

A Novel Concept of Transperineal Focused Ultrasound Transducer for Prostate Cancer Local Deep Hyperthermia Treatments
 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Transducer Design
2.1.1. Features
2.1.2. Images Segmentation
2.1.3. Acoustic and Thermal Fields Modelling
2.1.4. Numerical Optimization of the HIFU Transducer
2.2. Driving Electronics
2.3. Software
2.4. Positioning Device of the Applicator
2.5. MRI Guidance of Local Hyperthermia
2.6. Performance Test
2.7. Ex-Vivo Studies
3. Results
3.1. Transducer Design
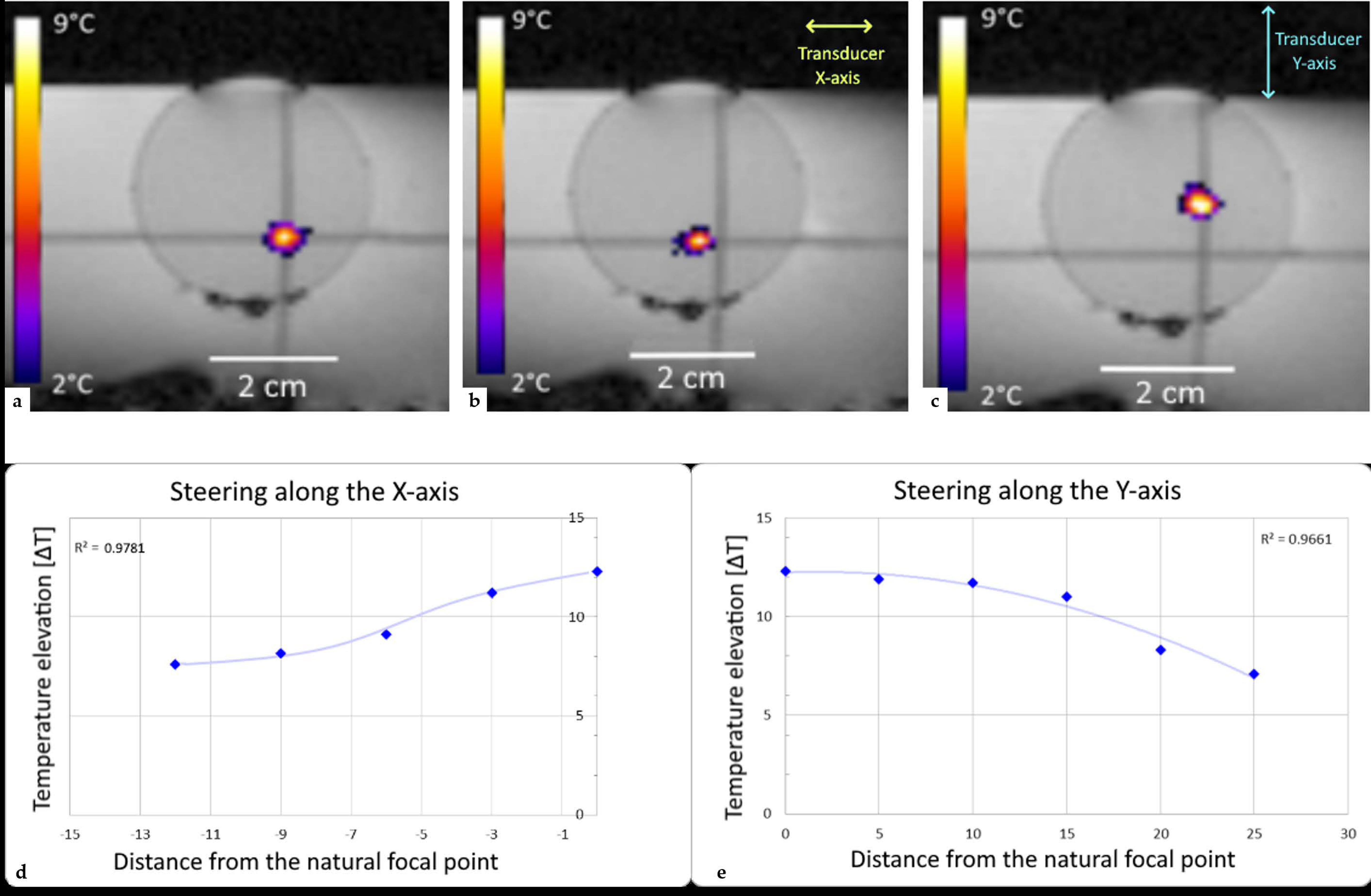
3.2. Performance Test in Tissue Mimicking Gel
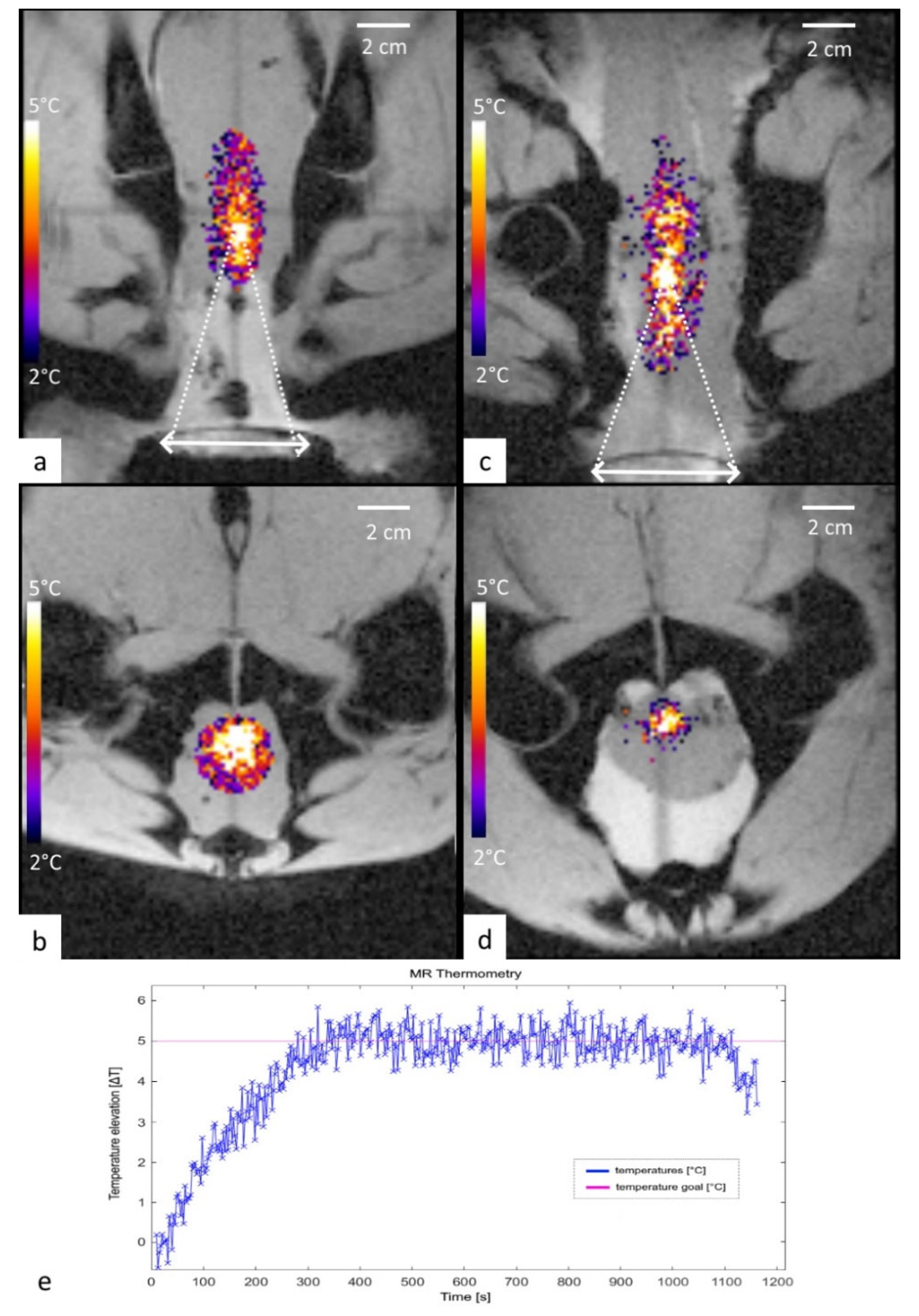
3.3. Ex Vivo Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Siegel, R.L.; Miller, K.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van der Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Loi, M.; Di Cataldo, V.; Simontacchi, G.; Detti, B.; Bonomo, P.; Masi, L.; Desideri, I.; Greto, D.; Francolini, G.; Carfora, V.; et al. Robotic Stereotactic Retreatment for Biochemical Control in Previously Irradiated Patients Affected by Recurrent Prostate Cancer. Clin. Oncol. 2018, 30, 93–100. [Google Scholar] [CrossRef]
- Cornford, P.; van der Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Alongi, F.; De Bari, B.; Campostrini, F.; Arcangeli, S.; Matei, D.V.; Lopci, E.; Petralia, G.; Bellomi, M.; Chiti, A.; Magrini, S.M.; et al. Salvage therapy of intraprostatic failure after radical external-beam radiotherapy for prostate cancer: A review. Crit. Rev. Oncol. 2013, 88, 550–563. [Google Scholar] [CrossRef] [PubMed]
- Arcangeli, S.; Agolli, L.; Donato, V. Retreatment for prostate cancer with stereotactic body radiation therapy (SBRT): Feasible or foolhardy? Rep. Pract. Oncol. Radiother. 2015, 20, 425–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crehange, G.; Roach, M., III; Martin, É.; Cormier, L.; Peiffert, D.; Cochet, A.; Chapet, O.; Supiot, S.; Cosset, J.-M.; Bolla, M.; et al. Salvage reirradiation for locoregional failure after radiation therapy for prostate cancer: Who, when, where and how? Cancer Radiother. 2014, 18, 524–534. [Google Scholar] [CrossRef] [PubMed]
