
Preclinical Evaluation of a Microwave-Based Accessory Device for Colonoscopy in an In Vivo Porcine Model with Colorectal Polyps

 , ,
, ,  , , , , and
, , , , and 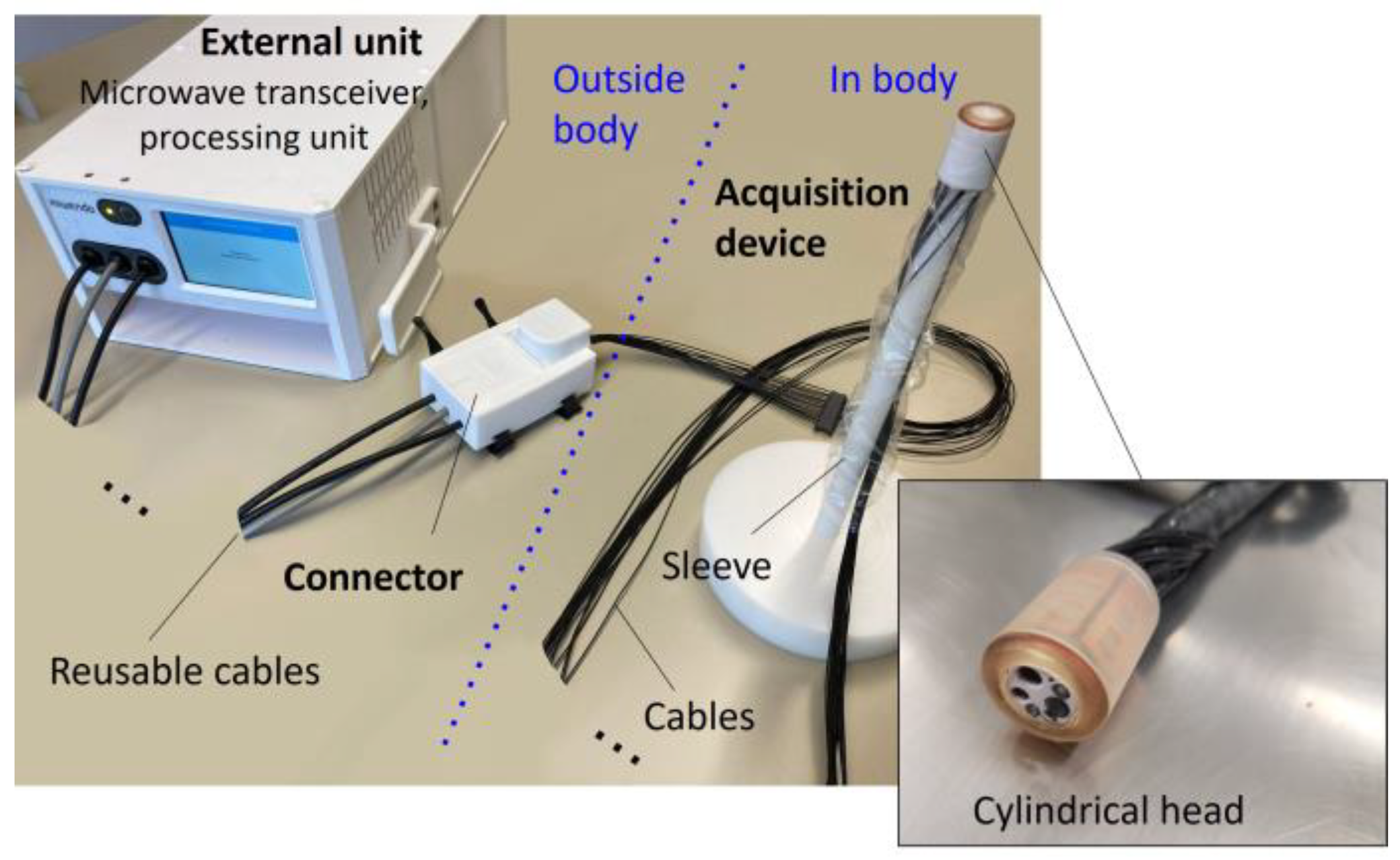{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Pig Model
2.2. Microwave-Based Device Description
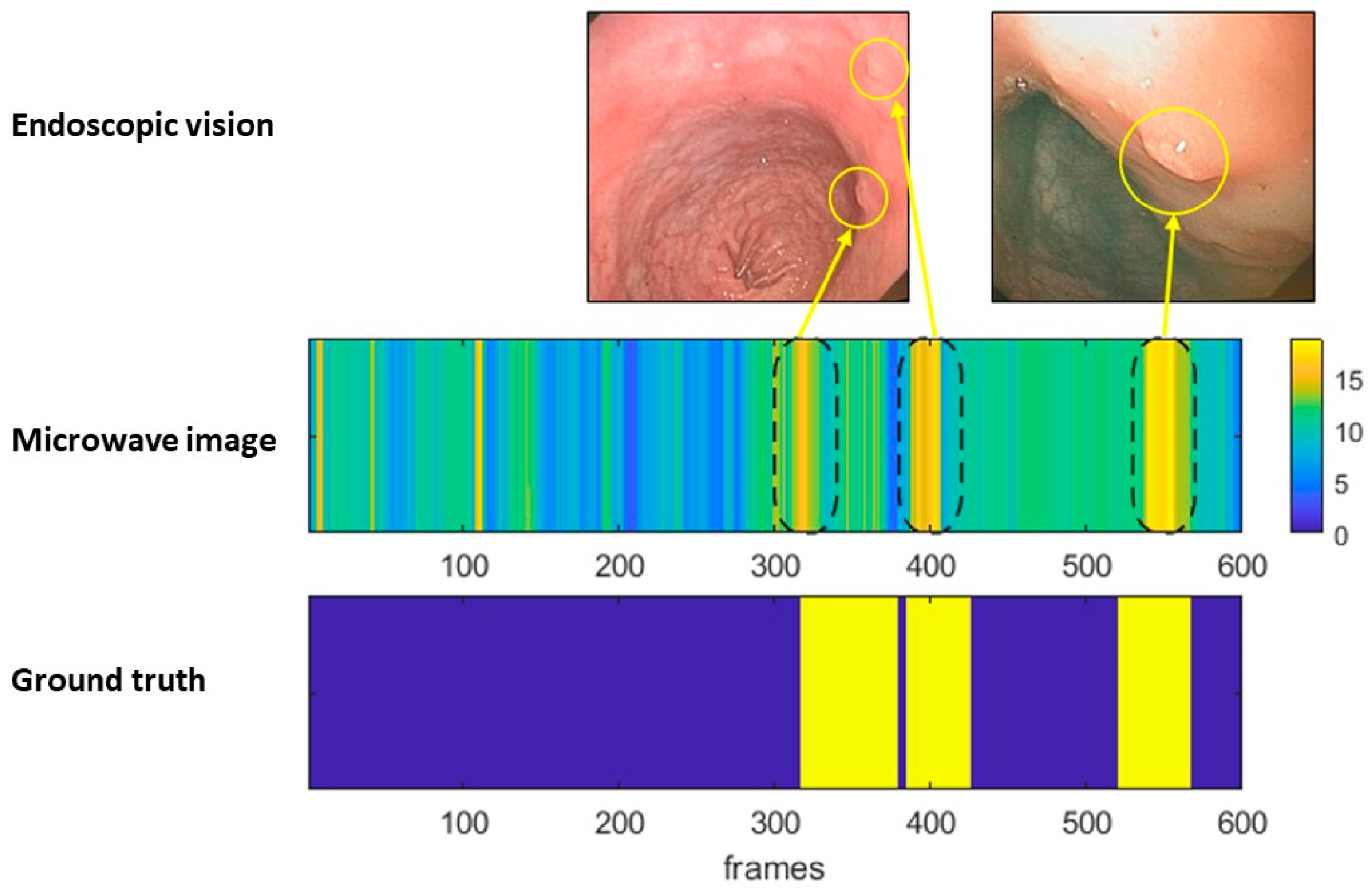
2.3. Description of Microwave Imaging Method for Colonoscopy
2.4. Study Protocol
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xi, Y.; Xu, P. Global colorectal cancer burden in 2020 and projections to 2040. Transl. Oncol. 2021, 14, 101174. [Google Scholar] [CrossRef]
- Müller, A.D.; Sonnenberg, A. Prevention of colorectal cancer by flexible endoscopy and polypectomy. A case-control study of 32,702 veterans. Ann. Intern. Med. 1995, 123, 904–910. [Google Scholar] [CrossRef] [PubMed]
- Winawer, S.J.; Zauber, A.G.; Ho, M.N.; O’Brien, M.J.; Gottlieb, L.S.; Sternberg, S.S.; Waye, J.D.; Schapiro, M.; Bond, J.H.; Panish, J.F.; et al. Prevention of Colorectal Cancer by Colonoscopic Polypectomy. N. Engl. J. Med. 1993, 29, 1977–1981. [Google Scholar] [CrossRef] [PubMed]
- van Rijn, J.C.; Reitsma, J.B.; Stoker, J.; Bossuyt, P.M.; van Deventer, S.J.; Dekker, E. Polyp miss rate determined by tandem colonoscopy: A systematic review. Am. J. Gastroenterol. 2006, 101, 343–350. [Google Scholar] [CrossRef]
- Samadder, N.J.; Curtin, K.; Tuohy, T.M.; Pappas, L.; Boucher, K.; Provenzale, D.; Rowe, K.G.; Mineau, G.P.; Smith, K.; Pimentel, R.; et al. Characteristics of missed or interval colorectal cancer and patient survival: A population-based study. Gastroenterology 2014, 146, 950–960. [Google Scholar] [CrossRef]
- Lee, T.; Rees, C.; Blanks, R.; Moss, S.M.; Nickerson, C.; Wright, K.C.; James, P.W.; McNally, R.J.Q.; Patnick, J.; Rutter, M.D. Colonoscopic factors associated with adenoma detection in a national colorectal cancer screening program. Endoscopy 2014, 46, 203–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- East, J.E.; Saunders, B.P.; Burling, D.; Boone, D.; Halligan, S.; Taylor, S.A. Surface visualization at CT colonography simulated colonoscopy: Effect of varying field of view and retrograde view. Am. J. Gastroenterol. 2007, 102, 2529–2535. [Google Scholar] [CrossRef]
