
Patient’s Desire and Real Availability Concerning Supportive Measures Accompanying Radical Prostatectomy: Differences between Certified Prostate Cancer Centers and Non-Certified Centers Based on Patient-Reported Outcomes within the Cross-Sectional Study Improve

 ,
,  ,
,  , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
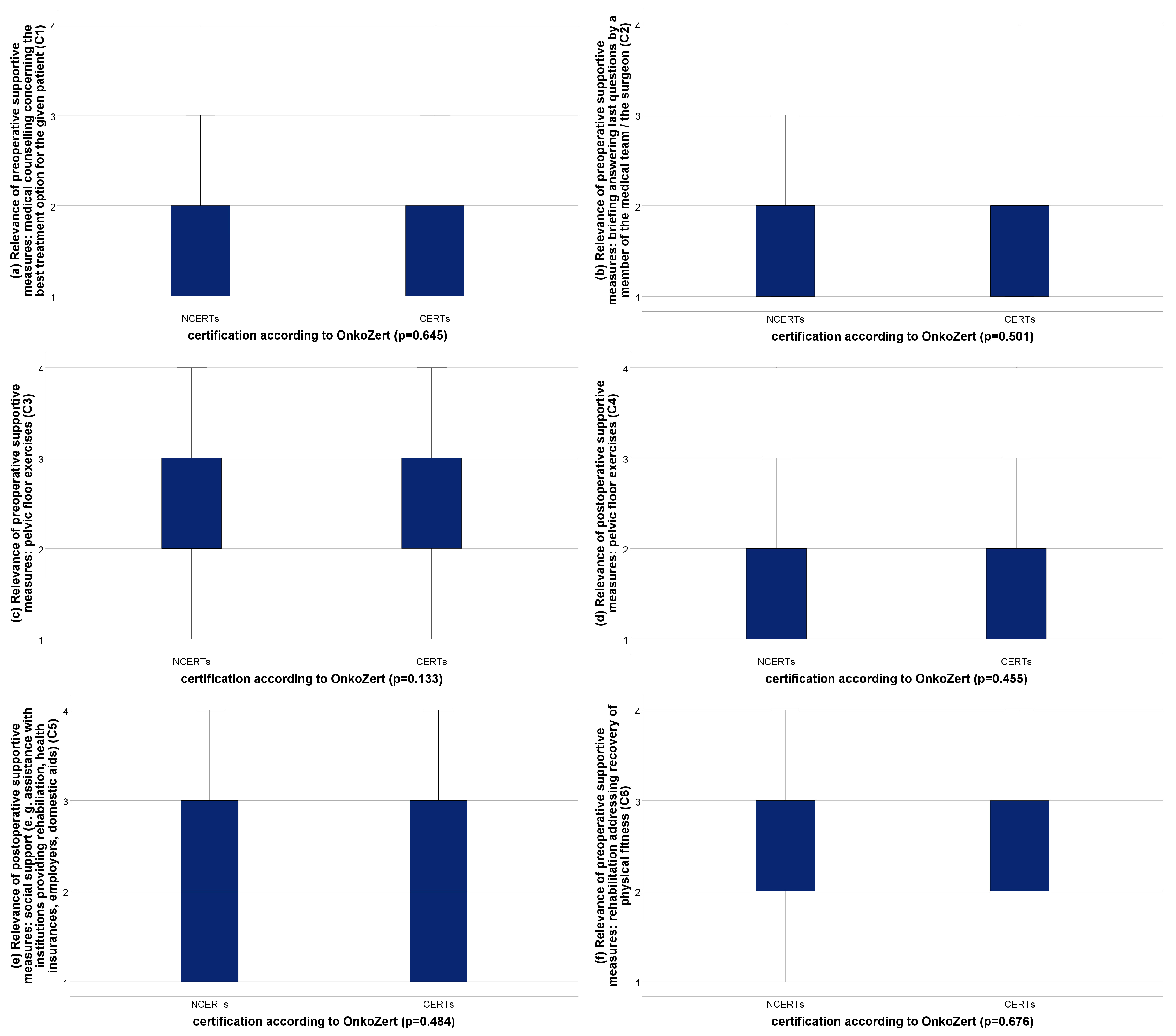
- preoperative medical counselling concerning the best treatment option for the given patient
- preoperative briefing answering last questions given by a member of the medical team/the surgeon
- preoperative pelvic floor exercises
- preoperative genetic counselling
- preoperative psycho-oncological support
- preoperative integration in a support group of prostate cancer patients
- postoperative pelvic floor exercises
- sufficient postoperative social support
- postoperative rehabilitation addressing recovery of physical fitness
- postoperative genetic counselling
- postoperative nutrition consultation
- postoperative psycho-oncological support
- postoperative access to a pain service
- postoperative integration into a support group of prostate cancer patients
- postoperative counselling regarding therapy options for possible erectile dysfunction.
