
Transarterial Radioembolization Planning and Treatment with Microspheres Containing Holmium-166: Determination of Renal and Intestinal Radionuclide Elimination, Effective Half-Life, and Regulatory Aspects

 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Measuring System Calibration
2.2. Excretion Measurements
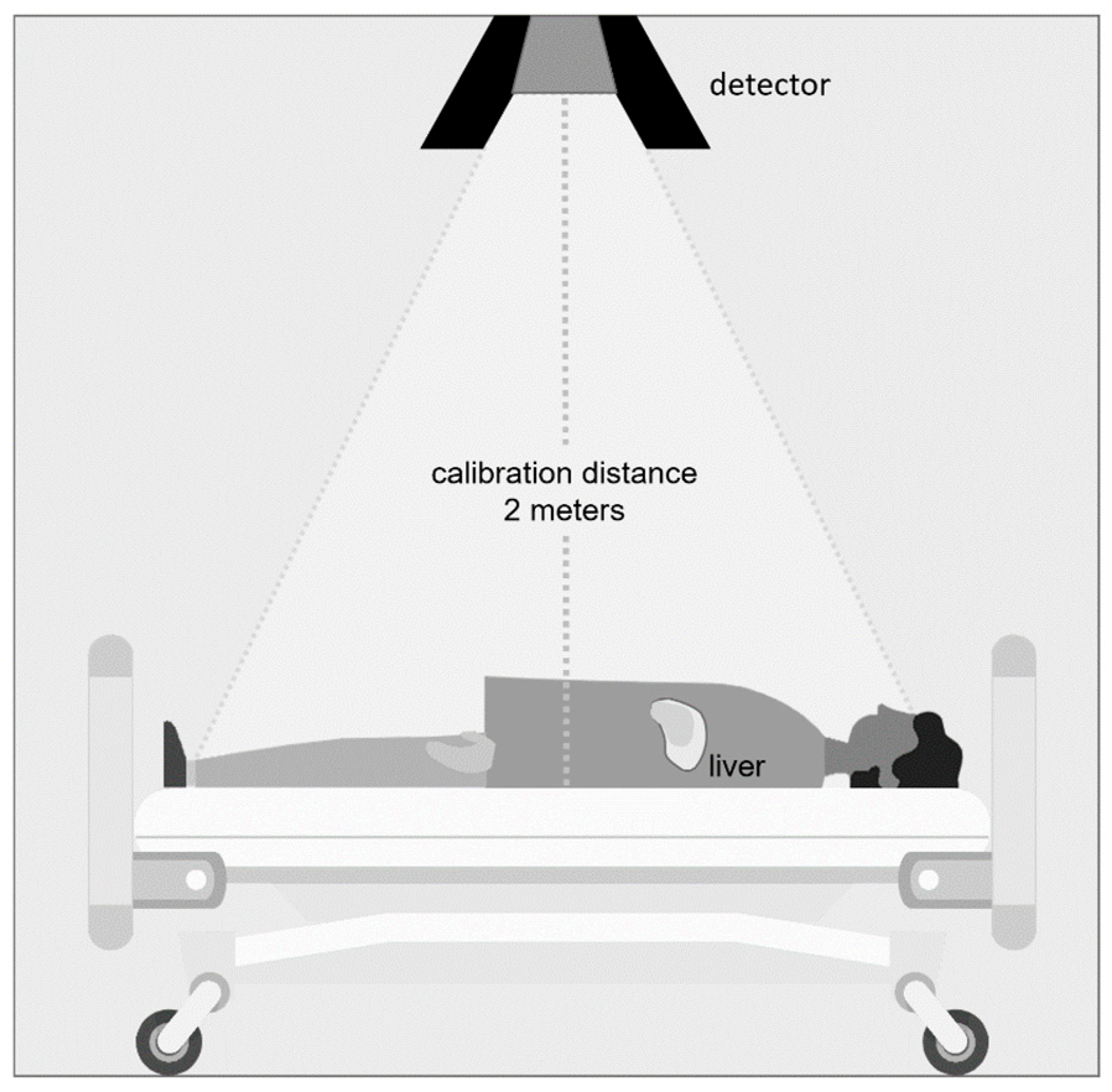
2.3. Effective Half-Life Measurements
2.4. Statistical Analysis
3. Results
3.1. Measuring System Calibration
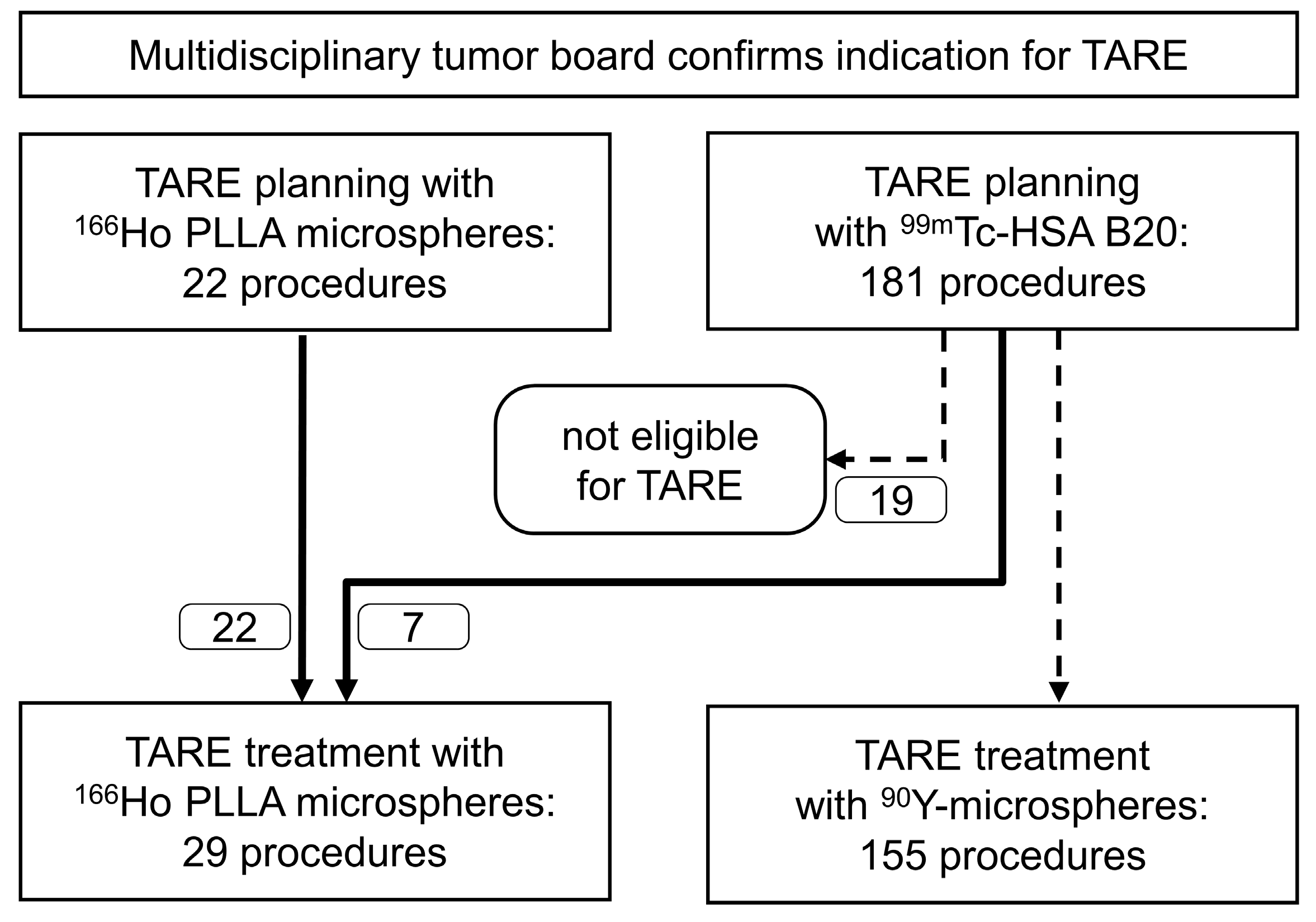
