1. Introduction
Breast cancer (BC) is the most common cancer and leading cause of cancer death worldwide [
1,
2]. According to the World Health Organization (WHO), 2.3 million women were diagnosed with BC in 2020, and 685,000 deaths were BC-related [
3]. As a highly heterogeneous disease, BC diagnosis and treatment are complex and differ according to clinical tumor subtypes [
4,
5]. Opportunities for breast cancer therapies have evolved tremendously in recent decades, offering a variety of therapeutic approaches depending on whether the therapy required is adjuvant, neoadjuvant or metastatic. Therapies include surgery, radiation, and systemic treatments, such as chemotherapy and endocrine therapy [
6,
7,
8]. New therapeutic options have been introduced and included in international therapeutic guidelines for BC treatment, including, for example, monoclonal antibodies that target human epidermal growth factor receptor 2 (HER2). Therapies that target nuclear receptors (NRs), such as the estrogen receptor (ER) and the progesterone receptor (PR), are very promising treatment options and have been shown to improve prognosis in studies conducted over many decades. Endocrine therapy regimens resulted in an approximately 30% decrease in BC-associated mortality, making them essential for the treatment of hormone receptor-positive (HR+) BC [
9,
10,
11]. Moreover, clinical studies indicate a strong correlation between the expression of “classical steroid hormone receptors”, such as ER and PR, and disease progression [
12,
13,
14,
15,
16]. Nevertheless, some tumors are resistant to these established therapeutic options, making the identification of new therapeutic targets central to our current research interests [
17].
Currently, personalized BC therapy already includes NR-specific targeted therapies for both prevention and treatment [
18]. NRs are activated via binding to amphiphilic hormones and function mainly as transcription factors in the nucleus [
19,
20]. Recent literature and data from our research group show that, in addition to the well-known NR, nuclear type II receptors, including retinoid X receptor alpha (RXRα), thyroid hormone receptors (TRs) and vitamin D receptor (VDR), play an important role in the pathophysiology of both BC and other cancers [
21,
22,
23]. Studies of the role of NR in different intracellular compartments have shown that its specific prognostic value depends on subcellular localization [
24]. Czogalla et al., demonstrated a direct association between cytoplasmic localization of VDR and poorer overall survival (OS) in ovarian cancer [
25]. In the case of TRalpha, strong nuclear localization was reported to be a positive predictor of survival in epithelial ovarian cancer [
22]. In addition, TRβ and TRβ1 were negative prognosticators if expressed in the cytoplasm [
26]. In contrast, nuclear TRβ1 has been identified to have cancer-promoting activities in BC development [
24]. Very recently, we found that cytoplasmic colocalization of RXRα and PPARγ, as well as cytoplasmic RXRα itself, are independent negative prognosticators in breast cancer patients [
27,
28].
Retinoids derived from vitamin A and co-activator molecules bind and activate RXRα, which then regulate the transcriptional activity of heterodimers with other nuclear receptors, like TR and VDR, and are activated in the nucleus to eventually promote its transcriptional activity after hormone binding [
29]. In addition, thyroid hormones bind to its receptor monomer, and the RXRα/TR heterodimer acts as transcription factor [
30,
31,
32,
33]. As we recently discovered that cytoplasmic TRβ1 was correlated with favorable survival, whereas nuclear TRβ1 had a statistically significant correlation with poor outcome, we were interested in finding subcellular-specific analyses of TRα-expression in this study [
24].
Due to its alleged contradictory role in BC prognosis, it appeared necessary to further investigate the behavior of TRα in BC. As cytoplasmic shuttling of type II nuclear receptors was found in many cases in our breast cancer collection, we focused on the relationship between TR-shuttling and survival. In addition, nucleocytoplasmic shuttling of TRα is a long-known phenomenon, albeit a phenomenon about which we lack understanding of its clinical relevance [
34]. Former studies of our group showed that shuttling of nuclear type II receptors from the nucleus to the cytoplasm is accompanied by unfavorable outcomes in breast [
27] and ovarian cancer [
22]. Although thyroid hormone receptors were also analyzed in these tumor entities [
22,
24], to date, no study has identified TRα subcellular localization as a prognostic factor in human breast cancer samples. New findings may be promising in regard to individualized targeted BC therapy. In this study, we define the prognostic role of TRα and its isoforms α1 and α2 in association with cytoplasmic and nuclear expression of RXRα, respectively, in BC and relate the results to clinico-pathological criteria.
