



Reproductive Results in Cancer Survivors after Fertility Sparing Management: The Need for the Standardization of Definitions


Abstract
:Simple Summary
Abstract
1. Introduction
2. Reproductive Definitions in Oncologic Patients: Live Birth Rate, Pregnancy Rate
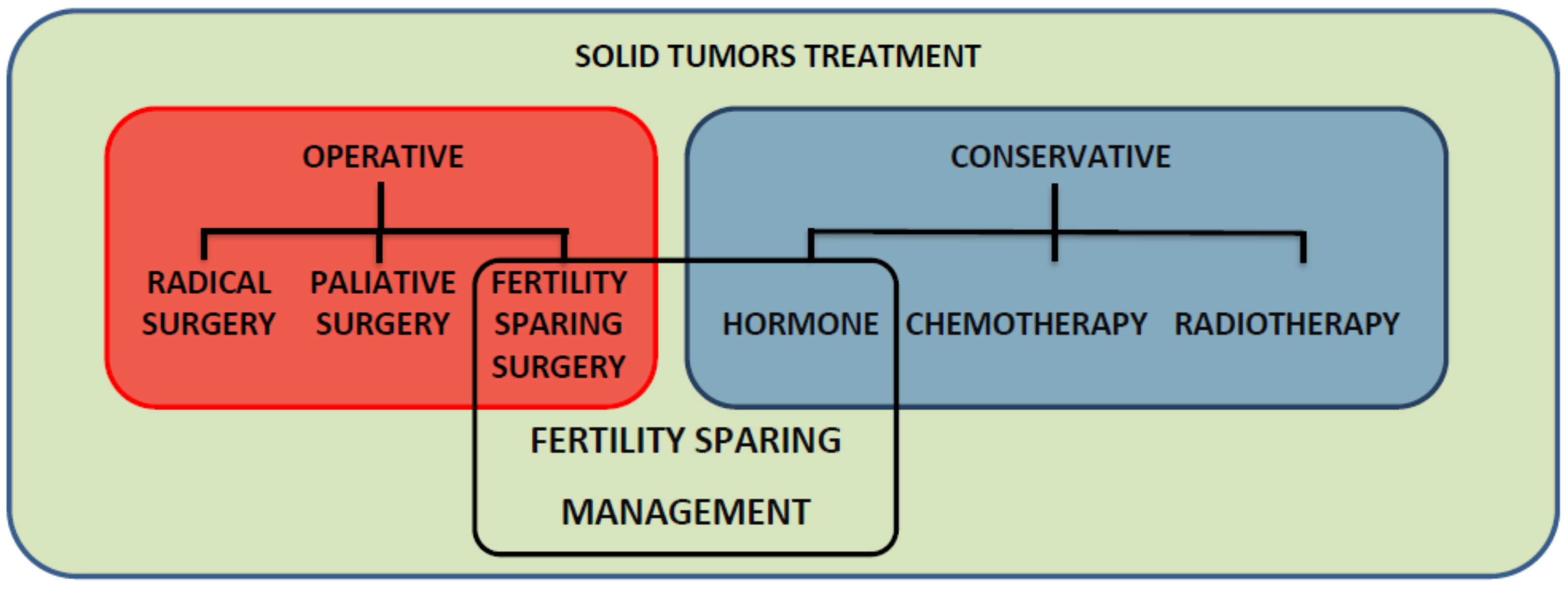
3. Fertility-Sparing Management vs. Conservative Management
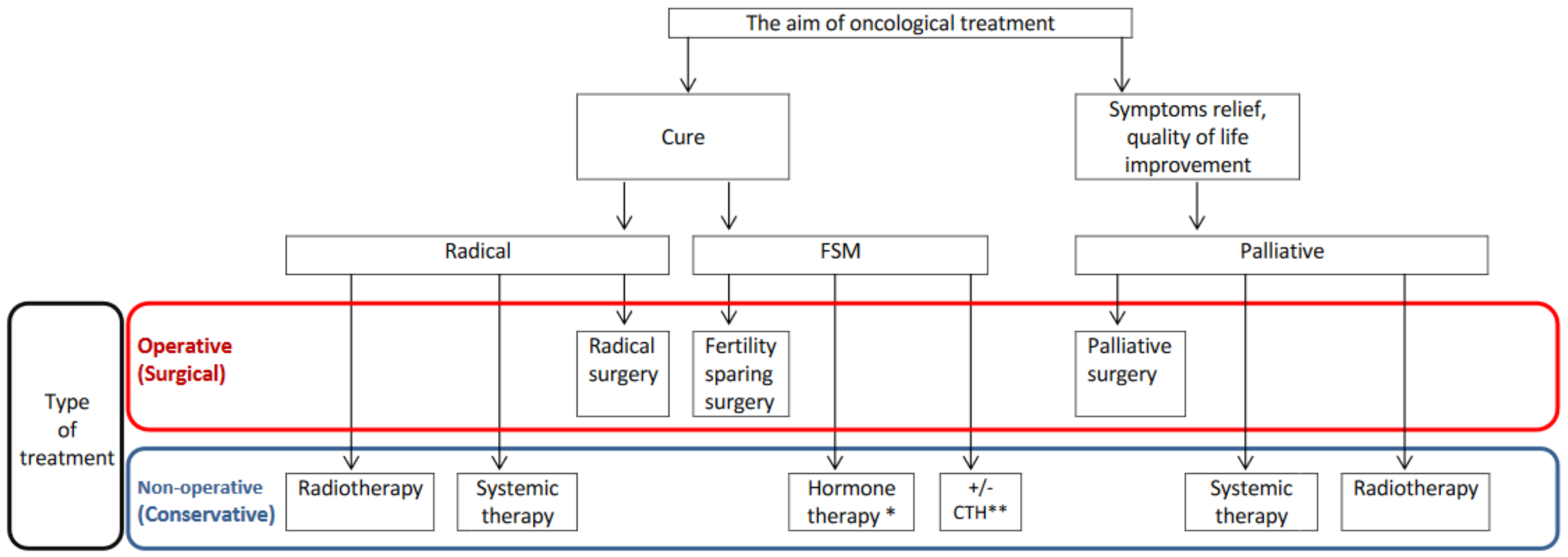
4. Fertility-Sparing Treatment vs. Less Radical Treatment: Treatment Mismatch
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Loren, A.W.; Mangu, P.B.; Beck, L.N.; Brennan, L.; Magdalinski, A.J.; Partridge, A.H.; Quinn, G.; Wallace, W.H.; Oktay, K. Fertility Preservation for Patients With Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 2500–2510. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Schover, L.R.; Partridge, A.H.; Patrizio, P.; Wallace, W.H.; Hagerty, K.; Beck, L.N.; Brennan, L.V.; Oktay, K. American Society of Clinical Oncology Recommendations on Fertility Preservation in Cancer Patients. J. Clin. Oncol. 2006, 24, 2917–2931. [Google Scholar] [CrossRef]
- Gonçalves, V.; Ferreira, P.L.; Saleh, M.; Tamargo, C.; Quinn, G.P. Perspectives of Young Women With Gynecologic Cancers on Fertility and Fertility Preservation: A Systematic Review. Oncologist 2022, 27, e251–e264. [Google Scholar] [CrossRef] [PubMed]