3.2. Patient and Procedural Characteristics
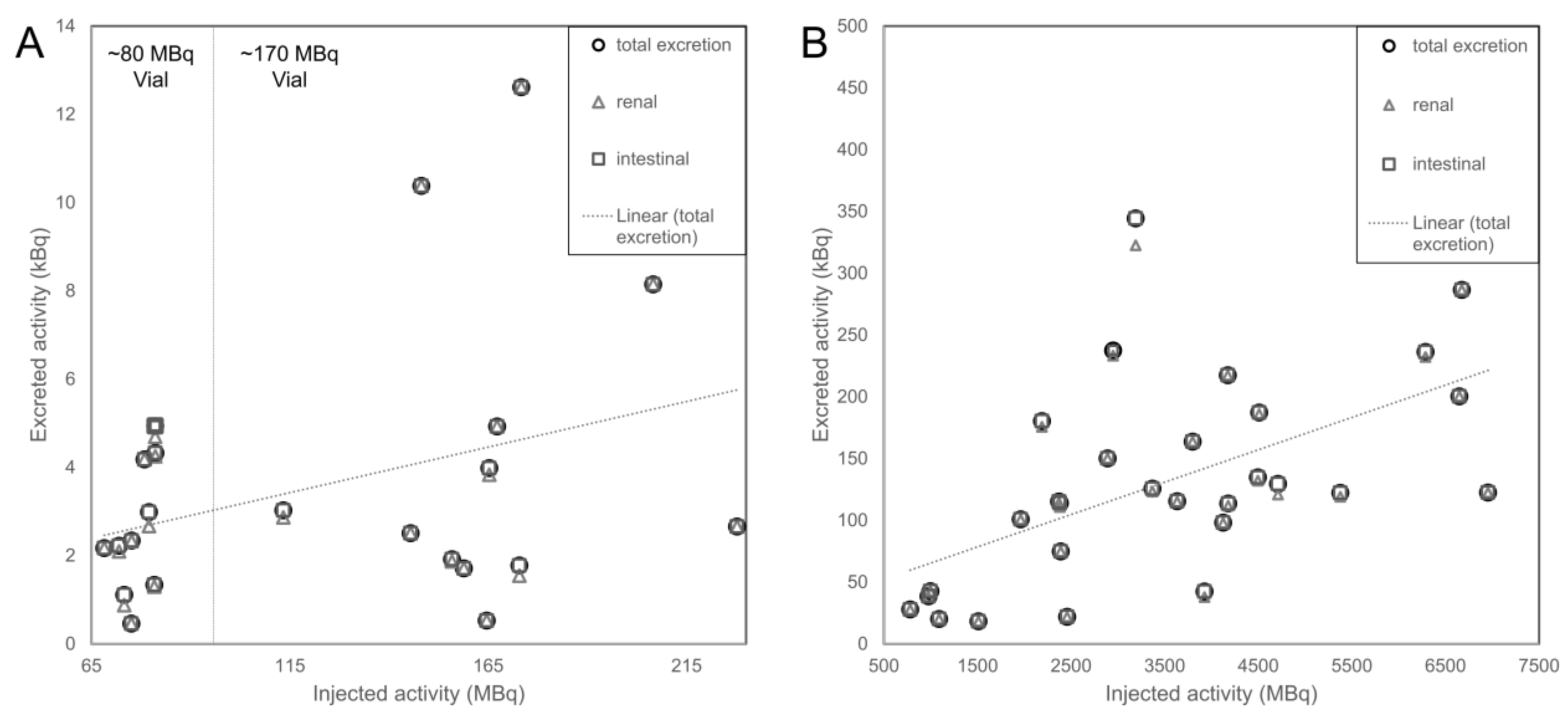
3.3. Excretion
3.3.1. Renal Excretion
3.3.2. Intestinal Excretion
3.3.3. Total Excretion
3.4. Effective Whole-Body Half-Life
4. Discussion
4.1. Excretion of Radioactivity after 166Ho TARE Procedures
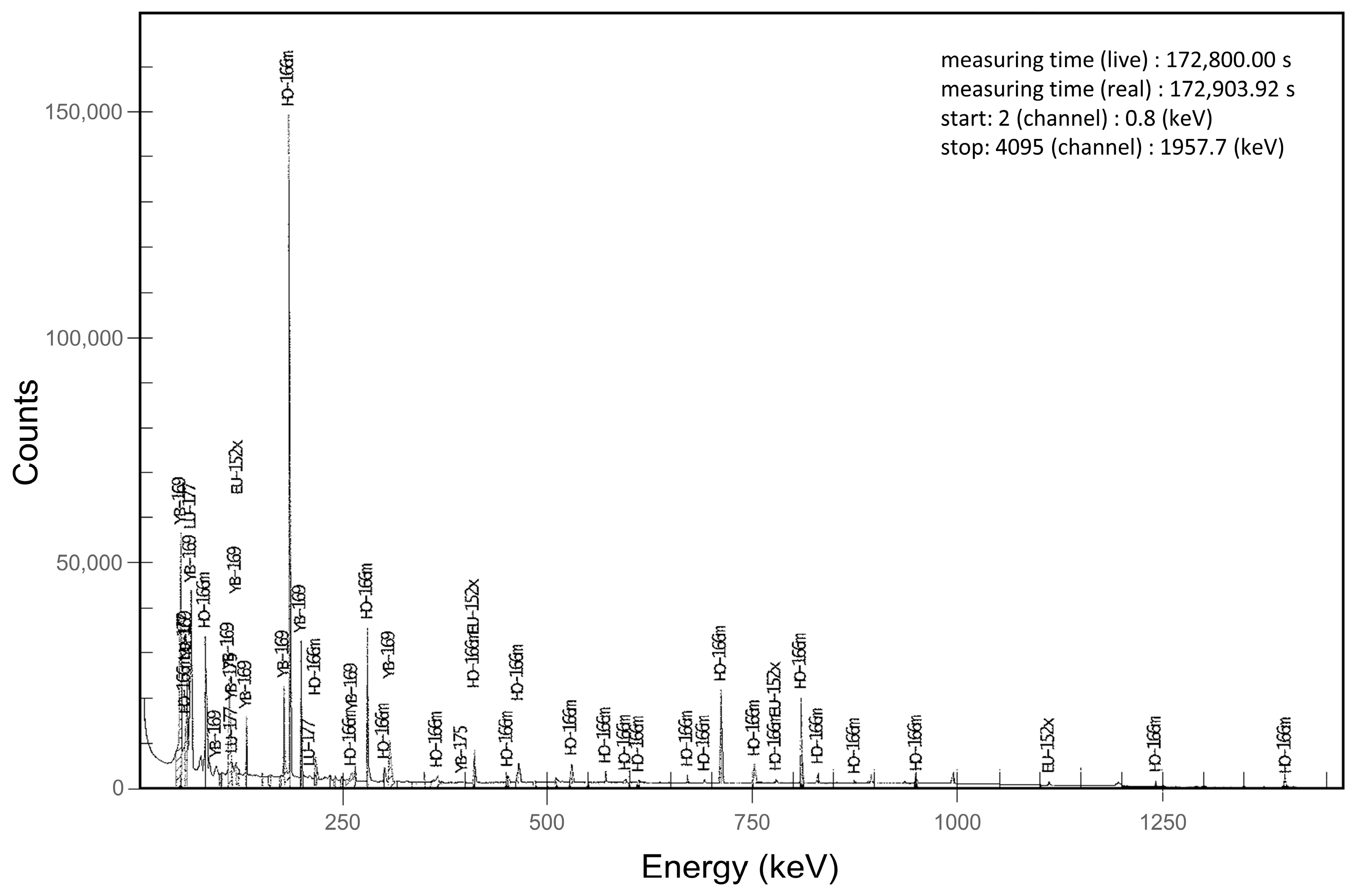
4.2. Long-Living Radioactive Impurities
4.3. Regulatory Aspects of Radioactivity Release
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bester, L.; Meteling, B.; Boshell, D.; Chua, T.C.; Morris, D.L. Transarterial chemoembolisation and radioembolisation for the treatment of primary liver cancer and secondary liver cancer: A review of the literature. J. Med. Imaging Radiat. Oncol. 2014, 58, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Gulec, S.A.; McGoron, A.J. Radiomicrosphere Dosimetry: Principles and Current State of the Art. Semin. Nucl. Med. 2022, 52, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Prince, J.F.; van den Bosch, M.; Nijsen, J.F.W.; Smits, M.L.J.; van den Hoven, A.F.; Nikolakopoulos, S.; Wessels, F.J.; Bruijnen, R.C.G.; Braat, M.; Zonnenberg, B.A.; et al. Efficacy of Radioembolization with (166)Ho-Microspheres in Salvage Patients with Liver Metastases: A Phase 2 Study. J. Nucl. Med. Off. Soc. Nucl. Med. 2018, 59, 582–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute of Nuclear Physics, Lunds University, Sweden. The Lund/LBNL Nuclear Data Search. Available online: http://nucleardata.nuclear.lu.se (accessed on 1 August 2022).
