
Benefit of Neoadjuvant Laparoscopic Hyperthermic Intraperitoneal Chemotherapy and Bidirectional Chemotherapy for Patients with Gastric Cancer with Peritoneal Carcinomatosis Considering Cytoreductive Surgery

 ,
,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
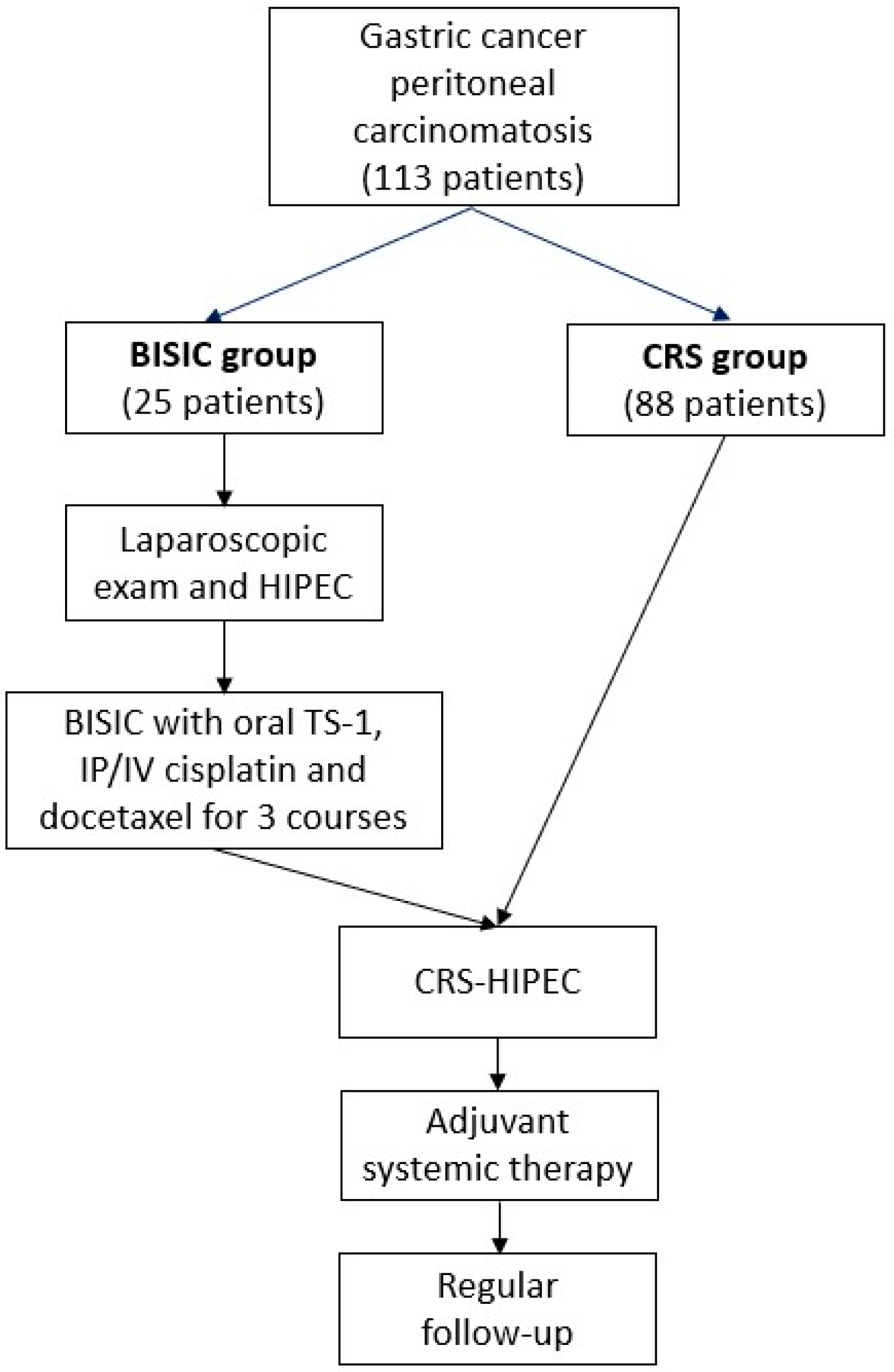
2.1. Patients
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Perioperative Outcomes of Cytoreductive Surgery
3.3. Survival Outcomes and Multivariable Analysis of Predictive Factors
3.4. Selection Criteria for BISIC Based on PC Grade
3.5. Oncological Effects of BISIC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Roviello, F.; Caruso, S.; Neri, A.; Marrelli, D. Treatment and prevention of peritoneal carcinomatosis from gastric cancer by cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: Overview and rationale. Eur. J. Surg. Oncol. 2013, 39, 1309–1316. [Google Scholar] [CrossRef]
- Maehara, Y.; Hasuda, S.; Koga, T.; Tokunaga, E.; Kakeji, Y.; Sugimachi, K. Postoperative outcome and sites of recurrence in patients following curative resection of gastric cancer. Br. J. Surg. 2000, 87, 353–357. [Google Scholar] [CrossRef]
- Kitayama, J.; Ishigami, H.; Yamaguchi, H.; Sakuma, Y.; Horie, H.; Hosoya, Y.; Lefor, A.K.; Sata, N. Treatment of patients with peritoneal metastases from gastric cancer. Ann. Gastroenterol. Surg. 2018, 2, 116–123. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. New standard of care for appendiceal epithelial neoplasms and pseudomyxoma peritonei syndrome? Lancet Oncol. 