

End-of-Life Care in the Last Three Months before Death in Older Patients with Cancer in Belgium: A Large Retrospective Cohort Study Using Data Linkage

 , ,
, ,  , , , add
Show full author list
, , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Sources
2.3. Study Participants
2.4. Geriatric Screening and Geriatric Assessment
2.5. Outcomes
2.6. Statistical Analysis
3. Results
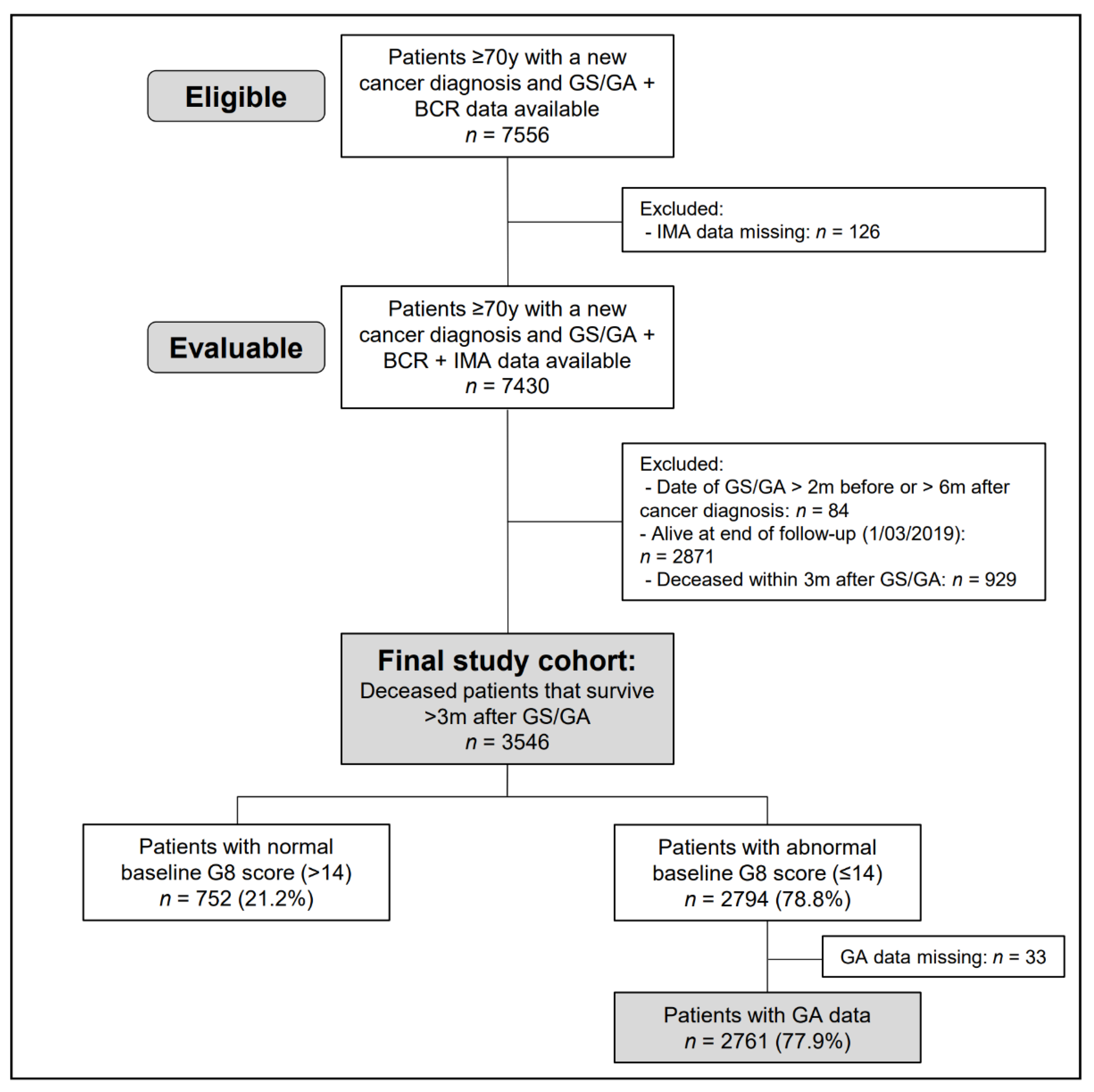
3.1. Patient Population and Baseline Characteristics
3.2. Geriatric Screening and Geriatric Assessment
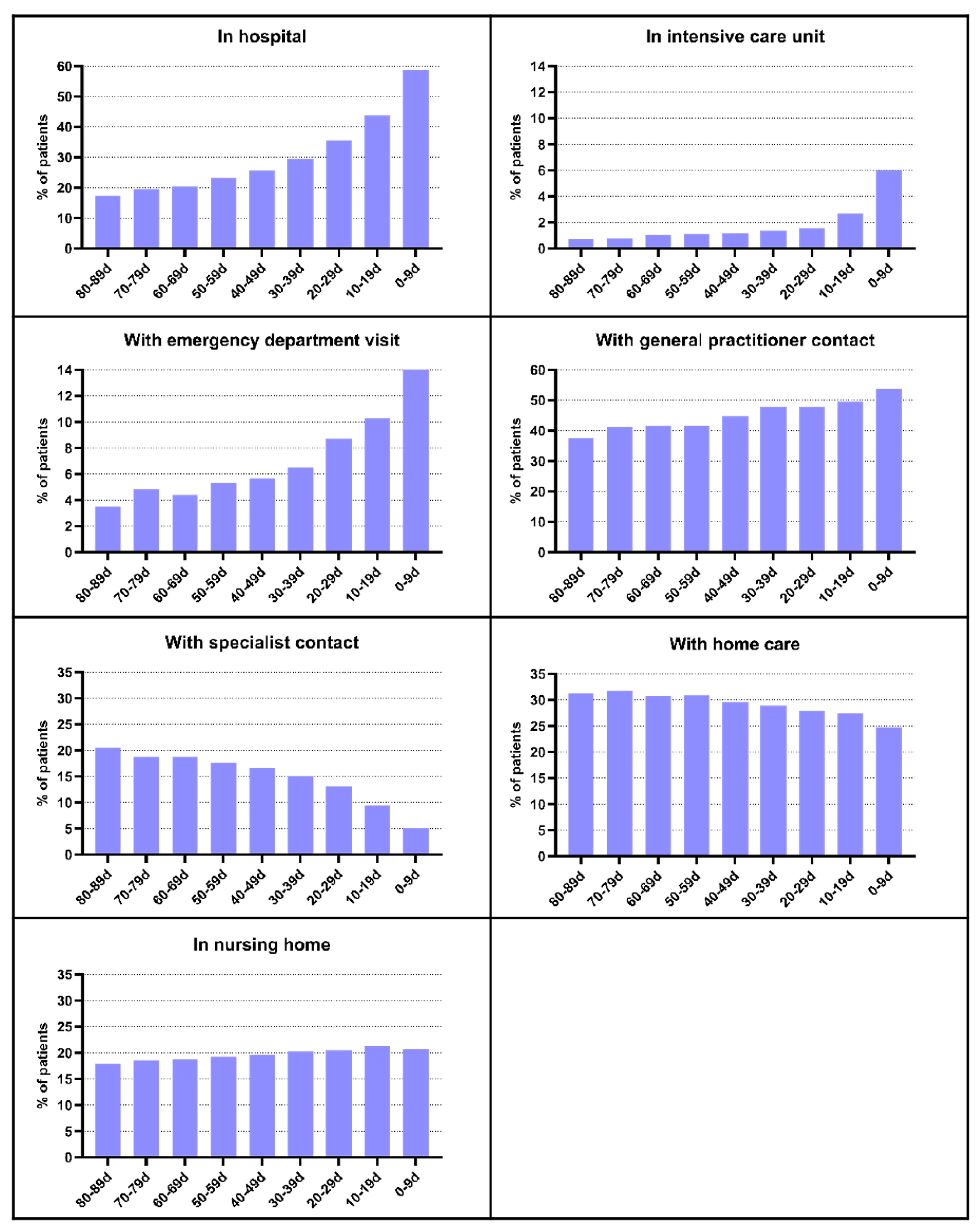
3.3. Healthcare Services Use and Medication Use in EOL
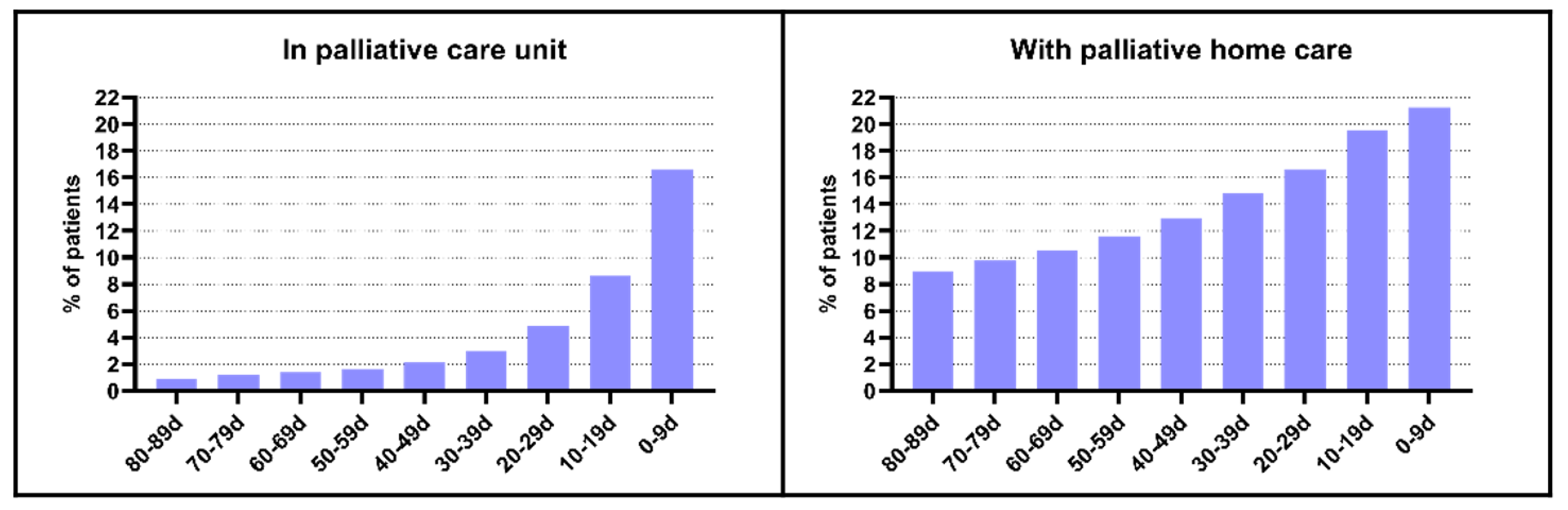
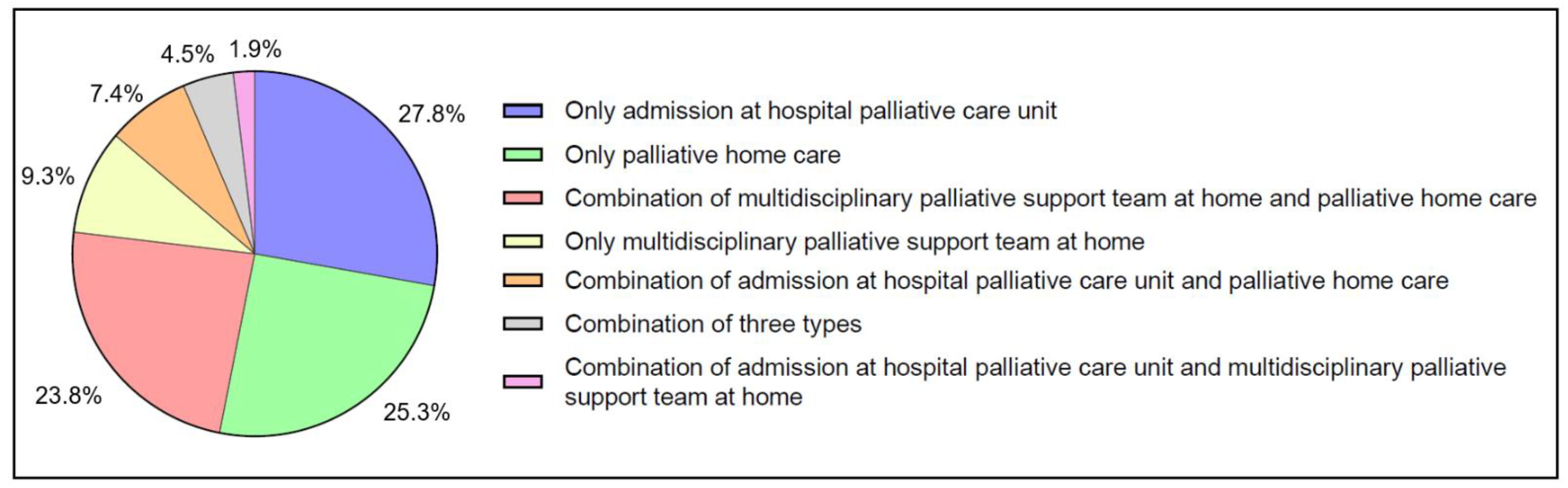
3.4. Specialized Palliative Care in EOL and Associated Factors
3.5. Circumstances of Death
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, D.H. Approach to end of life care. Ochsner J. 2002, 4, 98–103. [Google Scholar] [PubMed]
- Yabroff, K.R.; Lamont, E.B.; Mariotto, A.; Warren, J.L.; Topor, M.; Meekins, A.; Brown, M.L. Cost of care for elderly cancer patients in the United States. J. Natl. Cancer Inst. 2008, 100, 630–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, J.; Mohanti, B.K. Transition from curative to palliative care in cancer. Indian J. Palliat. Care 2011, 17, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Langton, J.M.; Blanch, B.; Drew, A.K.; Haas, M.; Ingham, J.M.; Pearson, S.A. Retrospective studies of end-of-life resource utilization and costs in cancer care using health administrative data: A systematic review. Palliat. Med. 2014, 28, 1167–1196. [Google Scholar] [CrossRef]
- De Schreye, R.; Smets, T.; Annemans, L.; Deliens, L.; Gielen, B.; De Gendt, C.; Cohen, J. Applying Quality Indicators For Administrative Databases To Evaluate End-Of-Life Care For Cancer Patients In Belgium. Health Aff. 2017, 36, 1234–1243. [Google Scholar] [CrossRef]
- Connor, S.R. Global Atlas of Palliative Care, 2nd ed.; World Health Organization (WHO): London, UK, 2020.
- Huo, B.; Song, Y.; Chang, L.; Tan, B. Effects of early palliative care on patients with incurable cancer: A meta-analysis and systematic review. Eur. J. Cancer Care 2022, 31, e13620. [Google Scholar] [CrossRef]
