
Calcium Channel Blocker Use and the Risk for Breast Cancer: A Population-Based Nested Case-Control Study

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Cases and Controls Selection
2.4. Exposure Assessment
2.5. Non-Exposures Assessment
2.6. Potential Confounders
2.7. Statistical Analysis
2.8. Ethics Approval
3. Results
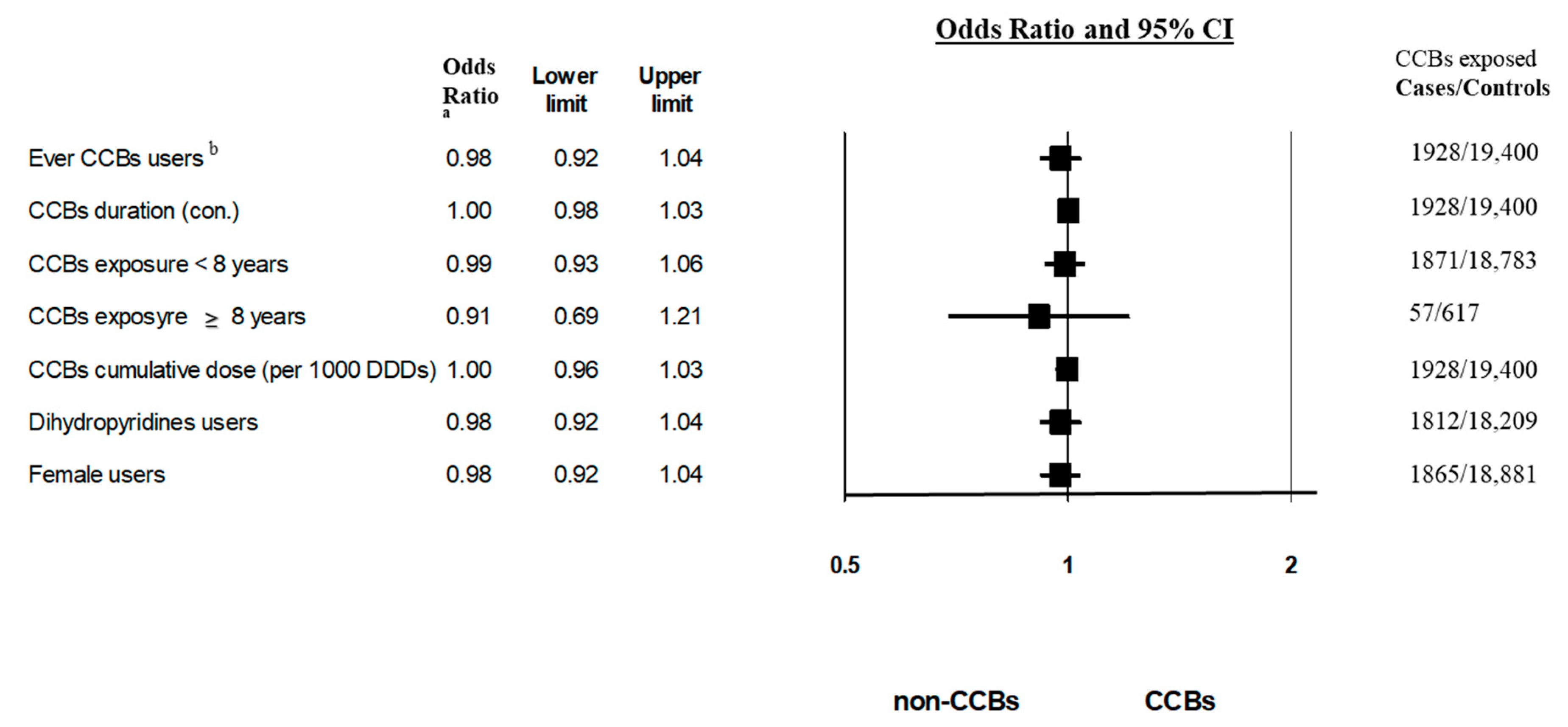
3.1. Primary Analysis
3.2. Sub-Group Analyses
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Miller, K.D.; Goding Sauer, A.; Jemal, A.; Siegel, R.L. Breast cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.S.; Ekwueme, D.U. Breast cancer as a global health concern. Cancer Epidemiol. 2009, 33, 315–318. [Google Scholar] [CrossRef] [PubMed]
- The Israel Cancer Association—Breast Cancer [Internet]. Available online: https://en.cancer.org.il/ (accessed on 12 September 2021).
