot Assisted Radical Prostatectomy. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 37.e11–37.e20. [Google Scholar] [CrossRef]
- Wei, L.; Huang, Y.; Chen, Z.; Lei, H.; Qin, X.; Cui, L.; Zhuo, Y. Artificial Intelligence Combined with Big Data to Predict Lymph Node Involvement in Prostate Cancer: A Population-Based Study. Front. Oncol. 2021, 11, 4148. [Google Scholar] [CrossRef]
- Laine, C.; Gandaglia, G.; Valerio, M.; Heidegger, I.; Tsaur, I.; Olivier, J.; Ceci, F.; van den Bergh, R.C.N.; Kretschmer, A.; Thibault, C.; et al. Features and Management of Men with PN1 CM0 Prostate Cancer after Radical Prostatectomy and Lymphadenectomy: A Systematic Review of Population-Based Evidence. Curr. Opin. Urol. 2022, 32, 69–84. [Google Scholar] [CrossRef]
- Zareba, P.; Eastham, J.; Scardino, P.T.; Touijer, K. Contemporary Patterns of Care and Outcomes of Men Found to Have Lymph Node Metastases at the Time of Radical Prostatectomy. J. Urol. 2017, 198, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Di Trapani, E.; Luzzago, S.; Peveri, G.; Catellani, M.; Ferro, M.; Cordima, G.; Mistretta, F.A.; Bianchi, R.; Cozzi, G.; Alessi, S.; et al. A Novel Nomogram Predicting Lymph Node Invasion among Patients with Prostate Cancer: The Importance of Extracapsular Extension at Multiparametric Magnetic Resonance Imaging. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 431.e15–431.e22. [Google Scholar] [CrossRef] [PubMed]
- Porcaro, A.B.; De Luyk, N.; Corsi, P.; Sebben, M.; Tafuri, A.; Mattevi, D.; Processali, T.; Cerruto, M.A.; Brunelli, M.; Zecchini Antoniolli, S.; et al. Clinical Factors Predicting and Stratifying the Risk of Lymph Node Invasion in Localized Prostate Cancer. Urol. Int. 2017, 99, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Xu, N.; Ke, Z.-B.; Chen, Y.H.; Wu, Y.P.; Chen, S.H.; Wei, Y.; Zheng, Q.S.; Huang, J.B.; Li, X.D.; Xue, X.Y. Risk Factors for Pathologically Confirmed Lymph Nodes Metastasis in Patients with Clinical T2N0M0 Stage Prostate Cancer. Front. Oncol. 2020, 10, 1547. [Google Scholar] [CrossRef]
- Hollemans, E.; Verhoef, E.I.; Bangma, C.H.; Rietbergen, J.; Osanto, S.; Pelger, R.C.M.; van Wezel, T.; van der Poel, H.; Bekers, E.; Helleman, J.; et al. Cribriform Architecture in Radical Prostatectomies Predicts Oncological Outcome in Gleason Score 8 Prostate Cancer Patients. Mod. Pathol. 2021, 34, 184–193. [Google Scholar] [CrossRef]
- Kweldam, C.F.; Wildhagen, M.F.; Steyerberg, E.W.; Bangma, C.H.; Van Der Kwast, T.H.; Van Leenders, G.J.L.H. Cribriform Growth Is Highly Predictive for Postoperative Metastasis and Disease-Specific Death in Gleason Score 7 Prostate Cancer. Mod. Pathol. 2015, 28, 457–464. [Google Scholar] [CrossRef] [Green Version]
- Downes, M.R.; Xu, B.; van der Kwast, T.H. Gleason Grade Patterns in Nodal Metastasis and Corresponding Prostatectomy Specimens: Impact on Patient Outcome. Histopathology 2019, 75, 715–722. [Google Scholar] [CrossRef]
- Kimura, K.; Tsuzuki, T.; Kato, M.; Saito, A.M.; Sassa, N.; Ishida, R.; Hirabayashi, H.; Yoshino, Y.; Hattori, R.; Gotoh, M. Prognostic Value of Intraductal Carcinoma of the Prostate in Radical Prostatectomy Specimens. Prostate 2014, 74, 680–687. [Google Scholar] [CrossRef]
- Boorjian, S.A.; Thompson, R.H.; Siddiqui, S.; Bagniewski, S.; Bergstralh, E.J.; Karnes, R.J.; Frank, I.; Blute, M.L. Long-Term Outcome After Radical Prostatectomy for Patients with Lymph Node Positive Prostate Cancer in the Prostate Specific Antigen Era. J. Urol. 2007, 178, 864–871. [Google Scholar] [CrossRef]