2006, 7, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Yan, T.D.; Deraco, M.; Baratti, D.; Kusamura, S.; Elias, D.; Glehen, O.; Gilly, F.N.; Levine, E.A.; Shen, P.; Mohamed, F.; et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: Multi-institutional experience. J. Clin. Oncol. 2009, 27, 6237–6242. [Google Scholar] [CrossRef]
- van Driel, W.J.; Koole, S.N.; Sikorska, K.; Schagen van Leeuwen, J.H.; Schreuder, H.W.R.; Hermans, R.H.M.; de Hingh, I.; van der Velden, J.; Arts, H.J.; Massuger, L.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N. Engl. J. Med. 2018, 378, 230–240. [Google Scholar] [CrossRef]
- Bonnot, P.E.; Piessen, G.; Kepenekian, V.; Decullier, E.; Pocard, M.; Meunier, B.; Bereder, J.M.; Abboud, K.; Marchal, F.; Quenet, F.; et al. Cytoreductive Surgery with or without Hyperthermic Intraperitoneal Chemotherapy for Gastric Cancer with Peritoneal Metastases (CYTO-CHIP study): A Propensity Score Analysis. J. Clin. Oncol. 2019, 37, 2028–2040. [Google Scholar] [CrossRef]
- Yonemura, Y.; Kawamura, T.; Bandou, E.; Takahashi, S.; Sawa, T.; Matsuki, N. Treatment of peritoneal dissemination from gastric cancer by peritonectomy and chemohyperthermic peritoneal perfusion. Br. J. Surg. 2005, 92, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Glehen, O.; Gilly, F.N.; Arvieux, C.; Cotte, E.; Boutitie, F.; Mansvelt, B.; Bereder, J.M.; Lorimier, G.; Quenet, F.; Elias, D. Peritoneal Carcinomatosis from Gastric Cancer: A Multi-Institutional Study of 159 Patients Treated by Cytoreductive Surgery Combined with Perioperative Intraperitoneal Chemotherapy. Ann. Surg. Oncol. 