- Pahor, M.; Guralnik, J.M.; Ferrucci, L.; Corti, M.C.; Salive, M.E.; Cerhan, J.R.; Wallace, R.B.; Havlik, R.J. Calcium-channel blockade and incidence of cancer in aged populations. Lancet 1996, 348, 493–497. [Google Scholar] [CrossRef]
- Fitzpatrick, A.L.; Daling, J.R.; Furberg, C.D.; Kronmal, R.A.; Weissfeld, J.L. Use of calcium channel blockers and breast carcinoma risk in postmenopausal women. Cancer 1997, 80, 1438–1447. [Google Scholar] [CrossRef]
- Li, C.I.; Daling, J.R.; Tang, M.-T.C.; Haugen, K.L.; Porter, P.L.; Malone, K.E. Use of antihypertensive medications and breast cancer risk among women aged 55 to 74 years. JAMA Intern. Med. 2013, 173, 1629–1637. [Google Scholar] [CrossRef]
- Rosenberg, L.; Rao, R.S.; Palmer, J.R.; Strom, B.L.; Stolley, P.D.; Zauber, A.G.; Warshauer, M.E.; Shapiro, S. Calcium channel blockers and the risk of cancer. J. Am. Med. Assoc. 1998, 279, 1000–1004. [Google Scholar] [CrossRef]
- Bergman, G.J.; Khan, S.; Danielsson, B.; Borg, N. Breast cancer risk and use of calcium channel blockers using Swedish population registries. JAMA Intern. Med. 2014, 174, 1700–1701. [Google Scholar] [CrossRef] [Green Version]
- Li, C.I.; Malone, K.E.; Weiss, N.S.; Boudreau, D.M.; Cushing-Haugen, K.L.; Daling, J.R. Relation between use of antihypertensive medications and risk of breast carcinoma among women ages 65–79 years. Int. J. Am. Cancer Soc. 2003, 98, 1504–1513. [Google Scholar] [CrossRef]
- Largent, J.A.; Bernstein, L.; Horn-Ross, P.L.; Marshall, S.F.; Neuhausen, S.; Reynolds, P.; Ursin, G.; Zell, J.A.; Ziogas, A.; Anton-Culver, H. Hypertension, antihypertensive medication use, and breast cancer risk in the California teachers study cohort. Cancer Causes Control 2010, 21, 1615–1624. [Google Scholar] [CrossRef] [Green Version]
- Mason, R.P. Calcium channel blockers, apoptosis and cancer: Is there a biologic relationship? J. Am. Coll. Cardiol. 1999, 34, 1857–1866. [Google Scholar] [CrossRef] [Green Version]
- Shih, J.H.; Kao, L.T.; Chung, C.H.; Liao, G.S.; Fann, L.Y.; Chien, W.C.; Li, I.H. Protective association between calcium channel blocker use and breast cancer recurrence in postsurgical women: A population-based case-control study in Taiwan. J. Clin. Pharmacol. 2020, 60, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, H.T.; Olsen, J.H.; Mellemkjær, L.; Thulstrup, A.M.; Steffensen, F.H.; McLaughlin, J.K.; Baron, J.A. Cancer risk and mortality in users of calcium channel blockers: A cohort study. Cancer 2000, 89, 165–170. [Google Scholar] [CrossRef]
- Meier, C.R.; Derby, L.E.; Jick, S.S.; Jick, H. Angiotensin-converting enzyme inhibitors, calcium channel blockers, and breast cancer. Arch. Intern. Med. 2000, 160, 349–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jick, H.; Jick, S.; Derby, L.E.; Vasilakis, C.; Myers, M.W.; Meier, C.R. Calcium-channel blockers and risk of cancer. Lancet 1997, 349, 525–528. [Google Scholar] [CrossRef]
- Michels, K.B.; Rosner, B.A.; Walker, A.M.; Stampfer, M.J.; Manson, J.E.; Colditz, G.A.; Hennekens, C.H.; Willett, W.C. Calcium channel blockers, cancer incidence, and cancer mortality in a cohort of U.S. Women: The nurses’ health study. Cancer 1998, 83, 2003–2007. [Google Scholar] [CrossRef]