4. Discussion
The aim of this study was to evaluate the prognostic impact of subcellular expression of thyroid hormone receptors TRα, TRα1, and TRα2 determined in a large group of BC tissues and correlate the results with clinicopathologic criteria. So far, the role of thyroid hormones and their receptors (TR) in BC patients has not been sufficiently investigated [
41].
TRs, which are members of the nuclear receptor superfamily, mediate the classical genomic actions of TH signaling in many tissues and regulate important developmental and homeostatic processes [
24,
45,
46]. The TRα isoforms (TRα1 and TRα2) arise due to alternative splicing of the THRA gene [
47]. TRα1 can bind thyroid hormone and mediate its biological effects [
47,
48]. TRα2 has no binding site for the thyroid hormone [
47,
49,
50,
51]. Unbound TRα2 is a weak antagonist of thyroid hormone-mediated transcription [
47]. TRα expression was significantly associated with DFS in patients with breast cancer [
52]. The expression of TRα2 correlated positively with the expression of ER and PR and correlated negatively with HER2 expression [
47]. Low TRα2 expression was associated with inferior 5-year OS compared to high expression [
47]. TRs heterodimerize with the retinoid X receptor (RXR) and act as ligand-dependent transcription factors [
24]. TH activity is influenced by TR mutations, interactions with heterodimerization partners and coregulators, and expression of TR subtypes and their intracellular localization [
53,
54]. The shuttling of several TR isoforms between the nucleus and cytoplasm occurs, which may lead to specific TH-signaling activities in the nucleus, cytoplasm, or mitochondria [
24,
45,
46]. Our previous studies showed that TRα and TRβ are expressed in the nuclei of breast cancer cells [