- Ingrosso, G.; Becherini, C.; Lancia, A.; Caini, S.; Ost, P.; Francolini, G.; Høyer, M.; Bottero, M.; Bossi, A.; Zilli, T.; et al. Nonsurgical Salvage Local Therapies for Radiorecurrent Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. Oncol. 2020, 3, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Jereczek-Fossa, B.A.; Marvaso, G.; Zaffaroni, M.; Gugliandolo, S.G.; Zerini, D.; Corso, F.; Gandini, S.; Alongi, F.; Bossi, A.; Cornford, P.; et al. Salvage stereotactic body radiotherapy (SBRT) for intraprostatic relapse after prostate cancer radiotherapy: An ESTRO ACROP Delphi consensus. Cancer Treat. Rev. 2021, 98, 102206. [Google Scholar] [CrossRef] [PubMed]
- Tetreault-Laflamme, A.; Crook, J. Options for Salvage of Radiation Failures for Prostate Cancer. Semin. Radiat. Oncol. 2017, 27, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Valle, L.F.; Lehrer, E.J.; Markovic, D.; Elashoff, D.; Levin-Epstein, R.; Karnes, R.J.; Reiter, R.E.; Rettig, M.; Calais, J.; Nickols, N.G.; et al. A Systematic Review and Meta-analysis of Local Salvage Therapies After Radiotherapy for Prostate Cancer (MASTER). Eur. Urol. 2020, 80, 280–292. [Google Scholar] [CrossRef] [PubMed]
- Le Guevelou, J.; Chirila, M.E.; Achard, V.; Guillemin, P.C.; Lorton, O.; Uiterwijk, J.W.E.; Dipasquale, G.; Salomir, R.; Zilli, T. Combined hyperthermia and radiotherapy for prostate cancer: A systematic review. Int. J. Hyperth. 2022, 39, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Datta, N.R.; Gómez Ordóñez, S.; Gaipl, U.S.; Paulides, M.M.; Crezee, H.; Gellermann, J.; Marder, D.; Puric, E.; Bodis, S. Local hyperthermia combined with radiotherapy and-/or chemotherapy: Recent advances and promises for the future. Cancer Treat. Rev. 2015, 41, 742–753. [Google Scholar] [CrossRef] [PubMed]
- Dewhirst, M.W.; Vujaskovic, Z.; Jones, E.; Thrall, D. Re-setting the biologic rationale for thermal therapy. Int. J. Hyperthermia 2005, 21, 779–790. [Google Scholar] [CrossRef]
- Song, C.W.; Park, H.; Griffin, R.J. Improvement of Tumor Oxygenation by Mild Hyperthermia. Radiat. Res. 2001, 155, 515–528. [Google Scholar] [CrossRef]
- Genet, S.C.; Fujii, Y.; Maeda, J.; Kaneko, M.; Genet, M.D.; Miyagawa, K.; Kato, T.A. Hyperthermia inhibits homologous recombination repair and sensitizes cells to ionizing radiation in a time- and temperature-dependent manner. J. Cell. Physiol. 2012, 228, 1473–1481. [Google Scholar] [CrossRef]
- Raaphorst, G.P.; Heller, D.P.; Bussey, A.; Ng, C.E. Thermal radiosensitization by 41 °C hyperthermia during low dose-rate irradiation in human normal and tumour cell lines. Int. J. Hyperthermia 1994, 10, 263–270. [Google Scholar] [CrossRef]
