
Oligometastatic Prostate Cancer Treated with Metastasis-Directed Therapy Guided by Positron Emission Tomography: Does the Tracer Matter?

 , ,
, ,  ,
, 
 , and
, and  add
Show full author list
add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Clinical Data Collection
2.2. PET/CT Images Acquisition and Analysis
2.3. PET-Guided MDT and Clinical Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patients’ Clinical Characteristics, PET-Guided MDT, and Clinical Follow-Up
3.2. Predictors of Clinical Outcome
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cornford, P.; van den Bergh, R.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef]
- Chi, K.N.; Agarwal, N.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Juárez Soto, Á.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide for Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2019, 381, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G.; et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroğlu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2017, 377, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Hussain, M.; Saad, F.; Fizazi, K.; Sternberg, C.N.; Crawford, E.D.; Kopyltsov, E.; Park, C.H.; Alekseev, B.; Montesa-Pino, Á.; et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2022, 386, 1132–1142. [Google Scholar] [CrossRef]
- Tucci, M.; Leone, G.; Buttigliero, C.; Zichi, C.; di Stefano, R.F.; Pignataro, D.; Vignani, F.; Scagliotti, G.V.; di Maio, M. Hormonal treatment and quality of life of prostate cancer patients: New evidence. Minerva Urol. Nefrol. 2018, 70, 144–151. [Google Scholar] [CrossRef]
- Ost, P.; Reynders, D.; Decaestecker, K.; Fonteyne, V.; Lumen, N.; de Bruycker, A.; Lambert, B.; Delrue, L.; Bultijnck, R.; Claeys, T.; et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J. Clin. Oncol. 2018, 36, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ross, A.E.; Gorin, M.A.; Deville, C.; et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 650–659. [Google Scholar] [CrossRef] [Green Version]
- Deek, M.P.; van der Eecken, K.; Sutera, P.; Deek, R.A.; Fonteyne, V.; Mendes, A.A.; Decaestecker, K.; Kiess, A.P.; Lumen, N.; Phillips, R.; et al. Long-Term Outcomes and Genetic Predictors of Response to Metastasis-Directed Therapy Versus Observation in Oligometastatic Prostate Cancer: Analysis of STOMP and ORIOLE Trials. J. Clin. Oncol. 2022, 40, 3377–3382. [Google Scholar] [CrossRef]
- Chiong, E.; Murphy, D.G.; Akaza, H.; Buchan, N.C.; Chung, B.H.; Kanesvaran, R.; Khochikar, M.; Letran, J.; Lojanapiwat, B.; Ng, C.F.; et al. Management of patients with advanced prostate cancer in the Asia Pacific region: ‘real-world’ consideration of results from the Advanced Prostate Cancer Consensus Conference (APCCC) 2017. BJU Int. 2019, 123, 22–34. [Google Scholar] [CrossRef]
- deSouza, N.M.; Liu, Y.; Chiti, A.; Oprea-Lager, D.; Gebhart, G.; van Beers, B.E.; Herrmann, K.; Lecouvet, F.E. Strategies and technical challenges for imaging oligometastatic disease: Recommendations from the European Organisation for Research and Treatment of Cancer imaging group. Eur. J. Cancer 2018, 91, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Fanti, S.; Minozzi, S.; Antoch, G.; Banks, I.; Briganti, A.; Carrio, I.; Chiti, A.; Clarke, N.; Eiber, M.; de Bono, J.; et al. Consensus on molecular imaging and theranostics in prostate cancer. Lancet Oncol. 2018, 19, e696–e708. [Google Scholar] [CrossRef] [PubMed]
- Cornford, P.; Bellmunt, J.; Bolla, M.; Briers, E.; de Santis, M.; Gross, T.; Henry, A.M.; Joniau, S.; Lam, T.B.; Mason, M.D.; et al. Guidelines on Prostate Cancer. Part II: Treatment of Relapsing, Metastatic, and Castration-Resistant Prostate Cancer. Eur. Urol. 2017, 71, 630–642. [Google Scholar] [CrossRef] [PubMed]
- EAU Guidelines. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines/ (accessed on 31 October 2022).
- Fendler, W.P.; Eiber, M.; Beheshti, M.; Bomanji, J.; Ceci, F.; Cho, S.; Giesel, F.; Haberkorn, U.; Hope, T.A.; Kopka, K.; et al. 68Ga-PSMA PET/CT: Joint EANM and SNMMI procedure guideline for prostate cancer imaging: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1014–1024. [Google Scholar] [CrossRef]
- Linee Guida dell’Associazione Italiana di medicina Nucleare. Available online: https://www.aimn.it/documenti/lineeguida/4_Imaging%20Oncologico%20con%2018F%20Colina.pdf (accessed on 21 December 2022).