- Hohmann, C.; Borgmann-Staudt, A.; Rendtorff, R.; Reinmuth, S.; Holzhausen, S.; Willich, S.N.; Henze, G.; Goldbeck, L.; Keil, T. Patient Counselling on the Risk of Infertility and Its Impact on Childhood Cancer Survivors: Results from a National Survey. J. Psychosoc. Oncol. 2011, 29, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Goodman, L.R.; Balthazar, U.; Kim, J.; Mersereau, J.E. Trends of socioeconomic disparities in referral patterns for fertility preservation consultation. Hum. Reprod. 2012, 27, 2076–2081. [Google Scholar] [CrossRef] [Green Version]
- Bastings, L.; Baysal, O.; Beerendonk, C.C.M.; Braat, D.D.M.; Nelen, W.L.D.M. Referral for fertility preservation counselling in female cancer patients. Hum. Reprod. 2014, 29, 2228–2237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, H.B.; Howards, P.P.; Kramer, M.R.; Mertens, A.C.; Spencer, J.B. Which female cancer patients fail to receive fertility counseling before treatment in the state of Georgia? Fertil. Steril. 2016, 106, 1763–1771.e1. [Google Scholar] [CrossRef] [Green Version]
- Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics: Guidance for Industry. 2018. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-trial-endpoints-approval-cancer-drugs-and-biologics (accessed on 10 October 2022).