- ASGE Technology Committee; Konda, V.; Chauhan, S.S.; Abu Dayyeh, B.K.; Hwang, J.H.; Komanduri, S.; Manfredi, M.A.; Maple, J.T.; Murad, F.M.; Siddiqui, U.D.; et al. Endoscopes and devices to improve colon polyp detection. Gastrointest. Endosc. 2015, 81, 1122–1129. [Google Scholar] [CrossRef]
- Kaminski, M.F.; Regula, J.; Kraszewska, E.; Polkowski, M.; Wojciechowska, U.; Didkowska, J.; Zwierko, M.; Rupinski, M.; Nowacki, M.P.; Butruk, E. Quality indicators for colonoscopy and the risk of interval cancer. N. Engl. J. Med. 2010, 362, 1795–1803. [Google Scholar] [CrossRef] [Green Version]
- Corley, D.A.; Jensen, C.D.; Marks, A.R.; Zhao, W.K.; Lee, J.K.; Doubeni, C.A.; Zauber, A.G.; de Boer, J.; Fireman, B.H.; Schottinger, J.E.; et al. Adenoma detection rate and risk of colorectal cancer and death. N. Engl. J. Med. 2014, 370, 1298–1306. [Google Scholar] [CrossRef] [Green Version]
- Repici, A.; Badalamenti, M.; Maselli, R.; Correale, L.; Radaelli, F.; Rondonotti, E. Efficacy of Real-Time Computer-Aided Detection of Colorectal Neoplasia in a Randomized Trial. Gastroenterology 2020, 159, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Nikolova, N.K. Introduction to Microwave Imaging; Cambridge University Press: Cambridge, UK, 2017. [Google Scholar] [CrossRef]
- O’Loughlin, D.; O’Halloran, M.; Moloney, B.M.; Glavin, M.; Jones, E.; Elahi, M.A. Microwave breast imaging: Clinical advances and remaining challenges. IEEE Trans. Biomed. Eng. 2018, 65, 2580–2590. [Google Scholar] [CrossRef]
- Guardiola, M.; Buitrago, S.; Fernández-Esparrach, G.; O’Callaghan, J.; Romeu, J.; Cuatrecasas, M.; Córdova, H.; González Ballester, M.A.; Cámara, O. Dielectric properties of colon polyps, cancer, and normal mucosa: Ex vivo measurements from 0.5 to 20 GHz. Med. Phys. 2018, 45, 3768–3782. [Google Scholar] [CrossRef] [Green Version]
- Garrido, A.; Sont, R.; Dghoughi, W.; Marcoval, S.; Romeu, J.; Fernández-Esparrach, G.; Belda, I.; Guardiola, M. Phantom Validation of Polyp Automatic Detection using Microwave Endoscopy for Colorectal Cancer Prevention and Early Detection. IEEE Access 2021, 9, 148048–148059. [Google Scholar] [CrossRef]