41]. TRα2 was significantly associated with prognostic histo-pathological parameters, such as tumor size, axillary lymph node involvement, and grading and hormone receptor status [
41]. There is a trend of TRα2 acting as an independent predictor of disease-free and overall survival (OS) [
41]. In BRCA1-associated breast cancer, TRβ is a positive prognostic factor of OS at 5 years post-treatment, while TRα positivity predicts a reduced OS at 5 years posy-treatment [
43]. Nuclear and cytoplasmic TRβ1 appear to be independent markers of either poor or good prognosis [
24].
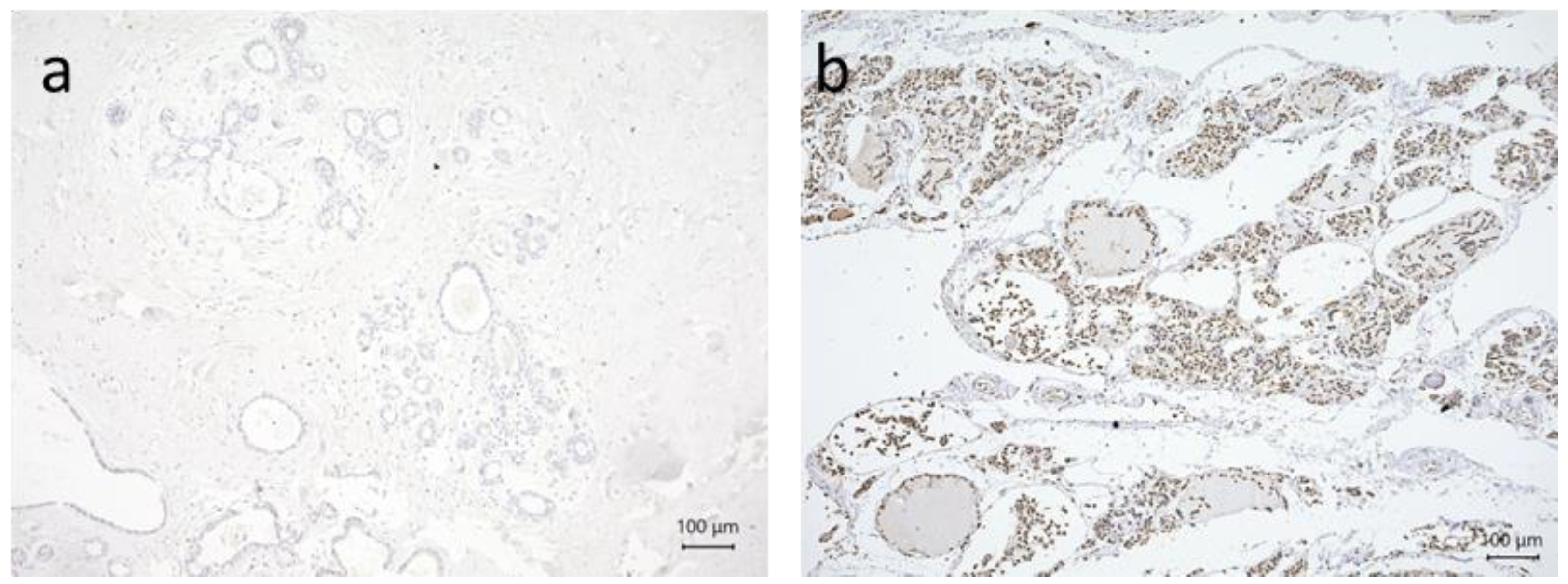
This paper represents the first study used to determine the respective prognostic roles of cytoplasmic and nuclear TRα expression in BC using a relatively large group of patients who received no treatment prior to surgery and completed long-term follow-up. The results of this study show that cytoplasmic TRα expression is a significant negative prognostic marker, while nuclear TR2α expression appears to be a protective factor.
To better understand the prognostic function of TRα in the pathogenesis of BC, this study focused separately on nuclear and cytoplasmic TRα, TRα1, and TRα2 expression in BC. Our study confirmed that TRα is expressed with a nuclear and cytoplasmic localization. Interestingly, nuclear and cytoplasmic forms of TRα may hereby exhibit opposite roles in mammary carcinogenesis.
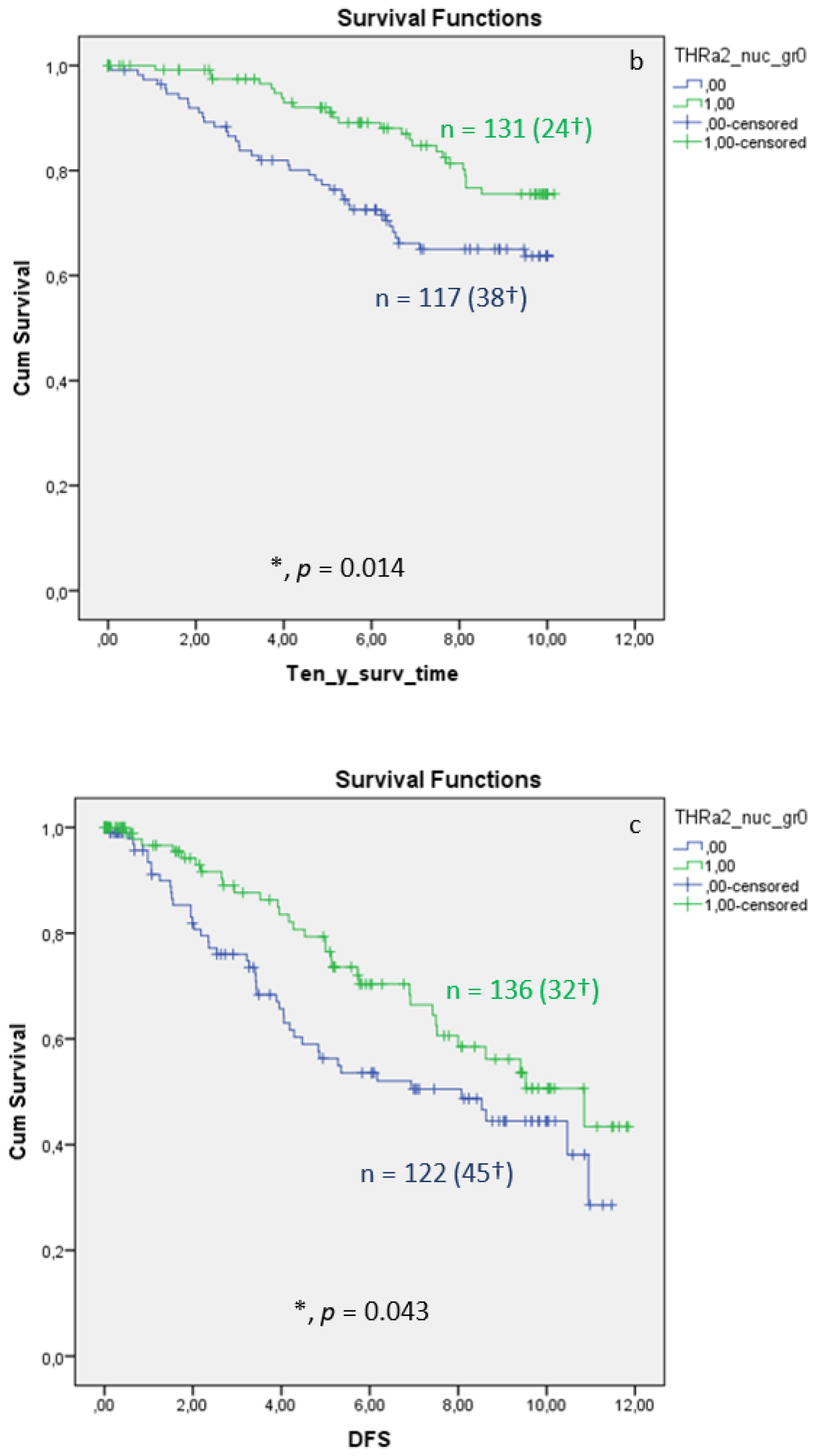
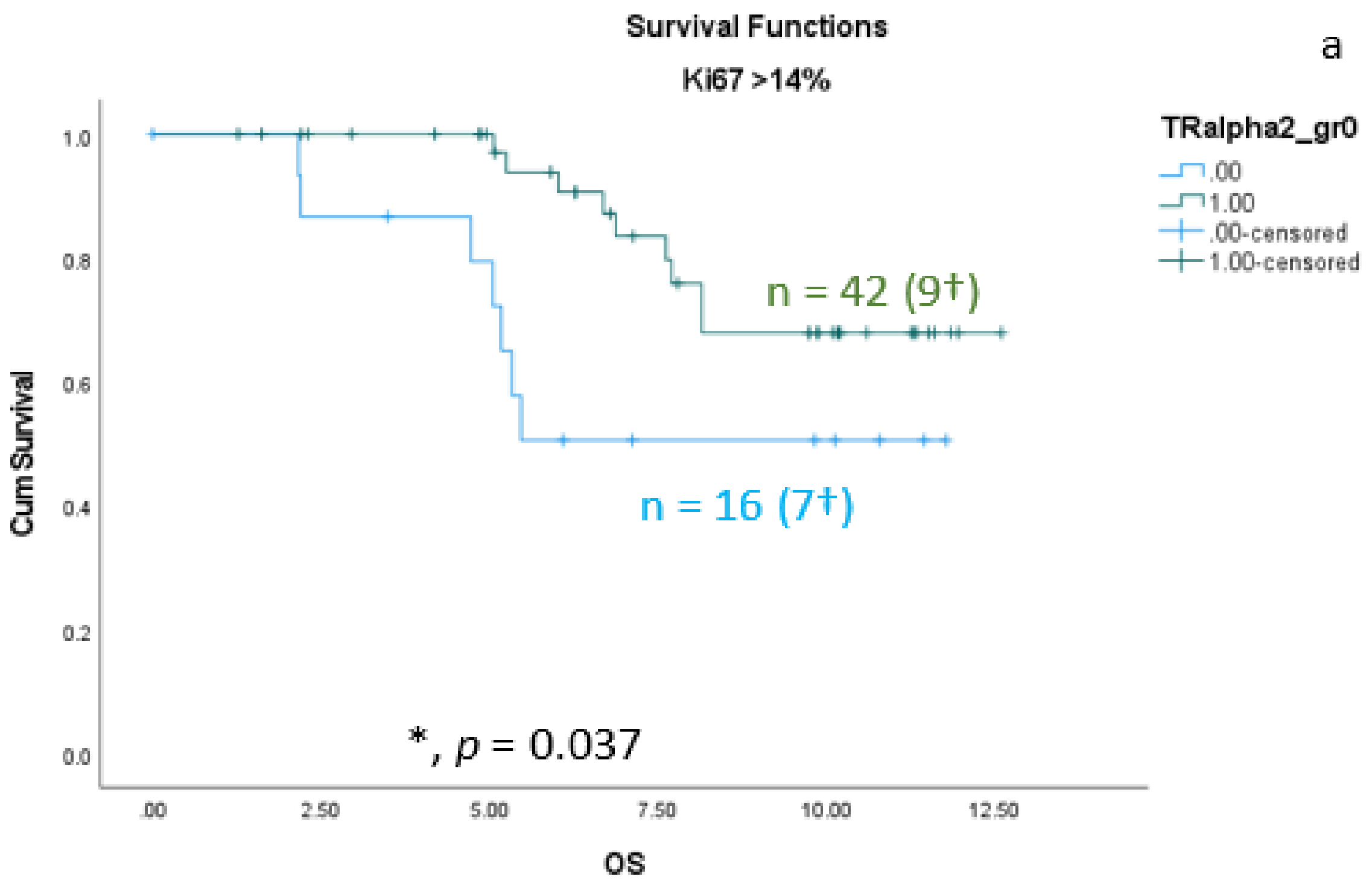
Cytoplasmic expression of TRα in BC tissue was associated with significantly lower OS and ten-year survival rate, as well as tendential lower DFS, whereas nuclear expression of TRα revealed a tendential association with improved OS. In a multivariate analysis, cytoplasmic TRα is considered to be an independent negative prognostic factor of OS when adjusted to fit clinico-pathological