- van Rooij, R.; Braat, A.; de Jong, H.; Lam, M. Simultaneous (166)Ho/(99m)Tc dual-isotope SPECT with Monte Carlo-based downscatter correction for automatic liver dosimetry in radioembolization. EJNMMI Phys. 2020, 7, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobin, C.; Bouchard, J.; Chiste, V.; Collins, S.M.; Dryak, P.; Fenwick, A.; Keightley, J.; Lepy, M.C.; Lourenco, V.; Robinson, A.P.; et al. Activity measurements and determination of nuclear decay data of (166)Ho in the MRTDosimetry project. Appl. Radiat. Isot. 2019, 153, 108826. [Google Scholar] [CrossRef] [PubMed]
- Seevinck, P.R.; Seppenwoolde, J.H.; de Wit, T.C.; Nijsen, J.F.; Beekman, F.J.; van Het Schip, A.D.; Bakker, C.J. Factors affecting the sensitivity and detection limits of MRI, CT, and SPECT for multimodal diagnostic and therapeutic agents. Anticancer. Agents Med Chem. 2007, 7, 317–334. [Google Scholar] [CrossRef] [PubMed]
- Smits, M.L.J.; Dassen, M.G.; Prince, J.F.; Braat, A.; Beijst, C.; Bruijnen, R.C.G.; de Jong, H.; Lam, M. The superior predictive value of (166)Ho-scout compared with (99m)Tc-macroaggregated albumin prior to (166)Ho-microspheres radioembolization in patients with liver metastases. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 798–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakker, R.C.; de Roos, R.; Ververs, F.F.T.; Lam, M.; van der Lee, M.K.; Zonnenberg, B.A.; Krijger, G.C. Blood and urine analyses after radioembolization of liver malignancies with [(166)Ho]Ho-acetylacetonate-poly(l-lactic acid) microspheres. Nucl. Med. Biol. 2019, 71, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Drescher, R.; Kuhnel, C.; Seifert, P.; Guhne, F.; Freesmeyer, M. Renal and Intestinal Excretion of (90)Y and (166)Ho After Transarterial Radioembolization of Liver Tumors. Am. J. Roentgenol. 2020, 214, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Prince, J.F.; Smits, M.L.; Krijger, G.C.; Zonnenberg, B.A.; van den Bosch, M.A.; Nijsen, J.F.; Lam, M.G. Radiation emission from patients treated with holmium-166 radioembolization. J. Vasc. Interv. Radiol. 2014, 25, 1956–1963.e1. [Google Scholar] [CrossRef] [PubMed]
- Reinders, M.T.M.; Smits, M.L.J.; van Roekel, C.; Braat, A. Holmium-166 Microsphere Radioembolization of Hepatic Malignancies. Semin. Nucl. Med. 2019, 49, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Quirem Medical, B.V. QuiremSpheres–Intrstuction for Use (Multi-Language). Available online: https://www.quirem.com/wp-content/uploads/2022/03/LC-8004307-IFU-QuiremSpheres-Multi-Language.pdf (accessed on 30 November 2022).
- Squair, P.; Pozzo, L.; Ivanov, E.; Osso, J. Neutron activation of microspheres containing 165Ho: Theoretical and experimental radionuclidic impurities study. In Proceedings of the 2011 International Nuclear Atlantic Conference-INAC 2011, Belo Horizonte, Brazil, 24–28 October 2011. [Google Scholar]
- Zielhuis, S.W.; Nijsen, J.F.; de Roos, R.; Krijger, G.C.; van Rijk, P.P.; Hennink, W.E.; van het Schip, A.D. Production of GMP-grade radioactive holmium loaded poly(L-lactic acid) microspheres for clinical application. Int. J. Pharm. 2006, 311, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Freudenberg, R.; Hesse, L.; Kotzerke, J. Evaluation of radionuclide impurities in several radiopharmaceuticals. Nucl. Med. 2022, 61, 339–346. [Google Scholar] [CrossRef]
- U.S. Nuclear Regulatory Commission. Yttrium-90 Theraspheres and SIRSpheres Impurities. NRC Information Notice 2007–10; 2007. Available online: https://www.nrc.gov/docs/ML0634/ML063470020.pdf (accessed on 30 November 2022).