- Zilli, T.; Achard, V.; dal Pra, A.; Schmidt-Hegemann, N.; Jereczek-Fossa, B.A.; Lancia, A.; Ingrosso, G.; Alongi, F.; Aluwini, S.; Arcangeli, S.; et al. Recommendations for radiation therapy in oligometastatic prostate cancer: An ESTRO-ACROP Delphi consensus. Radiother. Oncol 2022, 176, 199–207. [Google Scholar] [CrossRef]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations From the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [Green Version]
- Rao, A.; Vapiwala, N.; Schaeffer, E.M.; Ryan, C.J. Oligometastatic Prostate Cancer: A Shrinking Subset or an Opportunity for Cure? Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 309–320. [Google Scholar] [CrossRef]
- Lievens, Y.; Guckenberger, M.; Gomez, D.; Hoyer, M.; Iyengar, P.; Kindts, I.; Méndez Romero, A.; Nevens, D.; Palma, D.; Park, C.; et al. Defining oligometastatic disease from a radiation oncology perspective: An ESTRO-ASTRO consensus document. Radiother. Oncol. 2020, 148, 157–166. [Google Scholar] [CrossRef]
- Gundem, G.; van Loo, P.; Kremeyer, B.; Alexandrov, L.B.; Tubio, J.; Papaemmanuil, E.; Brewer, D.S.; Kallio, H.; Högnäs, G.; Annala, M.; et al. The evolutionary history of lethal metastatic prostate cancer. Nature 2015, 520, 353–357. [Google Scholar] [CrossRef] [Green Version]
- Fossati, N.; Suardi, N.; Gandaglia, G.; Bravi, C.A.; Soligo, M.; Karnes, R.J.; Shariat, S.; Battaglia, A.; Everaerts, W.; Joniau, S.; et al. Identifying the Optimal Candidate for Salvage Lymph Node Dissection for Nodal Recurrence of Prostate Cancer: Results from a Large, Multi-institutional Analysis. Eur. Urol. 2019, 75, 176–183. [Google Scholar] [CrossRef]
- Porres, D.; Pfister, D.; Thissen, A.; Kuru, T.H.; Zugor, V.; Buettner, R.; Knuechel, R.; Verburg, F.A.; Heidenreich, A. The role of salvage extended lymph node dissection in patients with rising PSA and PET/CT scan detected nodal recurrence of prostate cancer. Prostate. Cancer Prostatic. Dis. 2017, 20, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Ning, M.S.; Boyce-Fappiano, D.; Thaker, N.G. Oligometastatic Disease in Context of the Radiation Oncology Alternative Payment Model: Implications for Local Consolidative Therapy. JCO Oncol. Pract. 2021, 17, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Pereira Mestre, R.; Ferrari, M.; Bosetti, D.G.; Pascale, M.; Oikonomou, E.; de Dosso, S.; Jermini, F.; Prior, J.O.; Roggero, E.; et al. Radiolabelled choline versus PSMA PET/CT in prostate cancer restaging: A meta-analysis. Am. J. Nucl. Med. Mol. Imaging 2019, 9, 127–139. [Google Scholar] [PubMed]
