

Efficacy and Safety of First-Line Cytokines versus Sunitinib and Second-Line Axitinib for Patients with Metastatic Renal Cell Carcinoma (ESCAPE Study): A Phase III, Randomized, Sequential Open-Label Study

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
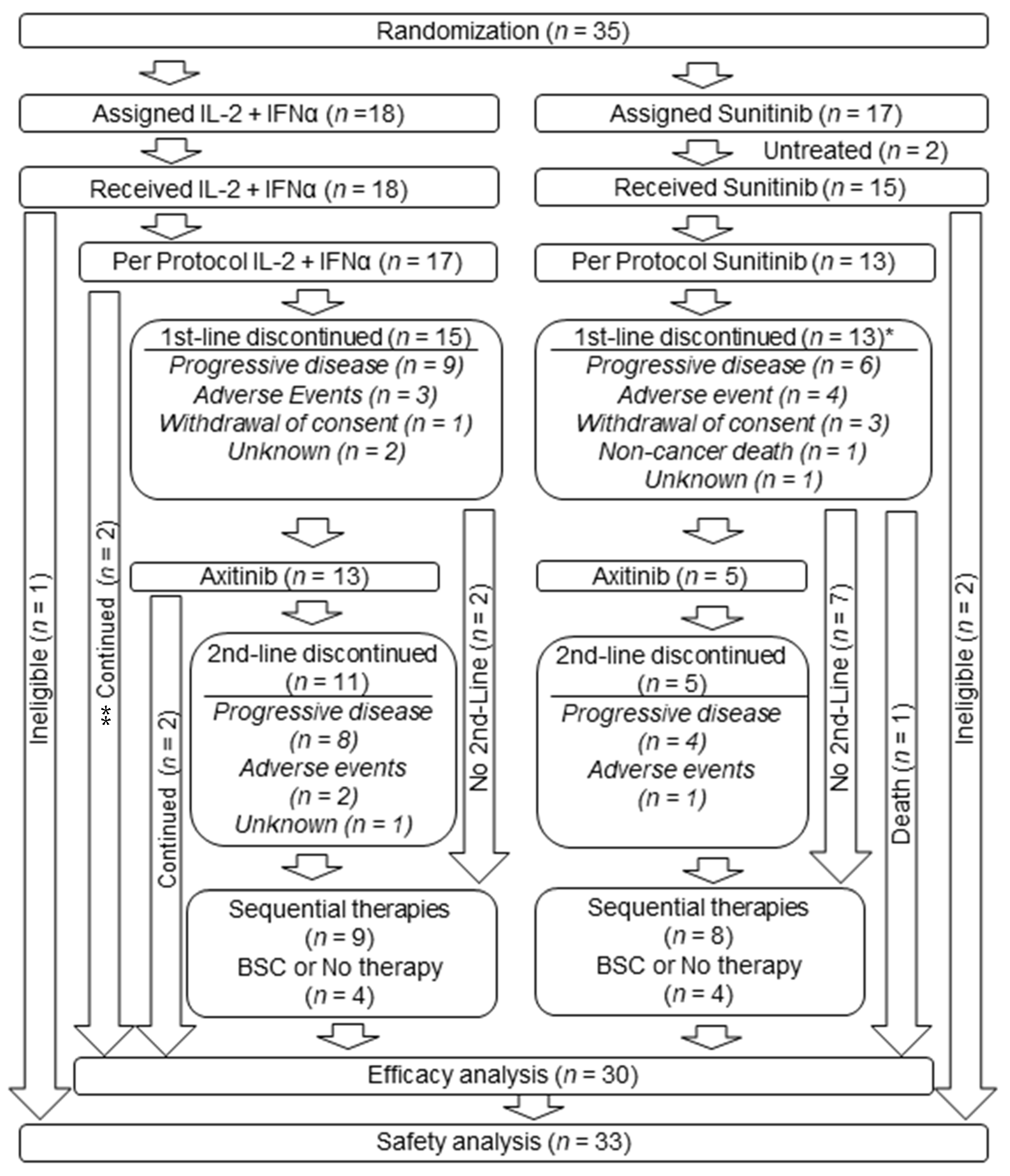
2.1. Patients
2.2. Study Design
2.3. Efficacy and Safety Assessment
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Treatment Duration
3.3. Adverse Events
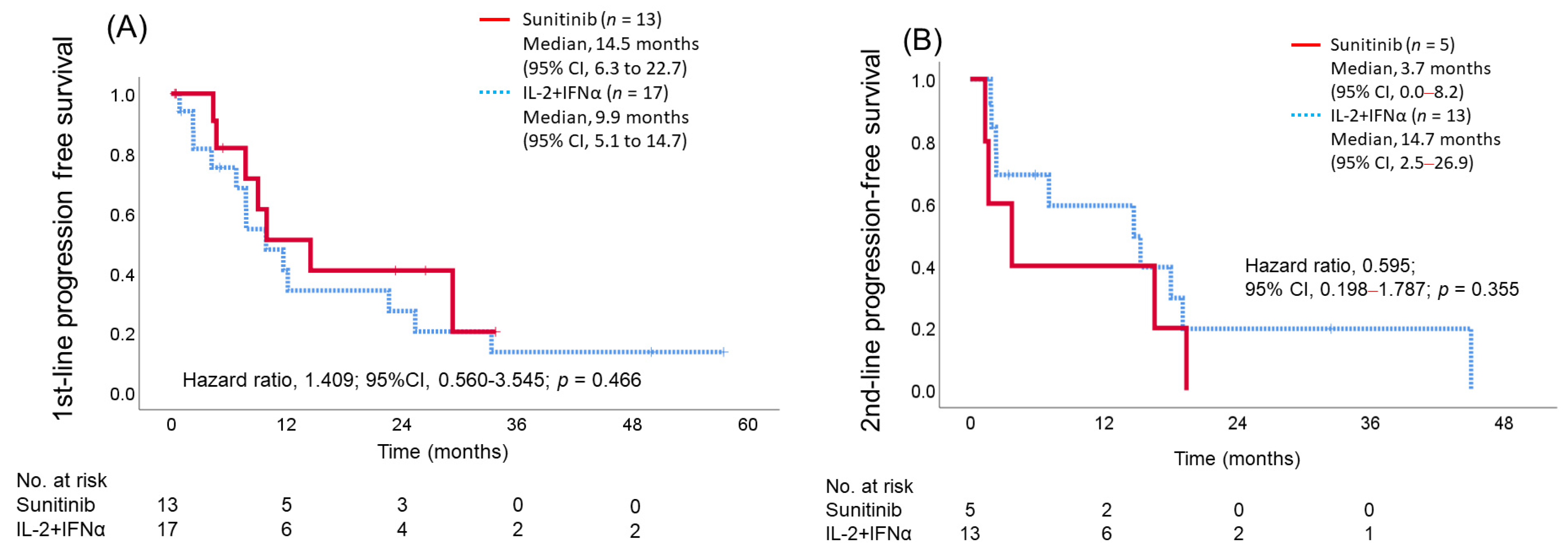
3.4. Objective Response Rate, Disease Control Rate, and Progression-Free Survival with each First-Line and Second-Line Treatment
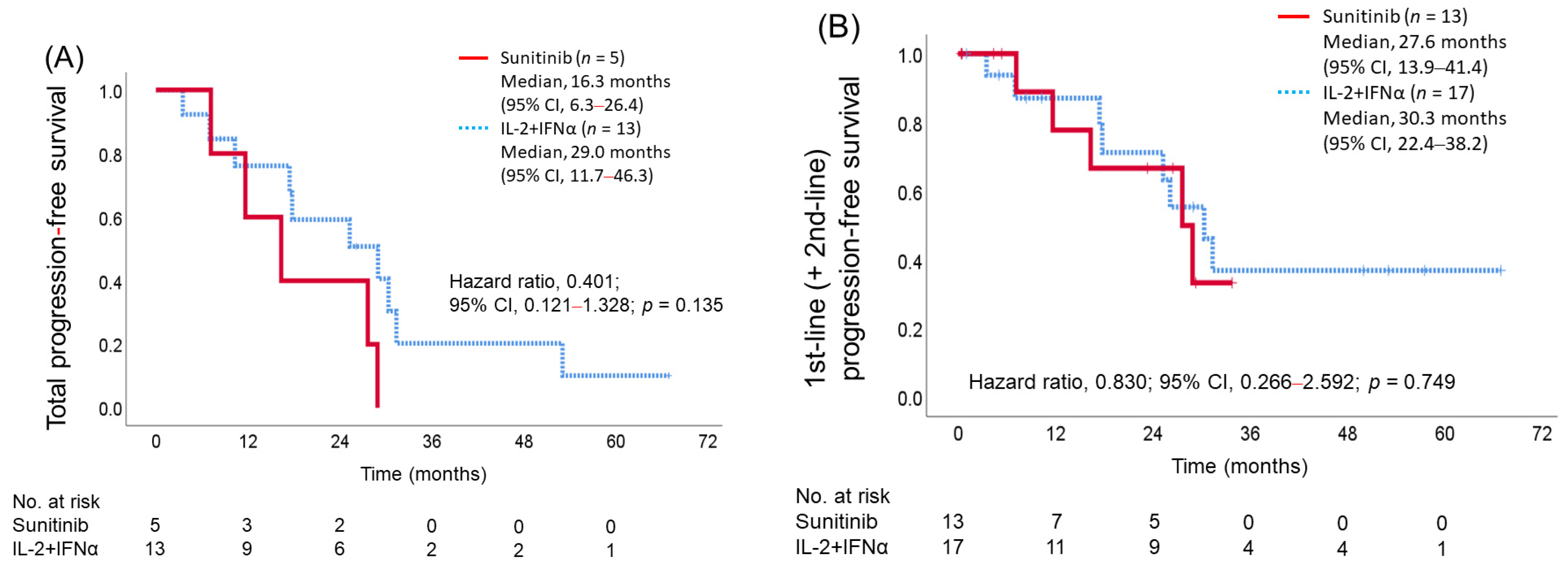
3.5. Total (First Line + Second Line) Progression-Free Survival
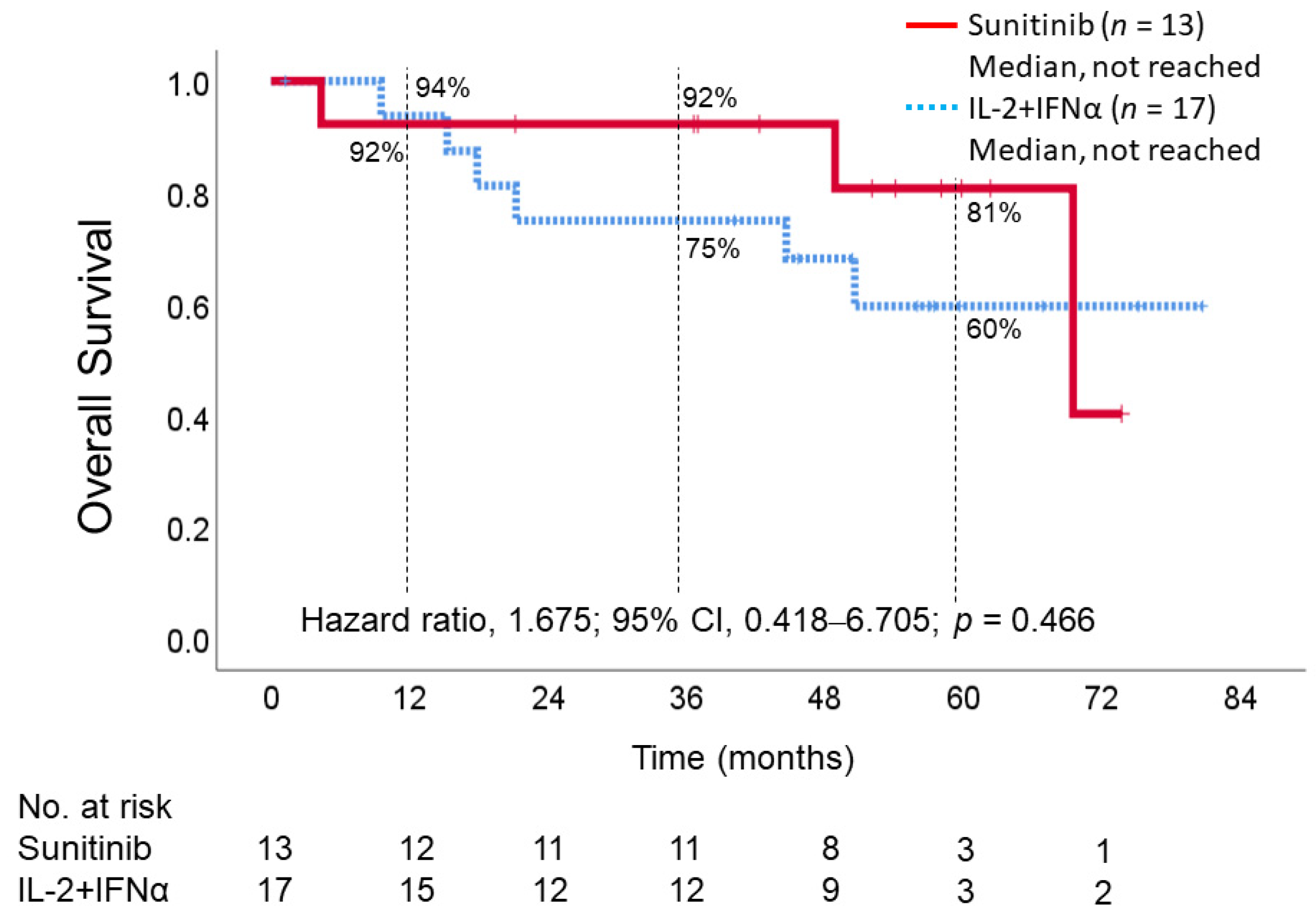
3.6. Overall Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Escudier, B.; Tomczak, P.; Kaprin, A.; Szczylik, C.; Hutson, T.E.; Michaelson, M.D.; Gorbunova, V.A.; Gore, M.E.; Rusakov, I.G.; et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): A randomised phase 3 trial. Lancet 2011, 378, 1931–1939. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Davis, I.D.; Mardiak, J.; Szczylik, C.; Lee, E.; Wagstaff, J.; Barrios, C.H.; Salman, P.; Gladkov, O.A.; Kavina, A.; et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: Results of a randomized phase III trial. J. Clin. Oncol. 2010, 28, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- O’Rourke, K. CheckMate-214 trial results show longer treatment-free survival with immunotherapy. Cancer 2022, 128, 1156. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Powles, T.; Burotto, M.; Escudier, B.; Bourlon, M.T.; Shah, A.Y.; Suarez, C.; Hamzaj, A.; Porta, C.; Hocking, C.M.; et al. Nivolumab plus cabozantinib versus sunitinib in first-line treatment for advanced renal cell carcinoma (CheckMate 9ER): Long-term follow-up results from an open-label, randomised, phase 3 trial. Lancet Oncol. 2022, 23, 888–898. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.; Alekseev, B.; Rha, S.Y.; Porta, C.; Eto, M.; Powles, T.; Grunwald, V.; Hutson, T.E.; Kopyltsov, E.; Mendez-Vidal, M.J.; et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N. Engl. J. Med. 2021, 384, 1289–1300. [Google Scholar] [CrossRef]