- Briganti, A.; Karnes, J.R.; Da Pozzo, L.F.; Cozzarini, C.; Gallina, A.; Suardi, N.; Bianchi, M.; Freschi, M.; Doglioni, C.; Fazio, F.; et al. Two Positive Nodes Represent a Significant Cut-off Value for Cancer Specific Survival in Patients with Node Positive Prostate Cancer. A New Proposal Based on a Two-Institution Experience on 703 Consecutive N+ Patients Treated with Radical Prostatectomy, Extended Pelvic Lymph Node Dissection and Adjuvant Therapy. Eur. Urol. 2009, 55, 261–270. [Google Scholar] [CrossRef]
- Qin, X.; Han, C.; Zhang, H.; Dai, B.; Zhu, Y.; Shen, Y.; Zhu, Y.; Shi, G.; Ye, D. Outcomes of Patients with Lymph Node Metastasis Treated with Radical Prostatectomy and Adjuvant Androgen Deprivation Therapy in a Chinese Population: Results from a Cohort Study. World J. Surg. Oncol. 2015, 13, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolzenbach, L.F.; Knipper, S.; Mandel, P.; Ascalone, L.; Deuker, M.; Tian, Z.; Heinzer, H.; Tilki, D.; Maurer, T.; Graefen, M.; et al. Oncological Outcomes of Pathologically Organ-Confined, Lymph Node-Positive Prostate Cancer after Radical Prostatectomy. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 234.e1–234.e7. [Google Scholar] [CrossRef] [PubMed]
- Froehner, M.; Koch, R.; Farahzadi, S.; Heberling, U.; Borkowetz, A.; Twelker, L.; Baretton, G.B.; Wirth, M.P.; Thomas, C. Long-Term Mortality in Patients with Positive Lymph Nodes at the Time of Radical Prostatectomy. Urol. Int. 2019, 103, 427–432. [Google Scholar] [CrossRef]
- Daneshmand, S.; Quek, M.L.; Stein, J.P.; Lieskovsky, G.; Cai, J.; Pinski, J.; Skinner, E.C.; Skinner, D.G. Prognosis of Patients with Lymph Node Positive Prostate Cancer Following Radical Prostatectomy: Long-Term Results. J. Urol. 2004, 172, 2252–2255. [Google Scholar] [CrossRef] [PubMed]
- Passoni, N.M.; Abdollah, F.; Suardi, N.; Gallina, A.; Bianchi, M.; Tutolo, M.; Fossati, N.; Gandaglia, G.; Salonia, A.; Freschi, M.; et al. Head-to-Head Comparison of Lymph Node Density and Number of Positive Lymph Nodes in Stratifying the Outcome of Patients with Lymph Node-Positive Prostate Cancer Submitted to Radical Prostatectomy and Extended Lymph Node Dissection. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 29.e21–29.e28. [Google Scholar] [CrossRef] [PubMed]
- Loeb, S.; Roehl, K.A.; Yu, X.; Antenor, J.A.V.; Han, M.; Gashti, S.N.; Yang, X.J.; Catalona, W.J. Lymphovascular Invasion in Radical Prostatectomy Specimens: Prediction of Adverse Pathologic Features and Biochemical Progression. Urology 2006, 68, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Kwon, Y.; Kim, I. Risk Stratification for Disease Progression in PT3 Prostate Cancer after Robot-Assisted Radical Prostatectomy. Asian J. Androl. 2017, 19, 700–706. [Google Scholar] [CrossRef]
- Jiang, W.; Zhang, L.; Wu, B.; Zha, Z.; Zhao, H.; Jun, Y.; Jiang, Y. The Impact of Lymphovascular Invasion in Patients with Prostate Cancer Following Radical Prostatectomy and Its Association with Their Clinicopathological Features: An Updated PRISMA-Compliant Systematic Review and Meta-Analysis. Medicine 2018, 97, e13537. [Google Scholar] [CrossRef]
- Huang, Y.; Huang, H.; Pan, X.W.; Xu, D.F.; Cui, X.G.; Chen, J.; Hong, Y.; Gao, Y.; Yin, L.; Ye, J.Q.; et al. The Prognostic Value of Lymphovascular Invasion in Radical Prostatectomy: A Systematic Review and Meta-Analysis. Asian J. Androl. 2016, 18, 780–785. [Google Scholar] [CrossRef]