3. Results
4. Discussion
- Patients have a very high need for pre-operative counselling concerning the best treatment option, which is not met sufficiently. Apparently, patients highly appreciate meeting their surgeon to answer any last questions prior to the surgical procedure. These two important points have to be considered even in economically driven healthcare systems that are associated with an ongoing increase in physicians’ workload.
- Contemporary studies have demonstrated that up to 31% of patients suffering from different levels of urinary incontinence which is defined as a need to be provided with at least one pad per day [30]. Therefore, it is understandable that patients show a high interest in perioperative supportive measures concerning pelvic floor exercises. In recent years, there is increasing evidence for additional pre-operative pelvic floor exercises as they are attributed to an increase in continence rates especially during the first months following radical prostatectomy [31]. Contrarily, our study reveals, as one of its most important findings, that patients are not counselled sufficiently about the potential impact of preoperative pelvic floor exercises.
- In our study, 25% of the entire cohort were aged 63 or younger at the time of radical prostatectomy. About 27% of them were professionally active at this time point. Hence, it is not surprising that postoperative rehabilitation addressing the recovery of physical fitness and sufficient social support were rated as highly relevant by the patients. Remarkably, no sufficient training offers and no adequate counselling concerning rational physical rehabilitation measures were offered to a substantial proportion of patients. In contrast, offering social support ensuring access to rehabilitation and improving communication with the employers of the patients seem to be better integrated into the daily routine of postoperative care.
- Surprisingly, our study found that perioperative offers concerning psycho-oncological support and the integration of patients with prostate cancer into a support group were not rated as very relevant by the patients. As there is a number of studies demonstrating the substantial need for such offers, it seems of utmost importance that these offers are explained to patients more intensively by their physicians [32,33].
- Interestingly, the offer of postoperative counselling regarding the therapy options for possible erectile dysfunction was not rated as very relevant by the patients, although the predefined definition for a very relevant supportive measure was only just missed. An impairment of erectile function, including clinically manifest erectile dysfunction, was reported in up to 88% of patients following radical prostatectomy, which assumes the high relevance of such supportive offers to patients. Again, this highlights the need for urologists to better communicate with their patients about existing supportive measures and their potential benefit to the patients [34].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Collaborators
References