- Powles, T.; Plimack, E.R.; Soulieres, D.; Waddell, T.; Stus, V.; Gafanov, R.; Nosov, D.; Pouliot, F.; Melichar, B.; Vynnychenko, I.; et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol. 2020, 21, 1563–1573. [Google Scholar] [CrossRef]
- Heng, D.Y.; Xie, W.; Regan, M.M.; Warren, M.A.; Golshayan, A.R.; Sahi, C.; Eigl, B.J.; Ruether, J.D.; Cheng, T.; North, S.; et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: Results from a large, multicenter study. J. Clin. Oncol. 2009, 27, 5794–5799. [Google Scholar] [CrossRef]
- Motzer, R.J.; Bacik, J.; Schwartz, L.H.; Reuter, V.; Russo, P.; Marion, S.; Mazumdar, M. Prognostic factors for survival in previously treated patients with metastatic renal cell carcinoma. J. Clin. Oncol. 2004, 22, 454–463. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef]
- Motzer, R.J.; Jonasch, E.; Agarwal, N.; Alva, A.; Baine, M.; Beckermann, K.; Carlo, M.I.; Choueiri, T.K.; Costello, B.A.; Derweesh, I.H.; et al. Kidney Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2022, 20, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Naito, S.; Yamamoto, N.; Takayama, T.; Muramoto, M.; Shinohara, N.; Nishiyama, K.; Takahashi, A.; Maruyama, R.; Saika, T.; Hoshi, S.; et al. Prognosis of Japanese metastatic renal cell carcinoma patients in the cytokine era: A cooperative group report of 1463 patients. Eur. Urol. 2010, 57, 317–325. [Google Scholar] [CrossRef]
- Donskov, F.; von der Maase, H. Impact of immune parameters on long-term survival in metastatic renal cell carcinoma. J. Clin. Oncol. 2006, 24, 1997–2005. [Google Scholar] [CrossRef] [PubMed]
- Vaglio, A.; Alberici, F.; Maggiore, U.; Buti, S.; Potenzoni, D.; Passalacqua, R.; Buzio, C. Chronically administered immunotherapy with low-dose IL-2 and IFN-alpha in metastatic renal cell carcinoma: A feasible option for patients with a good prognostic profile. Oncology 2009, 76, 69–76. [Google Scholar] [CrossRef]