- Wessels, F.; Schmitt, M.; Krieghoff-Henning, E.; Jutzi, T.; Worst, T.S.; Waldbillig, F.; Neuberger, M.; Maron, R.C.; Steeg, M.; Gaiser, T.; et al. Deep Learning Approach to Predict Lymph Node Metastasis Directly from Primary Tumour Histology in Prostate Cancer. BJU Int. 2021, 128, 352–360. [Google Scholar] [CrossRef]
- Fleischmann, A.; Schobinger, S.; Markwalder, R.; Schumacher, M.; Burkhard, F.; Thalmann, G.N.; Studer, U.E. Prognostic Factors in Lymph Node Metastases of Prostatic Cancer Patients: The Size of the Metastases but Not Extranodal Extension Independently Predicts Survival. Histopathology 2008, 53, 468–475. [Google Scholar] [CrossRef]
- Luchini, C.; Fleischmann, A.; Boormans, J.L.; Fassan, M.; Nottegar, A.; Lucato, P.; Stubbs, B.; Solmi, M.; Porcaro, A.; Veronese, N.; et al. Extranodal Extension of Lymph Node Metastasis Influences Recurrence in Prostate Cancer: A Systematic Review and Meta-Analysis. Sci. Rep. 2017, 7, 2374. [Google Scholar] [CrossRef] [PubMed]
- Porpiglia, F.; Manfredi, M.; Mele, F.; Bertolo, R.; Bollito, E.; Gned, D.; De Pascale, A.; Russo, F.; Passera, R.; Fiori, C.; et al. Indication to Pelvic Lymph Nodes Dissection for Prostate Cancer: The Role of Multiparametric Magnetic Resonance Imaging When the Risk of Lymph Nodes Invasion According to Briganti Updated Nomogram Is <5%. Prostate Cancer Prostatic Dis. 2018, 21, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Ploussard, G.; Valerio, M.; Mattei, A.; Fiori, C.; Fossati, N.; Stabile, A.; Beauval, J.B.; Malavaud, B.; Roumiguié, M.; et al. A Novel Nomogram to Identify Candidates for Extended Pelvic Lymph Node Dissection Among Patients with Clinically Localized Prostate Cancer Diagnosed with Magnetic Resonance Imaging-Targeted and Systematic Biopsies. Eur. Urol. 2019, 75, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Elsholtz, F.H.J.; Asbach, P.; Haas, M.; Becker, M.; Beets-Tan, R.G.H.; Thoeny, H.C.; Padhani, A.R.; Hamm, B. Introducing the Node Reporting and Data System 1.0 (Node-RADS): A Concept for Standardized Assessment of Lymph Nodes in Cancer. Eur. Radiol. 2021, 31, 6116–6124. [Google Scholar] [CrossRef]
- Von Eyben, F.E.; Picchio, M.; von Eyben, R.; Rhee, H.; Bauman, G. 68 Ga-Labeled Prostate-Specific Membrane Antigen Ligand Positron Emission Tomography/Computed Tomography for Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. Focus 2018, 4, 686–693. [Google Scholar] [CrossRef] [Green Version]
- Mazrani, W.; Cook, G.J.R.; Bomanji, J. Role of 68Ga and 18F PSMA PET/CT and PET/MRI in Biochemical Recurrence of Prostate Cancer: A Systematic Review of Prospective Studies. Nucl. Med. Commun. 2022; published online ahead of print, 2022 April 19. [Google Scholar] [CrossRef]
- Evangelista, L.; Zattoni, F.; Cassarino, G.; Artioli, P.; Cecchin, D.; dal Moro, F.; Zucchetta, P. PET/MRI in Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 859–873. [Google Scholar] [CrossRef]
- Petersen, L.J.; Zacho, H.D. PSMA PET for Primary Lymph Node Staging of Intermediate and High-Risk Prostate Cancer: An Expedited Systematic Review. Cancer Imaging 2020, 20, 10. [Google Scholar] [CrossRef] [Green Version]
- Stabile, A.; Pellegrino, A.; Mazzone, E.; Cannoletta, D.; de Angelis, M.; Barletta, F.; Scuderi, S.; Cucchiara, V.; Gandaglia, G.; Raggi, D.; et al. Can Negative Prostate-Specific Membrane Antigen Positron Emission Tomography/Computed Tomography Avoid the Need for Pelvic Lymph Node Dissection in Newly Diagnosed Prostate Cancer Patients? A Systematic Review and Meta-Analysis with Backup Histology as Reference Standard. Eur. Urol. Oncol. 2022, 5, 1–17. [Google Scholar] [CrossRef]
