
Assessing the Optimal Regimen: A Systematic Review and Network Meta-Analysis of the Efficacy and Safety of Long-Acting Granulocyte Colony-Stimulating Factors in Patients with Breast Cancer
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Method
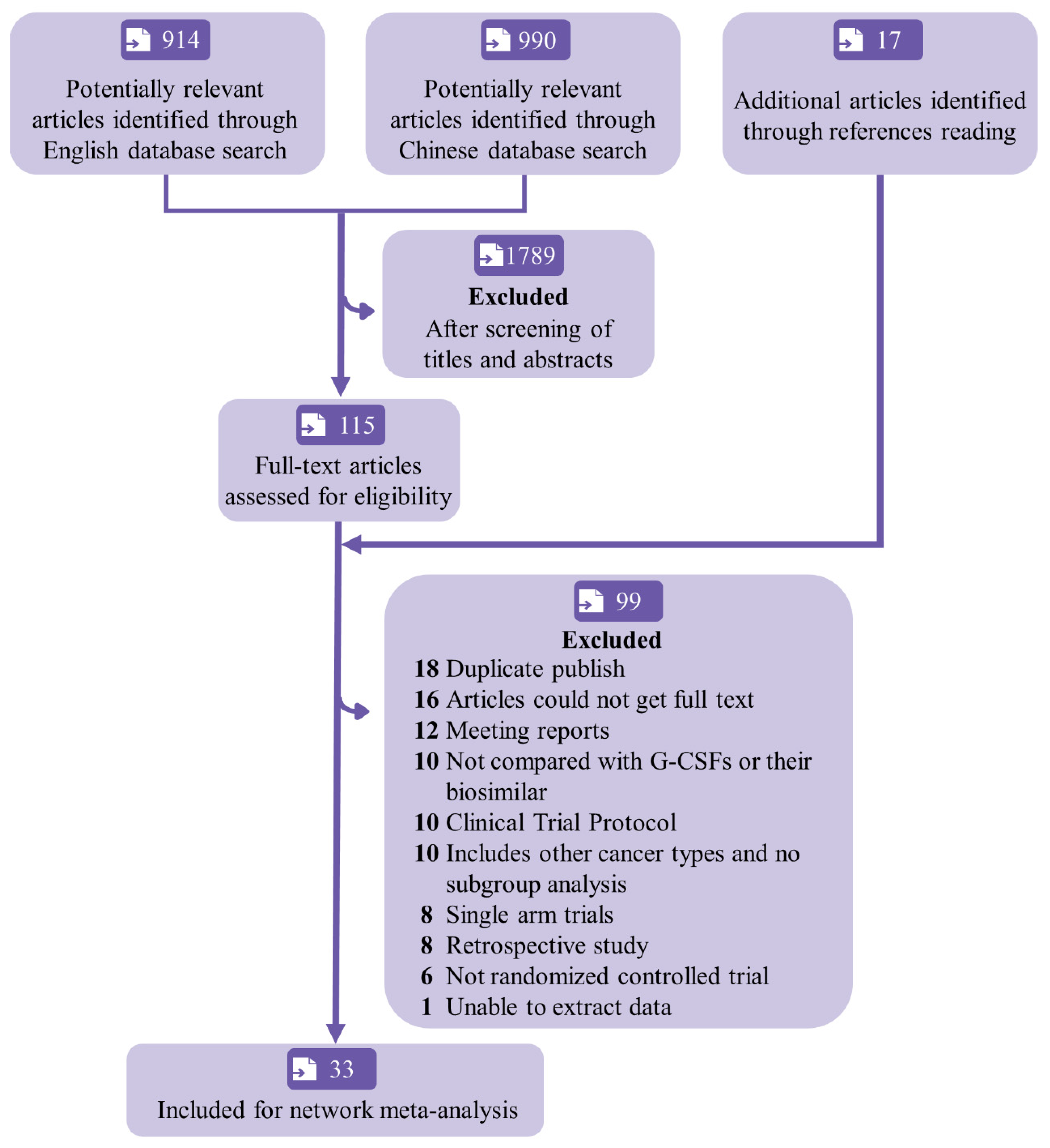
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction and Quality Assessment
2.3. Outcomes
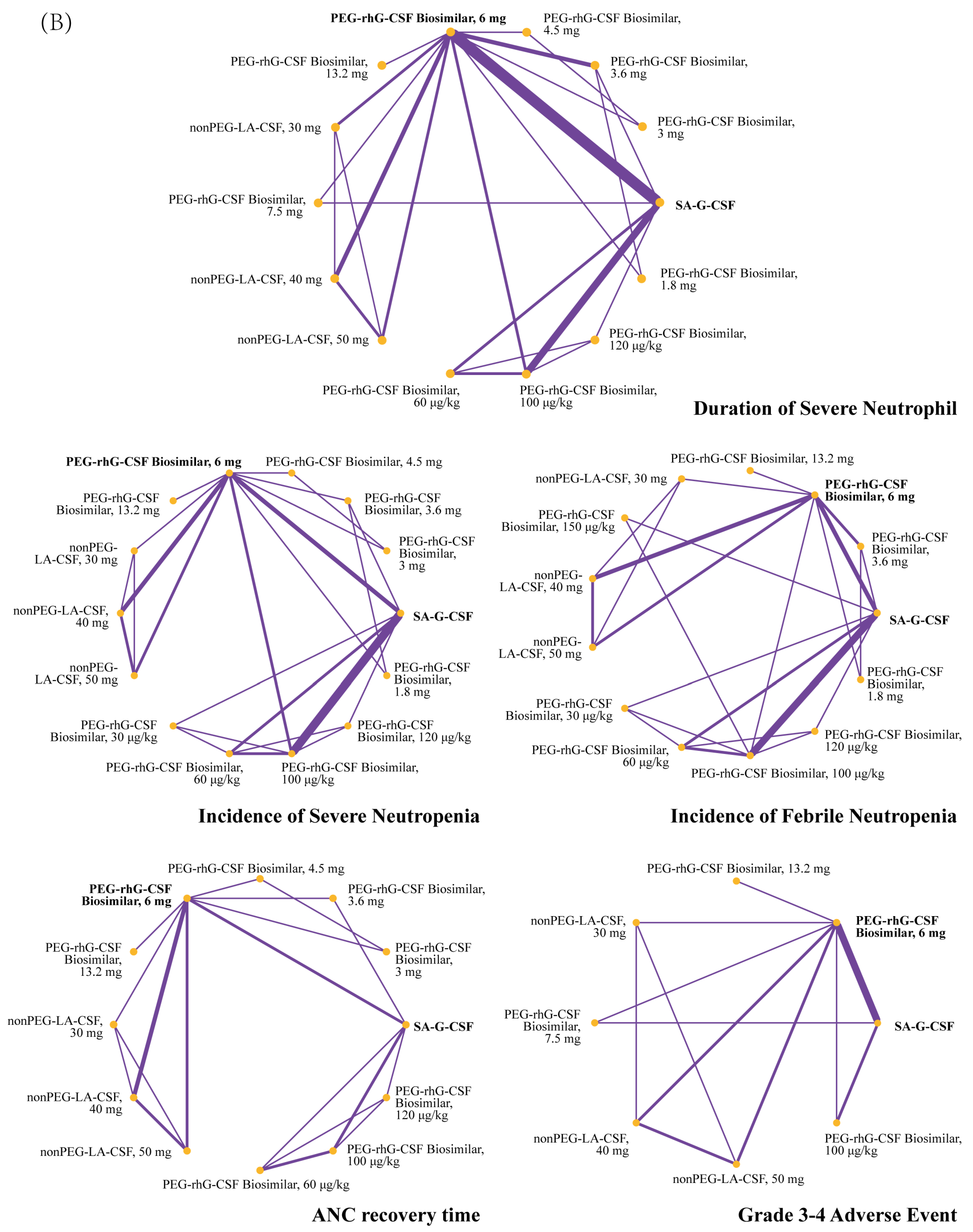
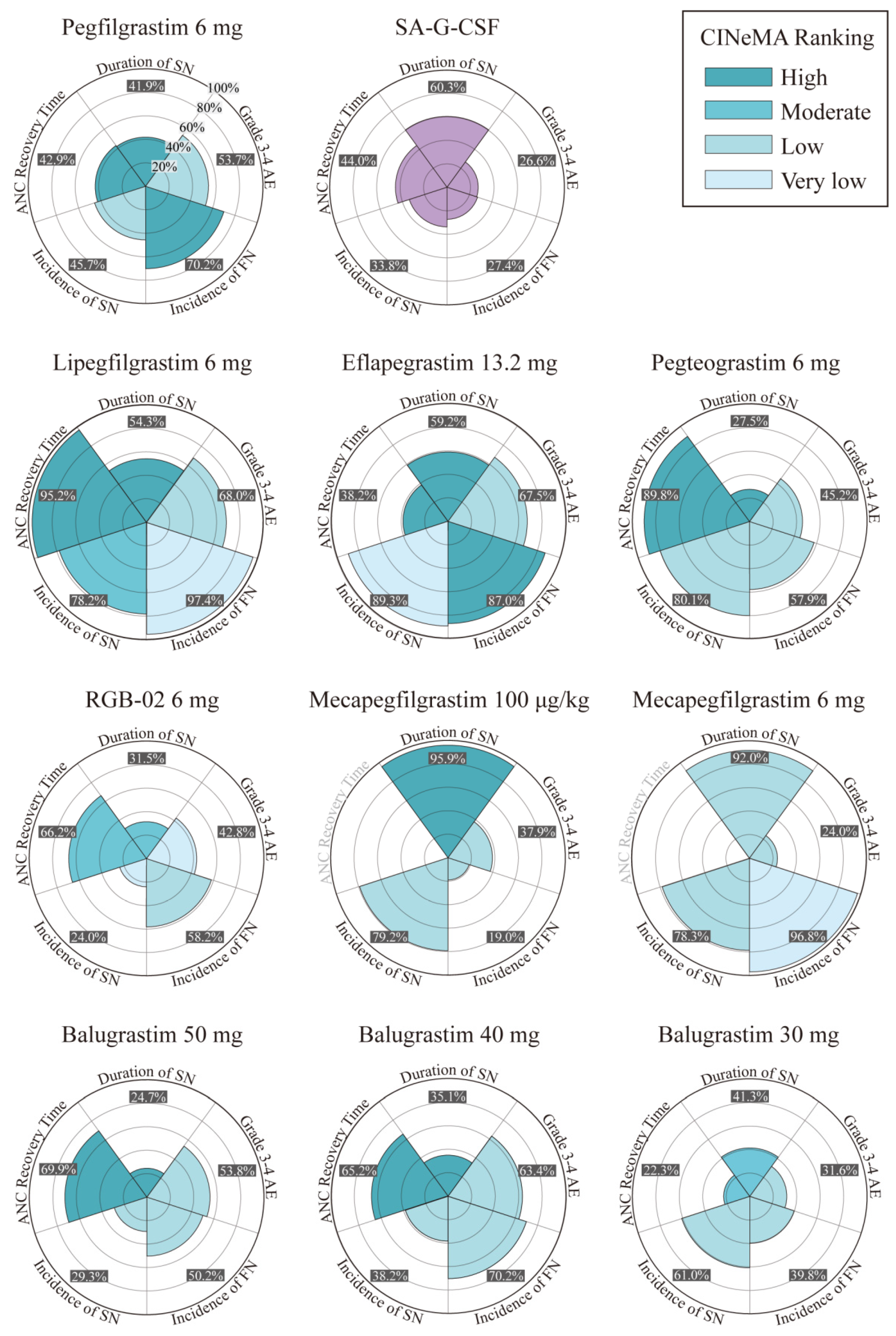
2.4. Data Synthesis and Statistical Analysis
3. Result
3.1. Quality Assessment
3.2. Outcome
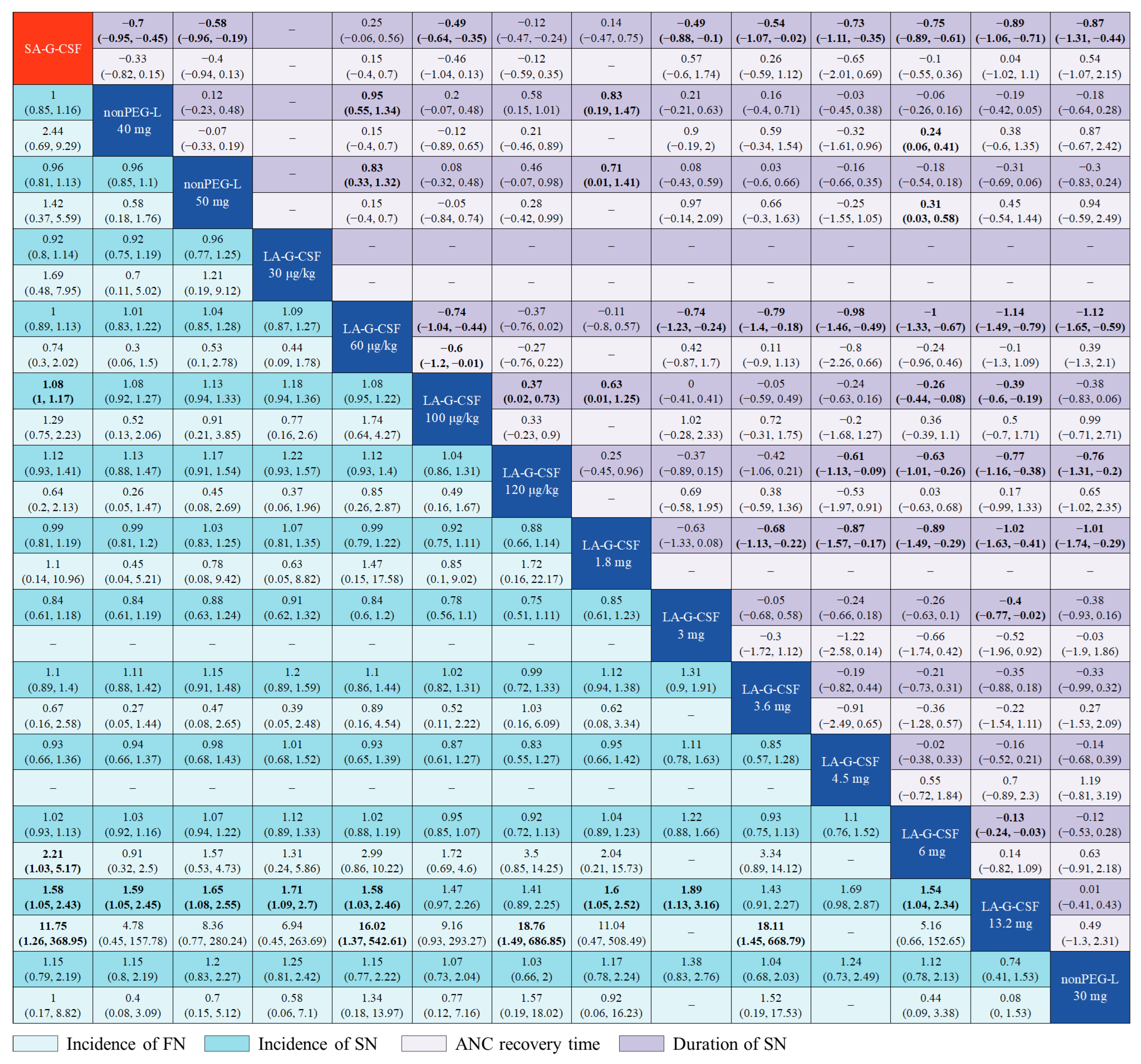
3.2.1. Some LA-G-CSFs Are Statically More Effective Than SA-G-CSF
3.2.2. Varying Efficacy of Different LA-G-CSF Agents
3.2.3. Dose-Based Network Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 691–722. [Google Scholar] [CrossRef]
- Crawford, J.; Dale, D.C.; Kuderer, N.M.; Culakova, E.; Poniewierski, M.S.; Wolff, D.; Lyman, G.H. Risk and Timing of Neutropenic Events in Adult Cancer Patients Receiving Chemotherapy: The Results of a Prospective Nationwide Study of Oncology Practice. J. Natl. Compr. Cancer Netw. 2008, 6, 109–118. [Google Scholar] [CrossRef]
- Caggiano, V.; Weiss, R.V.; Rickert, T.S.; Linde-Zwirble, W.T. Incidence, Cost, and Mortality of Neutropenia Hospitalization Associated with Chemotherapy. Cancer 2005, 103, 1916–1924. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, E.; Iversen, P.O.; Bøyum, A.; Seierstad, T.; Nicolaysen, G.; Benestad, H.B. G-CSF Enhances the Proliferation and Mobilization, but Not the Maturation Rate, of Murine Myeloid Cells. Eur. J. Haematol. 2011, 87, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Ding, P.Q.; Newcomer, B.J.; Cheung, W.Y. Real-World Use of Granulocyte-Colony Stimulating Factor in Patients with Breast Cancer from Alberta, Canada. Cancers 2022, 14, 6197. [Google Scholar] [CrossRef]
- Theyab, A.; Alsharif, K.F.; Alzahrani, K.J.; Oyouni AA, A.; Hawsawi, Y.M.; Algahtani, M.; Alghamdi, S.; Alshammary, A.F. New insight into strategies used to develop long-acting G-CSF biologics for neutropenia therapy. Front. Oncol. 2023, 12, 1026377. [Google Scholar] [CrossRef]
- Welte, K.; Gabrilove, J.; Bronchud, M.H.; Platzer, E.; Morstyn, G. Filgrastim (r-MetHuG-CSF): The First 10 Years. Blood 1996, 88, 1907–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, E.A.; Roy, V.; Alwan, L.; Bachiashvili, K.; Baird, J.; Cool, R.; Dinner, S.; Geyer, M.; Glaspy, J.; Gojo, I.; et al. NCCN Guidelines® Insights: Hematopoietic Growth Factors, Version 1.2022. J. Natl. Compr. Cancer Netw. 2022, 20, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Wu, B.; Hui, X.; Liu, J.; Zhang, T.; Li, F.; Sun, B.; Cai, L.; Li, X.; Chen, Z.; et al. A Randomized Multicenter Phase II Trial of Mecapegfilgrastim Single Administration versus Granulocyte Colony-Stimulating Growth Factor on Treating Chemotherapy-Induced Neutropenia in Breast Cancer Patients. Ann. Transl. Med. 2019, 7, 196. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Cao, J.; Wang, J.F.; Zhang, B.H.; Zeng, X.H.; Zheng, H.; Zhang, Y.; Cai, L.; Wu, Y.D.; Yao, Q.; et al. Advantages with Prophylactic PEG-RhG-CSF versus RhG-CSF in Breast Cancer Patients Receiving Multiple Cycles of Myelosuppressive Chemotherapy: An Open-Label, Randomized, Multicenter Phase III Study. Breast Cancer Res. Treat. 2018, 168, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Zhang, Y.; Miao, Z.; Zeng, X.; Wu, B.; Cai, L.; Liu, J.; Wang, S.; Hu, X.; Zheng, W.; et al. Efficacy and Safety of Mecapegfilgrastim for Prophylaxis of Chemotherapy-Induced Neutropenia in Patients with Breast Cancer: A Randomized, Multicenter, Active-Controlled Phase III Trial. Ann. Transl. Med. 2019, 7, 482. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Huang, W. Clinical Study of Pegylated Recombinant Human Granulocyte Colony-Stimulating Factor in the Treatment of Agranulocytosis after Neoadjuvant Chemotherapy for Breast Cancer. China Pract. Med. 2021, 16, 661. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Cochrane. 2022. Available online: https://training.cochrane.org/handbook (accessed on 20 December 2022).
