
Usefulness of Tumor Marker Score for Predicting the Prognosis of Hepatocellular Carcinoma Patients Treated with Atezolizumab Plus Bevacizumab: A Multicenter Retrospective Study

 , , , , , , , , , ,
, , , , , , , , , ,  , , , ,
, , , ,  , ,
, ,  , , ,
, , ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
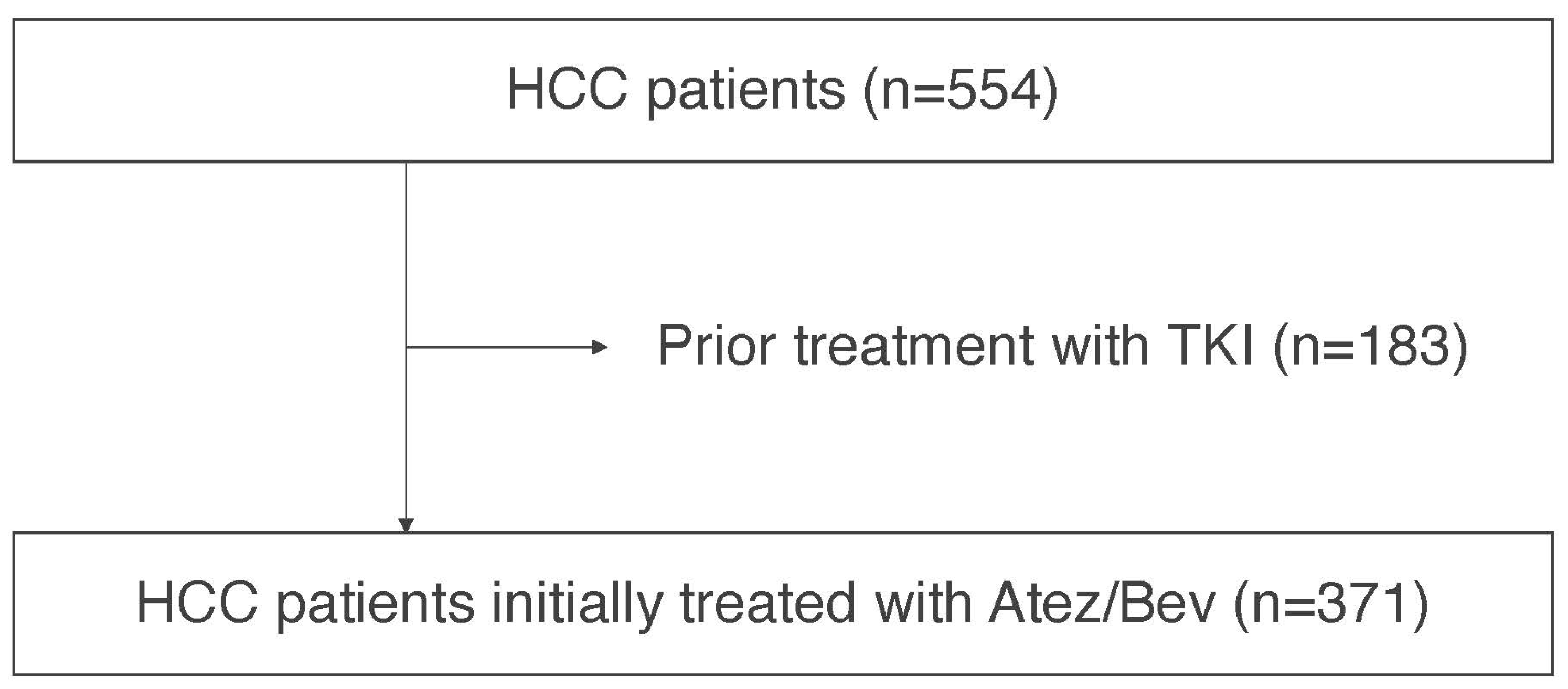
2.1. Patients