- Sella, A.; Michaelson, M.D.; Matczak, E.; Simantov, R.; Lin, X.; Figlin, R.A. Heterogeneity of Patients with Intermediate-Prognosis Metastatic Renal Cell Carcinoma Treated with Sunitinib. Clin. Genitourin. Cancer 2017, 15, 291–299.e1. [Google Scholar] [CrossRef]
- Kadono, Y.; Konaka, H.; Izumi, K.; Anai, S.; Fujimoto, K.; Ishibashi, K.; Kawai, N.; Kato, T.; Iba, A.; Masumori, N.; et al. Efficacy and safety of cytokines versus first-line sunitinib and second-line axitinib for patients with metastatic renal cell carcinoma (ESCAPE study): A study protocol for phase III randomized sequential open-label study. Contemp. Clin. Trials Commun. 2019, 15, 100403. [Google Scholar] [CrossRef] [PubMed]
- Akaza, H.; Tsukamoto, T.; Fujioka, T.; Tomita, Y.; Kitamura, T.; Ozono, S.; Miki, T.; Naito, S.; Zembutsu, H.; Nakamura, Y. Combined immunotherapy with low-dose IL-2 plus IFN-alpha for metastatic renal cell carcinoma: Survival benefit for selected patients with lung metastasis and serum sodium level. Jpn. J. Clin. Oncol. 2011, 41, 1023–1030. [Google Scholar] [CrossRef]
- Maroto, J.P.; del Muro, X.G.; Mellado, B.; Perez-Gracia, J.L.; Andres, R.; Cruz, J.; Gallardo, E.; Domenech, M.; Arranz, J.A.; Meana, J.A. Phase II trial of sequential subcutaneous interleukin-2 plus interferon alpha followed by sorafenib in renal cell carcinoma (RCC). Clin. Transl. Oncol. 2013, 15, 698–704. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Aren Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthelemy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bedke, J.; Capitanio, U.; Dabestani, S.; Fernandez-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022, 82, 399–410. [Google Scholar] [CrossRef]
- Rathmell, W.K.; Rumble, R.B.; Van Veldhuizen, P.J.; Al-Ahmadie, H.; Emamekhoo, H.; Hauke, R.J.; Louie, A.V.; Milowsky, M.I.; Molina, A.M.; Rose, T.L.; et al. Management of Metastatic Clear Cell Renal Cell Carcinoma: ASCO Guideline. J. Clin. Oncol. 2022, 40, 2957–2995. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Powles, T.; Burotto, M.; Escudier, B.; Bourlon, M.T.; Zurawski, B.; Oyervides Juarez, V.M.; Hsieh, J.J.; Basso, U.; Shah, A.Y.; et al. Nivolumab plus Cabozantinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2021, 384, 829–841. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulieres, D.; Melichar, B.; et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Bosma, N.A.; Warkentin, M.T.; Gan, C.L.; Karim, S.; Heng, D.Y.C.; Brenner, D.R.; Lee-Ying, R.M. Efficacy and Safety of First-line Systemic Therapy for Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-analysis. Eur. Urol. Open Sci. 2022, 37, 14–26. [Google Scholar] [CrossRef]
- Nocera, L.; Karakiewicz, P.I.; Wenzel, M.; Tian, Z.; Shariat, S.F.; Saad, F.; Chun, F.K.H.; Briganti, A.; Kapoor, A.; Lalani, A.K. Clinical Outcomes and Adverse Events after First-Line Treatment in Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-Analysis. J. Urol. 2022, 207, 16–24. [Google Scholar] [CrossRef]
- Ljungberg, B.; Bensalah, K.; Canfield, S.; Dabestani, S.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; Lam, T.; Marconi, L.; Merseburger, A.S.; et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur. Urol. 2015, 67, 913–924. [Google Scholar] [CrossRef]
- Bamias, A.; Escudier, B.; Sternberg, C.N.; Zagouri, F.; Dellis, A.; Djavan, B.; Tzannis, K.; Kontovinis, L.; Stravodimos, K.; Papatsoris, A.; et al. Current Clinical Practice Guidelines for the Treatment of Renal Cell Carcinoma: A Systematic Review and Critical Evaluation. Oncologist 2017, 22, 667–679. [Google Scholar] [CrossRef]
- Mendel, D.B.; Laird, A.D.; Xin, X.; Louie, S.G.; Christensen, J.G.; Li, G.; Schreck, R.E.; Abrams, T.J.; Ngai, T.J.; Lee, L.B.; et al. In vivo antitumor activity of SU11248, a novel tyrosine kinase inhibitor targeting vascular endothelial growth factor and platelet-derived growth factor receptors: Determination of a pharmacokinetic/pharmacodynamic relationship. Clin. Cancer Res. 2003, 9, 327–337. [Google Scholar]
- Abrams, T.J.; Lee, L.B.; Murray, L.J.; Pryer, N.K.; Cherrington, J.M. SU11248 inhibits KIT and platelet-derived growth factor receptor beta in preclinical models of human small cell lung cancer. Mol. Cancer Ther. 2003, 2, 471–478. [Google Scholar]