- Raaphorst, G.P.; Ng, C.; Yang, D. Thermal radiosensitization and repair inhibition in human melanoma cells: A comparison of survival and DNA double strand breaks. Int. J. Hyperthermia 1999, 15, 17–27. [Google Scholar] [CrossRef]
- Rau, B.; Gaestel, M.; Wust, P.; Stahl, J.; Mansmann, U.; Schlag, P.M.; Benndorf, R. Preoperative treatment of rectal cancer with radiation, chemotherapy and hyperthermia: Analysis of treatment efficacy and heat-shock response. Radiat. Res. 1999, 151, 479. [Google Scholar] [CrossRef]
- Vujaskovic, Z.; Song, C.W. Physiological mechanisms underlying heat-induced radiosensitization. Int. J. Hyperth. 2004, 20, 163–174. [Google Scholar] [CrossRef]
- Kok, H.P.; Crezee, J.; Franken, N.; Stalpers, L.J.; Barendsen, G.W.; Bel, A. Quantifying the Combined Effect of Radiation Therapy and Hyperthermia in Terms of Equivalent Dose Distributions. Int. J. Radiat. Oncol. 2014, 88, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Crezee, J.; Van Haaren, P.; Westendorp, H.; De Greef, M.; Kok, H.; Wiersma, J.; Van Stam, G.; Sijbrands, J.; Vörding, P.Z.V.S.; Van Dijk, J.; et al. Improving locoregional hyperthermia delivery using the 3-D controlled AMC-8 phased array hyperthermia system: A preclinical study. Int. J. Hyperth. 2009, 25, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Paulides, M.M.; Bakker, J.F.; Zwamborn, A.P.M.; Van Rhoon, G.C. A head and neck hyperthermia applicator: Theoretical antenna array design. Int. J. Hyperth. 2007, 23, 59–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, P.F.; Schaefermeyer, T. BSD-2000 approach for deep local and regional hyperthermia: Clinical utility. Strahlenther. Onkol. 1989, 165, 700–704. [Google Scholar]
- Kok, H.P.; Wust, P.; Stauffer, P.R.; Bardati, F.; van Rhoon, G.C.; Crezee, J. Current state of the art of regional hyperthermia treatment planning: A review. Radiat. Oncol. 2015, 10, 196. [Google Scholar] [CrossRef] [Green Version]
- Cline, H.E.; Schenck, J.F.; Hynynen, K.; Watkins, R.D.; Souza, S.P.; Jolesz, F.A. MR-Guided Focused Ultrasound Surgery. J. Comput. Assist. Tomogr. 1992, 16, 956–965. [Google Scholar] [CrossRef]