- Smith, E.S.; Moon, A.S.; O’Hanlon, R.; Leitao, M.M.; Sonoda, Y.; Abu-Rustum, N.R.; Mueller, J.J. Radical Trachelectomy for the Treatment of Early-Stage Cervical Cancer: A Systematic Review. Obstet. Gynecol. 2020, 136, 533–542. [Google Scholar] [CrossRef]
- Liu, D.; Cai, J.; Gao, A.; Wang, Z.; Cai, L. Fertility sparing surgery vs. radical surgery for epithelial ovarian cancer: A meta-analysis of overall survival and disease-free survival. BMC Cancer 2020, 20, 320. [Google Scholar] [CrossRef] [Green Version]
- Piatek, S.; Michalski, W.; Sobiczewski, P.; Bidzinski, M.; Szewczyk, G. The results of different fertility-sparing treatment modalities and obstetric outcomes in patients with early endometrial cancer and atypical endometrial hyperplasia: Case series of 30 patients and systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 263, 139–147. [Google Scholar] [CrossRef]
- Stensheim, H.; Cvancarova, M.; Møller, B.; Fosså, S.D. Pregnancy after adolescent and adult cancer: A population-based matched cohort study. Int. J. Cancer 2011, 129, 1225–1236. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.; Yang, J.; Yu, M.; Xie, W.; Cao, D.; Wu, M.; Pan, L.; Huang, H.; You, Y.; Shen, K. Oncofertility in patients with stage I epithelial ovarian cancer: Fertility-sparing surgery in young women of reproductive age. World J. Surg. Oncol. 2017, 15, 154. [Google Scholar] [CrossRef] [PubMed]
- Wethington, S.L.; Cibula, D.; Duska, L.R.; Garrett, L.; Kim, C.H.; Chi, D.S.; Sonoda, Y.; Abu-Rustum, N.R. An International Series on Abdominal Radical Trachelectomy: 101 Patients and 28 Pregnancies. Int. J. Gynecol. Cancer 2012, 22, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Tamauchi, S.; Kajiyama, H.; Yoshihara, M.; Ikeda, Y.; Yoshikawa, N.; Nishino, K.; Utsumi, F.; Niimi, K.; Suzuki, S.; Kikkawa, F. Reproductive outcomes of 105 malignant ovarian germ cell tumor survivors: A multicenter study. Am. J. Obstet. Gynecol. 2018, 219, 385.e1–385.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helpman, L.; Beiner, M.E.; Aviel-Ronen, S.; Perri, T.; Hogen, L.; Jakobson-Setton, A.; Ben-Baruch, G.; Korach, J. Safety of ovarian conservation and fertility preservation in advanced borderline ovarian tumors. Fertil. Steril. 2015, 104, 138–144. [Google Scholar] [CrossRef]
- Sobiczewski, P.; Piatek, S.; Michalski, W.; Kupryjańczyk, J.; Maciejewski, T.; Ołtarzewski, M.; Bidzinski, M. Obstetric outcomes after conservative management of ovarian borderline tumors in women of reproductive age: A single center experience. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 269, 126–131. [Google Scholar] [CrossRef]
- Fang, C.; Zhao, L.; Chen, X.; Yu, A.; Xia, L.; Zhang, P. The impact of clinicopathologic and surgical factors on relapse and pregnancy in young patients (≤40 years old) with borderline ovarian tumors. BMC Cancer 2018, 18, 1147. [Google Scholar] [CrossRef]
- Peiretti, M.; Congiu, F.; Ricciardi, E.; Maniglio, P.; Mais, V.; Angioni, S. Conservative treatment for well-differentiated endometrial cancer: When and why it should be considered in young women. Ecancermedicalscience 2019, 13, 892. [Google Scholar] [CrossRef]
- Jia, S.Z.; Xiang, Y.; Yang, J.J.; Shi, J.H.; Jia, C.W.; Leng, J.H. Oncofertility outcomes after fertility-sparing treatment of bilateral serous borderline ovarian tumors: Results of a large retrospective study. Hum. Reprod. 2020, 35, 328–339. [Google Scholar] [CrossRef]
- Ebisawa, K.; Takano, M.; Fukuda, M.; Fujiwara, K.; Hada, T.; Ota, Y.; Kurotsuchi, S.; Kanao, H.; Andou, M. Obstetric outcomes of patients undergoing total laparoscopic radical trachelectomy for early stage cervical cancer. Gynecol. Oncol. 2013, 131, 83–86. [Google Scholar] [CrossRef]