- Sonpavde, G.; Hutson, T.E.; Rini, B.I. Axitinib for renal cell carcinoma. Expert Opin. Investig. Drugs 2008, 17, 741–748. [Google Scholar] [CrossRef]
- Schindler, E.; Amantea, M.A.; Karlsson, M.O.; Friberg, L.E. A Pharmacometric Framework for Axitinib Exposure, Efficacy, and Safety in Metastatic Renal Cell Carcinoma Patients. CPT Pharmacomet. Syst. Pharmacol. 2017, 6, 373–382. [Google Scholar] [CrossRef] [PubMed]
- McDermott, D.F. Immunotherapy of metastatic renal cell carcinoma. Cancer 2009, 115, 2298–2305. [Google Scholar] [CrossRef] [PubMed]
- Akaza, H.; Tsukamoto, T.; Onishi, T.; Miki, T.; Kinouchi, T.; Naito, S. A low-dose combination therapy of interleukin-2 and interferon-alpha is effective for lung metastasis of renal cell carcinoma: A multicenter open study. Int. J. Clin. Oncol. 2006, 11, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Fyfe, G.; Fisher, R.I.; Rosenberg, S.A.; Sznol, M.; Parkinson, D.R.; Louie, A.C. Results of treatment of 255 patients with metastatic renal cell carcinoma who received high-dose recombinant interleukin-2 therapy. J. Clin. Oncol. 1995, 13, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Koreth, J.; Matsuoka, K.; Kim, H.T.; McDonough, S.M.; Bindra, B.; Alyea, E.P., 3rd; Armand, P.; Cutler, C.; Ho, V.T.; Treister, N.S.; et al. Interleukin-2 and regulatory T cells in graft-versus-host disease. N. Engl. J. Med. 2011, 365, 2055–2066. [Google Scholar] [CrossRef]
- Pace, L.; Vitale, S.; Dettori, B.; Palombi, C.; La Sorsa, V.; Belardelli, F.; Proietti, E.; Doria, G. APC activation by IFN-alpha decreases regulatory T cell and enhances Th cell functions. J. Immunol. 2010, 184, 5969–5979. [Google Scholar] [CrossRef]
- Ito, N.; Eto, M.; Nakamura, E.; Takahashi, A.; Tsukamoto, T.; Toma, H.; Nakazawa, H.; Hirao, Y.; Uemura, H.; Kagawa, S.; et al. STAT3 polymorphism predicts interferon-alfa response in patients with metastatic renal cell carcinoma. J. Clin. Oncol. 2007, 25, 2785–2791. [Google Scholar] [CrossRef]