- Kennedy, J.E. High-intensity focused ultrasound in the treatment of solid tumours. Nat. Rev. Cancer 2005, 5, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Moonen, C.T.; Quesson, B.; Salomir, R.; Vimeux, F.C.; A De Zwart, J.; Van Vaals, J.J.; Grenier, N.; Palussière, J. Thermal therapies in interventional MR imaging. Focused ultrasound. Neuroimaging Clin. N. Am. 2001, 11, 737–747. [Google Scholar]
- Petrusca, L.; Auboiroux, V.; Goget, T.; Viallon, M.; Muller, A.; Gross, P.; Becker, C.D.; Salomir, R. A Nonparametric Temperature Controller with Nonlinear Negative Reaction for Multi-Point Rapid MR-Guided HIFU Ablation. IEEE Trans. Med. Imaging 2014, 33, 1324–1337. [Google Scholar] [CrossRef]
- Gelet, A.; Chapelon, J.Y.; Bouvier, R.; Souchon, R.; Pangaud, C.; Abdelrahim, A.F.; Cathignol, D.; Dubernard, J.M. Treatment of prostate cancer with transrectal focused ultrasound: Early clinical experience. Eur. Urol. 1996, 29, 174–183. [Google Scholar] [CrossRef]
- Chopra, R.; Colquhoun, A.; Burtnyk, M.; N’Djin, W.A.; Kobelevskiy, I.; Boyes, A.; Siddiqui, K.; Foster, H.; Sugar, L.; Haider, M.A.; et al. MR Imaging—Controlled Transurethral Ultrasound Therapy for Conformal Treatment of Prostate Tissue: Initial Feasibility in Humans. Radiology 2012, 265, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Chaussy, C.; Thüroff, S. The status of high-intensity focused ultrasound in the treatment of localized prostate cancer and the impact of a combined resection. Curr. Urol. Rep. 2003, 4, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Beerlage, H.; Thüroff, S.; Debruyne, F.; Chaussy, C.; de la Rosette, J. Transrectal high-intensity focused ultrasound using the Ablatherm device in the treatment of localized prostate carcinoma. Urology 1999, 54, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Salgaonkar, V.A.; Prakash, P.; Rieke, V.; Ozhinsky, E.; Plata, J.; Kurhanewicz, J.; Hsu, I.-C.J.; Diederich, C.J. Model-based feasibility assessment and evaluation of prostate hyperthermia with a commercial MR-guided endorectal HIFU ablation array. Med. Phys. 2014, 41, 033301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, L.; Huang, Y.; Lam, D.; Gach, M.; Zoberi, I.; Hallahan, D.E.; Grisby, P.W.; Chen, H.; Altman, M.B. Targetability of cervical cancer by magnetic resonance-guided high-intensity focused ultrasound (MRgHIFU)-mediated hyperthermia (HT) for patients receiving radiation therapy. Int. J. Hyperthermia 2021, 38, 498–510. [Google Scholar] [CrossRef] [PubMed]