- Crawford, J.; Dale, D.C.; Lyman, G.H. Chemotherapy-Induced Neutropenia: Risks, Consequences, and New Directions for Its Management. Cancer 2004, 100, 228–237. [Google Scholar] [CrossRef]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. Using the Common Terminology Criteria for Adverse Events (CTCAE-Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. Actas Dermosifiliogr. (Engl. Ed.) 2021, 112, 90–92. [Google Scholar] [CrossRef]
- Caldwell, D.M.; Ades, A.E.; Higgins, J.P.T. Simultaneous Comparison of Multiple Treatments: Combining Direct and Indirect Evidence. BMJ 2005, 331, 897–900. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Sutton, A.J.; Ades, A.E.; Welton, N.J. Evidence Synthesis for Decision Making 2: A Generalized Linear Modeling Framework for Pairwise and Network Meta-Analysis of Randomized Controlled Trials. Med. Decis. Mak. 2013, 33, 607–617. [Google Scholar] [CrossRef] [Green Version]
- Lu, G.; Ades, A.E. Combination of Direct and Indirect Evidence in Mixed Treatment Comparisons. Stat. Med. 2004, 23, 3105–3124. [Google Scholar] [CrossRef]
- Holmes, F.A.; Jones, S.E.; O’Shaughnessy, J.; Vukelja, S.; George, T.; Savin, M.; Richards, D.; Glaspy, J.; Meza, L.; Cohen, G.; et al. Comparable Efficacy and Safety Profiles of Once-per-Cycle Pegfilgrastim and Daily Injection Filgrastim in Chemotherapy-Induced Neutropenia: A Multicenter Dose-Finding Study in Women with Breast Cancer. Ann. Oncol. 2002, 13, 903–909. [Google Scholar] [CrossRef]
- Holmes, F.A.; O’Shaughnessy, J.A.; Vukelja, S.; Jones, S.E.; Shogan, J.; Savin, M.; Glaspy, J.; Moore, M.; Meza, L.; Wiznitzer, I.; et al. Blinded, Randomized, Multicenter Study to Evaluate Single Administration Pegfilgrastim Once per Cycle versus Daily Filgrastim as an Adjunct to Chemotherapy in Patients with High-Risk Stage II or Stage III/IV Breast Cancer. J. Clin. Oncol. 2002, 20, 727–731. [Google Scholar] [CrossRef]
- Green, M.D.; Koelbl, H.; Baselga, J.; Galid, A.; Guillem, V.; Gascon, P.; Siena, S.; Lalisang, R.I.; Samonigg, H.; Clemens, M.R.; et al. A Randomized Double-Blind Multicenter Phase III Study of Fixed-Dose Single-Administration Pegfilgrastim versus Daily Filgrastim in Patients Receiving Myelosuppressive Chemotherapy. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2003, 14, 29–35. [Google Scholar] [CrossRef]
- Vogel, C.L.; Wojtukiewicz, M.Z.; Carroll, R.R.; Tjulandin, S.A.; Barajas-Figueroa, L.J.; Wiens, B.L.; Neumann, T.A.; Schwartzberg, L.S. First and Subsequent Cycle Use of Pegfilgrastim Prevents Febrile Neutropenia in Patients with Breast Cancer: A Multicenter, Double-Blind, Placebo-Controlled Phase III Study. J. Clin. Oncol. 2005, 23, 1178–1184. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Kümmel, S.; Du Bois, A.; Eiermann, W.; Eidtmann, H.; Gerber, B.; Hilfrich, J.; Huober, J.; Costa, S.D.; Jackisch, C.; et al. Pegfilgrastim ± Ciprofloxacin for Primary Prophylaxis with TAC (Docetaxel/Doxorubicin/Cyclophosphamide) Chemotherapy for Breast Cancer. Results from the GEPARTRIO Study. Ann. Oncol. 2008, 19, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Bondarenko, I.; Gladkov, O.A.; Elsaesser, R.; Buchner, A.; Bias, P. Efficacy and Safety of Lipegfilgrastim versus Pegfilgrastim: A Randomized, Multicenter, Active-Control Phase 3 Trial in Patients with Breast Cancer Receiving Doxorubicin/Docetaxel Chemotherapy. BMC Cancer 2013, 13, 386. [Google Scholar] [CrossRef] [PubMed]
- Park, K.H.; Sohn, J.H.; Lee, S.; Park, J.H.; Kang, S.Y.; Kim, H.Y.; Park, I.H.; Park, Y.H.; Im, Y.H.; Lee, H.J.; et al. A Randomized, Multi-Center, Open-Label, Phase II Study of Once-per-Cycle DA-3031, a Biosimilar Pegylated G-CSF, Compared with Daily Filgrastim in Patients Receiving TAC Chemotherapy for Early-Stage Breast Cancer. Investig. New Drugs 2013, 31, 1300–1306. [Google Scholar] [CrossRef] [PubMed]
- Buchner, A.; Elsässer, R.; Bias, P. A Randomized, Double-Blind, Active Control, Multicenter, Dose-Finding Study of Lipegfilgrastim (XM22) in Breast Cancer Patients Receiving Myelosuppressive Therapy. Breast Cancer Res. Treat. 2014, 148, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Volovat, C.; Gladkov, O.A.; Bondarenko, I.M.; Barash, S.; Buchner, A.; Bias, P.; Adar, L.; Avisar, N. Efficacy and Safety of Balugrastim Compared with Pegfilgrastim in Patients with Breast Cancer Receiving Chemotherapy. Clin. Breast Cancer 2014, 14, 101–108. [Google Scholar] [CrossRef]
- Filon, O.; Nechaeva, M.; Burdaeva, O.; Vladimirov, V.I.; Lifirenko, I.; Kovalenko, N.V.; Kopp, M.V.; Matrosova, M.; Mukhametsina, G.; Panchenko, S.; et al. Efficacy and Safety of Empegfilgrastim, a Novel Pegylated G-CSF: Results of Complete Analysis after 4 Cycles of Myelosuppressive Chemotherapy in Phase III Double-Dummy Randomized Clinical Study. J. Clin. Oncol. 2015, 33. [Google Scholar] [CrossRef]
- Gladkov, O.; Moiseyenko, V.; Bondarenko, I.N.; Shparyk, Y.; Barash, S.; Adar, L.; Bias, P.; Avisar, N. Phase II Dose-Finding Study of Balugrastim in Breast Cancer Patients Receiving Myelosuppressive Chemotherapy. Med. Oncol. 2015, 32, 623. [Google Scholar] [CrossRef]
- Kosaka, Y.; Rai, Y.; Masuda, N.; Takano, T.; Saeki, T.; Nakamura, S.; Shimazaki, R.; Ito, Y.; Tokuda, Y.; Tamura, K. Phase III Placebo-Controlled, Double-Blind, Randomized Trial of Pegfilgrastim to Reduce the Risk of Febrile Neutropenia in Breast Cancer Patients Receiving Docetaxel/Cyclophosphamide Chemotherapy. Support. Care Cancer 2015, 23, 1137–1143. [Google Scholar] [CrossRef] [Green Version]