- Eastham, J.A.; Auffenberg, G.B.; Barocas, D.A.; Chou, R.; Crispino, T.; Davis, J.W.; Eggener, S.; Horwitz, E.M.; Kane, C.J.; Kirkby, E.; et al. Clinically Localized Prostate Cancer: AUA/ASTRO Guideline, Part II: Principles of Active Surveillance, Principles of Surgery, and Follow-Up. J. Urol. 2022, 208, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Eastham, J.A.; Auffenberg, G.B.; Barocas, D.A.; Chou, R.; Crispino, T.; Davis, J.W.; Eggener, S.; Horwitz, E.M.; Kane, C.J.; Kirkby, E.; et al. Clinically Localized Prostate Cancer: AUA/ASTRO Guideline, Part I: Introduction, Risk Assessment, Staging, and Risk-Based Management. J. Urol. 2022, 208, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Giesler, R.B.; Miles, B.J.; Cowen, M.E.; Kattan, M.W. Assessing quality of life in men with clinically localized prostate cancer: Development of a new instrument for use in multiple settings. Qual. Life Res. 2000, 9, 645–665. [Google Scholar] [CrossRef]
- Groenvold, M.; Klee, M.C.; Sprangers, M.A.; Aaronson, N.K. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J. Clin. Epidemiol. 1997, 50, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, R.M.; Lo, M.; Clark, J.A.; Albertsen, P.C.; Barry, M.J.; Goodman, M.; Penson, D.F.; Stanford, J.L.; Stroup, A.M.; Hamilton, A.S. Treatment Decision Regret Among Long-Term Survivors of Localized Prostate Cancer: Results From the Prostate Cancer Outcomes Study. J. Clin. Oncol. 2017, 35, 2306–2314. [Google Scholar] [CrossRef]
- Lardas, M.; Liew, M.; van den Bergh, R.C.; De Santis, M.; Bellmunt, J.; Van den Broeck, T.; Cornford, P.; Cumberbatch, M.G.; Fossati, N.; Gross, T.; et al. Quality of Life Outcomes after Primary Treatment for Clinically Localised Prostate Cancer: A Systematic Review. Eur. Urol. 2017, 72, 869–885. [Google Scholar] [CrossRef]
- Potosky, A.L.; Harlan, L.C.; Stanford, J.L.; Gilliland, F.D.; Hamilton, A.S.; Albertsen, P.C.; Eley, J.W.; Liff, J.M.; Deapen, D.; Stephenson, R.A.; et al. Prostate cancer practice patterns and quality of life: The Prostate Cancer Outcomes Study. J. Natl. Cancer Inst. 1999, 91, 1719–1724. [Google Scholar] [CrossRef]
- van Andel, G.; Bottomley, A.; Fossa, S.D.; Efficace, F.; Coens, C.; Guerif, S.; Kynaston, H.; Gontero, P.; Thalmann, G.; Akdas, A.; et al. An international field study of the EORTC QLQ-PR25: A questionnaire for assessing the health-related quality of life of patients with prostate cancer. Eur. J. Cancer 2008, 44, 2418–2424. [Google Scholar] [CrossRef]
- Wei, J.T.; Dunn, R.L.; Litwin, M.S.; Sandler, H.M.; Sanda, M.G. Development and validation of the expanded prostate cancer index composite (EPIC) for comprehensive assessment of health-related quality of life in men with prostate cancer. Urology 2000, 56, 899–905. [Google Scholar] [CrossRef]
- Kowalski, C.; Graeven, U.; von Kalle, C.; Lang, H.; Beckmann, M.W.; Blohmer, J.U.; Burchardt, M.; Ehrenfeld, M.; Fichtner, J.; Grabbe, S.; et al. Shifting cancer care towards Multidisciplinarity: The cancer center certification program of the German cancer society. BMC Cancer 2017, 17, 850. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, C.; Ferencz, J.; Albers, P.; Fichtner, J.; Wiegel, T.; Feick, G.; Wesselmann, S. Quality assessment in prostate cancer centers certified by the German Cancer Society. World J. Urol. 2016, 34, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Griesshammer, E.; Adam, H.; Sibert, N.T.; Wesselmann, S. Implementing quality metrics in European Cancer Centers (ECCs). World J. Urol. 2021, 39, 49–56. [Google Scholar] [CrossRef]