- Kavalieratos, D.; Corbelli, J.; Zhang, D.; Dionne-Odom, J.N.; Ernecoff, N.C.; Hanmer, J.; Hoydich, Z.P.; Ikejiani, D.Z.; Klein-Fedyshin, M.; Zimmermann, C.; et al. Association Between Palliative Care and Patient and Caregiver Outcomes: A Systematic Review and Meta-analysis. JAMA 2016, 316, 2104–2114. [Google Scholar] [CrossRef] [Green Version]
- Temel, J.S.; Greer, J.A.; Muzikansky, A.; Gallagher, E.R.; Admane, S.; Jackson, V.A.; Dahlin, C.M.; Blinderman, C.D.; Jacobsen, J.; Pirl, W.F.; et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 733–742. [Google Scholar] [CrossRef] [Green Version]
- Hawley, P. Barriers to Access to Palliative Care. Palliat. Care 2017, 10, 1178224216688887. [Google Scholar] [CrossRef]
- Mills, J.; Abel, J.; Kellehear, A.; Patel, M. Access to palliative care: The primacy of public health partnerships and community participation. Lancet Public Health 2021, 6, e791–e792. [Google Scholar] [CrossRef]
- Keirse, E.; Beguin, C.; Desmedt, M.; Deveugele, M.; Menten, J.; Simoens, S.; Wens, J.; Borgermans, L.; Kohn, L.; Spinnewijn, B.C.A.; et al. Organisation of Palliative Care in Belgium–Supplement. Health Services Research (HSR); Belgian Health Care Knowledge Centre (KCE): Brussels, Belgium, 2009. [Google Scholar]
- Pilleron, S.; Sarfati, D.; Janssen-Heijnen, M.; Vignat, J.; Ferlay, J.; Bray, F.; Soerjomataram, I. Global cancer incidence in older adults, 2012 and 2035: A population-based study. Int. J. Cancer 2019, 144, 49–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadambi, S.; Loh, K.P.; Dunne, R.; Magnuson, A.; Maggiore, R.; Zittel, J.; Flannery, M.; Inglis, J.; Gilmore, N.; Mohamed, M.; et al. Older adults with cancer and their caregivers–current landscape and future directions for clinical care. Nat. Rev. Clin. Oncol. 2020, 17, 742–755. [Google Scholar] [CrossRef] [PubMed]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology consensus on geriatric assessment in older patients with cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamaker, M.E.; Te Molder, M.; Thielen, N.; van Munster, B.C.; Schiphorst, A.H.; van Huis, L.H. The effect of a geriatric evaluation on treatment decisions and outcome for older cancer patients–A systematic review. J. Geriatr. Oncol. 2018, 9, 430–440. [Google Scholar] [CrossRef]