- Masuda, N.; Tokuda, Y.; Nakamura, S.; Shimazaki, R.; Ito, Y.; Tamura, K. Dose Response of Pegfilgrastim in Japanese Breast Cancer Patients Receiving Six Cycles of Docetaxel, Doxorubicin, and Cyclophosphamide Therapy: A Randomized Controlled Trial. Support. Care Cancer 2015, 23, 2891–2898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Jiang, Z.; Wang, L.; Li, C.; Xia, J. An Open-Label, Randomized, Multicenter Dose-Finding Study of Once-per-Cycle Pegfilgrastim versus Daily Filgrastim in Chinese Breast Cancer Patients Receiving TAC Chemotherapy. Med. Oncol. 2015, 32, 147. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, K.; Donskih, R.; Michael Jones, C.; Nixon, A.; Vidal, M.J.; Nakov, R.; Singh, P.; Schaffar, G.; Gascón, P.; Harbeck, N. A Comparison of Proposed Biosimilar LA-EP2006 and Reference Pegfilgrastim for the Prevention of Neutropenia in Patients with Early-Stage Breast Cancer Receiving Myelosuppressive Adjuvant or Neoadjuvant Chemotherapy: Pegfilgrastim Randomized Oncology (Supportive Care) Trial to Evaluate Comparative Treatment (PROTECT-2), a Phase III, Randomized, Double-Blind Trial. Oncologist 2016, 21, 789–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladkov, O.; Moiseyenko, V.; Bondarenko, I.N.; Shparyk, Y.; Barash, S.; Adar, L.; Avisar, N. A Phase III Study of Balugrastim Versus Pegfilgrastim in Breast Cancer Patients Receiving Chemotherapy with Doxorubicin and Docetaxel. Oncologist 2016, 21, 7–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harbeck, N.; Lipatov, O.; Frolova, M.; Udovitsa, D.; Topuzov, E.; Ganea-Motan, D.E.; Nakov, R.; Singh, P.; Rudy, A.; Blackwell, K. Randomized, Double-Blind Study Comparing Proposed Biosimilar LA-EP2006 with Reference Pegfilgrastim in Breast Cancer. Future Oncol. 2016, 12, 1359–1367. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.H.; Kim, J.-Y.; Lee, M.H.; Han, H.S.; Lim, J.H.; Park, K.U.; Park, I.H.; Cho, E.K.; Yoon, S.Y.; Kim, J.H.; et al. A Randomized, Multicenter, Phase II/III Study to Determine the Optimal Dose and to Evaluate the Efficacy and Safety of Pegteograstim (GCPGC) on Chemotherapy-Induced Neutropenia Compared to Pegfilgrastim in Breast Cancer Patients: KCSG PC10-09. Support Care Cancer 2016, 24, 1709–1717. [Google Scholar] [CrossRef] [Green Version]
- Harbeck, N.; Gascon, P.; Jones, C.M.; Nixon, A.; Krendyukov, A.; Nakov, R.; Mo, M.; Blackwell, K.L. Proposed Biosimilar Pegfilgrastim (LA-EP2006) Compared with Reference Pegfilgrastim in Asian Patients with Breast Cancer Receiving Myelotoxic Chemotherapy: Pooled Subgroup Analysis of Two Randomized Trials. Ann. Oncol. 2017, 13, 1385–1393. [Google Scholar] [CrossRef] [Green Version]
- Park, K.H.; Lee, S.; Park, J.H.; Kang, S.Y.; Kim, H.Y.; Park, I.H.; Park, Y.H.; Im, Y.H.; Lee, H.J.; Park, S.; et al. A Randomized, Multi-Center, Open-Label, Phase III Study of Once-per-Cycle DA-3031, a Pegylated G-CSF, in Comparison with Daily Filgrastim in Patients Receiving TAC Chemotherapy for Breast Cancer. Support. Care Cancer 2017, 25, 505–511. [Google Scholar] [CrossRef]
- Wu, D.; Zhang, H.; Wang, B. Effect of PEG-rhG-CSF injection on the prevention and treatment of neutropenia induced by postoperative chemotherapy in breast cancer. J. Chongqing Med. 2018, 47, 546–548. [Google Scholar] [CrossRef]
- Ashrafi, F.; Salmasi, M. Comparison of the Effects of Pegylated Granulocyte-Colony Stimulating Factor and Granulocyte-Colony Stimulating Factor on Cytopenia Induced by Dose-Dense Chemotherapy in Breast Cancer Patients. J. Res. Med. Sci. 2018, 23, 73. [Google Scholar] [CrossRef] [PubMed]
- Desai, K.; Misra, P.; Kher, S.; Shah, N. Clinical Confirmation to Demonstrate Similarity for a Biosimilar Pegfilgrastim: A 3-Way Randomized Equivalence Study for a Proposed Biosimilar Pegfilgrastim versus US-Licensed and EU-Approved Reference Products in Breast Cancer Patients Receiving Myelosuppressive Chemotherapy. Exp. Hematol. Oncol. 2018, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Liu, J.; Zeng, Y.; Wu, F.; Li, N.; Chen, K.; Hong, Y.; Wang, L.; Zhen, H.; Lin, L. Randomized Controlled Clinical Trial of Polyethylene Glycol Recombinant Human Granulocyte Colony-Stimulating Factor in the Treatment of Neutropenia after Chemotherapy for Breast Cancer. Cancer Chemother. Pharmacol. 2018, 82, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Kahan, K.; Grecea, D.; Smakal, M.; Illes, A.; Kahan, Z. Efficacy and Safety of RGB-02, a Proposed Biosimilar Pegfilgrastim to Prevent Chemotherapy-Induced Neutropenia: Results of a Randomized, Double-Blind, Phase III Clinical Study vs. Reference Pegfilgrastim in Patients with Breast Cancer Receiving Docetaxel/Doxorubicin. Ann. Oncol. 2019, 28, v555. [Google Scholar]
- Waller, C.F.; Ranganna, G.M.; Pennella, E.J.; Blakeley, C.; Bronchud, M.H.; Mattano, L.A.; Berzoy, O.; Voitko, N.; Shparyk, Y.; Lytvyn, I.; et al. Randomized Phase 3 Efficacy and Safety Trial of Proposed Pegfilgrastim Biosimilar MYL-1401H in the Prophylactic Treatment of Chemotherapy-Induced Neutropenia. Ann. Hematol. 2019, 98, 1217–1224. [Google Scholar] [CrossRef]
- Cobb, P.W.; Moon, Y.W.; Mezei, K.; Láng, I.; Bhat, G.; Chawla, S.; Hasal, S.J.; Schwartzberg, L.S. A Comparison of Eflapegrastim to Pegfilgrastim in the Management of Chemotherapy-Induced Neutropenia in Patients with Early-Stage Breast Cancer Undergoing Cytotoxic Chemotherapy (RECOVER): A Phase 3 Study. Cancer Med. 2020, 9, 6234–6243. [Google Scholar] [CrossRef]