- Fernández-Esparrach, G.; Garrido, A.; Sont, R.; Dghoughi, W.; Marcoval, S.; Cuatrecasas, M.; López-Prades, S.; de Lacy, F.B.; Pellisé, M.; Belda, I.; et al. Microwave-Based Colonoscopy: Preclinical Evaluation in an Ex Vivo Human Colon Model. Gastroenterol. Res. Pract. 2022, 2022, 9522737. [Google Scholar] [CrossRef] [PubMed]
- Hirst, A.; Philippou, Y.; Blazeby, J.; Campbell, B.; Campbell, M.; Feinberg, J.; Rovers, M.; Blencowe, N.; Pennell, C.; Quinn, T.; et al. No surgical innovation without evaluation: Evolution and further development of the IDEAL framework and recommendations. Ann. Surg. 2019, 269, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flisikowska, T.; Merkl, C.; Landmann, M.; Eser, S.; Rezaei, N.; Cui, X.; Kurome, M.; Zakhartchenko, V.; Kessler, B.; Wieland, H.; et al. A porcine model of familial adenomatous polyposis. Gastroenterology 2012, 143, 1173–1175. [Google Scholar] [CrossRef]
- Troya, J.; Krenzer, A.; Flisikowski, K.; Sudarevic, B.; Banck, M.; Hann, A.; Puppe, F.; Meining, A. New concept for colonoscopy including side optics and artificial intelligence. Gastrointest. Endosc. 2022, 95, 794–798. [Google Scholar] [CrossRef]
- Guardiola, M.; Djafri, K.; Challal, M.; González Ballester, M.A.; Fernández-Esparrach, G.; Cámara, O.; Romeu, J. Design and Evaluation of an Antenna Applicator for a Microwave Colonoscopy System. IEEE Trans. Antennas Propag. 2019, 67, 4968–4977. [Google Scholar] [CrossRef]
- Lazebnik, M.; Popovic, D.; McCartney, L.; Watkins, C.B.; Lindstrom, M.J.; Harter, J.; Sewall, S.; Ogilvie, T.; Magliocco, A.; Breslin, T.M.; et al. A large-scale study of the ultrawideband microwave dielectric properties of normal, benign and malignant breast tissues obtained from cancer surgeries. Phys. Med. Biol. 2007, 52, 6093–6115. [Google Scholar] [CrossRef]
- AlSawaftah, N.; El-Abed, S.; Dhou, S.; Zakaria, A. Microwave Imaging for Early Breast Cancer Detection: Current State, Challenges, and Future Directions. J. Imaging 2022, 8, 123. [Google Scholar] [CrossRef] [PubMed]