- Kim, C.H.; Abu-Rustum, N.R.; Chi, D.S.; Gardner, G.J.; Leitao, M.M.; Carter, J.; Barakat, R.R.; Sonoda, Y. Reproductive outcomes of patients undergoing radical trachelectomy for early-stage cervical cancer. Gynecol. Oncol. 2012, 125, 585–588. [Google Scholar] [CrossRef]
- Olawaiye, A.; Del Carmen, M.; Tambouret, R.; Goodman, A.; Fuller, A.; Duska, L.R. Abdominal radical trachelectomy: Success and pitfalls in a general gynecologic oncology practice. Gynecol. Oncol. 2009, 112, 506–510. [Google Scholar] [CrossRef] [PubMed]
- Ungár, L.; Pálfalvi, L.; Hogg, R.; Siklós, P.; Boyle, D.C.M.; Del Priore, G.; Smith, J.R. Abdominal radical trachelectomy: A fertility-preserving option for women with early cervical cancer. BJOG Int. J. Obstet. Gynaecol. 2005, 112, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, Z.; Wang, H.; Zang, R.; Zhou, Y.; Ju, X.; Ke, G.; Wu, X. Radical abdominal trachelectomy for cervical malignancies: Surgical, oncological and fertility outcomes in 62 patients. Gynecol. Oncol. 2011, 121, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Speiser, D.; Mangler, M.; Köhler, C.; Hasenbein, K.; Hertel, H.; Chiantera, V.; Gottschalk, E.; Lanowska, M. Fertility outcome after radical vaginal trachelectomy: A prospective study of 212 patients. Int. J. Gynecol. Cancer 2011, 21, 1635–1639. [Google Scholar] [CrossRef]
- Casadio, P.; La Rosa, M.; Alletto, A.; Magnarelli, G.; Arena, A.; Fontana, E.; Fabbri, M.; Giovannico, K.; Virgilio, A.; Raimondo, D.; et al. Fertility Sparing Treatment of Endometrial Cancer with and without Initial Infiltration of Myometrium: A Single Center Experience. Cancers 2020, 12, 3571. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Li, J.; Zhu, T.; Yu, H.; Lu, X. Fertility-sparing surgery for young patients with borderline ovarian tumors (BOTs): Single institution experience. J. Ovarian Res. 2016, 9, 16. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, J.H.; Spencer, C.; Herod, J.; Ind, T.E.J. Radical vaginal trachelectomy as a fertility-sparing procedure in women with early-stage cervical cancer-cumulative pregnancy rate in a series of 123 women. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 719–724. [Google Scholar] [CrossRef]
- Delle Marchette, M.; Ceppi, L.; Andreano, A.; Bonazzi, C.M.; Buda, A.; Grassi, T.; Giuliani, D.; Sina, F.; Lamanna, M.; Bianchi, T.; et al. Oncologic and fertility impact of surgical approach for borderline ovarian tumours treated with fertility sparing surgery. Eur. J. Cancer 2019, 111, 61–68. [Google Scholar] [CrossRef]
- Falcone, F.; Laurelli, G.; Losito, S.; Di Napoli, M.; Granata, V.; Greggi, S. Fertility preserving treatment with hysteroscopic resection followed by progestin therapy in young women with early endometrial cancer. J. Gynecol. Oncol. 2017, 28, e2. [Google Scholar] [CrossRef] [Green Version]
- Ceppi, L.; Galli, F.; Lamanna, M.; Magni, S.; Dell’Orto, F.; Verri, D.; Delle Marchette, M.; Lissoni, A.A.; Sina, F.; Giuliani, D.; et al. Ovarian function, fertility, and menopause occurrence after fertility-sparing surgery and chemotherapy for ovarian neoplasms. Gynecol. Oncol. 2019, 152, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Capozzi, V.A.; Butera, D.; Armano, G.; Monfardini, L.; Gaiano, M.; Gambino, G.; Sozzi, G.; Merisio, C.; Berretta, R. Obstetrics outcomes after complete and partial molar pregnancy: Review of the literature and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 259, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Eskander, R.N.; Randall, L.M.; Berman, M.L.; Tewari, K.S.; Disaia, P.J.; Bristow, R.E. Fertility preserving options in patients with gynecologic malignancies. Am. J. Obstet. Gynecol. 2011, 205, 103–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallos, I.D.; Yap, J.; Rajkhowa, M.; Luesley, D.M.; Coomarasamy, A.; Gupta, J.K. Regression, relapse, and live birth rates with fertility-sparing therapy for endometrial cancer and atypical complex endometrial hyperplasia: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2012, 207, 266.e1–266.e12. [Google Scholar] [CrossRef] [PubMed]