- Kowalski, C.; Ferencz, J.; Singer, S.; Weis, I.; Wesselmann, S. Frequency of psycho-oncologic and social service counseling in cancer centers relative to center site and hospital characteristics: Findings from 879 center sites in Germany, Austria, Switzerland, and Italy. Cancer 2016, 122, 3538–3545. [Google Scholar] [CrossRef]
- Beyer, B.; Huland, H.; Feick, G.; Graefen, M. “Expanded prostate cancer index composite” (EPIC-26): Results of functional treatment in patients with localized prostate cancer. Urologe A 2015, 54, 1591–1595. [Google Scholar] [CrossRef]
- Sibert, N.T.; Dieng, S.; Oesterle, A.; Feick, G.; Carl, G.; Steiner, T.; Minner, J.; Roghmann, F.; Kaftan, B.; Zengerling, F.; et al. Psychometric validation of the German version of the EPIC-26 questionnaire for patients with localized and locally advanced prostate cancer. World J. Urol. 2021, 39, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Szymanski, K.M.; Wei, J.T.; Dunn, R.L.; Sanda, M.G. Development and validation of an abbreviated version of the expanded prostate cancer index composite instrument for measuring health-related quality of life among prostate cancer survivors. Urology 2010, 76, 1245–1250. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Hiess, M.; Ponholzer, A.; Lamche, M.; Schramek, P.; Seitz, C. The Clavien-Dindo classification of complications used for radical prostatectomy. Wien. Med. Wochenschr. 2014, 164, 297–301. [Google Scholar] [CrossRef]
- Wolff, I.; Burchardt, M.; Gilfrich, C.; Peter, J.; Baunacke, M.; Thomas, C.; Huber, J.; Gillitzer, R.; Sikic, D.; Fiebig, C.; et al. Patients Regret Their Choice of Therapy Significantly Less Frequently after Robot-Assisted Radical Prostatectomy as Opposed to Open Radical Prostatectomy: Patient-Reported Results of the Multicenter Cross-Sectional IMPROVE Study. Cancers 2022, 14, 5356. [Google Scholar] [CrossRef]
- Meissner, V.H.; Simson, B.W.; Dinkel, A.; Schiele, S.; Ankerst, D.P.; Lunger, L.; Gschwend, J.E.; Herkommer, K. Treatment decision regret in long-term survivors after radical prostatectomy: A longitudinal study. BJU Int. 2022, 131, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Choiniere, R.; Richard, P.O.; Morin, M.; Tu, L.M.; Guyatt, G.H.; Violette, P.D. Evaluation of benefits and harms of surgical treatments for post-radical prostatectomy urinary incontinence: A systematic review and meta-analysis protocol. F1000Res 2019, 8, 1155. [Google Scholar] [CrossRef] [PubMed]
- Neal, D.E.; Metcalfe, C.; Donovan, J.L.; Lane, J.A.; Davis, M.; Young, G.J.; Dutton, S.J.; Walsh, E.I.; Martin, R.M.; Peters, T.J.; et al. Ten-year Mortality, Disease Progression, and Treatment-related Side Effects in Men with Localised Prostate Cancer from the ProtecT Randomised Controlled Trial According to Treatment Received. Eur. Urol. 2020, 77, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Pinkhasov, R.M.; Lee, T.; Huang, R.; Berkley, B.; Pinkhasov, A.M.; Dodge, N.; Loecher, M.S.; James, G.; Pop, E.; Attwood, K.; et al. Prediction of Incontinence after Robot-Assisted Radical Prostatectomy: Development and Validation of a 24-Month Incontinence Nomogram. Cancers 2022, 14, 1644. [Google Scholar] [CrossRef] [PubMed]