2010, 17, 2370–2377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, B.; Morris, D.; Canbay, E.; Verwaal, V.; Sugarbaker, P.H.; Elias, D.; Coccolini, F.; Ishibashi, H.; Deraco, M.; Mahtem, H.; et al. A comprehensive treatment for peritoneal metastases from gastric cancer with curative intent. Eur. J. Surg. Oncol. 2016, 42, 1–9. [Google Scholar]
- Yonemura, Y. Comprehensive treatment for the peritoneal metastasis from gastric cancer. World J. Surg. Proced. 2015, 5, 187–197. [Google Scholar] [CrossRef]
- Yonemura, Y. A new bidirectional intraperitoneal and systemic induction chemotherapy (BISIC) for the peritoneal metastasis from gastric cancer in neoadjuvant setting. Integr. Cancer Sci. Ther. 2014, 1, 26–29. [Google Scholar] [CrossRef]
- Canbay, E.; Mizumoto, A.; Ichinose, M.; Ishibashi, H.; Sako, S.; Hirano, M.; Takao, N.; Yonemura, Y. Outcome data of patients with peritoneal carcinomatosis from gastric origin treated by a strategy of bidirectional chemotherapy prior to cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in a single specialized center in Japan. Ann. Surg. Oncol. 2014, 21, 1147–1152. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. Peritonectomy procedures. Ann. Surg. 1995, 221, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat. Res. 1996, 82, 359–374. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.J.; Huang, C.Q.; Suo, T.; Mei, L.J.; Yang, G.L.; Cheng, F.L.; Zhou, Y.F.; Xiong, B.; Yonemura, Y.; Li, Y. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from gastric cancer: Final results of a phase III randomized clinical trial. Ann. Surg. Oncol. 