parameters. TRα1 had no prognostic relevance, whereas nuclear TRα2 expression in BC tissue was associated with significantly longer OS, ten-year survival, and DFS. Additionally, a multivariate analysis identified nuclear TRα2 expression as an independent positive prognosticator of OS when adjusted to fit clinico-pathological parameters.
Interestingly, the results of our study confirm our former investigation into the subcellular localization of PPARγ [
27,
55] and RXRα [
27,
28] and its influence on survival in breast cancer patients. Within the latter studies, we showed that cytoplasmic localization of either PPARγ or RXRα is associated with shortened survival, whereas nuclear localization of both receptors leads to better outcomes. RXRα is, of course, also the heterodimeric partner of all thyroid hormone receptors [
56,
57,
58]. The positive impact of TRα on the BC prognosis is possibly caused by heterodimerization with RXRα in the nucleus of breast cancer cells. Nuclear RXRα expression in breast cancer tissue leads to an improved OS, whereas cytoplasmic RXRα expression is significantly correlated with poor outcomes in terms of both OS and DFS [
28]. The expression of cytoplasmic RXRα is correlated with more aggressive breast cancer types, whereas nuclear RXRα expression appears to be a protective factor [
28]. Cytoplasmic RXRα also seems to be a negative prognosticator of Her-2neu-negative and triple-negative patients [
28]. RXR- and PPARγ-forming heterodimers in breast cancer cells are reported to induce growth arrest and differentiation in breast cancer cells [
29]. Depending on the localization of TRα and corresponding NR, specific responses, such as growth arrest and apoptosis, may be induced [
59].
In contrast to the above-described situation, nuclear TRβ1 expression was related to poor outcomes, and cytoplasmic expression was related to favorable outcomes [