- Fryzek, J.P.; Poulsen, A.H.; Lipworth, L.; Pedersen, L.; Nørgaard, M.; McLaughlin, J.K.; Friis, S. A cohort study of antihypertensive medication use and breast cancer among Danish women. Breast Cancer Res. Treat. 2006, 97, 231–236. [Google Scholar] [CrossRef]
- Devore, E.E.; Kim, S.; Ramin, C.A.; Wegrzyn, L.R.; Massa, J.; Holmes, M.D.; Michels, K.B.; Tamimi, R.M.; Forman, J.P.; Schernhammer, E.S. Antihypertensive medication use and incident breast cancer in women. Breast Cancer Res. Treat. 2015, 150, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Wilson, L.E.; D’Aloisio, A.A.; Sandler, D.P.; Taylor, J.A. Long-term use of calcium channel blocking drugs and breast cancer risk in a prospective cohort of US and Puerto Rican women. Breast Cancer Res. 2016, 18, 61. [Google Scholar] [CrossRef] [Green Version]
- Brasky, T.M.; Krok-Schoen, J.L.; Liu, J.; Chlebowski, R.T.; Freudenheim, J.L.; Lavasani, S.; Margolis, K.L.; Qi, L.; Reding, K.W.; Shields, P.G.; et al. Use of calcium channel blockers and breast cancer risk in the women’s health initiative. Cancer Epidemiol. Prev. Biomark. 2017, 26, 1345–1348. [Google Scholar] [CrossRef] [Green Version]
- Raebel, M.A.; Zeng, C.; Cheetham, T.C.; Smith, D.H.; Feigelson, H.S.; Carroll, N.M.; Goddard, K.; Tavel, H.M.; Boudreau, D.M.; Shetterly, S.; et al. Risk of breast cancer with long-term use of calcium channel blockers or angiotensin-converting enzyme inhibitors among older women. Am. J. Epidemiol. 2017, 185, 264–273. [Google Scholar] [CrossRef]
- Azoulay, L.; Soldera, S.; Yin, H.; Bouganim, N. Use of calcium channel blockers and risk of breast cancer: A population-based cohort study. Epidemiology 2016, 27, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zhang, Q.; Zhong, F.; Guo, S.; Jin, Z.; Shi, W.; Chen, C.; He, J. Association between calcium channel blockers and breast cancer: A meta-analysis of observational studies. Pharmacoepidemiol. Drug Saf. 2014, 23, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.M.; Moorin, R.E.; Chowdhury, E.K.; Stricker, B.H.; Reid, C.M.; Saunders, C.M.; Hughes, J.D. Calcium channel blockers and breast cancer incidence: An updated systematic review and meta-analysis of the evidence. Cancer Epidemiol. 2017, 50, 113–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Shi, Q.; Wang, W.; Liu, J.; Li, Q.; Hou, F. Calcium channel blockers and risk of breast cancer: A meta-analysis of 17 observational studies. PLoS ONE 2014, 9, e105801. [Google Scholar] [CrossRef]
- Thakur, A.A.; Wang, X.; Garcia-Betancourt, M.M.; Forse, R.A. Calcium channel blockers and the incidence of breast and prostate cancer: A meta-analysis. J. Clin. Pharm. Ther. 2018, 43, 519–529. [Google Scholar] [CrossRef]
- Copland, E.; Canoy, D.; Nazarzadeh, M.; Bidel, Z.; Ramakrishnan, R.; Woodward, M.; Chalmers, J.; Teo, K.K.; Pepine, C.J.; Davis, B.R.; et al. Antihypertensive treatment and risk of cancer: An individual participant data meta-analysis. Lancet Oncol. 2021, 22, 558–570. [Google Scholar] [CrossRef]
- Cohen, R.; Rabin, H.; Membership in Sick Funds, 2016. National Insurance Institute [Internet]. 2017. Available online: https://www.btl.gov.il/Publications/survey/Documents/seker289/seker_289.pdf (accessed on 15 October 2021).