- Van Der Plas, R.C.J.; Bos, A.M.E.; Jürgenliemk-Schulz, I.M.; Gerestein, C.G.; Zweemer, R.P. Fertility-sparing surgery and fertility preservation in cervical cancer: The desire for parenthood, reproductive and obstetric outcomes. Gynecol. Oncol. 2021, 163, 538–544. [Google Scholar] [CrossRef]
- Wei, J.; Zhang, W.; Feng, L.; Gao, W. Comparison of fertility-sparing treatments in patients with early endometrial cancer and atypical complex hyperplasia: A meta-analysis and systematic review. Medicine 2017, 96, e8034. [Google Scholar] [CrossRef]
- Johansen, G.; Dahm-Kähler, P.; Staf, C.; Flöter Rådestad, A.; Rodriguez-Wallberg, K.A. Reproductive and obstetrical outcomes with the overall survival of fertile-age women treated with fertility-sparing surgery for borderline ovarian tumors in Sweden: A prospective nationwide population-based study. Fertil. Steril. 2021, 115, 157–163. [Google Scholar] [CrossRef]
- Schuurman, T.; Zilver, S.; Samuels, S.; Schats, W.; Amant, F.; van Trommel, N.; Lok, C. Fertility-Sparing Surgery in Gynecologic Cancer: A Systematic Review. Cancers 2021, 13, 1008. [Google Scholar] [CrossRef]
- Bercow, A.; Nitecki, R.; Brady, P.C.; Rauh-Hain, J.A. Outcomes after Fertility-sparing Surgery for Women with Ovarian Cancer: A Systematic Review of the Literature. J. Minim. Invasive Gynecol. 2021, 28, 527–536.e1. [Google Scholar] [CrossRef]
- Fauvet, R.; Poncelet, C.; Boccara, J.; Descamps, P.; Fondrinier, E.; Daraï, E. Fertility after conservative treatment for borderline ovarian tumors: A French multicenter study. Fertil. Steril. 2005, 83, 284–290. [Google Scholar] [CrossRef]
- Ouldamer, L.; Bendifallah, S.; Naoura, I.; Body, G.; Uzan, C.; Morice, P.; Ballester, M.; Daraï, E. Nomogram to predict live birth rate after fertility-sparing surgery for borderline ovarian tumours. Hum. Reprod. 2016, 31, 1732–1737. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.; Catena, U.; Saccone, G.; Di Spiezio Sardo, A. Conservative Surgery in Endometrial Cancer. J. Clin. Med. 2021, 11, 183. [Google Scholar] [CrossRef] [PubMed]
- Bearak, J.; Popinchalk, A.; Ganatra, B.; Moller, A.B.; Tunçalp, Ö.; Beavin, C.; Kwok, L.; Alkema, L. Unintended pregnancy and abortion by income, region, and the legal status of abortion: Estimates from a comprehensive model for 1990–2019. Lancet Glob. Health 2020, 8, e1152–e1161. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.C.; Clark, J.A.; Manola, J.; Talcott, J.A. Treatment ‘mismatch’ in early prostate cancer: Do treatment choices take patient quality of life into account? Cancer 2008, 112, 61–68. [Google Scholar] [CrossRef]
- Rozen, G.; Rogers, P.; Chander, S.; Anderson, R.; McNally, O.; Umstad, M.; Winship, A.; Hutt, K.; Teh, W.T.; Dobrotwir, A.; et al. Clinical summary guide: Reproduction in women with previous abdominopelvic radiotherapy or total body irradiation. Hum. Reprod. Open 2020, 2020, hoaa045. [Google Scholar] [CrossRef]
- Critchley, H.O.D. Impact of Cancer Treatment on Uterine Function. J. Natl. Cancer Inst. Monogr. 2005, 2005, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Fruscio, R.; Corso, S.; Ceppi, L.; Garavaglia, D.; Garbi, A.; Floriani, I.; Franchi, D.; Cantù, M.G.; Bonazzi, C.M.; Milani, R.; et al. Conservative management of early-stage epithelial ovarian cancer: Results of a large retrospective series. Ann. Oncol. 2013, 24, 138–144. [Google Scholar] [CrossRef]