- Ministry of Justice (Canada). Nuclear Substances and Radiation Devices Regulations (SOR/2000-207). Available online: https://laws.justice.gc.ca/eng/regulations/sor-2000-207/page-1.html#docCont (accessed on 30 November 2022).
- Council of the European Union. Directive 2013/59/EURATOM: Basic Safety Standards for Protection against the Dangers Arising from Exposure to Ionising Radiation (Version 17/01/2014). Available online: https://osha.europa.eu/en/legislation/directives/directive-2013-59-euratom-protection-against-ionising-radiation (accessed on 30 November 2022).
- Department for Business Energy & Industrial Strategy (UK). Scope of and Exemptions from the Radioactive Substances Legislation in England, Wales and Northern Ireland. 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/731733/RSL_Guidance_update_BEIS_format_v5_180803.pdf (accessed on 30 November 2022).
- Regulation on Protection against the Harmful Effects of Ionizing Radiation (Radiation Protection Regulation) (BGBl I 41/2018). Available online: https://www.bfs.de/SharedDocs/ExterneLinks/BfS/DE/gesetze-regelungen/strlschv.html (accessed on 13 November 2022).
- Australian Radiation Protection and Nuclear Safety Agency. Safety Guide for Radiation Protection in Nuclear Medicine (2008). Available online: https://www.arpansa.gov.au/regulation-and-licensing/regulatory-publications/radiation-protection-series/guides-and-recommendations/rps14-2 (accessed on 24 November 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TARE Planning | TARE Treatment | |
|---|---|---|
| No. of patients | 17 | 23 |
| Age (years) * | 70 ± 9 72, 58–82 | 70 ± 8 68, 57–82 |
| Sex | 14 male, 3 female | 20 male, 3 female |
| Tumor entity | 12 HCC, 4 mCRC, 1 CCC | 18 HCC, 4 mCRC, 1 CCC |
| Child–Pugh Score * | 5.6 ± 1.1 5, 5–8 | 5.5 ± 0.9 5, 5–8 |
| No. of procedures | 22 | 29 |
| eGFR (mL/min) * | 77 ± 8.6 73, 43–100 | 81 ± 24.5 88, 40–105 |
| Whole liver volume (mL) * | 2242 ± 816.5 2265, 896–3731 | 2255.7 ± 644.5 2153, 1276–3843 |
| Target liver volume (mL) * | 974 ± 537.2 978, 190–1917 | 1022 ± 520.4 987, 208–2133 |
| Injected activity (GBq) * | 0.125 ± 0.051 0.129, 0.068–0.228 | 3.482 ± 1.771 3.368, 0.781–6.955 |
| TARE Planning | TARE Treatment | p-Value | |
|---|---|---|---|
| 0–12 h | |||
| Urinary volume (mL) * | 929 ± 529.4 734, 162–2471 | 1021 ± 464.8 956, 244–2023 | 0.332 |
| Excreted activity (kBq) * | 2.8 ± 2.9 1.8, 0.2–12.6 | 71.5 ± 56 70.2, 3.2–286.6 | <0.00001 |
| Activity concentration (kBq/L) * | 3.9 ± 4.3 1.8, 0.3–16.4 | 81.2 ± 56.3 70.1, 3.1–197.7 | <0.00001 |
| Proportion of injected activity (kBq/GBq) * | 22.8 ± 19.5 15.9, 1.6–72.8 | 20.6 ± 11.8 17.9, 2.1–49.2 | 0.638 |
| Proportion of injected 166Ho (%) * | 0.0027 ± 0.0023 0.0019, 0.0002–0.0085 | 0.0024 ± 0.0014 0.0021, 0.0002–0.0057 | 0.624 |
| 12–24 h | |||