24]. This finding is an exceptional result, because cytoplasmic expression of nuclear receptors is usually associated with reduced overall survival, and our investigation into the role of TRβ1 subcellular localization and outcomes in ovarian cancer showed that cytoplasmic TRβ1 is associated with poor outcomes [
26]. Due to the fact that TRα2 has the strongest input in survival, while TRα1 has no impact on survival, the limited prognostic role of the general TRα antibody can be explained by the fact that it binds to both subtypes. This assumption is highly speculative because we have only limited information about the molecular role of both receptors.
The role of TRα2 in breast cancer was described previously by Sandsveden et al. [
60], although no subcellular localization was analyzed. They stated that low tumor-specific TRα2 expression was, in their study, associated with prognostically unfavorable tumor characteristics and a higher mortality in breast cancer, though it was not independent of other prognostic factors [
60].
In addition, in previous studies, we showed that TRα2 expression had a positive association with disease-free survival in multifocal breast cancer [
42]. In that study, we did not investigate the subcellular localization. Furthermore, in an earlier study, our group found an inverse correlation between TRα2 and tumor size, lymph node involvement, histological grade, and hormone receptor expression, as well as a better disease-free survival rate among 82 women with higher levels of tumor-specific TRα2 [
41]. Jerzak et al., also found evidence of an association between higher tumor-specific expression of TRα2 and favorable prognostic characteristics, as well as improved survival among 130 women with invasive breast cancer [
47].
