
Morphine Analgesia, Cannabinoid Receptor 2, and Opioid Growth Factor Receptor Cancer Tissue Expression Improve Survival after Pancreatic Cancer Surgery

 ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
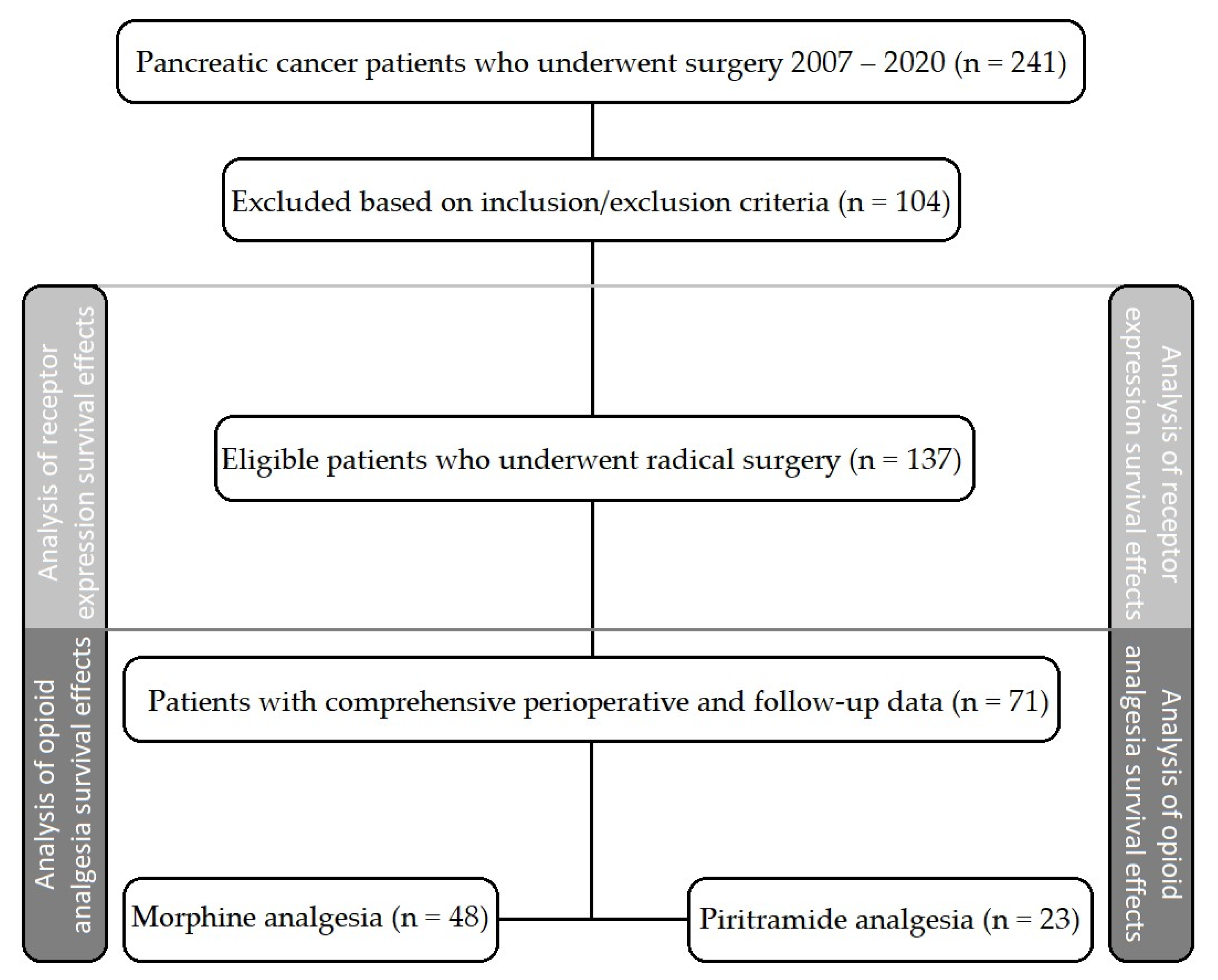
2. Materials and Methods
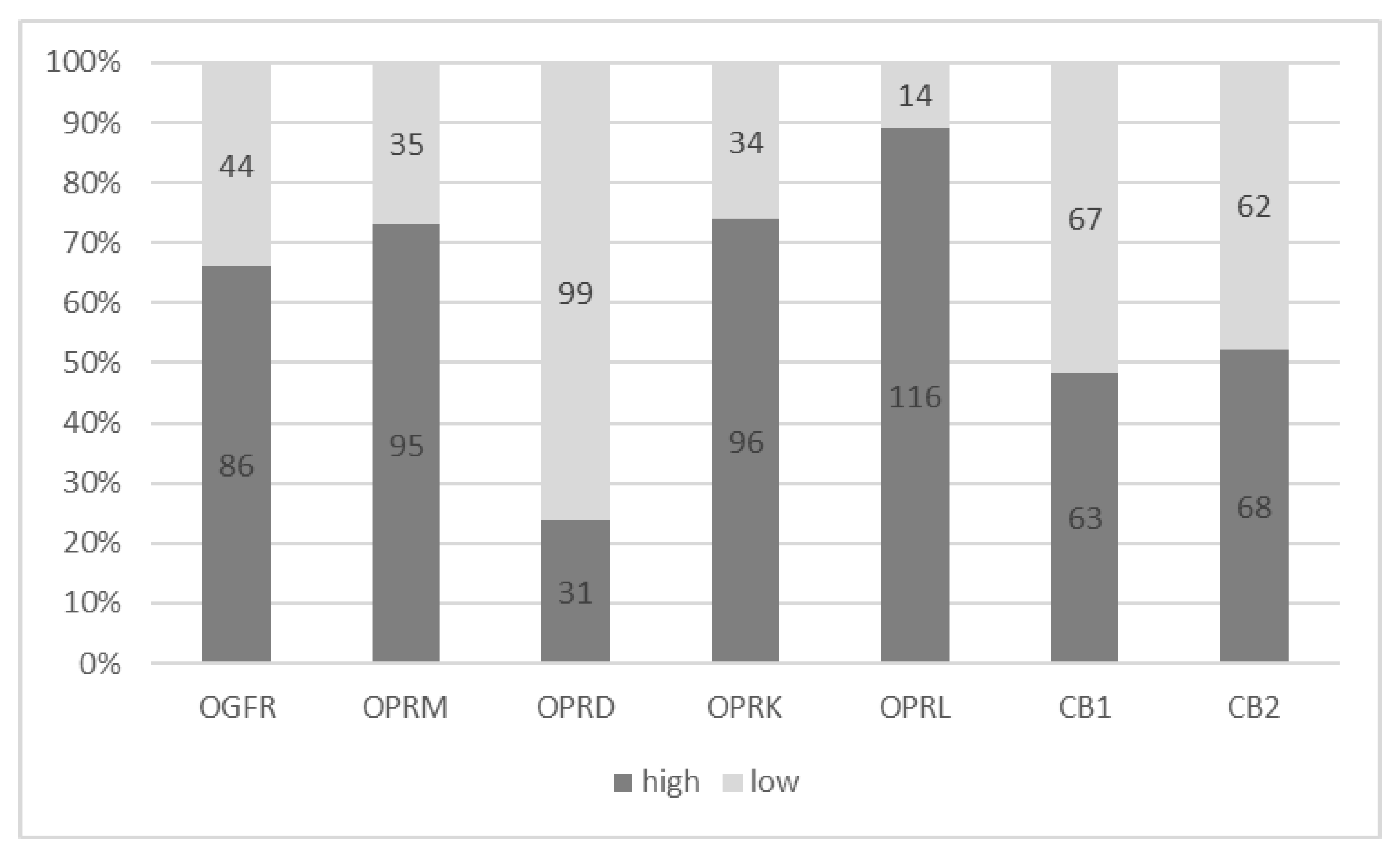
2.1. Analysis of Opioid and/or Cannabinoid Receptor Expression in Tumor Tissues
2.2. Statistical Analysis
3. Results
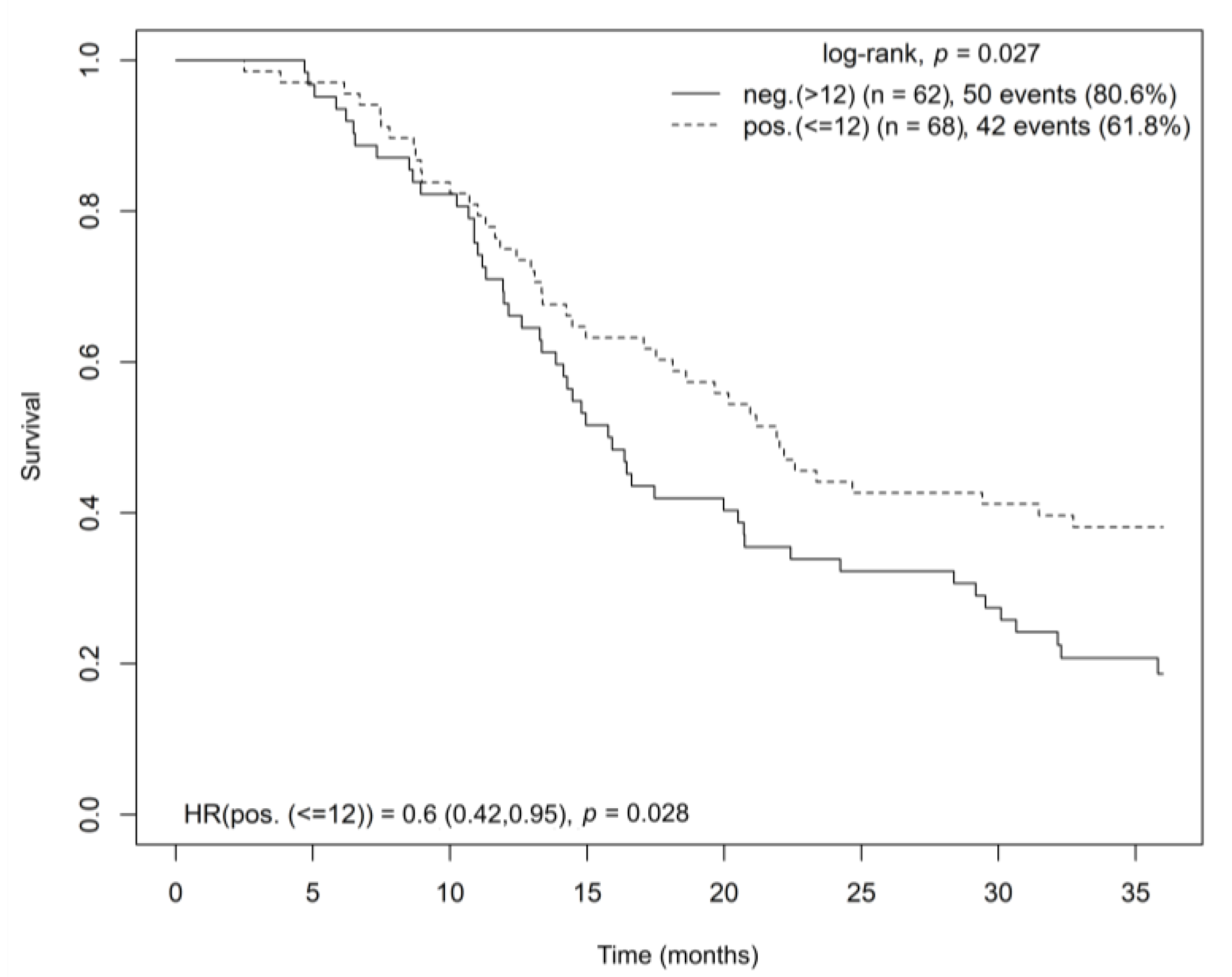
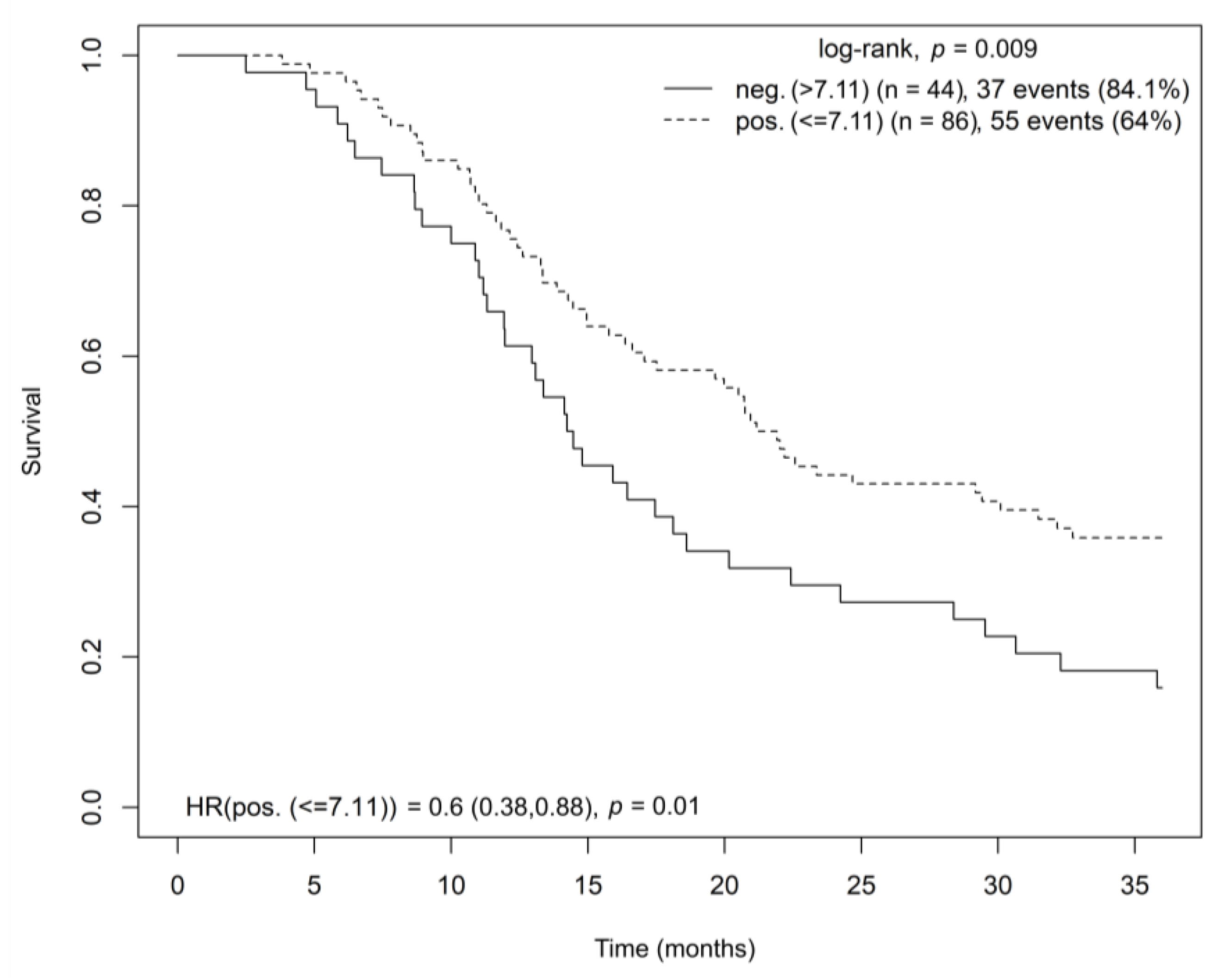
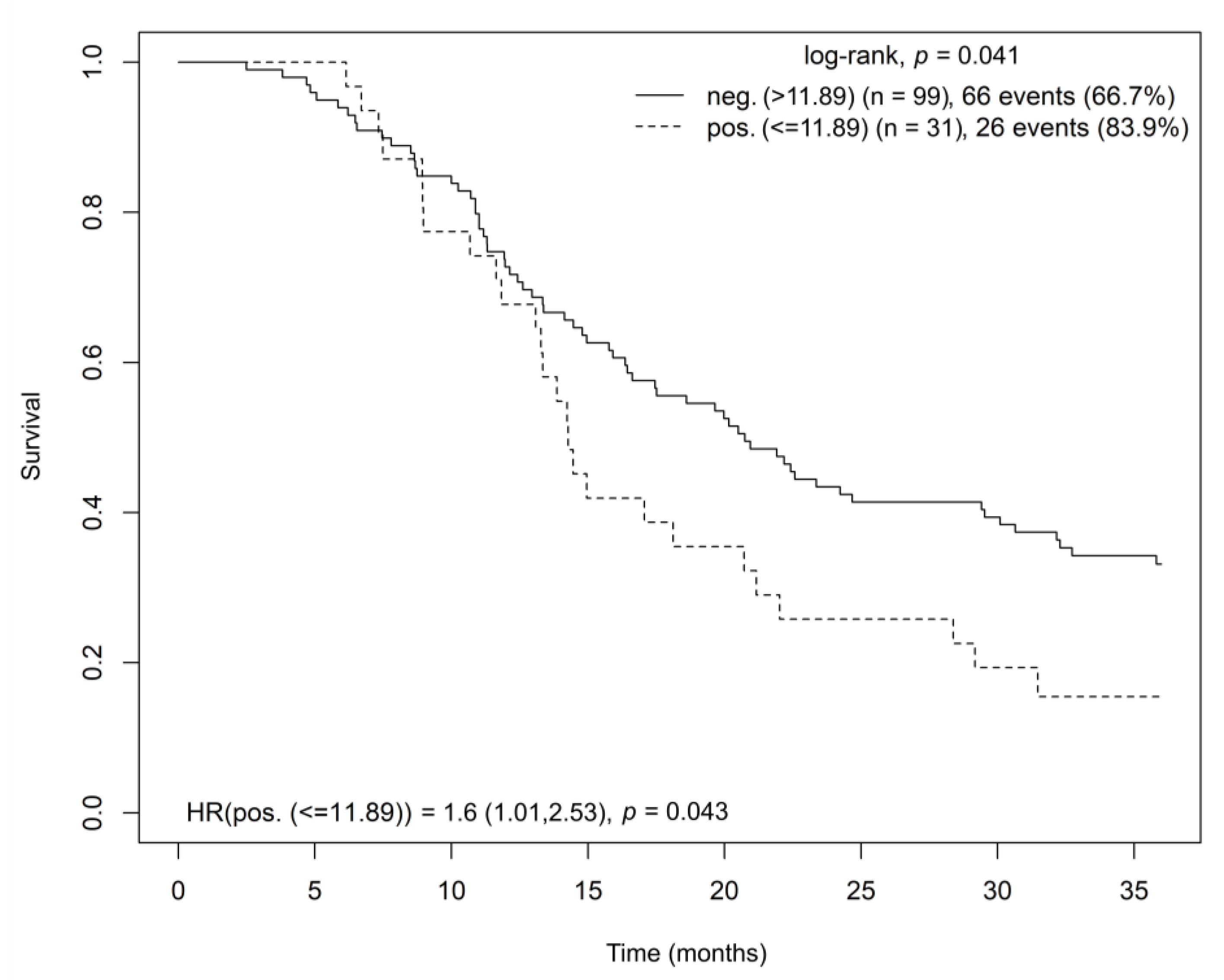
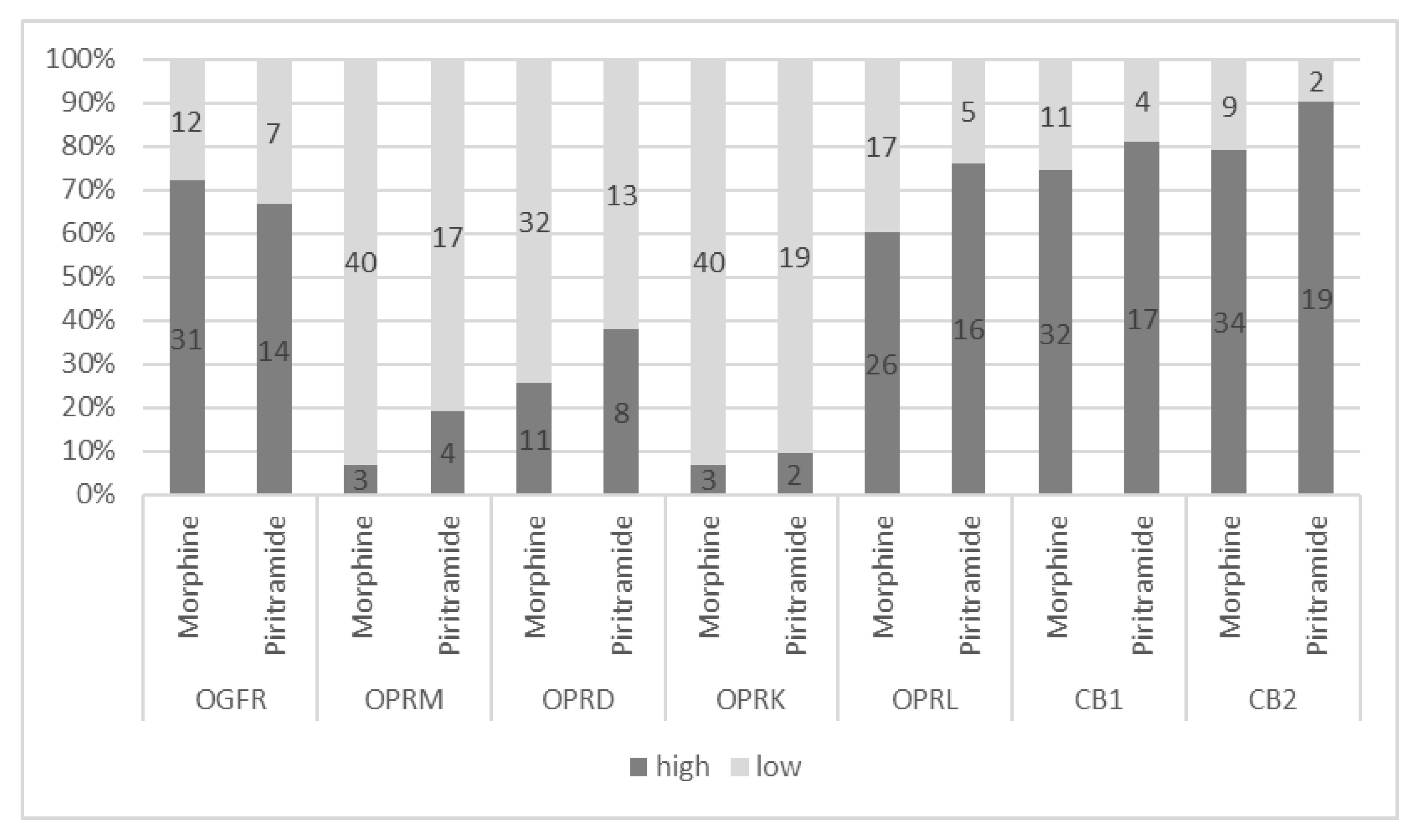
3.1. Opioid and Cannabinoid Receptor Gene Expressions’ Effects on Overall Survival
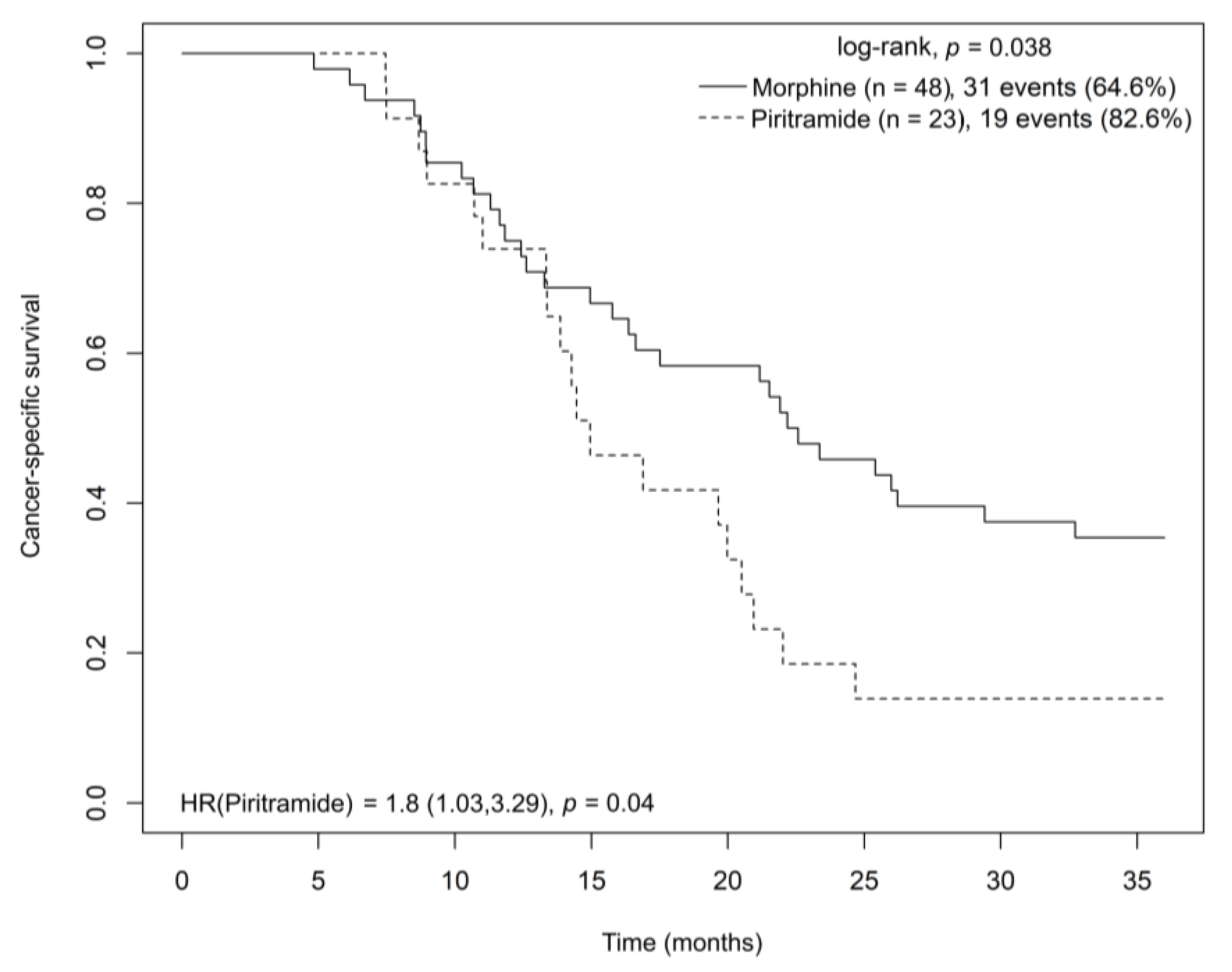
3.2. Postoperative Analgesia Effects on Cancer-Specific Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef]
- Latenstein, A.E.J.; van Roessel, S.; van der Geest, L.G.M.; Bonsing, B.A.; Dejong, C.H.C.; Groot Koerkamp, B.; de Hingh, I.H.J.T.; Homs, M.Y.V.; Klaase, J.M.; Lemmens, V.; et al. Conditional Survival After Resection for Pancreatic Cancer: A Population-Based Study and Prediction Model. Ann. Surg. Oncol. 2020, 27, 2516–2524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Call, T.R.; Pace, N.L.; Thorup, D.B.; Maxfield, D.; Chortkoff, B.; Christensen, J.; Mulvihill, S.J. Factors Associated with Improved Survival after Resection of Pancreatic Adenocarcinoma: A Multivariable Model. Anesthesiology 2015, 122, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Kobi, M.; Veillette, G.; Narurkar, R.; Sadowsky, D.; Paroder, V.; Shilagani, C.; Gilet, A.; Flusberg, M. Imaging and Management of Pancreatic Cancer. Semin. Ultrasound CT MR 2020, 41, 139–151. [Google Scholar] [CrossRef]
- Loveday, B.P.; Lipton, L.; Thomson, B.N. Pancreatic Cancer: An Update on Diagnosis and Management. Aust. J. Gen. Gen. Pract. 2019, 48, 826–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic Cancer: A Review of Clinical Diagnosis, Epidemiology, Treatment and Outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef] [PubMed]