2011, 18, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Rudloff, U.; Langan, R.C.; Mullinax, J.E.; Beane, J.D.; Steinberg, S.M.; Beresnev, T.; Webb, C.C.; Walker, M.; Toomey, M.A.; Schrump, D.; et al. Impact of maximal cytoreductive surgery plus regional heated intraperitoneal chemotherapy (HIPEC) on outcome of patients with peritoneal carcinomatosis of gastric origin: Results of the GYMSSA trial. J. Surg. Oncol. 2014, 110, 275–284. [Google Scholar] [CrossRef]
- Marano, L.; Marrelli, D.; Sammartino, P.; Biacchi, D.; Graziosi, L.; Marino, E.; Coccolini, F.; Fugazzola, P.; Valle, M.; Federici, O.; et al. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Gastric Cancer with Synchronous Peritoneal Metastases: Multicenter Study of ‘Italian Peritoneal Surface Malignancies Oncoteam-S.I.C.O. Ann. Surg. Oncol. 2021, 28, 9060–9070. [Google Scholar] [CrossRef] [PubMed]
- Yonemura, Y.; Bandou, E.; Sawa, T.; Yoshimitsu, Y.; Endou, Y.; Sasaki, T.; Sugarbaker, P.H. Neoadjuvant treatment of gastric cancer with peritoneal dissemination. Eur. J. Surg. Oncol. 2006, 32, 661–665. [Google Scholar] [CrossRef]
- Baron, M.A. Structure of the intestinal peritoneum in man. Am. J. Anat. 1941, 69, 439–497. [Google Scholar] [CrossRef]
- Fushida, S.; Furui, N.; Kinami, S.; Ninomiya, I.; Fujimura, T.; Nishimura, G.; Ohta, T.; Yokogawa, K.; Miyamoto, K.; Miwa, K. Pharmacologic study of intraperitoneal paclitaxel in gastric cancer patients with peritoneal dissemination. Jpn. J. Cancer Chemother. 2002, 29, 2164–2167. [Google Scholar]
- de Bree, E.; Tsiftsis, D.D. Experimental and pharmacokinetic studies in intraperitoneal chemotherapy: From laboratory bench to bedside. Recent Results Cancer Res. 2007, 169, 53–73. [Google Scholar] [PubMed]