- Park, J.J.; Kwon, A.; Park, J.Y.; Shim, S.R.; Kim, J.H. Efficacy of Pelvic Floor Exercise for Post-prostatectomy Incontinence: Systematic Review and Meta-analysis. Urology 2022, 168, 175–182. [Google Scholar] [CrossRef]
- Philippou, Y.A.; Jung, J.H.; Steggall, M.J.; O’Driscoll, S.T.; Bakker, C.J.; Bodie, J.A.; Dahm, P. Penile rehabilitation for postprostatectomy erectile dysfunction. Cochrane Database Syst. Rev. 2018, 10, CD012414. [Google Scholar] [CrossRef]
- Yang, J.M.; Ye, H.; Long, Y.; Zhu, Q.; Huang, H.; Xie, H.Y.; Luo, Y.; Zhong, Y.B.; Chen, J.; Wang, M.Y. Effect of pelvic floor muscle training on urinary incontinence after radical prostatectomy: An umbrella review of meta-analysis and systematic review. Clin. Rehabil. 2023, 37, 494–515. [Google Scholar] [CrossRef]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Metcalfe, C.; Davis, M.; Turner, E.L.; Martin, R.M.; Young, G.J.; Walsh, E.I.; Bryant, R.J.; et al. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N. Engl. J. Med. 2023, 388, 1547–1558. [Google Scholar] [CrossRef]
- Klinkhammer-Schalke, M.; Steinger, B.; Koller, M.; Zeman, F.; Furst, A.; Gumpp, J.; Obermaier, R.; Piso, P.; Lindberg-Scharf, P.; Regensburg Qo, L.S.G. Diagnosing deficits in quality of life and providing tailored therapeutic options: Results of a randomised trial in 220 patients with colorectal cancer. Eur. J. Cancer 2020, 130, 102–113. [Google Scholar] [CrossRef]
- Lardas, M.; Grivas, N.; Debray, T.P.A.; Zattoni, F.; Berridge, C.; Cumberbatch, M.; Van den Broeck, T.; Briers, E.; De Santis, M.; Farolfi, A.; et al. Patient- and Tumour-related Prognostic Factors for Urinary Incontinence After Radical Prostatectomy for Nonmetastatic Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. Focus. 2022, 8, 674–689. [Google Scholar] [CrossRef]
- Rangganata, E.; Rahardjo, H.E. The Effect of Preoperative Pelvic Floor Muscle Training on Incontinence Problems after Radical Prostatectomy: A Meta-Analysis. Urol. J. 2021, 18, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Baba, N.; Schrage, T.; Hartmann, A.; Baba, K.; Wuensch, A.; Schultze-Seemann, W.; Weis, J.; Joos, A. Mental distress and need for psychosocial support in prostate cancer patients: An observational cross-sectional study. Int. J. Psychiatry Med. 2021, 56, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Jahnen, M.; Lehner, L.; Meissner, V.H.; Andreas, D.; Schiele, S.; Schulwitz, H.; Gschwend, J.E.; Herkommer, K. Cancer-related self-perception in men affected by prostate cancer after radical prostatectomy. J. Cancer Surviv. 2022; Online ahead of print. [Google Scholar] [CrossRef]
- Capogrosso, P.; Pozzi, E.P.; Celentano, V.; Sanchez-Salas, R.; Salonia, A. Erectile Recovery After Radical Pelvic Surgery: Methodological Challenges and Recommendations for Data Reporting. J. Sex. Med. 2020, 17, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, L.M.; Cullen, J.; Kim, D.J.; Elsamanoudi, S.; Hudak, J.; Colston, M.; Travis, J.; Kuo, H.C.; Rice, K.R.; Porter, C.R.; et al. Longitudinal regret after treatment for low- and intermediate-risk prostate cancer. Cancer 2017, 123, 4252–4258. [Google Scholar] [CrossRef]