- Kase, A.M.; Tan, W.; Copland, J.A.; Cai, H.; Parent, E.E.; Madan, R.A. The Continuum of Metastatic Prostate Cancer: Interpreting PSMA PET Findings in Recurrent Prostate Cancer. Cancers 2022, 14, 1361. [Google Scholar] [CrossRef]
- Tafuri, A.; Rizzetto, R.; Amigoni, N.; Sebben, M.; Shakir, A.; Gozzo, A.; Odorizzi, K.; Gallina, S.; Bianchi, A.; Ornaghi, P.; et al. Predictors of Lymph Node Invasion in Patients with Clinically Localized Prostate Cancer Who Undergo Radical Prostatectomy and Extended Pelvic Lymph Node Dissection: The Role of Obesity. Urol. Int. 2021, 105, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Porcaro, A.B.; Tafuri, A.; Sebben, M.; Processali, T.; Pirozzi, M.; Amigoni, N.; Rizzetto, R.; Shakir, A.; Cacciamani, G.E.; Brunelli, M.; et al. Body Mass Index and Prostatic-Specific Antigen Are Predictors of Prostate Cancer Metastases in Patients Undergoing Robot-Assisted Radical Prostatectomy and Extended Pelvic Lymph Node Dissection. Minerva Urol. Nefrol. 2019, 71, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.D.; Byun, S.S.; Lee, S.E.; Hong, S.K. Impact of Body Mass Index on Oncological Outcomes of Prostate Cancer Patients after Radical Prostatectomy. Sci. Rep. 2018, 8, 11962. [Google Scholar] [CrossRef]
- Krönig, M.; Haverkamp, C.; Schulte, A.; Heinicke, L.; Schaal, K.; Drendel, V.; Werner, M.; Wetterauer, U.; Schultze-Seemann, W.; Jilg, C.A. Diabetes and Beta-Adrenergic Blockage Are Risk Factors for Metastatic Prostate Cancer. World J. Surg. Oncol. 2017, 15, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutz, S.Z.; Todenhöfer, T.; Wagner, R.; Hennenlotter, J.; Ferchl, J.M.; Scharpf, M.O.; Martus, P.; Staiger, H.; Fritsche, A.; Stenzl, A.; et al. Higher Prevalence of Lymph Node Metastasis in Prostate Cancer in Patients with Diabetes. Endocr. Relat. Cancer 2018, 25, L19–L22. [Google Scholar] [CrossRef] [Green Version]
- Kelkar, S.; Oyekunle, T.; Eisenberg, A.; Howard, L.; Aronson, W.J.; Kane, C.J.; Amling, C.L.; Cooperberg, M.R.; Klaassen, Z.; Terris, M.K.; et al. Diabetes and Prostate Cancer Outcomes in Obese and Nonobese Men After Radical Prostatectomy. JNCI Cancer Spectr. 2021, 5, pkab023. [Google Scholar] [CrossRef]
- Michaud, J.E.; Billups, K.L.; Partin, A.W. Testosterone and Prostate Cancer: An Evidence-Based Review of Pathogenesis and Oncologic Risk. Ther. Adv. Urol. 2015, 7, 378–387. [Google Scholar] [CrossRef] [Green Version]
- Porcaro, A.B.; Cerrato, C.; Tafuri, A.; Bianchi, A.; Gallina, S.; Orlando, R.; Amigoni, N.; Rizzetto, R.; Gozzo, A.; Migliorini, F.; et al. Low Endogenous Testosterone Levels Are Associated with the Extend of Lymphnodal Invasion at Radical Prostatectomy and Extended Pelvic Lymph Node Dissection. Int. Urol. Nephrol. 2021, 53, 2027–2039. [Google Scholar] [CrossRef]
- Porcaro, A.B.; Tafuri, A.; Panunzio, A.; Mazzucato, G.; Cerrato, C.; Gallina, S.; Bianchi, A.; Rizzetto, R.; Amigoni, N.; Serafin, E.; et al. Endogenous Testosterone Density Is an Independent Predictor of Pelvic Lymph Node Invasion in High-Risk Prostate Cancer: Results in 201 Consecutive Patients Treated with Radical Prostatectomy and Extended Pelvic Lymph Node Dissection. Int. Urol. Nephrol. 2022, 54, 541–550. [Google Scholar] [CrossRef]