- Cummings, K.C.; Xu, F.; Cummings, L.C.; Cooper, G.S. A Comparison of Epidural Analgesia and Traditional Pain Management Effects on Survival and Cancer Recurrence after Colectomy: A Population-Based Study. Anesthesiology 2012, 116, 797–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Z.-Z.; Li, H.-J.; Li, M.-H.; Huang, S.-M.; Li, X.; Liu, Q.-H.; Li, J.; Li, X.-Y.; Wang, D.-X.; Sessler, D.I. Epidural Anesthesia-Analgesia and Recurrence-Free Survival after Lung Cancer Surgery: A Randomized Trial. Anesthesiology 2021, 135, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Sessler, D.I. Does Regional Analgesia Reduce the Risk of Cancer Recurrence? A Hypothesis. Eur. J. Cancer Prev. 2008, 17, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Havlik, R.; Srovnal, J.; Klos, D.; Benedikova, A.; Lovecek, M.; Ghothim, M.; Cahova, D.; Neoral, C.; Hajduch, M. Occult Tumour Cells in Peritoneal Lavage Are a Negative Prognostic Factor in Pancreatic Cancer. Biomed. Pap. Med. Fac. Palacky Univ. Olomouc Czech Repub. 2013, 157, 233–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.; Jun, H.R.; Choi, H.W.; Hwang, D.W.; Lee, J.H.; Song, K.B.; Lee, W.; Kwon, J.; Ha, S.H.; Jun, E.; et al. Circulating Tumour Cells as an Indicator of Early and Systemic Recurrence after Surgical Resection in Pancreatic Ductal Adenocarcinoma. Sci. Rep. 2021, 11, 1644. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Wang, P.; Peng, J.; Wang, X.; Zhu, Y.; Shen, N. Meta-Analysis Reveals the Prognostic Value of Circulating Tumour Cells Detected in the Peripheral Blood in Patients with Non-Metastatic Colorectal Cancer. Sci. Rep. 2017, 7, 905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stejskal, P.; Srovnal, J.; Berta, E.; Rehulkova, A.; Vecera, L.; Haiduk, F.; Michalek, P.; Hajduch, M. Abstract 1956: Perioperative Opioid Analgesia Affects the Circulating Tumor Cells Levels in Colorectal Cancer Patients. Cancer Res. 2022, 82, 1956. [Google Scholar] [CrossRef]