- Müller-Klieser, W.; Vaupel, P. Effect of hyperthermia on tumor blood flow. Biorheology 1984, 21, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Van Vulpen, M.; Raaymakers, B.W.; de Leeuw, A.A.C.; van de Kamer, J.B.; Jeroen, A.; van Moorselaar, R.; Hobbelink, M.G.G.; Battermann, J.J.; Lagendijk, J.J.W. Prostate perfusion in patients with locally advanced prostate carcinoma treated with different hyperthermia techniques. J. Urol. 2002, 168 Pt 1, 1597–1602. [Google Scholar] [CrossRef]
- Vyas, U.; Christensen, D. Ultrasound beam simulations in inhomogeneous tissue geometries using the hybrid angular spectrum method. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2012, 59, 1093–1100. [Google Scholar] [CrossRef]
- Duck, F.A. Physical Properties of Tissue: A Comprehensive Reference Book; Academic Press: London, UK, 1990. [Google Scholar]
- Tilly, W.; Gellermann, J.; Graf, R.; Hildebrandt, B.; Weissbach, L.; Budach, V.; Felix, R.; Wust, P. Regional Hyperthermia in Conjunction with Definitive Radiotherapy against Recurrent or Locally Advanced Prostate Cancer T3 pN0 M0. Strahlenther. Onkol. 2005, 181, 35–41. [Google Scholar] [CrossRef]
- Stepanishen, P.R. Transient Radiation from Pistons in an Infinite Planar Baffle. J. Acoust. Soc. Am. 1971, 49, 1629–1638. [Google Scholar] [CrossRef]
- Pennes, H.H. Analysis of tissue and arterial blood temperatures in the resting human forearm. J. Appl. Physiol. 1948, 1, 93–122. [Google Scholar] [CrossRef] [PubMed]
- Rieder, C.; Schwenke, M.; Pätz, T.; Georgii, J.; Ballhausen, H.; Schwen, L.O.; Hasse, S.; Preusser, T. Evaluation of a numerical simulation for cryoablation—Comparison with bench data, clinical kidney and lung cases. Int. J. Hyperthermia 2020, 37, 1268–1278. [Google Scholar] [CrossRef] [PubMed]
- Lorton, O.; Gui, L.; Guillemin, P.C.; Mori, N.; Crowe, L.A.; Boudabbous, S.; Terraz, S.; Becker, C.D.; Cattin, P.; Salomir, R. Self-Scanned HIFU Ablation of Moving Tissue Using Real-Time Hybrid US-MR Imaging. IEEE Trans. Biomed. Eng. 2018, 66, 2182–2191. [Google Scholar] [CrossRef]
- Guillemin, P.C.; Gui, L.; Lorton, O.; Zilli, T.; Crowe, L.A.; Desgranges, S.; Montet, X.; Terraz, S.; Miralbell, R.; Salomir, R.; et al. Mild hyperthermia by MR-guided focused ultrasound in an ex vivo model of osteolytic bone tumour: Optimization of the spatio-temporal control of the delivered temperature. J. Transl. Med. 2019, 17, 350. [Google Scholar] [CrossRef] [Green Version]