It is already known that TRα2 is an alternative splice product of the TRα primary transcript, whose unique carboxyl terminus does not bind thyroid hormones and, therefore, does not activate transcription [
61]. In addition, the same group found that cellular localization studies demonstrated that phosphorylated TRα2 is primarily cytoplasmic, whereas unphosphorylated TRα2 is primarily nuclear. Since RNA binding is a property of unphosphorylated TRα2, the TRα2–RNA interaction likely represents a nuclear function of TRα2 [
61]. Therefore, nuclear-expressed TRα2 that is associated with favorable outcome in breast cancer seems to be unphosphorylated. Cytoplasmic-expressed TRα2 does not have any prognostic value (see
Supplementary Figures) based on the results that we identified regarding the subcellular expression of TRα1.
Newer investigation showed that TRα1 acts as a new squamous-cell lung cancer diagnostic marker and poor prognosis predictor [
62]. In addition, the TRα1 was the only receptor in a previous study of our group, showing a significant effect on unifocal BC. The Kaplan–Meier curve illustrated a worse DFS for unifocal BC patients when expressing the TRα1 [
42]. In the whole cohort, cytoplasmic expression of TRα1 showed a trend of favorable survival (see
Supplementary Figures), albeit without reaching significance. The same observation can be defined for nuclear expression of TRα1.
The
THRA gene encodes the TRα subtypes TRα1 and TRα2 [
63,
64]. In addition to antibodies detecting both TRα subtypes separately, there are also antibodies that detect TRα more generally [
22]. In a former study, we found that TRα and its isoforms 1 and 2 were associated with different prognoses in ovarian cancer [
22]. Nuclear TRα was associated with a reduced survival rate in clear-cell ovarian cancer, nuclear TRα1 was a positive prognosticator for all subtypes of ovarian cancer, nuclear TRα2 was a positive prognosticator for serous ovarian cancer, cytoplasmic TRα2 was associated with reduced OS in all subtypes, and cytoplasmic TRα1 was only associated with reduced OS in mucinous ovarian cancer [
22].
Within this study, we showed that cytoplasmic-expressed TRα acts as a negative prognosticator for OS and 10-year survival in BC and is an independent negative prognosticator for OS, as analyzed via Cox-regression. Although nuclear TRα showed a trend of being a positive prognosticator in OS, as well as in 10-year survival, differences did not reach a level of significance (see
Supplementary Figures).
To gain further insight into potential individualized targeted treatment of BC, we assessed subcellular TRα expression in the context of clinico-pathological characteristics. Cytoplasmic TRα was significantly correlated with a worse prognosis in BC. Furthermore, nuclear TRα expression in BC tissue tended to be associated with a favorable prognosis, and nuclear expression TRα2 was a significant positive prognostic factor in BC. A more detailed investigation of intracellular localization of TRα and its isoforms 1 and 2 in BC, especially triple-negative breast cancer, that is characterized by worse OS and DFS and increased metastatic potential compared to other major BC subtypes might be of interest, because the identification of reliable predictive biomarkers is fundamental to finding new therapeutic strategies.
This study has some limitations related to its retrospective nature and the way in which TRα-isoforms were assessed. The immuno-histochemical study only allows a semiquantitative analysis. In addition, immunofluorescence techniques would allow a simultaneous investigation of all three TRα-isoforms in one cell. For that approach to take place, antibodies from different species are necessary. On the other hand, complicated immunofluorescence techniques are not easy to transfer to the daily routine pathology, given limited time, technical, and monetary possibilities.
Therefore, our data show that the TRα pathway could represent a promising therapeutic target in BC after additional investigations. The crosstalk between potential NR-ligands, as well as TRα and its isoforms TRα1 and TRα2, in relation to the therapeutic potential of BC should be investigated. Overall, these results demonstrate the complexity of the links between nuclear and cytoplasmic TRα expression and their impact on patient outcomes and emphasize the need for more detailed investigations into intracellular localization of TRα and its isoforms 1 and 2, as well as its interaction with other nuclear receptors in breast carcinoma, in order to understand its biomolecular function and role as a possible biomarker in BC diagnostics.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}