- Srovnal, J.; Berta, E.; Rehulkova, A.; Vidlarova, M.; Prasil, P.; Vecera, L.; Stourac, P.; Kourilova, P.; Hajduch, M. Abstract B41: Piritramide Analgesia Reduces CEA MRNA-Positive Circulating Tumor Cells’ Presence Compared to Morphine and Epidural Analgesia Following Radical Colon Cancer Surgery. Clin. Cancer Res. 2020, 26, B41. [Google Scholar] [CrossRef]
- Vidlarova, M.; Berta, E.; Prasil, P.; Prokopova, A.; Gurska, S.; Khoylou, M.; Rehulkova, A.; Kourilova, P.; Chudacek, J.; Szkorupa, M.; et al. Cannabinoid Receptor 2 Expression in Early-Stage Non-Small Cell Lung Cancers Identifies Patients with Good Prognosis and Longer Survival. Transl. Lung Cancer Res. 2022, 11, 2040–2050. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Liu, Y.; Huang, S.; Liu, G.; Xie, C.; Zhou, J.; Fan, W.; Li, Q.; Wang, Q.; Zhong, D.; et al. Overexpression of Cannabinoid Receptors CB1 and CB2 Correlates with Improved Prognosis of Patients with Hepatocellular Carcinoma. Cancer Genet. Cytogenet. 2006, 171, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Carracedo, A.; Lorente, M.; Egia, A.; Blázquez, C.; García, S.; Giroux, V.; Malicet, C.; Villuendas, R.; Gironella, M.; González-Feria, L.; et al. The Stress-Regulated Protein P8 Mediates Cannabinoid-Induced Apoptosis of Tumor Cells. Cancer Cell 2006, 9, 301–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecera, L.; Gabrhelik, T.; Prasil, P.; Stourac, P. The Role of Cannabinoids in the Treatment of Cancer. Bratisl. Lek. Listy 2020, 121, 79–95. [Google Scholar] [CrossRef]
- Solinas, M.; Massi, P.; Cantelmo, A.R.; Cattaneo, M.G.; Cammarota, R.; Bartolini, D.; Cinquina, V.; Valenti, M.; Vicentini, L.M.; Noonan, D.M.; et al. Cannabidiol Inhibits Angiogenesis by Multiple Mechanisms. Br. J. Pharmacol. 2012, 167, 1218–1231. [Google Scholar] [CrossRef] [Green Version]
- Pisanti, S.; Picardi, P.; D’Alessandro, A.; Laezza, C.; Bifulco, M. The Endocannabinoid Signaling System in Cancer. Trends Pharmacol. Sci. 2013, 34, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.X.; Sharma, S.; Stolina, M.; Gardner, B.; Roth, M.D.; Tashkin, D.P.; Dubinett, S.M. Delta-9-Tetrahydrocannabinol Inhibits Antitumor Immunity by a CB2 Receptor-Mediated, Cytokine-Dependent Pathway. J. Immunol. 2000, 165, 373–380. [Google Scholar] [CrossRef]