- Clalit’s Database and the Research Institute—Mor Research Applications [Internet]. Available online: https://www.mor-research.com/ (accessed on 15 October 2021).
- Structure and Principles. WHO Collaborating Centre for Drug Statistics Methodology [Internet]. Available online: https://www.whocc.no/atc/structure_and_principles/ (accessed on 26 December 2020).
- Central Bureau of Statistics of Israel. Person reporting hypertension. 2009 [Internet]. Available online: https://www.cbs.gov.il/he/publications/doclib/2013/health_survey09_1500/pdf/t07.pdf (accessed on 2 May 2022).
- International Statistical Classification of Diseases and Related Health Problems. Classification of Diseases (ICD) [Internet]. Available online: https://www.who.int/standards/classifications/classification-of-diseases (accessed on 25 December 2020).
- Leader, A.; Zelikson-Saporta, R.; Pereg, D.; Spectre, G.; Rozovski, U.; Raanani, P.; Hermoni, D.; Lishner, M. The effect of combined aspirin and clopidogrel treatment on cancer incidence. Am. J. Med. 2017, 130, 826–832. Available online: http://ac.els-cdn.com/S0002934317301298/1-s2.0-S0002934317301298-main.pdf?_tid=7bcb4f72-259d-11e7-ad39-00000aacb35d&acdnat=1492674577_808cb2aba4e2b7aa16325dd21f14dfa3 (accessed on 20 April 2017). [CrossRef] [Green Version]
- Azrielant, S.; Tiosano, S.; Watad, A.; Mahroum, N.; Whitby, A.; Comaneshter, D.; Cohen, A.D.; Amital, H. Correlation between systemic lupus erythematosus and malignancies: A cross-sectional population-based study. Immunol. Res. 2017, 65, 464–469. Available online: http://link.springer.com/10.1007/s12026-016-8885-8 (accessed on 20 April 2017). [CrossRef]
- Dagan, A.; Segal, G.; Tiosano, S.; Watad, A.; Neumann, S.G.; Comaneshter, D.; Cohen, A.D.; Amital, H. Coexistent malignant conditions in rheumatoid arthritis—A population-based cross-sectional study. Int. J. Clin. Pract. 2017, 71, e12929. [Google Scholar] [CrossRef]
- Strengthening the Reporting of Observational Studies in Epidemiology. Available online: https://www.strobe-statement.org/ (accessed on 26 January 2022).