- Ozhinsky, E.; Salgaonkar, V.A.; Diederich, C.J.; Rieke, V. MR thermometry-guided ultrasound hyperthermia of user-defined regions using the ExAblate prostate ablation array. J. Ther. Ultrasound 2018, 6, 7. [Google Scholar] [CrossRef] [Green Version]
- Ferrer, C.J.; Bos, C.; De Senneville, B.D.; Borman, P.; Stemkens, B.; Tijssen, R.; Moonen, C.; Bartels, L. A planning strategy for combined motion-assisted/gated MR guided focused ultrasound treatment of the pancreas. Int. J. Hyperth. 2019, 36, 701–710. [Google Scholar] [CrossRef] [Green Version]
- Karzova, M.M.; Yuldashev, P.V.; Khokhlova, V.A.; Nartov, F.A.; Morrison, K.P.; Khokhlova, T.D. Dual-Use Transducer for Ultrasound Imaging and Pulsed Focused Ultrasound Therapy. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2021, 68, 2930–2941. [Google Scholar] [CrossRef]
- Guillemin, P.C.; Dipasquale, G.; Uiterwijk, J.W.; Jaccard, M.; Lorton, O.; Tsoutsou, P.; Gariani, J.; Poletti, P.-A.; Salomir, R.; Zilli, T. Magnetic resonance-guided ultrasound hyperthermia for prostate cancer radiotherapy: An immobilization device embedding the ultrasound applicator. J. 3D Print. Med. 2022, 6, 55–67. [Google Scholar] [CrossRef]
- Keizer, D.M.D.M.; Pathmanathan, A.U.; Andreychenko, A.; Kerkmeijer, L.G.W.; Zyp, J.R.N.V.D.V.V.; Tree, A.C.; Berg, C.A.T.V.D.; de Boer, J.C.J. Fiducial marker based intra-fraction motion assessment on cine-MR for MR-linac treatment of prostate cancer. Phys. Med. Biol. 2019, 64, 07NT02. [Google Scholar] [CrossRef]
- Løvf, M.; Zhao, S.; Axcrona, U.; Johannessen, B.; Bakken, A.C.; Carm, K.T.; Hoff, A.M.; Myklebost, O.; Meza-Zepeda, L.A.; Lie, A.K.; et al. Multifocal Primary Prostate Cancer Exhibits High Degree of Genomic Heterogeneity. Eur. Urol. 2018, 75, 498–505. [Google Scholar] [CrossRef]
- Suomi, V.; Treeby, B.; Jaros, J.; Makela, P.; Anttinen, M.; Saunavaara, J.; Sainio, T.; Kiviniemi, A.; Blanco, R. Transurethral ultrasound therapy of the prostate in the presence of calcifications: A simulation study. Med. Phys. 2018, 45, 4793–4805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorton, O.; Guillemin, P.C.; Holman, R.; Desgranges, S.; Gui, L.; Crowe, L.A.; Terraz, S.; Nastasi, A.; Lazeyras, F.; Contino-Pépin, C.; et al. Enhancement of HIFU thermal therapy in perfused tissue models using micron-sized FTAC-stabilized PFOB-core endovascular sonosensitizers. Int. J. Hyperth. 2020, 37, 1116–1130. [Google Scholar] [CrossRef] [PubMed]