- Bisschops, R.; East, J.E.; Hassan, C.; Hazewinkel, Y.; Kaminski, M.F.; Neumann, H.; Pellisé, M.; Antonelli, G.; Bustamante, M.; Coron, E.; et al. Advanced imaging for detection and differentiation of colorectal neoplasia: European Society of Gastrointestinal Endoscopy (ESGE) Guideline-update 2019. Endoscopy 2019, 51, 1155–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leufkens, A.M.; DeMarco, D.C.; Rastogi, A.; Akerman, P.A.; Azzouzi, K.; Rothstein, R.I.; Vleggaar, F.P.; Repici, A.; Rando, G.; Okolo, P.I.; et al. Effect of a retrograde-viewing device on adenoma detection rate during colonoscopy: The TERRACE study. Gastrointest. Endosc. 2011, 73, 480–489. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garrido, A.; Guardiola, M.; Neira, L.M.; Sont, R.; Córdova, H.; Cuatrecasas, M.; Flisikowski, K.; Troya, J.; Sanahuja, J.; Winogrodzki, T.; et al. Preclinical Evaluation of a Microwave-Based Accessory Device for Colonoscopy in an In Vivo Porcine Model with Colorectal Polyps. Cancers 2023, 15, 3122. https://doi.org/10.3390/cancers15123122
Garrido A, Guardiola M, Neira LM, Sont R, Córdova H, Cuatrecasas M, Flisikowski K, Troya J, Sanahuja J, Winogrodzki T, et al. Preclinical Evaluation of a Microwave-Based Accessory Device for Colonoscopy in an In Vivo Porcine Model with Colorectal Polyps. Cancers. 2023; 15(12):3122. https://doi.org/10.3390/cancers15123122
Chicago/Turabian StyleGarrido, Alejandra, Marta Guardiola, Luz María Neira, Roberto Sont, Henry Córdova, Miriam Cuatrecasas, Krzysztof Flisikowski, Joel Troya, Josep Sanahuja, Thomas Winogrodzki, and et al. 2023. "Preclinical Evaluation of a Microwave-Based Accessory Device for Colonoscopy in an In Vivo Porcine Model with Colorectal Polyps" Cancers 15, no. 12: 3122. https://doi.org/10.3390/cancers15123122
APA StyleGarrido, A., Guardiola, M., Neira, L. M., Sont, R., Córdova, H., Cuatrecasas, M., Flisikowski, K., Troya, J., Sanahuja, J., Winogrodzki, T., Belda, I., Meining, A., & Fernández-Esparrach, G. (2023). Preclinical Evaluation of a Microwave-Based Accessory Device for Colonoscopy in an In Vivo Porcine Model with Colorectal Polyps. Cancers, 15(12), 3122. https://doi.org/10.3390/cancers15123122