- Mattei, A.; Fuechsel, F.G.; Bhatta Dhar, N.; Warncke, S.H.; Thalmann, G.N.; Krause, T.; Studer, U.E. The Template of the Primary Lymphatic Landing Sites of the Prostate Should Be Revisited: Results of a Multimodality Mapping Study. Eur. Urol. 2008, 53, 118–125. [Google Scholar] [CrossRef]
- Heidenreich, A.; Ohlmann, C.H.; Polyakov, S. Anatomical Extent of Pelvic Lymphadenectomy in Patients Undergoing Radical Prostatectomy. Eur. Urol. 2007, 52, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Zaffuto, E.; Fossati, N.; Bandini, M.; Suardi, N.; Mazzone, E.; Dell’Oglio, P.; Stabile, A.; Freschi, M.; Montorsi, F.; et al. Identifying Candidates for Super-Extended Staging Pelvic Lymph Node Dissection among Patients with High-Risk Prostate Cancer. BJU Int. 2018, 121, 421–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fossati, N.; Willemse, P.P.M.; Van den Broeck, T.; van den Bergh, R.C.N.; Yuan, C.Y.; Briers, E.; Bellmunt, J.; Bolla, M.; Cornford, P.; De Santis, M.; et al. The Benefits and Harms of Different Extents of Lymph Node Dissection During Radical Prostatectomy for Prostate Cancer: A Systematic Review. Eur. Urol. 2017, 72, 84–109. [Google Scholar] [CrossRef] [PubMed]
- Joniau, S.; Van Den Bergh, L.; Lerut, E.; Deroose, C.M.; Haustermans, K.; Oyen, R.; Budiharto, T.; Ameye, F.; Bogaerts, K.; Van Poppel, H. Mapping of Pelvic Lymph Node Metastases in Prostate Cancer. Eur. Urol. 2013, 63, 450–458. [Google Scholar] [CrossRef]
- Albertsen, P.C.; Hanley, J.A.H.; Barrows, G.H.; Penson, D.F.; Kowalczyk, P.D.H.; Sanders, M.M.; Fine, J. Prostate Cancer and the Will Rogers Phenomenon. J. Natl. Cancer Inst. 2005, 97, 1248–1253. [Google Scholar] [CrossRef]
- Connor, M.J.; Winkler, M.; Ahmed, H.U. Survival in Oligometastatic Prostate Cancer-A New Dawn or the Will Rogers Phenomenon? JAMA Oncol. 2020, 6, 185–186. [Google Scholar] [CrossRef]
- Gupta, M.; Patel, H.D.; Schwen, Z.R.; Tran, P.T.; Partin, A.W. Adjuvant Radiation with Androgen-Deprivation Therapy for Men with Lymph Node Metastases after Radical Prostatectomy: Identifying Men Who Benefit. BJU Int. 2019, 123, 252–260. [Google Scholar] [CrossRef] [Green Version]
- Tilki, D.; Preisser, F.; Tennstedt, P.; Tober, P.; Mandel, P.; Schlomm, T.; Steuber, T.; Huland, H.; Schwarz, R.; Petersen, C.; et al. Adjuvant Radiation Therapy Is Associated with Better Oncological Outcome Compared with Salvage Radiation Therapy in Patients with PN1 Prostate Cancer Treated with Radical Prostatectomy. BJU Int. 2017, 119, 717–723. [Google Scholar] [CrossRef]
- Touijer, K.A.; Karnes, R.J.; Passoni, N.; Sjoberg, D.D.; Assel, M.; Fossati, N.; Gandaglia, G.; Eastham, J.A.; Scardino, P.T.; Vickers, A.; et al. Survival Outcomes of Men with Lymph Node-Positive Prostate Cancer After Radical Prostatectomy: A Comparative Analysis of Different Postoperative Management Strategies. Eur. Urol. 2018, 73, 890–896. [Google Scholar] [CrossRef]
- Messing, E.M.; Manola, J.; Yao, J.; Kiernan, M.; Crawford, D.; Wilding, G.; di’SantAgnese, P.A.; Trump, D. Immediate versus Deferred Androgen Deprivation Treatment in Patients with Node-Positive Prostate Cancer after Radical Prostatectomy and Pelvic Lymphadenectomy. Lancet Oncol. 2006, 7, 472–479. [Google Scholar] [CrossRef]
- Marra, G.; Valerio, M.; Heidegger, I.; Tsaur, I.; Mathieu, R.; Ceci, F.; Ploussard, G.; van den Bergh, R.C.N.; Kretschmer, A.; Thibault, C.; et al. Management of Patients with Node-Positive Prostate Cancer at Radical Prostatectomy and Pelvic Lymph Node Dissection: A Systematic Review. Eur. Urol. Oncol. 2020, 3, 565–581. [Google Scholar] [CrossRef] [PubMed]