| Urinary volume (mL) * | 711 ± 419.5 591, 210–1843 | 760 ± 427.1 680, 134–1641 | 0.728 |
| Excreted activity (kBq) * | 1.1 ± 1.2 0.6, 0.2–5.1 | 33.1 ± 24.2 30, 3.5–89.2 | <0.00001 |
| Activity concentration (kBq/L) * | 2.1 ± 2.6 1.2, 0.3–10.4 | 54.6 ± 50.4 46.8, 4–215.9 | <0.00001 |
| Proportion of injected activity (kBq/GBq) * | 9.2 ± 7.9 8.2, 1.6–34.2 | 10.2 ± 6.3 8.2, 1.4–25.6 | 0.516 |
| Proportion of injected 166Ho (%) * | 0.0015 ± 0.0013 0.0013, 0.0003–0.0054 | 0.0016 ± 0.0010 0.0013, 0.0002–0.0041 | 0.441 |
| 24–36 h | |||
| Urinary volume (mL) * | 658 ± 348.2 588, 63–1235 | ||
| Excreted activity (kBq) * | 18.3 ± 12.4 16.7, 2–45.9 | ||
| Activity concentration (kBq/L) * | 31.2 ± 19.9 29.4, 5.2–76.5 | ||
| Proportion of injected activity (kBq/GBq) * | 6.3 ± 4.1 6.6, 0.5–14.4 | ||
| Proportion of injected 166Ho (%) * | 0.0014 ± 0.0009 0.0014, 0.0001–0.0031 | ||
| 36–48 h | |||
| Urinary volume (mL) * | 779 ± 436.2 736, 59–1820 | ||
| Excreted activity (kBq) * | 13.7 ± 11.9 10.5, 1.3–56.7 | ||
| Activity concentration (kBq/L) * | 13.7 ± 12.2 10.5, 1.3–56.7 | ||
| Proportion of injected activity (kBq/GBq) * | 4 ± 3.6 3.2, 0–17.8 | ||
| Proportion of injected 166Ho (%) * | 0.0012 ± 0.0011 0.0010, 0.0000–0.0053 |
| TARE Planning | TARE Treatment | P-Value | |
|---|---|---|---|
| 0–12 h | |||
| Patients with defecation(s) | 9 | 12 | |
| Fecal mass (g) * | 160 ± 188.7 114, 31–634 | 143 ± 90.1 104, 43–304 | 0.802 |
| Excreted activity (kBq) * | 0.07 ± 0.05 0.05, 0.01–0.15 | 2.5 ± 5.6 0.5, 0.1–20.1 | 0.00034 |
| Proportion of injected activity (kBq/GBq) * | 0.6 ± 0.5 0.5, 0.1–1.4 | 0.9 ± 1.8 0.2, 0.0–6.3 | 0.190 |
| Proportion of injected 166Ho (%) * | 0.0001 ± 0.0001 0.0001, 0.00000– 0.0002 | 0.0001 ± 0.0002 0.00003, 0.0000– 0.0007 | 0.190 |
| 12–24 h | |||
| Patients with defecation(s) | 8 | 6 | |
| Fecal mass (g) * | 129 ± 66.6 124, 55–242 | 113 ± 54.7 99, 64–221 | 0.749 |
| Excreted activity (kBq) * | 0.13 ± 0.08 0.12, 0.1–0.24 | 1.2 ± 1.1 1.0, 0.0–2.7 | 0.061 |
| Proportion of injected activity (kBq/GBq) * | 1.5 ± 1.1 1.3, 0.01–3.0 | 0.3 ± 0.3 0.3, 0.0–0.7 | 0.033 |
| Proportion of injected 166Ho (%) * | 0.0002 ± 0.0001 0.0001, 0.0000–0.0004 | 0.0001 ± 0.00004 0.00004, 0.0000–0.0001 | 0.081 |
| 24–36 h | |||
| Patients with defecation(s) | 11 | ||
| Fecal mass (g) * | 100 ± 63.6 97, 28–257 | ||
| Excreted activity (kBq) * | 2.3 ± 2.5 1.8, 0.2–8.8 | ||
| Proportion of injected activity (kBq/GBq) * | 0.6 ± 0.6 0.5, 0.0–1.9 | ||
| Proportion of injected 166Ho (%) * | 0.0001 ± 0.0001 0.0001, 0.0000–0.0004 | ||
| 36–48 h | |||
| Patients with defecation(s) | 2 | ||
| Fecal mass (g) * | 51 ± 41.7 51, 21–80 | ||
| Excreted activity (kBq) * | 1.4 ± 0.2 1.4, 1.3–1.5 | ||
| Proportion of injected activity (kBq/GBq) * | 0.4 ± 0.2 0.4, 0.3–0.5 | ||
| Proportion of injected 166Ho (%) * | 0.0001 ± 0.00005 0.0001, 0.0001–0.0002 |