- Grassmann, F.; Yang, H.; Eriksson, M.; Azam, S.; Czene, K. Mammographic features are associated with cardiometabolic disease risk and mortality. Eur. Heart J. 2021, 42, 3361–3370. [Google Scholar] [CrossRef]
- Wu, C.Y.; Chang, C.K.; Robson, D.; Jackson, R.; Chen, S.J.; Hayes, R.D.; Stewart, R. Evaluation of smoking status identification using electronic health records and open-text information in a large mental health case register. PLoS ONE 2013, 8, e74262. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Cases (n = 4875) | Controls (n = 48750) | p-Value g |
|---|---|---|---|
| Age, a yrs, mean (SD) b | 61.31 (9.68) | 61.26 (9.67) | |
| Females b | 4744 (97.3%) | 47,440 (97.3%) | |
| Duration of follow-up, yrs, mean (SD) b | 5.16 (3.7) | 5.15 (3.7) | |
| Socioeconomic status, n (%) | <0.001 h | ||
| Low | 1550 (33.7%) | 18,974 (41.4%) | |
| Medium | 1991 (43.3%) | 18,344 (40.1%) | |
| High | 1058 (23%) | 8465 (18.5%) | |
| BMI, n (%) | 0.428 | ||
| <19 | 26 (0.6%) | 333 (0.8%) | |
| 19–24.5 | 669 (16.2%) | 6895 (16.7%) | |
| 24.6–30 | 1662 (40.3%) | 16,289 (39.5%) | |
| ≥30 | 1769 (42.9%) | 17,725 (43%) | |
| Ethnicity | 0.035 h | ||
| Arabic | 458 (9.39%) | 7262 (14.9%) | |
| Haridi | 117 (2.4%) | 1293 (2.65%) | |
| Jewish non-Haridi | 4223 (86.6%) | 39,236 (80.5%) | |
| Others | 1 (0.02%) | 20 (4.1%) | |
| Missing | 76 (1.55%) | 939 (1.93%) | |
| Smoking status | 1301 (26.7%) | 12,331 (25.29%) | 0.034 h |
| Family history of Breast Cancer | 643 (13.2%) | 2631 (5.4%) | <0.01 h |
| Comorbidities (%) | |||
| Hyperlipidemia | 4045 (83%) | 40,457 (83%) | 0.985 |
| Ischemic heart disease | 821 (16.8%) | 8781 (18%) | 0.042 h |
| Heart failure | 393 (8.1%) | 4009 (8.4%) | 0.433 |
| Cardiovascular disease | 1363 (28.0%) | 14,771 (30.3%) | 0.001 h |
| Peripheral vascular disease | 142 (2.9%) | 1313 (2.7%) | 0.368 |
| Chronic kidney disease | 425 (8.7%) | 4296 (8.8%) | 0.825 |
| Chronic lung disease | 687 (14.0.3%) | 6944 (14.24%) | 0.795 |
| Comorbidity score, mean (SD) | 1.75 (0.02) | 1.78 (0.01) | 0.165 |
| Antihypertensive drugs (ever users), n (%) | |||
| ACEIs and/or ARBs | 3538 (72.6%) | 35,094 (72%) | 0.384 |
| CCBs | 1928 (39.5%) | 19,400 (39.8%) | 0.727 |
| Diureticsc c | 2687 (55.11%) | 27,024 (55.43%) | 0.672 |
| BBs | 2725 (55.9%) | 26,205 (53.8%) | 0.047 h |
| α-Blockersd d | 203 (4.2%) | 1879 (3.9%) | 0.255 |
| α2 agonists e | 46 (0.9%) | 555 (1.1%) | 0.282 |
| Hormone replacement therapy f | 390 (8%) | 3245 (6.7%) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rotshild, V.; Hirsh Raccah, B.; Gazawe, M.; Matok, I. Calcium Channel Blocker Use and the Risk for Breast Cancer: A Population-Based Nested Case-Control Study. Cancers 2022, 14, 2344. https://doi.org/10.3390/cancers14092344
Rotshild V, Hirsh Raccah B, Gazawe M, Matok I. Calcium Channel Blocker Use and the Risk for Breast Cancer: A Population-Based Nested Case-Control Study. Cancers. 2022; 14(9):2344. https://doi.org/10.3390/cancers14092344
Chicago/Turabian StyleRotshild, Victoria, Bruria Hirsh Raccah, Muna Gazawe, and Ilan Matok. 2022. "Calcium Channel Blocker Use and the Risk for Breast Cancer: A Population-Based Nested Case-Control Study" Cancers 14, no. 9: 2344. https://doi.org/10.3390/cancers14092344
APA StyleRotshild, V., Hirsh Raccah, B., Gazawe, M., & Matok, I. (2022). Calcium Channel Blocker Use and the Risk for Breast Cancer: A Population-Based Nested Case-Control Study. Cancers, 14(9), 2344. https://doi.org/10.3390/cancers14092344