- Weber, M.; Hadaschik, B.; Ferdinandus, J.; Rahbar, K.; Bögemann, M.; Herrmann, K.; Fendler, W.P.; Kesch, C. Prostate-specific Membrane Antigen-based Imaging of Castration-resistant Prostate Cancer. Eur. Urol. Focus 2021, 7, 279–287. [Google Scholar] [CrossRef]
- Staniszewska, M.; Fragoso Costa, P.; Eiber, M.; Klose, J.M.; Wosniack, J.; Reis, H.; Szarvas, T.; Hadaschik, B.; Lückerath, K.; Herrmann, K.; et al. Enzalutamide Enhances PSMA Expression of PSMA-Low Prostate Cancer. Int. J. Mol. Sci. 2021, 22, 7431. [Google Scholar] [CrossRef]
- Zukotynski, K.A.; Emmenegger, U.; Hotte, S.; Kapoor, A.; Fu, W.; Blackford, A.L.; Valliant, J.; Bénard, F.; Kim, C.K.; Markowski, M.C.; et al. Prospective, Single-Arm Trial Evaluating Changes in Uptake Patterns on Prostate-Specific Membrane Antigen-Targeted 18F-DCFPyL PET/CT in Patients with Castration-Resistant Prostate Cancer Starting Abiraterone or Enzalutamide. J. Nucl. Med. 2021, 62, 1430–1437. [Google Scholar] [CrossRef]
- Mazzola, R.; Francolini, G.; Triggiani, L.; Napoli, G.; Cuccia, F.; Nicosia, L.; Livi, L.; Magrini, S.M.; Salgarello, M.; Alongi, F. Metastasis-directed Therapy (SBRT) Guided by PET-CT 18F-choline Versus PET-CT 68Ga-PSMA in Castration-sensitive Oligorecurrent Prostate Cancer: A Comparative Analysis of Effectiveness. Clin. Genitourin. Cancer 2021, 19, 230–236. [Google Scholar] [CrossRef]
- Crawford, E.D.; Koo, P.J.; Shore, N.; Slovin, S.F.; Concepcion, R.S.; Freedland, S.J.; Gomella, L.G.; Karsh, L.; Keane, T.E.; Maroni, P.; et al. A Clinician’s Guide to Next Generation Imaging in Patients With Advanced Prostate Cancer (RADAR III). J. Urol. 2019, 201, 682–692. [Google Scholar] [CrossRef] [Green Version]
- Lucchini, R.; Francolini, G.; Matrone, F.; Timon, G.; Franzese, C.; Marvaso, G.; Borghetti, P.; Nicosia, L.; Trodella, L.E.; Vinciguerra, A.; et al. Attitudes, practices and perspectives on imaging strategies in prostate cancer: A national cross-sectional survey involving expert radiation oncologists on behalf of AIRO (Italian association of radiotherapy and clinical oncology) GU group. Med. Oncol. 2021, 39, 3. [Google Scholar] [CrossRef]
- Sundahl, N.; Gillessen, S.; Sweeney, C.; Ost, P. When What You See Is Not Always What You Get: Raising the Bar of Evidence for New Diagnostic Imaging Modalities. Eur. Urol. 2021, 79, 565–567. [Google Scholar] [CrossRef]
- Jadvar, H.; Abreu, A.L.; Ballas, L.K.; Quinn, D.I. Oligometastatic Prostate Cancer: Current Status and Future Challenges. J. Nucl. Med. 2022, 63, 1628–1635. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall | [18F]F-Fluorocholine Guided MDT | [68Ga]Ga-PSMA-11 Guided MDT | p Value | |