- Michalski, C.W.; Oti, F.E.; Erkan, M.; Sauliunaite, D.; Bergmann, F.; Pacher, P.; Batkai, S.; Müller, M.W.; Giese, N.A.; Friess, H.; et al. Cannabinoids in Pancreatic Cancer: Correlation with Survival and Pain. Int. J. Cancer 2008, 122, 742–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Qu, M.; Gorur, A.; Sun, Z.; Cata, J.P.; Chen, W.; Miao, C. Association of Mu-Opioid Receptor (MOR) Expression and Opioids Requirement with Survival in Patients with Stage I-III Pancreatic Ductal Adenocarcinoma. Front. Oncol. 2021, 11, 686877. [Google Scholar] [CrossRef]
- Zagon, I.S.; Smith, J.P.; McLaughlin, P.J. Human Pancreatic Cancer Cell Proliferation in Tissue Culture Is Tonically Inhibited by Opioid Growth Factor. Int. J. Oncol. 1999, 14, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.R.; Barlass, U.; Armstrong, A.; Shaikh, M.; Bishehsari, F. Novel Role of the Mu-Opioid Receptor in Pancreatic Cancer: Potential Link between Opioid Use and Cancer Progression. Mol. Cell. Biochem. 2022, 477, 1339–1345. [Google Scholar] [CrossRef] [PubMed]
- Shakhar, G.; Ben-Eliyahu, S. Potential Prophylactic Measures against Postoperative Immunosuppression: Could They Reduce Recurrence Rates in Oncological Patients? Ann. Surg. Oncol. 2003, 10, 972–992. [Google Scholar] [CrossRef] [PubMed]
- Stamer, U.; Mpasios, N.; Stüber, F.; Laubenthal, H.; Maier, C. Postoperative Schmerztherapie in Deutschland Ergebnisse einer Umfrage. Anaesthesist 2002, 51, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Kinstner, C.; Likar, R.; Sandner-Kiesling, A.; Hutschala, D.; Pipam, W.; Gustorff, B. Qualität der postoperativen Schmerztherapie in Österreich. Anaesthesist 2011, 60, 827. [Google Scholar] [CrossRef]
- Gabrhelík, T.; Pieran, M. Léčba Pooperační Bolesti. Interní Medicína Pro Praxi 2012, 14, 23–25. [Google Scholar]
- Gramke, H.-F.; de Rijke, J.M.; van Kleef, M.; Raps, F.; Kessels, A.G.H.; Peters, M.L.; Sommer, M.; Marcus, M.A.E. The Prevalence of Postoperative Pain in a Cross-Sectional Group of Patients after Day-Case Surgery in a University Hospital. Clin. J. Pain 2007, 23, 543–548. [Google Scholar] [CrossRef]