- Motzer, R.J.; Bacik, J.; Murphy, B.A.; Russo, P.; Mazumdar, M. Interferon-alfa as a comparative treatment for clinical trials of new therapies against advanced renal cell carcinoma. J. Clin. Oncol. 2002, 20, 289–296. [Google Scholar] [CrossRef]
- Chow, S.; Galvis, V.; Pillai, M.; Leach, R.; Keene, E.; Spencer-Shaw, A.; Shablak, A.; Shanks, J.; Liptrot, T.; Thistlethwaite, F.; et al. High-dose interleukin2-a 10-year single-site experience in the treatment of metastatic renal cell carcinoma: Careful selection of patients gives an excellent outcome. J. Immunother. Cancer 2016, 4, 67. [Google Scholar] [CrossRef]
- Zhang, X.; Sun, G.; Zhao, J.; Shu, K.; Zhao, P.; Liu, J.; Yang, Y.; Tang, Q.; Chen, J.; Shen, P.; et al. Improved Long-Term Clinical Outcomes and Safety Profile Of Sunitinib Dosing Schedule with 4/2 Switched To 2/1 In Patients with Metastatic Renal Cell Carcinoma. J. Cancer 2018, 9, 3303–3310. [Google Scholar] [CrossRef]
- Motzer, R.J.; Hutson, T.E.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; de Souza, P.; Merchan, J.R.; et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Arasaratnam, M.; Gurney, H. Nivolumab in the treatment of advanced renal cell carcinoma. Future Oncol. 2018, 14, 1679–1689. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Median (Range), Number (%) | |
|---|---|---|
| IL-2 + IFNa | Sunutinib | |
| Number | 18 | 15 |
| Sex, male | 14 (78%) | 13 (87%) |
| Age | 68.5 (54–79) | 68 (41–76) |
| Previous nephrectomy | 16 (89%) | 15 (100%) |
| Previous partial nephrectomy | 2 (11%) | 0 (0%) |
| Previous radiation therapy | 1 (6%) | 1 (7%) |
| Hitology, clear cell carcinoma | 18 (100%) | 13 (87%) |
| Metastasis site | ||
| Regional lymphnode | 0 (0%) | 1 (7%) |
| Distant lymphnode | 2 (12%) | 2 (13%) |
| Lung | 15 (83%) | 11 (73%) |
| Bone | 1 (6%) | 4 (27%) |
| Liver | 0 (0%) | 0 (0%) |
| Pancreas | 3 (17%) | 2 (13%) |
| Contralateral kidney | 1 (6%) | 0 (0%) |
| Others | 3 (18%) | 0 (0%) |
| MSKCC risk factors * | ||
| 0 (favorable) | 5 (28%) | 6 (40%) |
| 1–2 (intermediate) | 13 (72%) | 9 (60%) |
| >3 (poor) | 0 (0%) | 0 (0%) |
| 1st-Line | 2nd-Line: Axitinib | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| IL-2 + IFNa (n = 18) | Sunitinib (n = 15) | (IL-2 + IFNa, n = 13) | (Sunitinib, n = 5) | |||||||