- Baunacke, M.; Schmidt, M.L.; Groeben, C.; Borkowetz, A.; Thomas, C.; Koch, R.; Chun, F.K.H.; Ihrig, A.; Weissbach, L.; Huber, J. Decision Regret after Radical Prostatectomy does Not Depend on Surgical Approach: 6-Year Followup of a Large German Cohort Undergoing Routine Care. J. Urol. 2020, 203, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Davison, B.J.; So, A.I.; Goldenberg, S.L. Quality of life, sexual function and decisional regret at 1 year after surgical treatment for localized prostate cancer. BJU Int. 2007, 100, 780–785. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Entire Cohort (n = 750) | CERTs (n = 480) | NCERTs (n = 270) | p Value |
|---|---|---|---|---|
| Age (n = 750): | <0.001 | |||
| median (IQR) in years | 68 (63–72) | 67 (62–71) | 69 (64–73) | |
| Personal relationship status (n = 747): | 0.071 | |||
| fixed partnership | 675 (90.4%) | 440 (91.9%) | 235 (87.7%) | |
| no fixed partnership | 72 (9.6%) | 39 (8.1%) | 33 (12.3%) | |
| Social security status (n = 750): | 0.864 | |||
| statutory health insurance | 548 (73.1%) | 352 (73.3%) | 196 (72.6%) | |
| private health insurance | 202 (26.9%) | 128 (26.7%) | 74 (27.4%) | |
| Educational qualification (n = 747): | 0.566 | |||
| university or technical college degree | 237 (31.7%) | 156 (32.6%) | 81 (30.2%) | |
| no such qualification | 510 (68.3%) | 323 (67.4%) | 187 (69.8%) | |
| Professional status (n = 745): | 0.069 | |||
| professionally active or professional activity scheduled again | 198 (26.6%) | 138 (28.9%) | 60 (22.5%) | |
| retired | 547 (73.4%) | 340 (71.1%) | 207 (77.5%) | |
| Time interval between RP and survey in month (IQR) (n = 750) | 15 (11–21) | 14 (11–21) | 17 (12–21) | <0.001 |
| Clinical decision making regarding surgical approach (n = 742): | 0.051 | |||
| Decision by physician alone (passive decision) | 181 (24.4%) | 105 (22.0%) | 76 (28.7%) | |
| Consensual | ||||
| (patient and physician together) | 361 (48.6%) | 232 (48.6%) | 129 (48.7%) | |
| Decision by patient alone (active decision) | 200 (27.0%) | 140 (29.4%) | 60 (22.6%) | |
| Center’s level of care: | <0.001 | |||
| non-university center | 432 (57.6%) | 162 (33.8%) | 270 (100%) | |
| university (n = 750) | 318 (42.4%) | 318 (66.2%) | 0 | |
| Center’s mean RP caseload per year 2018–2020 (IQR) (n = 750) | 87 (52–134) | 125 (67–150) | 29 (19–92) | <0.001 |
| Preoperative PSA level in ng/mL (IQR) (n = 703) | 7.9 (5.6–12.1) | 7.7 (5.4–12.3) | 8.4 (6.0–12.0) | 0.224 |
| ISUP group 1–2 | 438 (58.4%) | 262 5(54.6%) | 176 (65.2%) | 0.005 |
| (Gleason score 3 + 3 = 6 and 3 + 4 = 7) | ||||
| ISUP group 3–5 | 312 (41.6%) | 218 (45.4%) | 94 (34.8%) | |
| (Gleason score 4 + 3 = 7, 4 + 4 = 8, 3 + 5 = 8, 5 + 3 = 8, 4 + 5 = 9, 5 + 4 = 9, and 5 + 5 = 10) | ||||
| (n = 750) | ||||
| pT stage (n = 750): | 0.057 | |||
| pT2 | 482 (64.3%) | 296 (61.7%) | 186 (68.9%) | |
| pT3 + pT4 | 268 (35.7%) | 184 (38.3%) | 84 (31.1%) | |
| pN stage (n = 749): | 0.283 | |||
| pN0 + pNx | 683 (91.2%) | 441 (92.1%) | 242 (89.6%) | |
| pN1 | 66 (8.8%) | 38 (7.9%) | 28 (10.4%) | |