- Schwartzberg, L.S.; Bhat, G.; Peguero, J.; Agajanian, R.; Bharadwaj, J.S.; Restrepo, A.; Hlalah, O.; Mehmi, I.; Chawla, S.; Hasal, S.J.; et al. Eflapegrastim, a Long-Acting Granulocyte-Colony Stimulating Factor for the Management of Chemotherapy-Induced Neutropenia: Results of a Phase III Trial. Oncologist 2020, 25, e1233–e1241. [Google Scholar] [CrossRef]
- Sohn, B.S.; Jeong, J.H.; Ahn, J.H.; Jung, K.H.; Kim, J.E.; Sohn, J.H.; Koh, S.J.; Seo, J.H.; Lee, K.S.; Kim, S.B. A Pilot Study on Intermittent Every Other Days of 5-Dose Filgrastim Compared with Single Pegfilgrastim in Breast Cancer Patients Receiving Adjuvant Docetaxel, Doxorubicin, and Cyclophosphamide (TAC) Chemotherapy. Investig. New Drugs 2020, 38, 866–873. [Google Scholar] [CrossRef]
- Smith, T.J.; Bohlke, K.; Lyman, G.H.; Carson, K.R.; Crawford, J.; Cross, S.J.; Goldberg, J.M.; Khatcheressian, J.L.; Leighl, N.B.; Perkins, C.L.; et al. Recommendations for the Use of WBC Growth Factors: American Society of Clinical Oncology Clinical Practice Guideline Update. JCO 2015, 33, 3199–3212. [Google Scholar] [CrossRef] [Green Version]
- Crawford, J.; Caserta, C.; Roila, F. Hematopoietic Growth Factors: ESMO Clinical Practice Guidelines for the Applications. Ann. Oncol. 2010, 21, v248–v251. [Google Scholar] [CrossRef]
- Li, X.; Zheng, H.; Yu, M.-C.; Wang, W.; Wu, X.-H.; Yang, D.-M.; Xu, J. Is PEGylated G-CSF Superior to G-CSF in Patients with Breast Cancer Receiving Chemotherapy? A Systematic Review and Meta-Analysis. Support. Care Cancer 2020, 28, 5085–5097. [Google Scholar] [CrossRef] [PubMed]
- Cornes, P.; Gascon, P.; Vulto, A.G.; Aapro, M. Biosimilar Pegfilgrastim: Improving Access and Optimising Practice to Supportive Care That Enables Cure. BioDrugs Clin. Immunother. Biopharm. Gene Ther. 2020, 34, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, J.; Ozer, H.; Stoller, R.; Johnson, D.; Lyman, G.; Tabbara, I.; Kris, M.; Grous, J.; Picozzi, V.; Rausch, G.; et al. Reduction by Granulocyte Colony-Stimulating Factor of Fever and Neutropenia Induced by Chemotherapy in Patients with Small-Cell Lung Cancer. N. Engl. J. Med. 1991, 325, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Molineux, G. The Design and Development of Pegfilgrastim (PEG-RmetHuG-CSF, Neulasta). Curr. Pharm. Des. 2004, 10, 1235–1244. [Google Scholar] [CrossRef]
- Hoggatt, J.; Pelus, L.M. New G-CSF Agonists for Neutropenia Therapy. Expert Opin. Investig. Drugs 2014, 23, 21–35. [Google Scholar] [CrossRef]
- Hoggatt, J.; Tate, T.A.; Pelus, L.M. Role of Lipegfilgrastim in the Management of Chemotherapy-Induced Neutropenia. Int. J. Nanomed. 2015, 10, 2647–2652. [Google Scholar] [CrossRef] [Green Version]
- Aapro, M.S.; Bohlius, J.; Cameron, D.A.; Lago, L.D.; Donnelly, J.P.; Kearney, N.; Lyman, G.H.; Pettengell, R.; Tjan-Heijnen, V.C.; Walewski, J.; et al. 2010 Update of EORTC Guidelines for the Use of Granulocyte-Colony Stimulating Factor to Reduce the Incidence of Chemotherapy-Induced Febrile Neutropenia in Adult Patients with Lymphoproliferative Disorders and Solid Tumours. Eur. J. Cancer 2011, 47, 8–32. [Google Scholar] [CrossRef]
- Aapro, M.S.; Cameron, D.A.; Pettengell, R.; Bohlius, J.; Crawford, J.; Ellis, M.; Kearney, N.; Lyman, G.H.; Tjan-Heijnen, V.C.; Walewski, J.; et al. EORTC Guidelines for the Use of Granulocyte-Colony Stimulating Factor to Reduce the Incidence of Chemotherapy-Induced Febrile Neutropenia in Adult Patients with Lymphomas and Solid Tumours. Eur. J. Cancer 2006, 42, 2433–2453. [Google Scholar] [CrossRef]
- Mahlert, F.; Schmidt, K.; Allgaier, H.; Liu, P.; Mueller, U.; Shen, W.D. Rational Development of Lipegfilgrastim a Novel Long-Acting Granulocyte Colony-Stimulating Factor, Using Glycopegylation Technology. Blood 2013, 122, 4853. [Google Scholar] [CrossRef]
- Gasparic, M.; Leyman, S. Review on Lipegfilgrastim. Int. J. Nanomed. 2015, 10, 6863–6864. [Google Scholar] [CrossRef] [Green Version]
- Barnes, G.; Pathak, A.; Schwartzberg, L. G-CSF Utilization Rate and Prescribing Patterns in United States: Associations between Physician and Patient Factors and GCSF Use. Cancer Med. 2014, 3, 1477–1484. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.C.; Demetri, G.D.; Berry, D.A.; Norton, L.; Broadwater, G.; Robert, N.J.; Duggan, D.; Hayes, D.F.; Henderson, I.C.; Lyss, A.; et al. Dose-Escalation of Filgrastim Does Not Improve Efficacy: Clinical Tolerability and Long-Term Follow-up on CALGB Study 9141 Adjuvant Chemotherapy for Node-Positive Breast Cancer Patients Using Dose-Intensified Doxorubicin plus Cyclophosphamide Followed by Paclitaxel. Cancer Treat. Rev. 2008, 34, 223–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dufour, C.; Cappelli, B.; Calvillo, M.; Fioredda, F.; Tonelli, R.; Crocchiolo, R. Similar Favorable Outcome of Pegfilgrastim Overdose in Patients with Different Age and Underlying Disease. Haematologica 2010, 95, 684–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Study ID | Region | Type of Intervention and Dose | Initiation Time of the G-CSF | Number of Patients | Age (Mean, SD) | Chemotherapy Regimen |
|---|---|---|---|---|---|---|---|
| 1 | Holmes et al., study 1, 2002 [21] | USA | SA-G-CSF | 24 h post-chemotherapy and continued (1) for 14 days, or (2) until the ANC reached 10 × 109/L post-ANC nadir. | 25 | 50, 9 | AT (60/75, 4 cycles) |
| Pegfilgrastim, 30 μg/kg | 24 h post-chemotherapy | 19 | 51, 13 | ||||
| Pegfilgrastim, 60 μg/kg | 24 h post-chemotherapy | 60 | 51, 11 | ||||
| Pegfilgrastim, 100 μg/kg | 24 h post-chemotherapy | 46 | 49, 11 | ||||
| 2 | Holmes et al., study 2, 2002 [22] | Multi | SA-G-CSF | 24 h post-chemotherapy and continued (1) for 14 days, or (2) until the ANC reached 10 × 109/L post-ANC nadir. | 149 | 50.9, 11.7 | AT (60/75, 4 cycles) |