- Messing, E.M.; Manola, J.; Sarosdy, M.; Wilding, G.; Crawford, E.D.; Trump, D. Immediate Hormonal Therapy Compared with Observation after Radical Prostatectomy and Pelvic Lymphadenectomy in Men with Node-Positive Prostate Cancer. N. Engl. J. Med. 1999, 341, 1781–1788. [Google Scholar] [CrossRef] [PubMed]
- Braga-Basaria, M.; Dobs, A.S.; Muller, D.C.; Carducci, M.A.; John, M.; Egan, J.; Basaria, S. Metabolic Syndrome in Men with Prostate Cancer Undergoing Long-Term Androgen-Deprivation Therapy. J. Clin. Oncol. 2006, 24, 3979–3983. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Unger, J.M.; Wright, J.D.; Ramsey, S.; Till, C.; Tangen, C.M.; Barlow, W.E.; Blanke, C.; Thompson, I.M.; Hussain, M. Adverse Health Events Following Intermittent and Continuous Androgen Deprivation in Patients with Metastatic Prostate Cancer. JAMA Oncol. 2016, 2, 453–461. [Google Scholar] [CrossRef] [PubMed]
- David Crawford, E.; Moul, J.W. ADT Risks and Side Effects in Advanced Prostate Cancer: Cardiovascular and Acute Renal Injury. Oncology 2015, 29, 1–2. [Google Scholar]
- Magee, D.E.; Singal, R.K. Androgen Deprivation Therapy: Indications, Methods of Utilization, Side Effects and Their Management. Can. J. Urol. 2020, 27, 11–16. [Google Scholar]
- Tran, C.; Ouk, S.; Clegg, N.J.; Chen, Y.; Watson, P.A.; Arora, V.; Wongvipat, J.; Smith-Jones, P.M.; Yoo, D.; Kwon, A.; et al. Development of a Second-Generation Antiandrogen for Treatment of Advanced Prostate Cancer. Science 2009, 324, 787–790. [Google Scholar] [CrossRef] [Green Version]
- Clegg, N.J.; Wongvipat, J.; Joseph, J.D.; Tran, C.; Ouk, S.; Dilhas, A.; Chen, Y.; Grillot, K.; Bischoff, E.D.; Cai, L.; et al. ARN-509: A Novel Antiandrogen for Prostate Cancer Treatment. Cancer Res. 2012, 72, 1494–1503. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.R.; Saad, F.; Chowdhury, S.; Oudard, S.; Hadaschik, B.A.; Graff, J.N.; Olmos, D.; Mainwaring, P.N.; Lee, J.Y.; Uemura, H.; et al. Apalutamide Treatment and Metastasis-Free Survival in Prostate Cancer. N. Engl. J. Med. 2018, 378, 1408–1418. [Google Scholar] [CrossRef]
- Hussain, M.; Fizazi, K.; Saad, F.; Rathenborg, P.; Shore, N.; Ferreira, U.; Ivashchenko, P.; Demirhan, E.; Modelska, K.; Phung, D.; et al. Enzalutamide in Men with Nonmetastatic, Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2018, 378, 2465–2474. [Google Scholar] [CrossRef]
- Fizazi, K.; Shore, N.; Tammela, T.L.; Ulys, A.; Vjaters, E.; Polyakov, S.; Jievaltas, M.; Luz, M.; Alekseev, B.; Kuss, I.; et al. Darolutamide in Nonmetastatic, Castration-Resistant Prostate Cancer. J. Urol. 2019, 202, 660–661. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II—2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef]
- Parker, C.; Castro, E.; Fizazi, K.; Heidenreich, A.; Ost, P.; Procopio, G.; Tombal, B.; Gillessen, S. Prostate Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2020, 31, 1119–1134. [Google Scholar] [CrossRef] [PubMed]
- Mohler, J.L.; Antonarakis, E.S. NCCN Guidelines Updates: Management of Prostate Cancer. J. Natl. Compr. Canc. Netw. 2019, 17, 583–586. [Google Scholar] [CrossRef]
- Broughman, J.R.; Chen, R.C. Management of Node-Positive and Oligometastatic Prostate Cancer. Semin. Radiat. Oncol. 2017, 27, 79–86. [Google Scholar] [CrossRef]