|---|---|---|---|---|
| Number of patients | 37 | 11 | 26 | |
| ISUP grade | ||||
| ISUP 1 | 8 (21.6%) | 2 (18.2%) | 6 (23.1%) | 0.747 |
| ISUP 2 | 8 (21.6%) | 3 (27.3%) | 5 (19.2%) | |
| ISUP 3 | 8 (21.6%) | 1 (9.0%) | 7 (27.0%) | |
| ISUP 4 | 8 (21.6%) | 3 (27.3%) | 5 (19.2%) | |
| ISUP 5 | 5 (13.6%) | 2 (18.2%) | 3 (11.5%) | |
| Primary treatment (radiotherapy vs. surgery) | ||||
| Surgery | 29 (78.4%) | 7 (63.6%) | 22 (84.6%) | 0.157 |
| Radiotherapy (± ADT) | 8 (21.6%) | 4 (36.4%) | 4 (15.4%) | |
| Previous salvage radiotherapy | 29 (78.4%) | 9 (81.8%) | 20 (76.9%) | 0.741 |
| Time to oligometastases, months (range) | 91 (2–245) | 79 (2–209) | 104 (2–245) | 0.551 |
| Age at MDT | 73.7 ± 7.57 | 70.45 ± 8.9 | 75.08 ± 6.65 | 0.142 |
| CRPC at MDT | 8 (21.6%) | 3 (27.3%) | 5 (19.2%) | 0.587 |
| PSA pre-MDT | 3.01 ± 6.34 | 4.19 ± 5.38 | 2.5 ± 6.74 | 0.468 |
| Medical therapy in addition to MDT | 29 (78.4%) | 10 (90.9%) | 19 (73.2%) | 0.228 |
| PSA nadir after MDT | 0.76 ± 0.1 | 1.54 ± 1.83 | 0.43 ± 0.91 | 0.018 |
| Time to PSA nadir, months (range) | 4 (1–29) | 4 (1–17) | 5 (1–29) | 0.545 |
| Number of metastases treated with MDT | ||||
| 1 lesion | 30 (81.0%) | 11 (100%) | 19 (73.2%) | 0.302 |
| 2 lesions | 5 (13.6%) | 0 (0%) | 5 (19.2%) | |
| 3 lesions | 1 (2.7%) | 0 (0%) | 1 (3.8%) | |
| 5 lesions | 1 (2.7%) | 0 (0%) | 1 (3.8%) | |
| Site of metastases treated with MDT | ||||
| Lymph nodes | 24 (64.9%) | 7 (63.6%) | 17 (65.4%) | 0.582 |
| Bones | 11 (29.7%) | 4 (36.4%) | 7 (27.0%) | |
| Both | 2 (5.4%) | 0 (0%) | 2 (7.6%) | |
| MDT total dose | 34.99 ± 3.54 | 34.09 ± 2.02 | 35.37 ± 3.99 | 0.324 |
| MDT biologically effective dose | 112.08 ± 14.21 | 111 ± 15.51 | 112.56 ± 13.91 | 0.766 |
| Progression | 15 (40.5%) | 9 (81.8%) | 6 (23.1%) | 0.001 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | 0.973 (0.914–1.036) | 0.390 | ||
| ISUP grade | ||||
| ISUP 1 | 1.000 (Ref.) | |||
| ISUP 2 | 0.694 (0.097–4.972) | 0.716 | ||
| ISUP 3 | 0.993 (0.163–6.030) | 0.994 | ||
| ISUP 4 | 1.474 (0.268–8.097) | 0.656 | ||
| ISUP 5 | 1.536 (0.265–8.916) | 0.632 | ||
| Primary treatment (radiotherapy vs. surgery) | ||||
| Surgery | 1.000 (Ref.) | |||
| Radiotherapy (± ADT) | 2.617 (0.784–8.736) | 0.143 | ||
| Previous salvage radiotherapy | 0.698 (0.217–2.243) | 0.546 | ||
| CRPC | 6.238 (1.939–20.073) | 0.002 | 4.587 (1.226–17.154) | 0.024 |