| Pegfilgrastim, 100 μg/kg | 24 h post-chemotherapy | 147 | 51.9, 11.1 | ||||
| 3 | Green et al., 2003 [23] | Multi | SA-G-CSF | ≥24 h post-chemotherapy, continued daily until (1) an ANC ≥ 10.0 × 109/L was documented after the expected nadir or (2) for a maximum of 14 days. | 75 | 52.8, 11.5 | AT (60/75, 4 cycles) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 77 | 52.1, 9.2 | ||||
| 4 | Vogel et al., 2005 [24] | Multi | Placebo | 24 h post-chemotherapy | 465 | 52.1, 8.7 | T (100, 4 cycles) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 463 | 51.9, 11.2 | ||||
| 5 | Minckwitz et al., 2008 [25] | German | filgrastim 5 ug/kg/day or lenograstim 150 ug/m2/day | 24 h post-chemotherapy | 377 | - | TAC (75/50/500, 6 cycles) |
| pegfilgrastim 6.0 mg | 24 h post-chemotherapy | 305 | - | ||||
| 6 | Bondarenko et al., 2013 [26] | Multi | Lipegfilgrastim, 6 mg | 24 h post-chemotherapy | 94 | 49.3, 10.0 | AT (60/75, 4 cycles) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 94 | 50.9, 9.3 | ||||
| 7 | Park et al., 2013 [27] | Korea | SA-G-CSF | 24 h after chemotherapy and continued until (1) documented ANC 5 × 109/L after nadir, or (2) up to 10 days. | 21 | 45.29, 6.13 | TAC (70/75/500, 6 cycles) |
| DA-3031, 3.6 mg | 24 h post-chemotherapy | 20 | 42.50, 5.62 | ||||
| DA-3031, 6 mg | 24 h post-chemotherapy | 20 | 46.95, 9.19 | ||||
| 8 | Volovat et al., 2014 [29] | Multi | Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 151 | 50.8, 9.65 | AT (60/75, 4 cycles) |
| Balugrastim, 40 mg | 24 h post-chemotherapy | 153 | 51.5, 10.28 | ||||
| 9 | Buchner et al., 2014 [28] | Multi | Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 54 | 49.5, 11.1 | AT (60/75, 4 cycles) |
| Lipegfilgrastim, 3 mg | 24 h post-chemotherapy | 53 | 53.1, 9.2 | ||||
| Lipegfilgrastim, 4.5 mg | 24 h post-chemotherapy | 51 | 52.8, 10.1 | ||||
| Lipegfilgrastim, 6 mg | 24 h post-chemotherapy | 50 | 51.4, 9.8 | ||||
| 10 | Filon et al., 2015 [30] | Russia | SA-G-CSF | 24 h post-chemotherapy, until (1) ANC reached 10,000/μL or (2) for 14 days. | 43 | 51.86, 9.68 | AT (60/75, 4 cycles) |
| Empegfilgrastim, 6 mg | 24 h post-chemotherapy | 42 | 50.42, 9.19 | ||||
| Empegfilgrastim, 7.5 mg | 24 h post-chemotherapy | 43 | 48.38, 1.07 | ||||
| 11 | Gladkov et al., 2015 [31] | Multi | Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 25 | 52.8, 10.4 | AT (60/75, 4 cycles) |
| Balugrastim, 30 mg | 24 h post-chemotherapy | 10 | 56.9, 9.5 | ||||
| Balugrastim, 40 mg | 24 h post-chemotherapy | 21 | 51.4, 10.3 | ||||
| Balugrastim, 50 mg | 24 h post-chemotherapy | 20 | 53.8, 9.5 | ||||
| 12 | Kosaka et al., 2015 [32] | Japan | Placebo, 3.6 mg | 24 h post-chemotherapy | 173 | 49.8, 7.8 | TC (75/600, 4–6 cycles) |
| Pegfilgrastim, 3.6 mg | 24 h post-chemotherapy | 173 | 50.7, 8.0 | ||||
| 13 | Lee et al., 2016 [38] | South Korea | Pegteograstim 6.0 mg | 24 h post-chemotherapy | 57 | 49,10.5 | TAC (75/50/500, 6 cycles) |
| Pegfilgrastim 6.0 mg | 24 h post-chemotherapy | 59 | 49,11 | ||||
| 14 | Masuda et al., 2015 [33] | Japan | Pegfilgrastim, 1.8 mg | 24 h post-chemotherapy | 29 | 46.5, 7.4 | TAC (70/75/500, 6 cycles) |
| Pegfilgrastim, 3.6 mg | 24 h post-chemotherapy | 29 | 46.5, 9.4 | ||||
| Pegfilgrastim, 6.0 mg | 24 h post-chemotherapy | 29 | 47.3, 9.4 | ||||
| 15 | Zhang et al., 2015 [34] | China | SA-G-CSF | 48 h post-chemotherapy, continued either for 14 days or until the ANC reached 109/L post-ANC nadir, whichever occurred first, but for at least 7 days. | 43 | 47.35, 8.14 | TAC (70/75/500, 6 cycles) |
| Pegfilgrastim, 60 μg/kg | 48 h post-chemotherapy | 43 | 47.03, 7.66 | ||||
| Pegfilgrastim, 100 μg/kg | 48 h post-chemotherapy | 43 | 48.1, 8.09 | ||||
| Pegfilgrastim, 120 μg/kg | 48 h post-chemotherapy | 42 | 46.71, 6.80 | ||||
| 16 | Blackwell et al., 2016 [35] | Multi | Pegfilgrastim, 6.0 mg | 24 h post-chemotherapy | 153 | 49.1, 10.07 | TAC (70/75/500, 6 cycles or more) |
| LA-EP2006, 6.0 mg | 24 h post-chemotherapy | 155 | 48.8, 10.5 | ||||
| 17 | Gladkov et al., 2016 [36] | Multi | Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 86 | 50.3, 9.1 | AT (60/75, 4 cycles) |
| Balugrastim, 40 mg | 24 h post-chemotherapy | 85 | 49.2, 9.9 | ||||
| Balugrastim, 50 mg | 24 h post-chemotherapy | 84 | 49.8, 9.6 | ||||
| 18 | Harbeck et al., 2016 [37] | Multi | LA-EP2006, 6 mg | 24 h post-chemotherapy | 159 | 49.9, 9.5 | TAC (70/75/500, 6 cycles) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 157 | 50.5, 10.9 | ||||
| 19 | Harbeck et al., 2017 [39] | Multi | LA-EP2006, 6 mg | 24 h post-chemotherapy | 90 | 47.8, 10.42 | TAC (70/75/500, 6 cycles) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 84 | 47.4, 9.53 | ||||
| 20 | Park et al., 2017 [40] | Korean | SA-G-CSF | 24 h post-chemotherapy and continued until (1) ANC was documented to be 5 × 109/L after nadir, or (2) for up to 10 days | 38 | 45.76, 8.12 | TAC (75/50/500, 6 cycles) |
| DA-3031, 6 mg | 24 h post-chemotherapy | 36 | 47.11, 6.37 | ||||
| 21 | Ashrafi et al., 2018 [42] | Iran | SA-G-CSF | 24 h post-chemotherapy | 12 | 45.3, 10.5 | AC-T (60/600/80) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 12 | 45.3, 10.5 | ||||
| 22 | Desai et al., 2018 [43] | Multi | APO-Peg, 6 mg | 24 h post-chemotherapy | 294 | 51.9, 10.0 | TAC (75/50/500, 6 cycles) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 295 | 51.4, 10.3 | ||||
| 23 | Huang et al., 2018 [44] | China | SA-G-CSF | 48 h post-chemotherapy, continued for 14 days or until the ANC became ≥ 10 × 109/L. | 22 | 47.5, 7 | AC (60/600, 4 cycles) |