| ALL | >G3 | G4 | ALL | G3 | ALL | >G3 | G4 | ALL | G3 | |
|
Total, number (%) | 18 | 8 | 4 | 15 | 13 | 11 | 7 | 1 | 5 | 3 |
| (100) | (44) | (22) | (100) | (87) | (92) | (54) | (8) | (100) | (60) | |
| Adverse event, number | ||||||||||
| Chills | 3 | 1 | ||||||||
| Decreased appetite | 6 | 3 | 1 | 4 | 1 | 3 | ||||
| Diarrhoea | 4 | 2 | 1 | 3 | 1 | |||||
| Dyspepsia | 1 | |||||||||
| Epistaxis | 1 | |||||||||
| Face oedema | 1 | |||||||||
| Fatigue | 2 | 1 | 3 | |||||||
| Gastric perforation | 1 | 1 | 1 | |||||||
| Gastritis | 1 | |||||||||
| Gastrointestinal haemorrhage | 1 | |||||||||
| Hoarseness | 3 | |||||||||
| Hypertension | 2 | 1 | 7 | 6 | 9 | 7 | 3 | 2 | ||
| Hypothyroidism | 5 | 4 | ||||||||
| Interstitial lung disease | 1 | |||||||||
| Lymphopenia | 1 | 1 | ||||||||
| Malaise | 9 | 4 | ||||||||
| Pain | 1 | |||||||||
| Palmar-plantar erythrodysaesthesia | 8 | 1 | 2 | |||||||
| syndrome | ||||||||||
| Pancreatitis | 1 | 1 | 1 | |||||||
| Pleural effusion | 1 | |||||||||
| Proteinuria | 2 | 2 | 2 | 5 | 1 | 1 | 1 | |||
| Pyrexia | 13 | 5 | 1 | |||||||
| Stomatitis | 4 | 1 | 1 | |||||||
| Swelling | 1 | |||||||||
| Vomiting | 1 | |||||||||
| Laboratory abnormality number | ||||||||||
| Anaemia | 4 | 1 | 2 | |||||||
| Aspartate aminotransferase increased | 1 | |||||||||
| AST/ALT ratio abnormal | 1 | |||||||||
| Blood alkaline phosphatase increased | 1 | 1 | ||||||||
| Blood bilirubin increased | 1 | 1 | ||||||||
| Blood creatinine increased | 2 | 4 | 1 | 1 | 1 | |||||
| Hyperglycemia | 1 | 1 | 1 | |||||||
| Hypoalbuminemia | 1 | |||||||||
| Hyponatremia | 1 | 1 | ||||||||
| Neutrophil count decreased | 7 | 3 | 1 | 6 | 1 | 1 | ||||
| Platelet count decreased | 3 | 9 | 6 | 1 | ||||||
| White blood cell count decreased | 8 | 3 | 6 | 1 | 1 | |||||
| Response | 1st-Line | 2nd-Line Axitinib | ||||
|---|---|---|---|---|---|---|
| IL-2 + IFNa (n = 16) | Sunutinib (n = 13) | p-Value | IL-2 + 1FNa (n = 13, 81%) | Sunutinib (n = 5, 39%) | p-Value | |
| Objective response rate | 7 (43%) | 4 (31%) | 0.474 | 8 (62%) | 0 (0%) | 0.019 |