- Mohile, S.G.; Epstein, R.M.; Hurria, A.; Heckler, C.E.; Canin, B.; Culakova, E.; Duberstein, P.; Gilmore, N.; Xu, H.; Plumb, S.; et al. Communication With Older Patients With Cancer Using Geriatric Assessment: A Cluster-Randomized Clinical Trial From the National Cancer Institute Community Oncology Research Program. JAMA Oncol. 2020, 6, 196–204. [Google Scholar] [CrossRef] [Green Version]
- Wildes, T.M.; Ruwe, A.P.; Fournier, C.; Gao, F.; Carson, K.R.; Piccirillo, J.F.; Tan, B.; Colditz, G.A. Geriatric assessment is associated with completion of chemotherapy, toxicity, and survival in older adults with cancer. J. Geriatr. Oncol. 2013, 4, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Soo, W.K.; King, M.T.; Pope, A.; Parente, P.; Dārziņš, P.; Davis, I.D. Integrated Geriatric Assessment and Treatment Effectiveness (INTEGERATE) in older people with cancer starting systemic anticancer treatment in Australia: A multicentre, open-label, randomised controlled trial. Lancet Healthy Longev. 2022, 3, e617–e627. [Google Scholar] [CrossRef]
- Luta, X.; Maessen, M.; Egger, M.; Stuck, A.E.; Goodman, D.; Clough-Gorr, K.M. Measuring intensity of end of life care: A systematic review. PLoS ONE 2015, 10, e0123764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekelman, J.E.; Halpern, S.D.; Blankart, C.R.; Bynum, J.P.; Cohen, J.; Fowler, R.; Kaasa, S.; Kwietniewski, L.; Melberg, H.O.; Onwuteaka-Philipsen, B.; et al. Comparison of Site of Death, Health Care Utilization, and Hospital Expenditures for Patients Dying With Cancer in 7 Developed Countries. Jama 2016, 315, 272–283. [Google Scholar] [CrossRef]
- Gielen, B.; Remacle, A.; Mertens, R. Patterns of health care use and expenditure during the last 6 months of life in Belgium: Differences between age categories in cancer and non-cancer patients. Health Policy 2010, 97, 53–61. [Google Scholar] [CrossRef]