- Yonemura, Y.; Endou, Y.; Shinbo, M.; Sasaki, T.; Hirano, M.; Mizumoto, A.; Matsuda, T.; Takao, N.; Ichinose, M.; Mizuno, M.; et al. Safety and efficacy of bidirectional chemotherapy for treatment of patients with peritoneal dissemination from gastric cancer: Selection for cytoreductive surgery. J. Surg. Oncol. 2009, 100, 311–316. [Google Scholar] [CrossRef]
- Brandl, A.; Yonemura, Y.; Glehen, O.; Sugarbaker, P.; Rau, B. Long term survival in patients with peritoneal metastasised gastric cancer treated with cytoreductive surgery and HIPEC: A multi-institutional cohort from PSOGI. Eur. J. Surg. Oncol. 2020, 47, 172–180. [Google Scholar] [CrossRef]
- Yonemura, Y.; Prabhu, A.; Sako, S.; Ishibashi, H.; Mizumoto, A.; Takao, N.; Ichinose, M.; Motoi, S.; Liu, Y.; Nishihara, K.; et al. Long Term Survival after Cytoreductive Surgery Combined with Perioperative Chemotherapy in Gastric Cancer Patients with Peritoneal Metastasis. Cancers 2020, 12, 116. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients | BISIC Group | CRS Group | p-Value |
|---|---|---|---|---|
| (n = 113) | (n = 25) | (n = 88) | ||
| Age (years ± SE) | 53.1 ± 1.1 | 50.8 ± 2.3 | 53.8 ± 1.2 | 0.232 |
| (range) | (29–79) | |||
| Gender | 0.06 | |||
| Male | 42 (37%) | 5 (20%) | 37 (42%) | |
| Female | 71 (63%) | 20 (80%) | 51 (58%) | |
| BMI | 21.0 ± 0.4 | 21.0 ± 0.7 | 21.1 ± 0.4 | 0.902 |
| Preoperative TPN | 70 (62%) | 13 (52%) | 57 (65%) | 0.254 |
| ASA score | 0.778 | |||
| 2 | 91 (81%) | 21 (84%) | 70 (80%) | |
| 3 | 22 (19%) | 4 (16%) | 18 (20%) | |