- Mok, G.; Benz, E.; Vallee, J.-P.; Miralbell, R.; Zilli, T. Optimization of Radiation Therapy Techniques for Prostate Cancer with Prostate-Rectum Spacers: A Systematic Review. Int. J. Radiat. Oncol. 2014, 90, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Pepe, P.; Tamburo, M.; Pennisi, M.; Marletta, D.; Marletta, F. Clinical Outcomes of Hydrogel Spacer Injection Space OAR in Men Submitted to Hypofractionated Radiotherapy for Prostate Cancer. In Vivo 2021, 35, 3385–3389. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue | ρ [kg/m3] | c [m/s] | α [Np/m] | κ [W/ (m · K)] | ||
|---|---|---|---|---|---|---|
| Water | 1000 | 1050 | 0.006 | 4180 | 0.621 | - |
| Soft Tissue | 1087 | 1577 | 6.00 | 3668 | 0.475 | 0.0011 |
| Bone | 1900 | 2990 | 60.0 | 1370 | 0.0435 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guillemin, P.C.; Sinden, D.; M’Rad, Y.; Schwenke, M.; Le Guevelou, J.; Uiterwijk, J.W.E.; Lorton, O.; Scheffler, M.; Poletti, P.-A.; Jenne, J.; et al. A Novel Concept of Transperineal Focused Ultrasound Transducer for Prostate Cancer Local Deep Hyperthermia Treatments. Cancers 2023, 15, 163. https://doi.org/10.3390/cancers15010163
Guillemin PC, Sinden D, M’Rad Y, Schwenke M, Le Guevelou J, Uiterwijk JWE, Lorton O, Scheffler M, Poletti P-A, Jenne J, et al. A Novel Concept of Transperineal Focused Ultrasound Transducer for Prostate Cancer Local Deep Hyperthermia Treatments. Cancers. 2023; 15(1):163. https://doi.org/10.3390/cancers15010163
Chicago/Turabian StyleGuillemin, Pauline Coralie, David Sinden, Yacine M’Rad, Michael Schwenke, Jennifer Le Guevelou, Johannes W. E. Uiterwijk, Orane Lorton, Max Scheffler, Pierre-Alexandre Poletti, Juergen Jenne, and et al. 2023. "A Novel Concept of Transperineal Focused Ultrasound Transducer for Prostate Cancer Local Deep Hyperthermia Treatments" Cancers 15, no. 1: 163. https://doi.org/10.3390/cancers15010163
APA StyleGuillemin, P. C., Sinden, D., M’Rad, Y., Schwenke, M., Le Guevelou, J., Uiterwijk, J. W. E., Lorton, O., Scheffler, M., Poletti, P. -A., Jenne, J., Zilli, T., & Salomir, R. (2023). A Novel Concept of Transperineal Focused Ultrasound Transducer for Prostate Cancer Local Deep Hyperthermia Treatments. Cancers, 15(1), 163. https://doi.org/10.3390/cancers15010163