| TARE Planning | TARE Treatment | |
|---|---|---|
| Time Frame | 24 h | 48 h |
| Renal excretion | ||
| Excreted activity (kBq) * | 3.6 ± 3.1 2.6, 0.5–14.6 | 128.2 ± 80.1 119.2, 18.3–322.6 |
| Proportion of injected activity (kBq/GBq) * | 30.2 ± 20.6 28.1, 3.2–72.8 | 38.5 ± 21.0 36.6, 8.9–101.1 |
| Proportion of injected 166Ho (%) * | 0.0037 ± 0.0025 0.0036, 0.0004–0.0096 | 0.0060 ± 0.0035 0.0051, 0.0012–0.0175 |
| Proportion of total excreted activity (%) * | 97.1 ± 4.8 100.0, 82.5–100.0 | 98.1 ± 3.3 99.5, 84.6–100.0 |
| Intestinal excretion | ||
| Excreted activity (kBq)* | 0.2 ± 0.1 0.2, 0–0.3 | 3.3 ± 4.9 0.2, 0.1–21.8 |
| Proportion of injected activity (kBq/GBq) * | 0.7 ± 0.1 0.006, 0–0.3 | 0.7 ± 1.3 0.2, 0–6.8 |
| Proportion of injected 166Ho (%) * | 0.0002 ± 0.0001 0.0002, 0.0000–0.0005 | 0.0002 ± 0.0002 0.0001, 0.0000–0.0009 |
| Proportion of total excreted activity (%) * | 2.9 ± 4.8 0.0, 0.0–17.5 | 1.8 ± 3.3 0.5, 0.0–15.4 |
| Total | ||
| Excreted activity (kBq) * | 3.6 ± 3.1 2.6, 0.5–12.6 | 130.5 ± 82.3 122.3, 18.3–344.4 |
| Proportion of injected activity (kBq/GBq) * | 30.2 ± 20.6 28.1, 3.2–72.8 | 39.2 ± 21.9 37.3, 8.9–108 |
| Proportion of injected 166Ho (%) * | 0.0038 ± 0.0025 0.0036, 0.0004–0.0096 | 0.0061 ± 0.0037 0.0053, 0.0012–0.0184 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kühnel, C.; Gühne, F.; Seifert, P.; Freudenberg, R.; Freesmeyer, M.; Drescher, R. Transarterial Radioembolization Planning and Treatment with Microspheres Containing Holmium-166: Determination of Renal and Intestinal Radionuclide Elimination, Effective Half-Life, and Regulatory Aspects. Cancers 2023, 15, 68. https://doi.org/10.3390/cancers15010068
Kühnel C, Gühne F, Seifert P, Freudenberg R, Freesmeyer M, Drescher R. Transarterial Radioembolization Planning and Treatment with Microspheres Containing Holmium-166: Determination of Renal and Intestinal Radionuclide Elimination, Effective Half-Life, and Regulatory Aspects. Cancers. 2023; 15(1):68. https://doi.org/10.3390/cancers15010068
Chicago/Turabian StyleKühnel, Christian, Falk Gühne, Philipp Seifert, Robert Freudenberg, Martin Freesmeyer, and Robert Drescher. 2023. "Transarterial Radioembolization Planning and Treatment with Microspheres Containing Holmium-166: Determination of Renal and Intestinal Radionuclide Elimination, Effective Half-Life, and Regulatory Aspects" Cancers 15, no. 1: 68. https://doi.org/10.3390/cancers15010068
APA StyleKühnel, C., Gühne, F., Seifert, P., Freudenberg, R., Freesmeyer, M., & Drescher, R. (2023). Transarterial Radioembolization Planning and Treatment with Microspheres Containing Holmium-166: Determination of Renal and Intestinal Radionuclide Elimination, Effective Half-Life, and Regulatory Aspects. Cancers, 15(1), 68. https://doi.org/10.3390/cancers15010068