- Janssen, P.A. Pirinitramide (R 3365), a Potent Analgesic with Unusual Chemical Structure. J. Pharm. Pharmacol. 1961, 13, 513–530. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Rowbotham, D.J. Piritramide. Br. J. Anaesth. 1999, 82, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Hinrichs, M.; Weyland, A.; Bantel, C. Piritramid. Schmerz 2017, 31, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Kay, B. A Clinical Investigation of Piritramide in the Treatment of Postoperative Pain. Br. J. Anaesth. 1971, 43, 1167–1171. [Google Scholar] [CrossRef]
- Gottschalk, A.; Sharma, S.; Ford, J.; Durieux, M.E.; Tiouririne, M. Review Article: The Role of the Perioperative Period in Recurrence after Cancer Surgery. Anesth. Analg. 2010, 110, 1636–1643. [Google Scholar] [CrossRef]
- Harimaya, Y.; Koizumi, K.; Andoh, T.; Nojima, H.; Kuraishi, Y.; Saiki, I. Potential Ability of Morphine to Inhibit the Adhesion, Invasion and Metastasis of Metastatic Colon 26-L5 Carcinoma Cells. Cancer Lett. 2002, 187, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Zagon, I.S.; Rahn, K.A.; McLaughlin, P.J. Opioids and Migration, Chemotaxis, Invasion, and Adhesion of Human Cancer Cells. Neuropeptides 2007, 41, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Kshirsagar, S.; Chang, L.; Schwartz, R.; Law, P.-Y.; Yee, D.; Hebbel, R.P. Morphine Stimulates Angiogenesis by Activating Proangiogenic and Survival-Promoting Signaling and Promotes Breast Tumor Growth. Cancer Res. 2002, 62, 4491–4498. [Google Scholar]
- Ustun, F.; Durmus-Altun, G.; Altaner, S.; Tuncbilek, N.; Uzal, C.; Berkarda, S. Evaluation of Morphine Effect on Tumour Angiogenesis in Mouse Breast Tumour Model, EATC. Med. Oncol. 2011, 28, 1264–1272. [Google Scholar] [CrossRef]
- Koodie, L.; Ramakrishnan, S.; Roy, S. Morphine Suppresses Tumor Angiogenesis through a HIF-1alpha/P38MAPK Pathway. Am. J. Pathol. 2010, 177, 984–997. [Google Scholar] [CrossRef]