- Rostoft, S.; Thomas, M.J.; Slaaen, M.; Møller, B.; Syse, A. The effect of age on specialized palliative care use in the last year of life for patients who die of cancer: A nationwide study from Norway. J. Geriatr. Oncol. 2022, 13, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Kenis, C.; Bron, D.; Libert, Y.; Decoster, L.; Van Puyvelde, K.; Scalliet, P.; Cornette, P.; Pepersack, T.; Luce, S.; Langenaeken, C.; et al. Relevance of a systematic geriatric screening and assessment in older patients with cancer: Results of a prospective multicentric study. Ann. Oncol. 2013, 24, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- Baitar, A.; Kenis, C.; Moor, R.; Decoster, L.; Luce, S.; Bron, D.; Van Rijswijk, R.; Rasschaert, M.; Langenaeken, C.; Jerusalem, G.; et al. Implementation of geriatric assessment-based recommendations in older patients with cancer: A multicentre prospective study. J. Geriatr. Oncol. 2015, 6, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Kenis, C.; Decoster, L.; Flamaing, J.; Debruyne, P.R.; De Groof, I.; Focan, C.; Cornelis, F.; Verschaeve, V.; Bachmann, C.; Bron, D.; et al. Adherence to geriatric assessment-based recommendations in older patients with cancer: A multicenter prospective cohort study in Belgium. Ann. Oncol. 2018, 29, 1987–1994. [Google Scholar] [CrossRef] [PubMed]
- Depoorter, V.; Vanschoenbeek, K.; Decoster, L.; De Schutter, H.; Debruyne, P.R.; De Groof, I.; Bron, D.; Cornélis, F.; Luce, S.; Focan, C.; et al. Linking clinical and population-based data in older patients with cancer in Belgium: Feasibility and clinical outcomes. J. Geriatr. Oncol. 2023, 14, 101428. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- International Statistical Classification of Diseases and Related Health Problems, Tenth Revision; World Health Organization: Geneva, Switzerland, 1992–1994; Volume 1–3.
- Sobin, L.H.; Wittekind, C. International Union Against Cancer (UICC): TNM Classification of Malignant Tumours, 6th ed.; Wiley: New York, NY, USA, 2002. [Google Scholar]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. International Union Against Cancer (UICC): TNM Classification of Malignant Tumours, 7th ed.; Wiley-Blackwell: Oxford, UK, 2009. [Google Scholar]
- Nomensoft: Nomenclature and Pseudonomenclature for Healthcare Services. Available online: https://webappsa.riziv-inami.fgov.be/Nomen/fr/search (accessed on 14 March 2023).
- Anatomical Therapeutic Chemical (ATC) Classification System. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 14 March 2023).