| Surgical margin status (n = 750): | 0.042 | |||
| R0 | 568 (75.7%) | 352 (73.3%) | 216 (80.0%) | |
| R1 | 182 (24.3%) | 128 (26.7%) | 54 (20.0%) | |
| no adjuvant local radiation adjuvant local radiation (n = 746) | 614 (82.3%) 132 (17.7%) | 389 (81.2%) 90 (18.8%) | 225 (84.3%) 42 (15.7%) | 0.318 |
| Nerve sparing (n = 703): | 0.074 | |||
| no nerve sparing | 275 (39.1%) | 200 (41.7%) | 75 (33.6%) | |
| unilateral nerve sparing | 108 (15.4%) | 75 (15.6%) | 33 (14.8%) | |
| bilateral nerve sparing | 320 (45.5%) | 205 (42.7%) | 115 (51.6%) | |
| Postoperative complications according to CDC grades (n = 703): | 0.087 | |||
| 0–2 | 662 (94.2%) | 447 (93.1%) | 215 (96.4%) | |
| 3–5 | 41 (5.8%) | 33 (6.9%) | 8 (3.6%) | |
| Urinary stress incontinence (n = 747): | 0.131 | |||
| 0–1 safety pad/day | 594 (79.5%) | 389 (81.2%) | 205 (76.5%) | |
| >1 pad/day | 153 (20.5%) | 90 (18.8%) | 63 (23.5%) | |
| Surgical approach (n = 750): | <0.001 | |||
| open surgical procedures | 325 (43.3%) | 110 (22.9%) | 215 (79.6%) | |
| laparoscopic (not robot- | 57 (7.6%) | 42 (8.8%) | 15 (5.6%) | |
| assisted) | ||||
| robot-assisted procedures | 368 (49.1%) | 328 (68.3%) | 40 (14.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolff, I.; Burchardt, M.; Peter, J.; Thomas, C.; Sikic, D.; Fiebig, C.; Promnitz, S.; Hoschke, B.; Burger, M.; Schnabel, M.J.; et al. Patient’s Desire and Real Availability Concerning Supportive Measures Accompanying Radical Prostatectomy: Differences between Certified Prostate Cancer Centers and Non-Certified Centers Based on Patient-Reported Outcomes within the Cross-Sectional Study Improve. Cancers 2023, 15, 2830. https://doi.org/10.3390/cancers15102830
Wolff I, Burchardt M, Peter J, Thomas C, Sikic D, Fiebig C, Promnitz S, Hoschke B, Burger M, Schnabel MJ, et al. Patient’s Desire and Real Availability Concerning Supportive Measures Accompanying Radical Prostatectomy: Differences between Certified Prostate Cancer Centers and Non-Certified Centers Based on Patient-Reported Outcomes within the Cross-Sectional Study Improve. Cancers. 2023; 15(10):2830. https://doi.org/10.3390/cancers15102830
Chicago/Turabian StyleWolff, Ingmar, Martin Burchardt, Julia Peter, Christian Thomas, Danijel Sikic, Christian Fiebig, Sören Promnitz, Bernd Hoschke, Maximilian Burger, Marco J. Schnabel, and et al. 2023. "Patient’s Desire and Real Availability Concerning Supportive Measures Accompanying Radical Prostatectomy: Differences between Certified Prostate Cancer Centers and Non-Certified Centers Based on Patient-Reported Outcomes within the Cross-Sectional Study Improve" Cancers 15, no. 10: 2830. https://doi.org/10.3390/cancers15102830
APA StyleWolff, I., Burchardt, M., Peter, J., Thomas, C., Sikic, D., Fiebig, C., Promnitz, S., Hoschke, B., Burger, M., Schnabel, M. J., Gilfrich, C., Löbig, N., Harke, N. N., Distler, F. A., & May, M. (2023). Patient’s Desire and Real Availability Concerning Supportive Measures Accompanying Radical Prostatectomy: Differences between Certified Prostate Cancer Centers and Non-Certified Centers Based on Patient-Reported Outcomes within the Cross-Sectional Study Improve. Cancers, 15(10), 2830. https://doi.org/10.3390/cancers15102830