- Zagon, I.S.; McLaughlin, P.J. Opioid Growth Factor and the Treatment of Human Pancreatic Cancer: A Review. World J. Gastroenterol. 2014, 20, 2218–2223. [Google Scholar] [CrossRef] [PubMed]
- Zagon, I.S.; Verderame, M.F.; Hankins, J.; McLaughlin, P.J. Overexpression of the Opioid Growth Factor Receptor Potentiates Growth Inhibition in Human Pancreatic Cancer Cells. Int. J. Oncol. 2007, 30, 775–783. [Google Scholar] [CrossRef] [Green Version]
- Zagon, I.S.; Smith, J.P.; Conter, R.; McLaughlin, P.J. Identification and Characterization of Opioid Growth Factor Receptor in Human Pancreatic Adenocarcinoma. Int. J. Mol. Med. 2000, 5, 77–84. [Google Scholar]
- Falk, W.; Magnuson, A.; Eintrei, C.; Henningsson, R.; Myrelid, P.; Matthiessen, P.; Gupta, A. Comparison between Epidural and Intravenous Analgesia Effects on Disease-Free Survival after Colorectal Cancer Surgery: A Randomised Multicentre Controlled Trial. Br. J. Anaesth. 2021, 127, 65–74. [Google Scholar] [CrossRef]
- Prasil, P.; Berta, E.; Srovnal, J.; Gabrhelik, T.; Adamus, M.; Hajduch, M. Morphinebut Not Piritramide-Based Postoperative Analgesia Negatively Influences Levels of Circulating Tumor Cells and Patients’ Survival Following Colorectal Cancer Surgery: 14AP6-1. Eur. J. Anaesthesiol. EJA 2014, 31, 229. [Google Scholar] [CrossRef] [Green Version]
- Ravi, J.; Sneh, A.; Shilo, K.; Nasser, M.W.; Ganju, R.K. FAAH Inhibition Enhances Anandamide Mediated Anti-Tumorigenic Effects in Non-Small Cell Lung Cancer by Downregulating the EGF/EGFR Pathway. Oncotarget 2014, 5, 2475–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierra, S.; Gupta, A.; Gomes, I.; Fowkes, M.; Ram, A.; Bobeck, E.N.; Devi, L.A. Targeting Cannabinoid 1 and Delta Opioid Receptor Heteromers Alleviates Chemotherapy-Induced Neuropathic Pain. ACS Pharmacol. Transl. Sci. 2019, 2, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Page, G.G. Immunologic Effects of Opioids in the Presence or Absence of Pain. J. Pain Symptom Manag. 2005, 29, S25–S31. [Google Scholar] [CrossRef]
- Martinez, L.; Ekman, E.; Nakhla, N. Perioperative Opioid-Sparing Strategies: Utility of Conventional NSAIDs in Adults. Clin. Ther. 2019, 41, 2612–2628. [Google Scholar] [CrossRef] [PubMed]