- Miesfeldt, S.; Murray, K.; Lucas, L.; Chang, C.H.; Goodman, D.; Morden, N.E. Association of age, gender, and race with intensity of end-of-life care for Medicare beneficiaries with cancer. J. Palliat. Med. 2012, 15, 548–554. [Google Scholar] [CrossRef]
- Sharma, N.; Sharma, A.M.; Wojtowycz, M.A.; Wang, D.; Gajra, A. Utilization of palliative care and acute care services in older adults with advanced cancer. J. Geriatr. Oncol. 2016, 7, 39–46. [Google Scholar] [CrossRef]
- Reeve, R.; Srasuebkul, P.; Langton, J.M.; Haas, M.; Viney, R.; Pearson, S.A. Health care use and costs at the end of life: A comparison of elderly Australian decedents with and without a cancer history. BMC Palliat. Care 2017, 17, 1. [Google Scholar] [CrossRef]
- Bremner, K.E.; Yabroff, K.R.; Coughlan, D.; Liu, N.; Zeruto, C.; Warren, J.L.; de Oliveira, C.; Mariotto, A.B.; Lam, C.; Barrett, M.J.; et al. Patterns of Care and Costs for Older Patients With Colorectal Cancer at the End of Life: Descriptive Study of the United States and Canada. JCO Oncol. Pract. 2020, 16, e1–e18. [Google Scholar] [CrossRef]
- Gao, W.; Gulliford, M.; Morgan, M.; Higginson, I.J. Primary care service use by end-of-life cancer patients: A nationwide population-based cohort study in the United Kingdom. BMC Fam. Pract. 2020, 21, 76. [Google Scholar] [CrossRef] [PubMed]
- Koroukian, S.M.; Douglas, S.L.; Vu, L.; Fein, H.L.; Gairola, R.; Warner, D.F.; Schiltz, N.K.; Cullen, J.; Owusu, C.; Sajatovic, M.; et al. Incidence of Aggressive End-of-Life Care Among Older Adults With Metastatic Cancer Living in Nursing Homes and Community Settings. JAMA Netw. Open 2023, 6, e230394. [Google Scholar] [CrossRef] [PubMed]
- Teno, J.M.; Gozalo, P.L.; Bynum, J.P.; Leland, N.E.; Miller, S.C.; Morden, N.E.; Scupp, T.; Goodman, D.C.; Mor, V. Change in end-of-life care for Medicare beneficiaries: Site of death, place of care, and health care transitions in 2000, 2005, and 2009. JAMA 2013, 309, 470–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luta, X.; Diernberger, K.; Bowden, J.; Droney, J.; Hall, P.; Marti, J. Intensity of care in cancer patients in the last year of life: A retrospective data linkage study. Br. J. Cancer 2022, 127, 712–719. [Google Scholar] [CrossRef]
- Weng, X.; Shen, C.; Van Scoy, L.J.; Boltz, M.; Joshi, M.; Wang, L. A comparison of end-of-life care patterns between older patients with both cancer and Alzheimer’s disease and related dementias versus those with only cancer. J. Geriatr. Oncol. 2022, 13, 1111–1121. [Google Scholar] [CrossRef]
- Langton, J.M.; Reeve, R.; Srasuebkul, P.; Haas, M.; Viney, R.; Currow, D.; Pearson, S.A. Health service use and costs in the last 6 months of life in elderly decedents with a history of cancer: A comprehensive analysis from a health payer perspective. Br. J. Cancer 2016, 114, 1293–1302. [Google Scholar] [CrossRef] [Green Version]
- Craigs, C.L.; West, R.M.; Hurlow, A.; Bennett, M.I.; Ziegler, L.E. Access to hospital and community palliative care for patients with advanced cancer: A longitudinal population analysis. PLoS ONE 2018, 13, e0200071. [Google Scholar] [CrossRef] [Green Version]
- Parajuli, J.; Tark, A.; Jao, Y.L.; Hupcey, J. Barriers to palliative and hospice care utilization in older adults with cancer: A systematic review. J. Geriatr. Oncol. 2020, 11, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Van den Block, L.; Deschepper, R.; Bossuyt, N.; Drieskens, K.; Bauwens, S.; Van Casteren, V.; Deliens, L. Care for patients in the last months of life: The Belgian Sentinel Network Monitoring End-of-Life Care study. Arch. Intern. Med. 2008, 168, 1747–1754. [Google Scholar] [CrossRef]
- Jordan, R.I.; Allsop, M.J.; ElMokhallalati, Y.; Jackson, C.E.; Edwards, H.L.; Chapman, E.J.; Deliens, L.; Bennett, M.I. Duration of palliative care before death in international routine practice: A systematic review and meta-analysis. BMC Med. 2020, 18, 368. [Google Scholar] [CrossRef] [PubMed]
- Penders, Y.W.H.; Gilissen, J.; Moreels, S.; Deliens, L.; Van den Block, L. Palliative care service use by older people: Time trends from a mortality follow-back study between 2005 and 2014. Palliat. Med. 2018, 32, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Mathews, J.; Hannon, B.; Zimmermann, C. Models of Integration of Specialized Palliative Care with Oncology. Curr. Treat. Options Oncol. 2021, 22, 44. [Google Scholar] [CrossRef]