| PSA pre-MDT | 1.005 (0.922–1.095) | 0.907 | ||
| Medical therapy in addition to MDT | 0.635 (0.142–2.843) | 0.553 | ||
| PSA nadir after MDT | 2.979 (1.882–4.717) | <0.001 | 2.937 (1.750–4.928) | <0.001 |
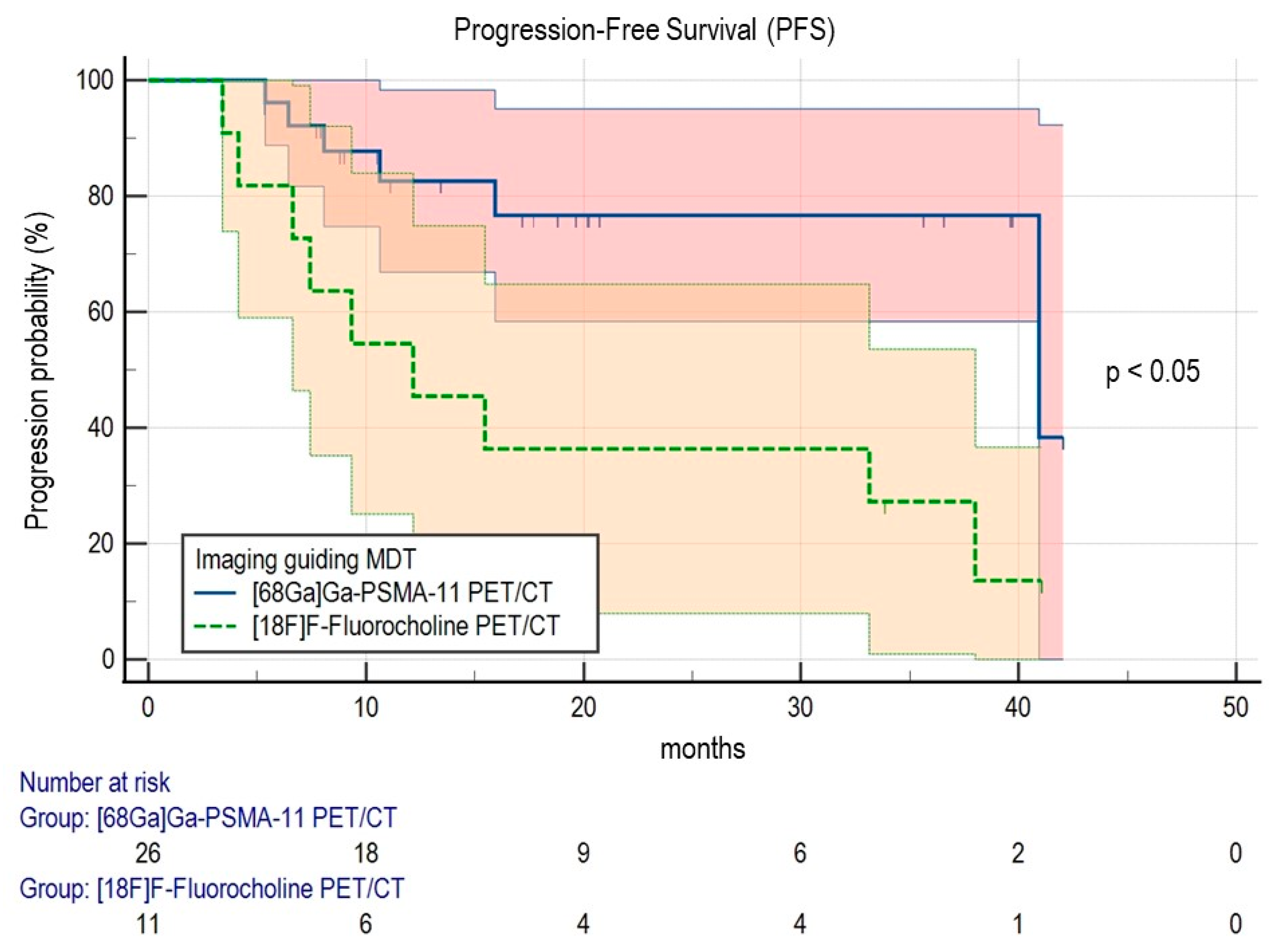
| PET/CT imaging | ||||
| [68Ga]Ga-PSMA-11 | 1.000 (Ref.) | |||
| [18F]F-Fluorocholine | 3.813 (1.351–10.760) | 0.011 | 2.603 (0.829–8.172) | 0.100 |
| SUVmax | 1.031 (0.981–1.084) | 0.232 | ||
| MTV | 0.936 (0.707–1.240) | 0.645 | ||
| TLG | 1.002 (0.977–1.028) | 0.870 | ||
| Number of metastases treated with MDT | ||||
| 1 lesion | 1.000 (Ref.) | |||
| 2 or more lesions | 1.550 (0.532–4.518) | 0.422 | ||
| Site of metastases treated with MDT | ||||
| Lymph node | 1.000 (Ref.) | |||
| Bones or both | 0.926 (0.283–3.031) | 0.899 | ||
| MDT total dose | 0.952 (0.812–1.117) | 0.546 | ||
| MDT biologically effective dose | 0.993 (0.958–1.029) | 0.695 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lanfranchi, F.; Belgioia, L.; Marcenaro, M.; Zanardi, E.; Timon, G.; Riondato, M.; Giasotto, V.; Zawaideh, J.P.; Tomasello, L.; Mantica, G.; et al. Oligometastatic Prostate Cancer Treated with Metastasis-Directed Therapy Guided by Positron Emission Tomography: Does the Tracer Matter? Cancers 2023, 15, 323. https://doi.org/10.3390/cancers15010323
Lanfranchi F, Belgioia L, Marcenaro M, Zanardi E, Timon G, Riondato M, Giasotto V, Zawaideh JP, Tomasello L, Mantica G, et al. Oligometastatic Prostate Cancer Treated with Metastasis-Directed Therapy Guided by Positron Emission Tomography: Does the Tracer Matter? Cancers. 2023; 15(1):323. https://doi.org/10.3390/cancers15010323
Chicago/Turabian StyleLanfranchi, Francesco, Liliana Belgioia, Michela Marcenaro, Elisa Zanardi, Giorgia Timon, Mattia Riondato, Veronica Giasotto, Jeries Paolo Zawaideh, Laura Tomasello, Guglielmo Mantica, and et al. 2023. "Oligometastatic Prostate Cancer Treated with Metastasis-Directed Therapy Guided by Positron Emission Tomography: Does the Tracer Matter?" Cancers 15, no. 1: 323. https://doi.org/10.3390/cancers15010323
APA StyleLanfranchi, F., Belgioia, L., Marcenaro, M., Zanardi, E., Timon, G., Riondato, M., Giasotto, V., Zawaideh, J. P., Tomasello, L., Mantica, G., Piol, N., Borghesi, M., Traverso, P., Satragno, C., Panarello, D., Scaffidi, C., Romagnoli, A., Rebuzzi, S. E., Coco, A., ... Bauckneht, M. (2023). Oligometastatic Prostate Cancer Treated with Metastasis-Directed Therapy Guided by Positron Emission Tomography: Does the Tracer Matter? Cancers, 15(1), 323. https://doi.org/10.3390/cancers15010323