- Mulita, F.; Karpetas, G.; Liolis, E.; Vailas, M.; Tchabashvili, L.; Maroulis, I. Comparison of Analgesic Efficacy of Acetaminophen Monotherapy versus Acetaminophen Combinations with Either Pethidine or Parecoxib in Patients Undergoing Laparoscopic Cholecystectomy: A Randomized Prospective Study. Med. Glas. 2021, 18, 27–32. [Google Scholar] [CrossRef]
- Petrelli, F.; Tomasello, G.; Ghidini, M.; Lonati, V.; Passalacqua, R.; Barni, S. Disease-Free Survival Is Not a Surrogate Endpoint for Overall Survival in Adjuvant Trials of Pancreatic Cancer: A Systematic Review of Randomized Trials. HPB 2017, 19, 944–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Age > 18 years | Tumor duplicity |
| Pancreatic adenocarcinoma (except ampullary carcinoma) | Death or reoperation within 30 days of surgery |
| Stage I, II, III (TNM classification) | |
| R0/R1 resection radicality | |
| Morphine or piritramide postoperative analgesia |
| Patient Characteristics | All Patients (n = 137) n (%) | Morphine (n = 48) n (%) | Piritramide (n = 23) n (%) |
|---|---|---|---|
| Sex | |||
| Male | 66 (48.5) | 24 (50) | 16 (69.6) |
| Female | 70 (51.5) | 24 (50) | 7 (30.4) |
| Tumor stage | |||
| I | 14 (10.2) | 7 (14.6) | 7 (30.4) |
| II | 109 (79.6) | 40 (83.3) | 16 (69.6) |
| III | 14 (10.2) | 1 (2.1) | 0 (0) |
| Tumor grade | |||
| 1 | 6 (4.4) | 2 (4.2) | 4 (17.4) |
| 2 | 78 (56.9) | 26 (54.2) | 11 (47.8) |
| 3 | 53 (38.7) | 20 (41.7) | 8 (34.8) |
| Age (years) | |||
| Median (q1–q3) | 63 (58.5–69) | 63 (58.5–69) | 65 (58.5–69) |
| Resection | |||
| R0 | 80 (58.4) | 48 (100) | 20 (87) |
| R1 | 57 (41.6) | 0 (0) | 3 (13) |
| Dosage (milligrams) | |||
| Median (q1–q3) | NA | 90 (70–120) | 101.2 (61.88–135) |
| OS (months) Median (95% CI) | 20.2 (16.4; 23.4) | 22.4 (16.6; NA) | 15.0 (13.4; 20.9) |
| CSS (months) Median (95% CI) | NA | 22.4 (16.6; NA) | 15.0 (13.4; 20.9) |
| HR | 95% CI | p-Value | |
|---|---|---|---|
| Age | 1.011 | 0.987–1.036 | 0.363 |
| Sex | 1.057 | 0.677–1.65 | 0.806 |