- Morice, P.; Leblanc, E.; Rey, A.; Baron, M.; Querleu, D.; Blanchot, J.; Duvillard, P.; Lhommé, C.; Castaigne, D.; Classe, J.M.; et al. Conservative treatment in epithelial ovarian cancer: Results of a multicentre study of the GCCLCC (Groupe des Chirurgiens de Centre de Lutte Contre le Cancer) and SFOG (Société Française d’Oncologie Gynécologique). Hum. Reprod. 2005, 20, 1379–1385. [Google Scholar] [CrossRef] [Green Version]
- CDC’s Division of Reproductive Health Works to Improve Mental Health among Women of Reproductive Age. Available online: https://www.cdc.gov/ccindex/pdf/mentalhealthamongwomenofreproductiveage_vb.pdf (accessed on 27 April 2023).
- World Health Organization. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/women-of-reproductive-age-(15-49-years)-population-(thousands) (accessed on 27 April 2023).
- Yang, B.; Gulinazi, Y.; Du, Y.; Ning, C.; Cheng, Y.; Shan, W.; Luo, X.; Zhang, H.; Zhu, Q.; Ma, F.; et al. Metformin plus megestrol acetate compared with megestrol acetate alone as fertility-sparing treatment in patients with atypical endometrial hyperplasia and well-differentiated endometrial cancer: A randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 848–857. [Google Scholar] [CrossRef]
- The ESHRE Guideline Group on Female Fertility Preservation; Anderson, R.A.; Amant, F.; Braat, D.; D’Angelo, A.; Chuva De Sousa Lopes, S.M.; Demeestere, I.; Dwek, S.; Frith, L.; Lambertini, M.; et al. ESHRE guideline: Female fertility preservation. Hum. Reprod. Open 2020, 2020, hoaa052. [Google Scholar] [CrossRef]
- Vollenhoven, B.; Hunt, S. Ovarian ageing and the impact on female fertility. F1000Research 2018, 7, 1835. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists Committee on Gynecologic Practice and Practice Committee. Female age-related fertility decline. Committee Opinion No. 589. Fertil. Steril. 2014, 101, 633–634. [Google Scholar] [CrossRef] [PubMed]
- Bentivegna, E.; Gouy, S.; Maulard, A.; Pautier, P.; Leary, A.; Colombo, N.; Morice, P. Fertility-sparing surgery in epithelial ovarian cancer: A systematic review of oncological issues. Ann. Oncol. 2016, 27, 1994–2004. [Google Scholar] [CrossRef] [PubMed]
- Frick, A.C.; Barber, M.D.; Paraiso, M.F.R.; Ridgeway, B.; Jelovsek, J.E.; Walters, M.D. Attitudes Toward Hysterectomy in Women Undergoing Evaluation for Uterovaginal Prolapse. Female Pelvic Med. Reconstr. Surg. 2013, 19, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Korbly, N.B.; Kassis, N.C.; Good, M.M.; Richardson, M.L.; Book, N.M.; Yip, S.; Saguan, D.; Gross, C.; Evans, J.; Lopes, V.V.; et al. Patient preferences for uterine preservation and hysterectomy in women with pelvic organ prolapse. Am. J. Obstet. Gynecol. 2013, 209, 470.e1–470.e6. [Google Scholar] [CrossRef]
- Wong, K.; Jakus-Waldman, S.; Yazdany, T. Patient Beliefs Regarding Hysterectomy in Women Seeking Surgery for Pelvic Organ Prolapse: Findings in a Predominantly Hispanic Population. Female Pelvic Med. Reconstr. Surg. 2014, 20, 267–271. [Google Scholar] [CrossRef]
- Lyatoshinsky, P.; Fünfgeld, C.; Popov, A.; Bezhenar, V.; Krutova, V.; Ulrich, D.; Umek, W. Pelvic organ prolapse patients’ attitudes and preferences regarding their uterus: Comparing German- and Russian-speaking women. Int. Urogynecol. J. 2019, 30, 2077–2083. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, N.T.; Merchant, M.; Ritterman Weintraub, M.L.; Salyer, C.; Poceta, J.; Diaz, L.; Zaritsky, E.F. Alternative Treatment Utilization Before Hysterectomy for Benign Gynecologic Conditions at a Large Integrated Health System. J. Minim. Invasive Gynecol. 2019, 26, 847–855. [Google Scholar] [CrossRef]