- Ahmed, N.; Bestall, J.C.; Ahmedzai, S.H.; Payne, S.A.; Clark, D.; Noble, B. Systematic review of the problems and issues of accessing specialist palliative care by patients, carers and health and social care professionals. Palliat. Med. 2004, 18, 525–542. [Google Scholar] [CrossRef]
- van der Vlies, E.; Kurk, S.A.; Roodhart, J.M.L.; Gerritse, F.L.; Pelgrim, T.C.; Vos, J.M.; Sohne, M.; Hunting, C.B.; Noordzij, P.G.; van der Velden, A.M.T.; et al. The relevance of geriatric assessment for older patients receiving palliative chemotherapy. J. Geriatr. Oncol. 2020, 11, 482–487. [Google Scholar] [CrossRef]
- Hirooka, K.; Nakanishi, M.; Fukahori, H.; Nishida, A. Impact of dementia on quality of death among cancer patients: An observational study of home palliative care users. Geriatr. Gerontol. Int. 2020, 20, 354–359. [Google Scholar] [CrossRef]
- Huang, H.K.; Hsieh, J.G.; Hsieh, C.J.; Wang, Y.W. Do cancer patients with dementia receive less aggressive treatment in end-of-life care? A nationwide population-based cohort study. Oncotarget 2017, 8, 63596–63604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lage, D.E.; El-Jawahri, A.; Fuh, C.X.; Newcomb, R.A.; Jackson, V.A.; Ryan, D.P.; Greer, J.A.; Temel, J.S.; Nipp, R.D. Functional Impairment, Symptom Burden, and Clinical Outcomes Among Hospitalized Patients With Advanced Cancer. J. Natl. Compr. Cancer Netw. 2020, 18, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Hamaker, M.E.; van den Bos, F.; Rostoft, S. Frailty and palliative care. BMJ Support Palliat. Care 2020, 10, 262–264. [Google Scholar] [CrossRef]
- Sedhom, R.; Kuo, P.L.; Gupta, A.; Smith, T.J.; Chino, F.; Carducci, M.A.; Bandeen-Roche, K. Changes in the place of death for older adults with cancer: Reason to celebrate or a risk for unintended disparities? J. Geriatr. Oncol. 2021, 12, 361–367. [Google Scholar] [CrossRef]
- Fereidouni, A.; Rassouli, M.; Salesi, M.; Ashrafizadeh, H.; Vahedian-Azimi, A.; Barasteh, S. Preferred Place of Death in Adult Cancer Patients: A Systematic Review and Meta-Analysis. Front. Psychol. 2021, 12, 704590. [Google Scholar] [CrossRef]
- Abian, M.H.; Antón Rodríguez, C.; Noguera, A. End of Life Cost Savings in the Palliative Care Unit Compared to Other Services. J. Pain Symptom Manag. 2022, 64, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.D.; Stukel, T.A.; Fu, L.; Scales, D.C.; Laupacis, A.; Rubenfeld, G.D.; Wunsch, H.; Downar, J.; Rockwood, K.; Heyland, D.K.; et al. Trends in site of death and health care utilization at the end of life: A population-based cohort study. CMAJ Open 2019, 7, E306–E315. [Google Scholar] [CrossRef] [Green Version]
- Schaffar, R.; Rapiti, E.; Rachet, B.; Woods, L. Accuracy of cause of death data routinely recorded in a population-based cancer registry: Impact on cause-specific survival and validation using the Geneva Cancer Registry. BMC Cancer 2013, 13, 609. [Google Scholar] [CrossRef] [Green Version]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged. The Index of Adl: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Lamb, S.E.; Jã¸rstad-Stein, E.C.; Hauer, K.; Becker, C.; on behalf of the Prevention of Falls Network Europe and Outcomes Consensus Group. Development of a Common Outcome Data Set for Fall Injury Prevention Trials: The Prevention of Falls Network Europe Consensus. J. Am. Geriatr. Soc. 2005, 53, 1618–1622. [Google Scholar] [CrossRef] [PubMed]
- Collins, S.; Moore, A.R.; McQuay, H.J. The visual analogue pain intensity scale: What is moderate pain in millimetres? Pain 1997, 72, 95–97. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for Undernutrition in Geriatric Practice: Developing the Short-Form Mini-Nutritional Assessment (MNA-SF). J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Full Cohort (Normal and Abnormal G8 Score) | Cohort with GA Data (Only Abnormal G8 Score) | ||
|---|---|---|---|
| N (%) | N (%) | ||
| Total | 3546 (100.0) | 2761 (100.0) | |
| Age | 70–74 y | 883 (24.9) | 598 (21.7) |
| 75–79 y | 1039 (29.3) | 737 (26.7) | |
| 80–84 y | 939 (26.5) | 783 (28.4) | |
| ≥85 y | 685 (19.3) | 643 (23.3) | |
| Median (IQR) | 79 (75–83) | 80 (75–84) | |
| Sex | Female | 1902 (53.6) | 1494 (54.1) |