| Ejection fraction of heart (%) | 61.28 ± 2.4 | 56.8 ± 5.7 | 63.3 ± 2.4 | 0.296 |
| Laboratory data | ||||
| CEA (ng/mL) | 12.1 ± 4.1 | 8.3 ± 3.6 | 13.3 ± 5.2 | 0.607 |
| CA 19-9 (U/mL) | 555.8 ± 213.3 | 1097.0 ± 706.7 | 375.4 ± 159.4 | 0.329 |
| CA-125 (U/mL) | 83.8 ± 14.2 | 74.3 ± 21.5 | 87.3 ± 17.9 | 0.686 |
| AFP | 7.2 ± 1.8 | 5.8 ±1.2 | 7.8 ± 2.5 | 0.611 |
| CRP (mg/dL) | 1.6 ± 0.4 | 1.6 ± 0.6 | 1.6 ± 3.6 | 0.953 |
| Hb | 11.0 ± 0.2 | 10.4 ± 0.3 | 11.2 ± 0.2 | 0.08 |
| PLT (103/μL) | 259.6 ± 11.1 | 196.0 ± 19.0 | 279.4 ± 12.6 | 0.001 |
| ALB | 3.6 ± 0.1 | 3.5 ± 0.1 | 3.6 ± 0.1 | 0.158 |
| Variables | All Patients | BISIC Group | CRS Group | p-Value |
|---|---|---|---|---|
| (n = 113) | (n = 25) | (n = 88) | ||
| Pre-CRS PCI | ||||
| Total | 20 | 16 | 21 | 0.017 |
| Region 0–8 | 15 | 12 | 15 | 0.057 |
| Region 9–12 | 5 | 3 | 6 | 0.009 |
| Post-CRS PCI | ||||
| Total | 13 | 6 | 14 | 0.002 |
| Region 0–8 | 8 | 3 | 9 | 0.001 |
| Region 9–12 | 4 | 3 | 5 | 0.025 |
| CC score | 0.329 | |||
| 0 | 34 (30.4%) | 9 (36.0%) | 25 (28.4%) | |
| 1 | 20 (17.9%) | 6 (24.0%) | 14 (15.9%) | |
| 2 | 18 (16.1%) | 5 (20%) | 14 (15.9%) | |
| 3 | 40 (35.6%) | 5 (20%) | 35 (39.8%) | |
| Morbidity | 37 (32.7%) | 7 (28%) | 30 (34%) | 0.636 |
| Clavien–Dindo class | 0.68 | |||
| 0–2 | 76 (67.3%) | 17 (68.0%) | 59 (67.0%) | |
| 3–4 | 28 (24.7%) | 7 (28.0%) | 21 (23.9%) | |
| 5 | 9 (8.0%) | 1 (4.0%) | 8 (9.1%) | |
| Peritonectomy | 52 (46.0%) | 13 (52.0%) | 39 (44.3%) | 0.506 |
| Operation time (minutes) | 506 | 633 ± 47 | 466 ± 23 | 0.001 |
| Transfusion | ||||
| PRBC (unit) | 4 | 8 | 3 | 0.001 |