- Pinquart, M.; Duberstein, P.R. Information needs and decision-making processes in older cancer patients. Crit. Rev. Oncol. Hematol. 2004, 51, 69–80. [Google Scholar] [CrossRef]
- Murthy, D.; Eldredge, M. Who tweets about cancer? An analysis of cancer-related tweets in the USA. Digit. Health 2016, 2, 205520761665767. [Google Scholar] [CrossRef] [Green Version]
- Sio, T.T.; Chang, K.; Jayakrishnan, R.; Wu, D.; Politi, M.; Malacarne, D.; Saletnik, J.; Chung, M. Patient age is related to decision-making, treatment selection, and perceived quality of life in breast cancer survivors. World J. Surg. Oncol. 2014, 12, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, J.L.; Letourneau, J.; Salem, W.; Cil, A.P.; Chan, S.W.; Chen, L.; Rosen, M.P. Regret around fertility choices is decreased with pre-treatment counseling in gynecologic cancer patients. J. Cancer Surviv. 2017, 11, 58–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, R.G.; Hart, A.; Dawes, P.J. Mastectomy or conservation: The patient’s choice. BMJ 1988, 297, 1167–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NIH Consensus Conference. Treatment of early-stage breast cancer. JAMA 1991, 265, 391–395. [Google Scholar] [CrossRef]
- Denberg, T.D.; Melhado, T.V.; Steiner, J.F. Patient treatment preferences in localized prostate carcinoma: The influence of emotion, misconception, and anecdote. Cancer 2006, 107, 620–630. [Google Scholar] [CrossRef]
- Samuel, D.; Kwon, D.; Huang, M.; Zhao, W.; Roy, M.; Tabuyo-Martin, A.; Siemon, J.; Schlumbrecht, M.P.; Pearson, J.M.; Sinno, A.K. Disparities in refusal of surgery for gynecologic cancer. Gynecol. Oncol. 2023, 174, 1–10. [Google Scholar] [CrossRef]
- Sud, S.; Holmes, J.; Eblan, M.; Chen, R.; Jones, E. Clinical characteristics associated with racial disparities in endometrial cancer outcomes: A surveillance, epidemiology and end results analysis. Gynecol. Oncol. 2018, 148, 349–356. [Google Scholar] [CrossRef]
- Straubhar, A.M.; Parsons, M.W.; Francis, S.; Gaffney, D.; Maurer, K.A. Refusal of surgery and survival outcomes in endometrial cancer. Int. J. Gynecol. Cancer 2021, 31, 1236–1241. [Google Scholar] [CrossRef]
- Denberg, T.D.; Beaty, B.L.; Kim, F.J.; Steiner, J.F. Marriage and ethnicity predict treatment in localized prostate carcinoma. Cancer 2005, 103, 1819–1825. [Google Scholar] [CrossRef]
- Gaitanidis, A.; Alevizakos, M.; Tsalikidis, C.; Tsaroucha, A.; Simopoulos, C.; Pitiakoudis, M. Refusal of Cancer-Directed Surgery by Breast Cancer Patients: Risk Factors and Survival Outcomes. Clin. Breast Cancer 2018, 18, e469–e476. [Google Scholar] [CrossRef]
- Kaltenmeier, C.; Malik, J.; Yazdani, H.; Geller, D.A.; Medich, D.; Zureikat, A.; Tohme, S. Refusal of cancer-directed treatment by colon cancer patients: Risk factors and survival outcomes. Am. J. Surg. 2020, 220, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Amini, A.; Verma, V.; Li, R.; Vora, N.; Kang, R.; Gernon, T.J.; Chang, S.; Karam, S.; Massarelli, E.; Maghami, E.G.; et al. Factors predicting for patient refusal of head and neck cancer therapy. Head Neck 2020, 42, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Tohme, S.; Kaltenmeier, C.; Bou-Samra, P.; Varley, P.R.; Tsung, A. Race and Health Disparities in Patient Refusal of Surgery for Early-Stage Pancreatic Cancer: An NCDB Cohort Study. Ann. Surg. Oncol. 2018, 25, 3427–3435. [Google Scholar] [CrossRef] [PubMed]