| Jin You Li, 100 μg/kg | 48 h post-chemotherapy | 24 | 46.5, 6.75 | ||||
| 24 | Wu et al., 2018 [41] | China | SA-G-CSF | 48 h post-chemotherapy, continued until (1) a documented ANC ≥ 5.0×109/L twice post-ANC nadir; (2) for up to 14 days. | 44 | 59.25, 6.79 | EC-T (100/600/100, 4 cycles) |
| Xinruibai, 100 μg/kg | 48 h post-chemotherapy | 45 | 52.36, 5.48 | ||||
| 25 | Xie et al., 2018 [11] | China | SA-G-CSF | 48 h post-chemotherapy, and continued daily until (1) an ANC ≥ 5.0 × 109/L or (2) for a maximum of 14 days. | 194 | 49.22, 9.24 | EC (100/600, 4 cycles) or TC (75/75, 4 cycles) or ET (600/75, 4 cycles) |
| Shenlida, 100 µg/kg | 48 h post-chemotherapy | 187 | 47.12, 8.81 | ||||
| Shenlida, 6 mg | 48 h post-chemotherapy | 188 | 49.40, 8.84 | ||||
| 26 | Kahan et al., 2019 [45] | Multi | RGB-02, 6 mg | 24 h post-chemotherapy | 121 | 51.0, 8.20 | AT (60/75, 4 cycles) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 118 | 51.2, 9.56 | ||||
| 27 | Sohn et al., 2019 [49] | Korea | SA-G-CSF | On D3, D5, D7, D9, and D11 of each cycle | 11 | 55, 3.8 | TAC (75/50/500, 6 cycles) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 11 | 50.6, 10.0 | ||||
| 28 | Waller et al., 2019 [46] | Multi | MYL-1401H, 6 mg | 24 h post-chemotherapy | 127 | 50, 11 | TAC (75/50/500, 6 cycles) |
| Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 67 | 50, 10 | ||||
| 29 | Wang et al., 2019 [10] | China | SA-G-CSF | 48 h post-chemotherapy and continued (1) for 14 days; (2) until ANC ≥ 5.0 × 109/L in two consecutive examinations after ANC reached the lowest point; (3) until ANC ≥ 15×109/L. | 61 | 47.84, 8.67 | AT (75/75, 4 cycles) or AC (100/600, 4 cycles) |
| HHPG-19K, 100 μg/kg | 48 h post-chemotherapy | 60 | 47.58, 8.88 | ||||
| HHPG-19, 150 μg/kg | 48 h post-chemotherapy | 61 | 48.97, 8.59 | ||||
| 30 | Xu et al., 2019 [12] | China | SA-G-CSF | 48 h post-chemotherapy, continued (1) until a documented ANC ≥ 5.0×109/L twice; (2) until ANC ≥ 15×109/L once after the expected nadir; (3) for up to 14 days. | 111 | 48.21, 8.55 | AT (75/75, 4 cycles) or AC (100/600, 4 cycles) |
| Mecapegfilgrastim (HHPG-19K), 6 mg | 48 h post-chemotherapy | 110 | 47.37, 8.60 | ||||
| Mecapegfilgrastim (HHPG-19K), 100 μg/kg | 48 h post-chemotherapy | 110 | 48.03, 9.01 | ||||
| 31 | Cobb et al., 2020 [47] | Multi | Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 119 | 59.2, 10.5 | TC (75/600, 4 cycles) |
| Eflapegrastim, 13.2 mg | 24 h post-chemotherapy | 118 | 57.6, 10 | ||||
| 32 | Schwartzberg et al., 2020 [48] | USA | Pegfilgrastim, 6 mg | 24 h post-chemotherapy | 210 | 59.59, 10.91 | TC (75/600, 4 cycles) |
| EflaPegrastim, 13.2 mg | 24 h post-chemotherapy | 196 | 60.61, 10.08 | ||||
| 33 | Liang et al., 2021 [13] | China | SA-G-CSF | 24 h post-chemotherapy and continued for 3 days | 20 | 64.79, 6.34 | not clear |
| Jin You Li, 6 mg | 24 h post-chemotherapy | 20 | 64.45, 5.87 |
| Dose | Outcome | ||||
|---|---|---|---|---|---|
| DSN | Incidence of SN | Incidence of FN | ANC Recovery Time | Grade 3–4 AE | |
| SA-G-CSF | 14.6% | 42.4% | 38.7% | 41.4% | 49.7% |
| LA-G-CSF biosimilar 6 mg | 74.3% | 53.0% | 74.9% | 48.4% | 44.5% |
| LA-G-CSF biosimilar 13.2 mg | 91.4% | 96.4% | 95.5% | 42.8% | 30.0% |
| LA-G-CSF biosimilar 7.5 mg | 66.9% | - | - | - | 89.1% |
| LA-G-CSF biosimilar 4.5 mg | 71.1% | 33.6% | - | 78.8% | - |
| LA-G-CSF biosimilar 3.6 mg | 52.5% | 70.4% | 25.9% | 29.0% | - |
| LA-G-CSF biosimilar 3 mg | 45.4% | 15.2% | - | 17.7% | - |
| LA-G-CSF biosimilar 1.8 mg | 10.2% | 39.5% | 46.0% | - | - |
| LA-G-CSF biosimilar 150 μg/kg | - | - | 31.1% | - | |
| LA-G-CSF biosimilar 120 μg/kg | 21.2% | 72.7% | 23.5% | 54.7% | - |
| LA-G-CSF biosimilar 100 μg/kg | 43.6% | 69.5% | 52.9% | 79.4% | 80.5% |
| LA-G-CSF biosimilar 60 μg/kg | 3.6% | 43.1% | 27.8% | 31.8% | - |
| LA-G-CSF biosimilar 30 μg/kg | - | 23.0% | 62.0% | - | - |
| non-PEG-LA-CSF 50 mg | 53.7% | 30.5% | 53.6% | 78.9% | 47.9% |
| non-PEG-LA-CSF 40 mg | 67.2% | 42.7% | 76.1% | 72.8% | 62.8% |
| non-PEG-LA-CSF 30 mg | 84.3% | 68.0% | 41.8% | 24.3% | 15.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
You, Z.; Zhang, H.; Huang, Y.; Zhao, L.; Tu, H.; Zhang, Y.; Lin, X.; Liang, W. Assessing the Optimal Regimen: A Systematic Review and Network Meta-Analysis of the Efficacy and Safety of Long-Acting Granulocyte Colony-Stimulating Factors in Patients with Breast Cancer. Cancers 2023, 15, 3675. https://doi.org/10.3390/cancers15143675
You Z, Zhang H, Huang Y, Zhao L, Tu H, Zhang Y, Lin X, Liang W. Assessing the Optimal Regimen: A Systematic Review and Network Meta-Analysis of the Efficacy and Safety of Long-Acting Granulocyte Colony-Stimulating Factors in Patients with Breast Cancer. Cancers. 2023; 15(14):3675. https://doi.org/10.3390/cancers15143675
Chicago/Turabian StyleYou, Zhixuan, Haotian Zhang, Yining Huang, Lei Zhao, Hengjia Tu, Yuzhuo Zhang, Xinqing Lin, and Wenhua Liang. 2023. "Assessing the Optimal Regimen: A Systematic Review and Network Meta-Analysis of the Efficacy and Safety of Long-Acting Granulocyte Colony-Stimulating Factors in Patients with Breast Cancer" Cancers 15, no. 14: 3675. https://doi.org/10.3390/cancers15143675
APA StyleYou, Z., Zhang, H., Huang, Y., Zhao, L., Tu, H., Zhang, Y., Lin, X., & Liang, W. (2023). Assessing the Optimal Regimen: A Systematic Review and Network Meta-Analysis of the Efficacy and Safety of Long-Acting Granulocyte Colony-Stimulating Factors in Patients with Breast Cancer. Cancers, 15(14), 3675. https://doi.org/10.3390/cancers15143675