- Jegadeesh, N.; Liu, Y.; Zhang, C.; Zhong, J.; Cassidy, R.J.; Gillespie, T.; Kucuk, O.; Rossi, P.; Master, V.A.; Alemozaffar, M.; et al. The Role of Adjuvant Radiotherapy in Pathologically Lymph Node-Positive Prostate Cancer. Cancer 2017, 123, 512–520. [Google Scholar] [CrossRef]
- Guo, L.; Zhu, Z.; Zhang, X. Adding Radiotherapy to Androgen Deprivation Therapy in Men with Node-Positive Prostate Cancer after Radical Prostatectomy: A Meta-Analysis. Medicine 2020, 99, e19153. [Google Scholar] [CrossRef]
- Abdollah, F.; Karnes, R.J.; Suardi, N.; Cozzarini, C.; Gandaglia, G.; Fossati, N.; Vizziello, D.; Sun, M.; Karakiewicz, P.I.; Menon, M.; et al. Impact of Adjuvant Radiotherapy on Survival of Patients with Node-Positive Prostate Cancer. J. Clin. Oncol. 2014, 32, 3939–3947. [Google Scholar] [CrossRef]
- Bravi, C.A.; Tin, A.; Vertosick, E.; Mazzone, E.; Bandini, M.; Dell’Oglio, P.; Stabile, A.; Gandaglia, G.; Fossati, N.; Sjoberg, D.; et al. Androgen Deprivation Therapy in Men with Node-Positive Prostate Cancer Treated with Postoperative Radiotherapy. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 204–209. [Google Scholar] [CrossRef]
- Lin, C.C.; Gray, P.J.; Jemal, A.; Efstathiou, J.A. Androgen Deprivation with or Without Radiation Therapy for Clinically Node-Positive Prostate Cancer. J. Natl. Cancer Inst. 2015, 107, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero, A.; Fossella, F.; Hortobagyi, G.; Valero, V. Docetaxel for Treatment of Solid Tumours: A Systematic Review of Clinical Data. Lancet Oncol. 2005, 6, 229–239. [Google Scholar] [CrossRef]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus Prednisone or Mitoxantrone plus Prednisone for Advanced Prostate Cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zattoni, F.; Morlacco, A.; Matrone, F.; Arcicasa, M.; Buttazzi, L.; Maruzzi, D.; Fratino, L.; Bortolus, R. Multimodal Treatment for High-Risk Locally-Advanced Prostate Cancer Following Radical Prostatectomy and Extended Lymphadenectomy. Minerva Urol. Nefrol. 2019, 71, 508–515. [Google Scholar] [CrossRef] [PubMed]
- James, N.D.; Sydes, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Spears, M.R.; Ritchie, A.W.S.; Parker, C.C.; Russell, J.M.; Attard, G.; et al. Addition of Docetaxel, Zoledronic Acid, or Both to First-Line Long-Term Hormone Therapy in Prostate Cancer (STAMPEDE): Survival Results from an Adaptive, Multiarm, Multistage, Platform Randomised Controlled Trial. Lancet 2016, 387, 1163–1177. [Google Scholar] [CrossRef] [Green Version]
- Fizazi, K.; Faivre, L.; Lesaunier, F.; Delva, R.; Gravis, G.; Rolland, F.; Priou, F.; Ferrero, J.M.; Houede, N.; Mourey, L.; et al. Androgen Deprivation Therapy plus Docetaxel and Estramustine versus Androgen Deprivation Therapy Alone for High-Risk Localised Prostate Cancer (GETUG 12): A Phase 3 Randomised Controlled Trial. Lancet Oncol. 2015, 16, 787–794. [Google Scholar] [CrossRef]
- Ahlgren, G.M.; Flodgren, P.; Tammela, T.L.J.; Kellokumpu-Lehtinen, P.; Borre, M.; Angelsen, A.; Iversen, J.R.; Sverrisdottir, A.; Jonsson, E.; Sengelov, L. Docetaxel Versus Surveillance After Radical Prostatectomy for High-Risk Prostate Cancer: Results from the Prospective Randomised, Open-Label Phase 3 Scandinavian Prostate Cancer Group 12 Trial. Eur. Urol. 2018, 73, 870–876. [Google Scholar] [CrossRef]
- Nct Antiandrogen Therapy and Radiation Therapy with or without Docetaxel in Treating Patients with Prostate Cancer That Has Been Removed by Surgery. Available online: https://clinicaltrials.gov/ct2/show/NCT03070886 (accessed on 7 March 2022).