| FFP (unit) | 3 | 6 | 2 | |
| Blood loss (mL) | 558 (0–7000) | 1131 | 377 | 0.019 |
| Length of stay (days) | 20 ± 22 | 19 ± 3 | 20 ± 4 | 0.848 |
| Variables | All Patients | BISIC Group | CRS Group | p-Value |
|---|---|---|---|---|
| (n = 113) | (n = 25) | (n = 88) | ||
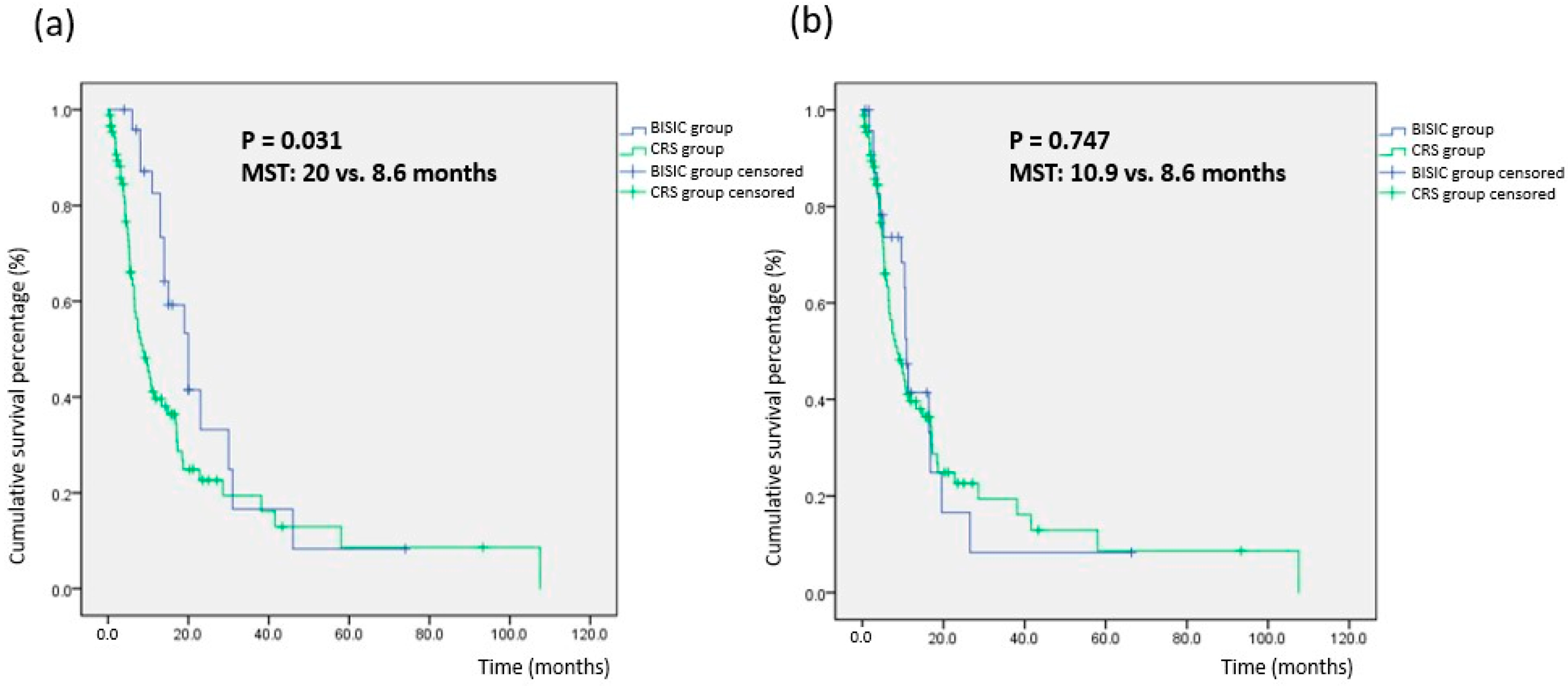
| Median survival time after enrollment (months) | 20 | 8.6 | 0.031 | |
| Median survival time after CRS (months) | 10.9 | 8.6 | 0.747 | |
| Overall survival rate (%) after first HIPEC | 0.031 | |||
| 1-year | 52% | 83% | 43% | |
| 2-year | 27% | 35% | 25% | |
| 3-year | 20% | 17% | 22% | |
| 4-year | 12% | 9% | 14% | |
| 5-year | 9% | 9% | 9% |
| Risk Factor | Hazard Ratio (95% CI) | p-Value |
|---|---|---|
| Group (BISIC vs. CRS) | 0.541 (0.293–0.998) | 0.049 |
| Gender (male vs. female) | 1.028 (0.607–1.739) | 0.919 |
| Age | 1.027 (1.006–1.049) | 0.013 |
| Initial PCI 9–12 | 0.939 (0.827–1.065) | 0.939 |
| Post-CRS remnant PCI 9–12 | 1.218 (1.078–1.376) | 0.002 |
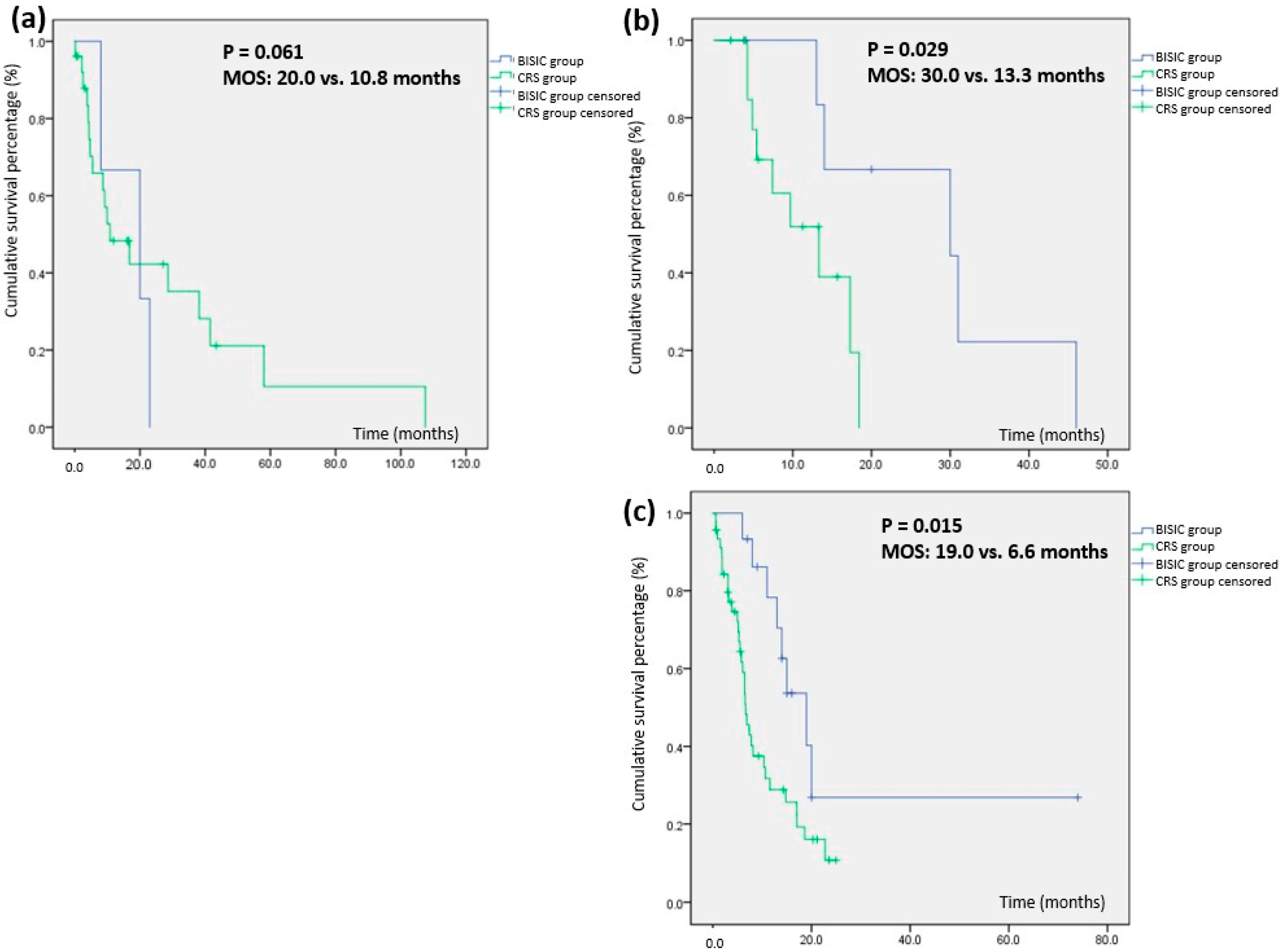
| First Encounter PCI | Median Survival Time | p-Value | Range (Overall) |
|---|---|---|---|
| 1–10 (n = 29) | 0.061 | ||
| BISIC group (n = 3) | 20 | 0.8–39.2 | |
| CRS group (n = 26) | 10.8 | 0.3–21.3 | |
| 11–19 (n = 23) | 0.029 | ||
| BISIC group (n = 7) | 30 | 0.1–61.4 | |
| CRS group (n = 16) | 13.3 | 5.0–21.6 | |
| 20–39 (n = 61) | 0.015 | ||
| BISIC group (n = 15) | 19 | 12.1–25.9 | |
| CRS group (n = 46) | 6.6 | 5.3–7.9 |
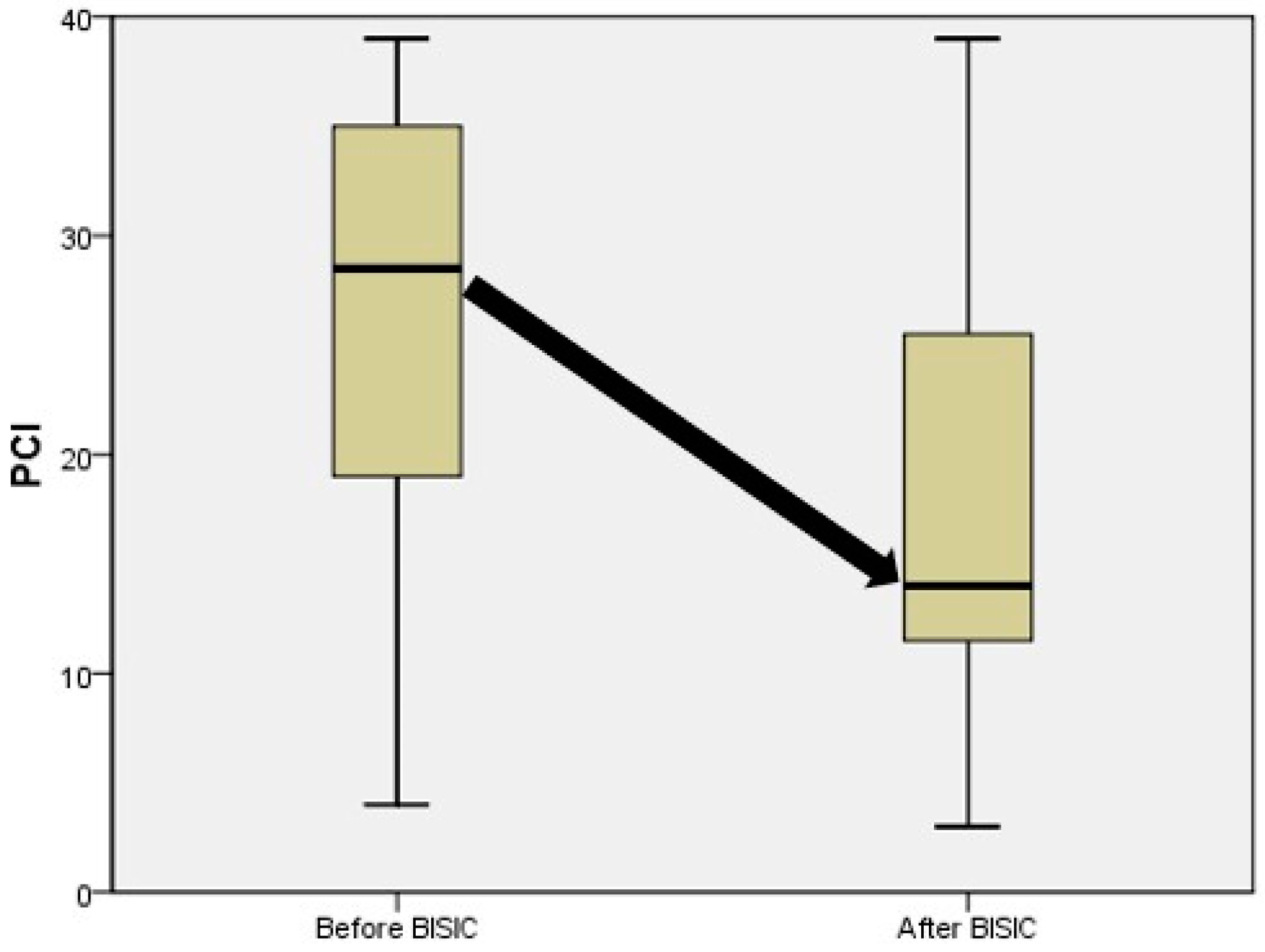
| BISIC Group | Pre-BISIC | Post-BISIC | Significance |
|---|---|---|---|
| PCI (mean ± SE) | 27 ± 2.3 | 16 ± 2.1 | 0.003 |