| Complete response | 0 (0%) | 0 (0%) | 1 (8%) | 0 (0%) | ||
| Partial response | 7 (43%) | 4 (31%) | 7 (54%) | 0 (0%) | ||
| Disease control rate | 13 (81%) | 15 (100%) | 0.099 | 11 (85%) | 3 (60%) | 0.261 |
| Stable disease | 6 (38%) | 9 (69%) | 3 (23%) | 3 (60%) | ||
| Progressive disease | 3 (19%) | 0 (0%) | 2 (15%) | 2 (40%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadono, Y.; Konaka, H.; Nohara, T.; Izumi, K.; Anai, S.; Fujimoto, K.; Koguchi, T.; Ishibashi, K.; Kawai, N.; Nakane, K.; et al. Efficacy and Safety of First-Line Cytokines versus Sunitinib and Second-Line Axitinib for Patients with Metastatic Renal Cell Carcinoma (ESCAPE Study): A Phase III, Randomized, Sequential Open-Label Study. Cancers 2023, 15, 2745. https://doi.org/10.3390/cancers15102745
Kadono Y, Konaka H, Nohara T, Izumi K, Anai S, Fujimoto K, Koguchi T, Ishibashi K, Kawai N, Nakane K, et al. Efficacy and Safety of First-Line Cytokines versus Sunitinib and Second-Line Axitinib for Patients with Metastatic Renal Cell Carcinoma (ESCAPE Study): A Phase III, Randomized, Sequential Open-Label Study. Cancers. 2023; 15(10):2745. https://doi.org/10.3390/cancers15102745
Chicago/Turabian StyleKadono, Yoshifumi, Hiroyuki Konaka, Takahiro Nohara, Kouji Izumi, Satoshi Anai, Kiyohide Fujimoto, Tomoyuki Koguchi, Kei Ishibashi, Noriyasu Kawai, Keita Nakane, and et al. 2023. "Efficacy and Safety of First-Line Cytokines versus Sunitinib and Second-Line Axitinib for Patients with Metastatic Renal Cell Carcinoma (ESCAPE Study): A Phase III, Randomized, Sequential Open-Label Study" Cancers 15, no. 10: 2745. https://doi.org/10.3390/cancers15102745
APA StyleKadono, Y., Konaka, H., Nohara, T., Izumi, K., Anai, S., Fujimoto, K., Koguchi, T., Ishibashi, K., Kawai, N., Nakane, K., Iba, A., Masumori, N., Takahara, S., & Mizokami, A. (2023). Efficacy and Safety of First-Line Cytokines versus Sunitinib and Second-Line Axitinib for Patients with Metastatic Renal Cell Carcinoma (ESCAPE Study): A Phase III, Randomized, Sequential Open-Label Study. Cancers, 15(10), 2745. https://doi.org/10.3390/cancers15102745