- Piątek, S.; Szymusik, I.; Dańska-Bidzińska, A.; Ołtarzewski, M.; Trojan, G.; Bidziński, M. Fertility-Sparing Management May Be Considered in Young Women with Uterine Sarcoma. J. Clin. Med. 2022, 11, 4761. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Live Birth Rate | |
|---|---|
| Author | Definitions |
| Capozzi et al. [33] | The number of live-term births divided by the number of pregnancies. |
| Eskander et al. [34] | The number of live births divided by the number of pregnancies. |
| Gallos et al. [35] | The number of women who gave birth to healthy infants divided by the total number of women undergoing fertility-sparing therapy. |
| Peiretti et. al. [19] | The total number of live births divided by patients who attempted to conceive. |
| Plas et al. [36] | The number of live births divided by the number of pregnancies. |
| Shepherd et al. [29] | The number of live births divided by the number of pregnancies (excluding patients who terminated the pregnancy). |
| Wei et al. [37] | The number of women who delivered divided by the total number of patients. |
| Pregnancy rate | |
| Author | Definitions |
| Eskander et al. [34] | The number of pregnancies divided by the total number of patients. |
| Peiretti et al. [19] | The total number of pregnancies divided by the number of patients who attempted to conceive. |
| Plas et al. [36] | The number of patients who achieved pregnancy divided by the number of patients who attempted to get pregnant. |
| Jia et al. [20] | The number of patients who achieved pregnancy divided by the number of patients who tried to conceive. |
| Author | Other terms and definitions |
| Fang et al. [18] | Pregnancy outcome—The number of patients achieving pregnancy divided by the number of patients attempting to get pregnant. |
| Johansen et al. [38] | Conception rate—The number of patients with childbirth after surgery divided by the patients treated with fertility-sparing surgery. |
| Shepherd et al. [29] | Cumulative pregnancy rate—Based on the women who desired to conceive as a denominator using the Kaplan–Meier method. Cumulative actuarial probability of conception adjusted for contraceptive usage—Proposed for women who are trying to conceive following successful treatment (the Kaplan–Meier method). |
| Treatment Method | ||
|---|---|---|
| Cancer Type | Operative (Surgical) | Non-Operative (Conservative) |
| Cervical cancer | + | − * |
| Endometrial cancer | − | + (Hormone based therapy) |
| Borderline ovarian tumor | + | − |
| Ovarian/Fallopian tube cancer | + | −/+ ** |
| Nonepithelial ovarian cancer | + | + (Chemotherapy) |
| Gestational trophoblastic neoplasia | − | + (Chemotherapy) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piątek, S.; Szymusik, I.; Bidziński, M. Reproductive Results in Cancer Survivors after Fertility Sparing Management: The Need for the Standardization of Definitions. Cancers 2023, 15, 3569. https://doi.org/10.3390/cancers15143569
Piątek S, Szymusik I, Bidziński M. Reproductive Results in Cancer Survivors after Fertility Sparing Management: The Need for the Standardization of Definitions. Cancers. 2023; 15(14):3569. https://doi.org/10.3390/cancers15143569
Chicago/Turabian StylePiątek, Szymon, Iwona Szymusik, and Mariusz Bidziński. 2023. "Reproductive Results in Cancer Survivors after Fertility Sparing Management: The Need for the Standardization of Definitions" Cancers 15, no. 14: 3569. https://doi.org/10.3390/cancers15143569
APA StylePiątek, S., Szymusik, I., & Bidziński, M. (2023). Reproductive Results in Cancer Survivors after Fertility Sparing Management: The Need for the Standardization of Definitions. Cancers, 15(14), 3569. https://doi.org/10.3390/cancers15143569