| Male | 1644 (46.4) | 1267 (45.9) | |
| Cancer site | Breast | 655 (18.5) | 466 (16.9) |
| Colon | 536 (15.1) | 440 (15.9) | |
| Lung | 514 (14.5) | 394 (14.3) | |
| Rectum | 215 (6.0) | 167 (6.0) | |
| Pancreas | 152 (4.3) | 134 (4.9) | |
| Other a | 1474 (41.6) | 1160 (42.0) | |
| Cancer stage b | I | 399 (11.2) | 290 (10.5) |
| II | 702 (19.8) | 544 (19.7) | |
| III | 742 (20.9) | 563 (20.4) | |
| IV | 956 (27.0) | 765 (27.7) | |
| NA c | 456 (12.9) | 361 (13.1) | |
| Unknown | 291 (8.2) | 238 (8.6) | |
| G8 | Normal | 752 (21.2) | 0 (0.0) |
| Abnormal | 2794 (78.8) | 2761 (100.0) | |
| CCI | No comorbidity: score 0 | 1015 (28.6) | 728 (26.4) |
| Mild comorbidity: score 1–2 | 1446 (40.8) | 1143 (41.4) | |
| Moderate comorbidity: score 3–4 | 722 (20.4) | 588 (21.3) | |
| Severe comorbidity: score ≥ 5 | 341 (9.6) | 285 (10.3) | |
| Missing | 22 (0.6) | 17 (0.6) | |
| Polypharmacy | 0–4 medications | 1520 (42.9) | 1042 (37.7) |
| ≥5 medications | 1962 (55.3) | 1675 (60.7) | |
| Missing | 64 (1.8) | 44 (1.6) | |
| ECOG-PS | Score 0–1 | 2229 (62.9) | 1514 (54.8) |
| Score ≥ 2 | 1307 (36.8) | 1246 (45.1) | |
| Missing | 10 (0.3) | 1 (0.0) | |
| Attained educational level | Higher education | 587 (16.5) | 456 (16.5) |
| Upper secondary education | 958 (27.0) | 749 (27.1) | |
| Lower secondary education | 1388 (39.1) | 1108 (40.1) | |
| Primary education | 393 (11.1) | 346 (12.5) | |
| Illiterate | 27 (0.8) | 26 (1.0) | |
| Other | 34 (1.0) | 30 (1.1) | |
| Missing | 159 (4.5) | 46 (1.7) | |
| Marital status | Partnered (married or legally co-habiting) | 1810 (51.0) | 1392 (50.4) |
| Not partnered (single, widow/er, divorced) | 1611 (45.4) | 1351 (48.9) | |
| Other | 20 (0.6) | 16 (0.6) | |
| Missing | 105 (3.0) | 2 (0.1) | |
| Cohort identification d | Study 1 | 593 (16.7) | 471 (17.1) |
| Study 2 | 444 (12.5) | 328 (11.9) | |
| Study 3 | 2509 (70.8) | 1962 (71.1) | |
| Time between GS/GA and death in years | 3 months–1 year e | 1211 (34.1) | 1030 (37.3) |
| 1–2 years | 878 (24.8) | 698 (25.3) | |
| 2–3 years | 533 (15.0) | 396 (14.3) | |
| 3–4 years | 364 (10.3) | 249 (9.0) | |
| 4–5 years | 284 (8.0) | 195 (7.1) | |
| >5 years | 276 (7.8) | 193 (7.0) | |
| Median (IQR) | 1.6 (0.7–3.1) | 1.4 (0.7–2.9) |
| N (%) | Median Number in Last 3 m (In Case of Use) (IQR) | |
|---|---|---|
| Hospital admission | 2705 (76.3) | 20 days (9–36) |
| ICU admission | 371 (10.5) | 4 days (2–8) |
| ED visits | 1743 (49.1) | 1 visit (1–2) |
| GP contacts a | 3148 (89.9) | 6 contacts (3–10) |
| Specialist contacts | 2147 (60.5) | 2 contacts (1–3) |
| Home care use | 1895 (53.4) | 26 days (8–58) |
| Nursing home stay | 856 (24.1) | 83 days (53–90) |
| Medication Use | N (%) |
|---|---|
| Systemic anti-neoplastic therapy | 1038 (29.2) |
| Endocrine therapy | 422 (11.9) |
| Systemic corticosteroids | 1985 (56.0) |
| Opioids | 2757 (77.7) |
| Midazolam | 1066 (30.1) |
| N (%) | Median Number of Days in Last 3 m (In Case of Use) (IQR) | Median Start in Days before Death (IQR) | |
|---|---|---|---|
| Specialized palliative care a | 1544 (43.5) | - | 30 (11–74) |
| Palliative care unit admission | 604 (17.0) | 11 (5–24) | 11 (5–25) |
| Palliative home care | 979 (27.6) | 28 (11–64) | 42 (15–88) |
| Multidisciplinary palliative support team at home | 610 (17.2) | - | 22 (8–43) |
| No specialized palliative care | 1992 (56.5) | - | - |
| OR (95% CI) | p-Value | Type III p-Value | ||
|---|---|---|---|---|
| Age category | 70–74 y | 1 | <0.001 | |
| 75–79 y | 0.90 (0.75–1.08) | 0.25 | ||
| 80–84 y | 0.71 (0.59–0.85) | <0.001 | ||
| ≥85 y | 0.44 (0.36–0.54) | <0.001 | ||
| Sex | Female | 1 | 0.08 | |
| Male | 1.13 (0.99–1.29) | 0.08 | ||
| Cancer site | Breast | 1 | <0.001 | |
| Colon | 1.37 (1.08–1.74) | 0.009 | ||
| Lung | 2.36 (1.86–2.99) | <0.001 | ||
| Rectum | 1.10 (0.80–1.53) | 0.55 | ||
| Pancreas | 4.12 (2.83–5.99) | <0.001 | ||
| Other a | 1.31 (0.96–1.79) | 0.09 | ||
| Cancer stage b | I | 1 | <0.001 | |
| II | 1.21 (0.93–1.58) | 0.16 | ||
| III | 1.92 (1.48–2.49) | <0.001 | ||
| IV | 3.46 (2.69–4.45) | <0.001 | ||
| NA c | 1.74 (1.31–2.31) | <0.001 | ||
| Missing | 2.22 (1.62–3.05) | <0.001 | ||
| Charlson comorbidity index | No comorbidity: score 0 | 1 | 0.0013 | |
| Mild comorbidity: score 1–2 | 0.91 (0.78–1.07) | 0.25 | ||