- Bitting, R.L.; Healy, P.; George, D.J.; Anand, M.; Kim, S.; Mayer, T.; Winters, C.; Riggan, C.; Rasmussen, J.; Wilder, R.; et al. Phase II Trial of Enzalutamide and Androgen Deprivation Therapy with Salvage Radiation in Men with High-Risk Prostate-Specific Antigen Recurrent Prostate Cancer: The STREAM Trial. Eur. Urol. Oncol. 2020, 4, 948–954. [Google Scholar] [CrossRef] [Green Version]
- James, N.; de Bono, J.; Spears, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.; Ritchie, A.W.S.; Russell, M.; Gilson, C.; Jones, R.; et al. Adding Abiraterone for Patients (Pts) with High-Risk Prostate Cancer (PCa) Starting Long-Term Androgen Deprivation Therapy (ADT): Outcomes in Non-Metastatic (M0) Patients from STAMPEDE (NCT00268476). Ann. Oncol. 2017, 28, v620. [Google Scholar] [CrossRef] [Green Version]
- © NICE (2019) Prostate Cancer: Diagnosis and Management. NICE Guidance—Prostate cancer: Diagnosis and management. BJU Int. 2019, 124, 9–26. [Google Scholar] [CrossRef]
- Guideline, C. CUA-CUOG GUIDELINE 2021 Canadian Urological Association (CUA)—Canadian Uro Oncology Group (CUOG) Guideline: Management of Castration-Resistant Prostate Cancer (CRPC). Can. Urol. Assoc. J. 2021, 15, 81–90. [Google Scholar]
- Lowrance, W.T.; Breau, R.H.; Chou, R.; Jarrard, D.F.; Kibel, A.S.; Morgan, T.M.; Morgans, A.K.; Oh, W.K.; Resnick, M.; Zietman, A.; et al. Advanced Prostate Cancer: AUA/ASTRO/SUO Guideline PART I. J. Urol. 2021, 205, 14–21. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Guidelines | Specific Indications and Patient Characteristics | Management Strategies |
|---|---|---|
| EAU |
|
|
|
| |
|
| |
| NCCN |
|
|
|
| |
|
| |
|
| |
| ESMO |
|
|
| NICE |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Małkiewicz, B.; Knura, M.; Łątkowska, M.; Kobylański, M.; Nagi, K.; Janczak, D.; Chorbińska, J.; Krajewski, W.; Karwacki, J.; Szydełko, T. Patients with Positive Lymph Nodes after Radical Prostatectomy and Pelvic Lymphadenectomy—Do We Know the Proper Way of Management? Cancers 2022, 14, 2326. https://doi.org/10.3390/cancers14092326
Małkiewicz B, Knura M, Łątkowska M, Kobylański M, Nagi K, Janczak D, Chorbińska J, Krajewski W, Karwacki J, Szydełko T. Patients with Positive Lymph Nodes after Radical Prostatectomy and Pelvic Lymphadenectomy—Do We Know the Proper Way of Management? Cancers. 2022; 14(9):2326. https://doi.org/10.3390/cancers14092326
Chicago/Turabian StyleMałkiewicz, Bartosz, Miłosz Knura, Małgorzata Łątkowska, Maximilian Kobylański, Krystian Nagi, Dawid Janczak, Joanna Chorbińska, Wojciech Krajewski, Jakub Karwacki, and Tomasz Szydełko. 2022. "Patients with Positive Lymph Nodes after Radical Prostatectomy and Pelvic Lymphadenectomy—Do We Know the Proper Way of Management?" Cancers 14, no. 9: 2326. https://doi.org/10.3390/cancers14092326
APA StyleMałkiewicz, B., Knura, M., Łątkowska, M., Kobylański, M., Nagi, K., Janczak, D., Chorbińska, J., Krajewski, W., Karwacki, J., & Szydełko, T. (2022). Patients with Positive Lymph Nodes after Radical Prostatectomy and Pelvic Lymphadenectomy—Do We Know the Proper Way of Management? Cancers, 14(9), 2326. https://doi.org/10.3390/cancers14092326