| PCI (median) | 27 | 14 | |
| Cytology | Conversion rate: 33% | ||
| positive | 12 | 8 | |
| negative | 13 | 17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.-H.; Yonemura, Y.; Ng, H.-J.; Lee, M.-C.; Su, B.-C.; Hsieh, M.-C. Benefit of Neoadjuvant Laparoscopic Hyperthermic Intraperitoneal Chemotherapy and Bidirectional Chemotherapy for Patients with Gastric Cancer with Peritoneal Carcinomatosis Considering Cytoreductive Surgery. Cancers 2023, 15, 3401. https://doi.org/10.3390/cancers15133401
Yu H-H, Yonemura Y, Ng H-J, Lee M-C, Su B-C, Hsieh M-C. Benefit of Neoadjuvant Laparoscopic Hyperthermic Intraperitoneal Chemotherapy and Bidirectional Chemotherapy for Patients with Gastric Cancer with Peritoneal Carcinomatosis Considering Cytoreductive Surgery. Cancers. 2023; 15(13):3401. https://doi.org/10.3390/cancers15133401
Chicago/Turabian StyleYu, Hsin-Hsien, Yutaka Yonemura, Hui-Ji Ng, Ming-Che Lee, Bor-Chyuan Su, and Mao-Chih Hsieh. 2023. "Benefit of Neoadjuvant Laparoscopic Hyperthermic Intraperitoneal Chemotherapy and Bidirectional Chemotherapy for Patients with Gastric Cancer with Peritoneal Carcinomatosis Considering Cytoreductive Surgery" Cancers 15, no. 13: 3401. https://doi.org/10.3390/cancers15133401
APA StyleYu, H. -H., Yonemura, Y., Ng, H. -J., Lee, M. -C., Su, B. -C., & Hsieh, M. -C. (2023). Benefit of Neoadjuvant Laparoscopic Hyperthermic Intraperitoneal Chemotherapy and Bidirectional Chemotherapy for Patients with Gastric Cancer with Peritoneal Carcinomatosis Considering Cytoreductive Surgery. Cancers, 15(13), 3401. https://doi.org/10.3390/cancers15133401