| OGFR | 0.435 | 0.264–0.717 | 0.001 |
| OPRM | 2.076 | 1.199–3.594 | 0.009 |
| OPRD | 2.264 | 1.334–3.843 | 0.002 |
| OPRK | 0.480 | 0.286–0.805 | 0.005 |
| OPRL | 3.017 | 1.344–6.775 | 0.007 |
| CB2 | 0.538 | 0.333–0.869 | 0.011 |
| HR | 95% CI | p-Value | |
|---|---|---|---|
| Age | 1.023 | 0.978–1.07 | 0.318 |
| Sex | 1.234 | 0.632–2.409 | 0.538 |
| Piritramide | 3.060 | 1.478–6.337 | 0.003 |
| OPRM | 0.203 | 0.055–0.750 | 0.017 |
| OPRD | 4.886 | 2.228–10.717 | <0.001 |
| CB2 | 0.185 | 0.079–0.435 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vecera, L.; Prasil, P.; Srovnal, J.; Berta, E.; Vidlarova, M.; Gabrhelik, T.; Kourilova, P.; Lovecek, M.; Skalicky, P.; Skarda, J.; et al. Morphine Analgesia, Cannabinoid Receptor 2, and Opioid Growth Factor Receptor Cancer Tissue Expression Improve Survival after Pancreatic Cancer Surgery. Cancers 2023, 15, 4038. https://doi.org/10.3390/cancers15164038
Vecera L, Prasil P, Srovnal J, Berta E, Vidlarova M, Gabrhelik T, Kourilova P, Lovecek M, Skalicky P, Skarda J, et al. Morphine Analgesia, Cannabinoid Receptor 2, and Opioid Growth Factor Receptor Cancer Tissue Expression Improve Survival after Pancreatic Cancer Surgery. Cancers. 2023; 15(16):4038. https://doi.org/10.3390/cancers15164038
Chicago/Turabian StyleVecera, Lubomir, Petr Prasil, Josef Srovnal, Emil Berta, Monika Vidlarova, Tomas Gabrhelik, Pavla Kourilova, Martin Lovecek, Pavel Skalicky, Jozef Skarda, and et al. 2023. "Morphine Analgesia, Cannabinoid Receptor 2, and Opioid Growth Factor Receptor Cancer Tissue Expression Improve Survival after Pancreatic Cancer Surgery" Cancers 15, no. 16: 4038. https://doi.org/10.3390/cancers15164038
APA StyleVecera, L., Prasil, P., Srovnal, J., Berta, E., Vidlarova, M., Gabrhelik, T., Kourilova, P., Lovecek, M., Skalicky, P., Skarda, J., Kala, Z., Michalek, P., & Hajduch, M. (2023). Morphine Analgesia, Cannabinoid Receptor 2, and Opioid Growth Factor Receptor Cancer Tissue Expression Improve Survival after Pancreatic Cancer Surgery. Cancers, 15(16), 4038. https://doi.org/10.3390/cancers15164038