| Moderate comorbidity: score 3–4 | 0.78 (0.64–0.95) | 0.01 | ||
| Severe comorbidity: score ≥ 5 | 0.62 (0.48–0.78) | <0.001 | ||
| Missing | 1.36 (0.58–3.19) | 0.47 | ||
| Polypharmacy | 0–4 medications | 1 | <0.001 | |
| ≥5 medications | 0.72 (0.63–0.82) | <0.001 | ||
| Missing | 0.79 (0.47–1.30) | 0.35 | ||
| ECOG-PS | Score 0–1 | 1 | <0.001 | |
| Score ≥ 2 | 0.69 (0.60–0.79) | <0.001 | ||
| Missing | 0.75 (0.21–2.68) | 0.66 | ||
| Attained educational level | Higher education | 1 | 0.40 | |
| Upper secondary education | 0.90 (0.73–1.10) | 0.31 | ||
| Lower secondary education | 0.98 (0.81–1.19) | 0.82 | ||
| Primary education | 0.88 (0.68–1.14) | 0.33 | ||
| Illiterate | 1.31 (0.61–2.83) | 0.49 | ||
| Other | 1.1 (0.54–2.16) | 0.83 | ||
| Missing | 0.70 (0.49–1.00) | 0.05 | ||
| Marital status | Partnered | 1 | <0.001 | |
| Not partnered | 0.61 (0.53–0.70) | <0.001 | ||
| Other | 0.18 (0.05–0.61) | 0.006 | ||
| Missing | 0.60 (0.40–0.90) | 0.01 | ||
| Cohort identification d | Study 1 | 1 | 0.1521 | |
| Study 2 | 1.17 | 0.23 | ||
| Study 3 | 1.20 | 0.05 | ||
| The time between G8 and death in days e | 90–267 f | 1 | <0.001 | |
| 268–568 | 1.21 (1.01–1.46) | 0.04 | ||
| 569–1135 | 0.93 (0.77–1.12) | 0.44 | ||
| >1135 | 0.61 (0.51–0.74) | <0.001 |
| Unadjusted Analysis | Adjusted Analysis a | ||||
|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | ||
| Geriatric screening at cancer diagnosis (n = 3546) | |||||
| G8 | Normal vs. abnormal | 0.93 (0.79–1.09) | 0.3803 | 0.94 (0.78–1.14) | 0.5412 |
| Geriatric assessment at cancer diagnosis (n = 2761) | |||||
| Functional status: ADL | Dependent vs. independent | 0.66 (0.57–0.77) | <0.0001 | 0.82 (0.69–0.96) | 0.0172 |
| Functional status: IADL b | Dependent vs. independent | 0.64 (0.55–0.75) | <0.0001 | 0.76 (0.64–0.91) | 0.0028 |
| Falls history b | Falls vs. no falls | 0.77 (0.66–0.90) | 0.0011 | 0.88 (0.74–1.04) | 0.1319 |
| Pain: VAS b | Pain vs. no pain | 1.21 (1.04–1.40) | 0.0156 | 1.15 (0.98–1.36) | 0.0933 |
| Cognition: MMSE b | Mild/severe cognitive impairment vs. normal | 0.64 (0.53–0.78) | <0.0001 | 0.73 (0.59–0.91) | 0.0046 |
| Depression: GDS-4 b | At risk for depression vs. not at risk | 0.96 (0.82–1.12) | 0.6127 | 0.89 (0.76–1.06) | 0.1963 |
| Nutrition: MNA-SF b | At risk for malnutrition/malnourished vs. normal | 1.39 (1.14–1.70) | 0.0013 | 1.04 (0.84–1.30) | 0.7062 |
| Place of Death | N (%) |
|---|---|
| Hospital: palliative care unit | 583 (16.4) |
| Hospital: geriatric department | 279 (7.9) |
| Hospital: other department | 1087 (30.7) |
| Nursing home | 620 (17.5) |
| Home | 977 (27.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Depoorter, V.; Vanschoenbeek, K.; Decoster, L.; Silversmit, G.; Debruyne, P.R.; De Groof, I.; Bron, D.; Cornélis, F.; Luce, S.; Focan, C.; et al. End-of-Life Care in the Last Three Months before Death in Older Patients with Cancer in Belgium: A Large Retrospective Cohort Study Using Data Linkage. Cancers 2023, 15, 3349. https://doi.org/10.3390/cancers15133349
Depoorter V, Vanschoenbeek K, Decoster L, Silversmit G, Debruyne PR, De Groof I, Bron D, Cornélis F, Luce S, Focan C, et al. End-of-Life Care in the Last Three Months before Death in Older Patients with Cancer in Belgium: A Large Retrospective Cohort Study Using Data Linkage. Cancers. 2023; 15(13):3349. https://doi.org/10.3390/cancers15133349
Chicago/Turabian StyleDepoorter, Victoria, Katrijn Vanschoenbeek, Lore Decoster, Geert Silversmit, Philip R. Debruyne, Inge De Groof, Dominique Bron, Frank Cornélis, Sylvie Luce, Christian Focan, and et al. 2023. "End-of-Life Care in the Last Three Months before Death in Older Patients with Cancer in Belgium: A Large Retrospective Cohort Study Using Data Linkage" Cancers 15, no. 13: 3349. https://doi.org/10.3390/cancers15133349
APA StyleDepoorter, V., Vanschoenbeek, K., Decoster, L., Silversmit, G., Debruyne, P. R., De Groof, I., Bron, D., Cornélis, F., Luce, S., Focan, C., Verschaeve, V., Debugne, G., Langenaeken, C., Van Den Bulck, H., Goeminne, J. -C., Teurfs, W., Jerusalem, G., Schrijvers, D., Petit, B., ... Wildiers, H. (2023). End-of-Life Care in the Last Three Months before Death in Older Patients with Cancer in Belgium: A Large Retrospective Cohort Study Using Data Linkage. Cancers, 15(13), 3349. https://doi.org/10.3390/cancers15133349