2.2. Basal Hepatic Disease and Assessment Methods for Hepatic Function
2.3. Diagnosis and Therapeutic Strategies for HCC
2.4. Assessment of Treatment Response
2.5. Methods for Assessment of Prognosis
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the HCC Patients
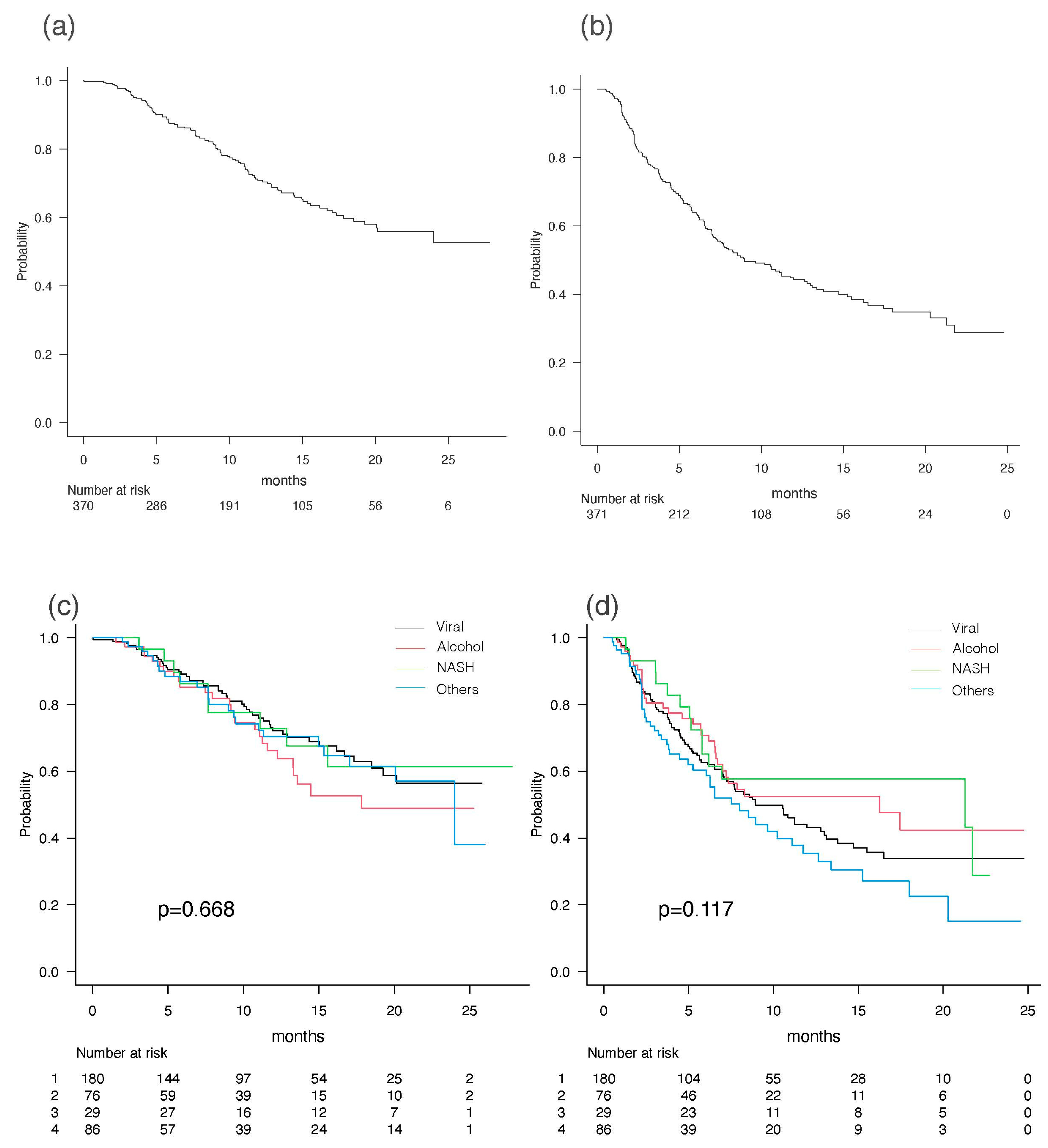
3.2. Prognosis of HCC Patients Treated with Atez/Bev
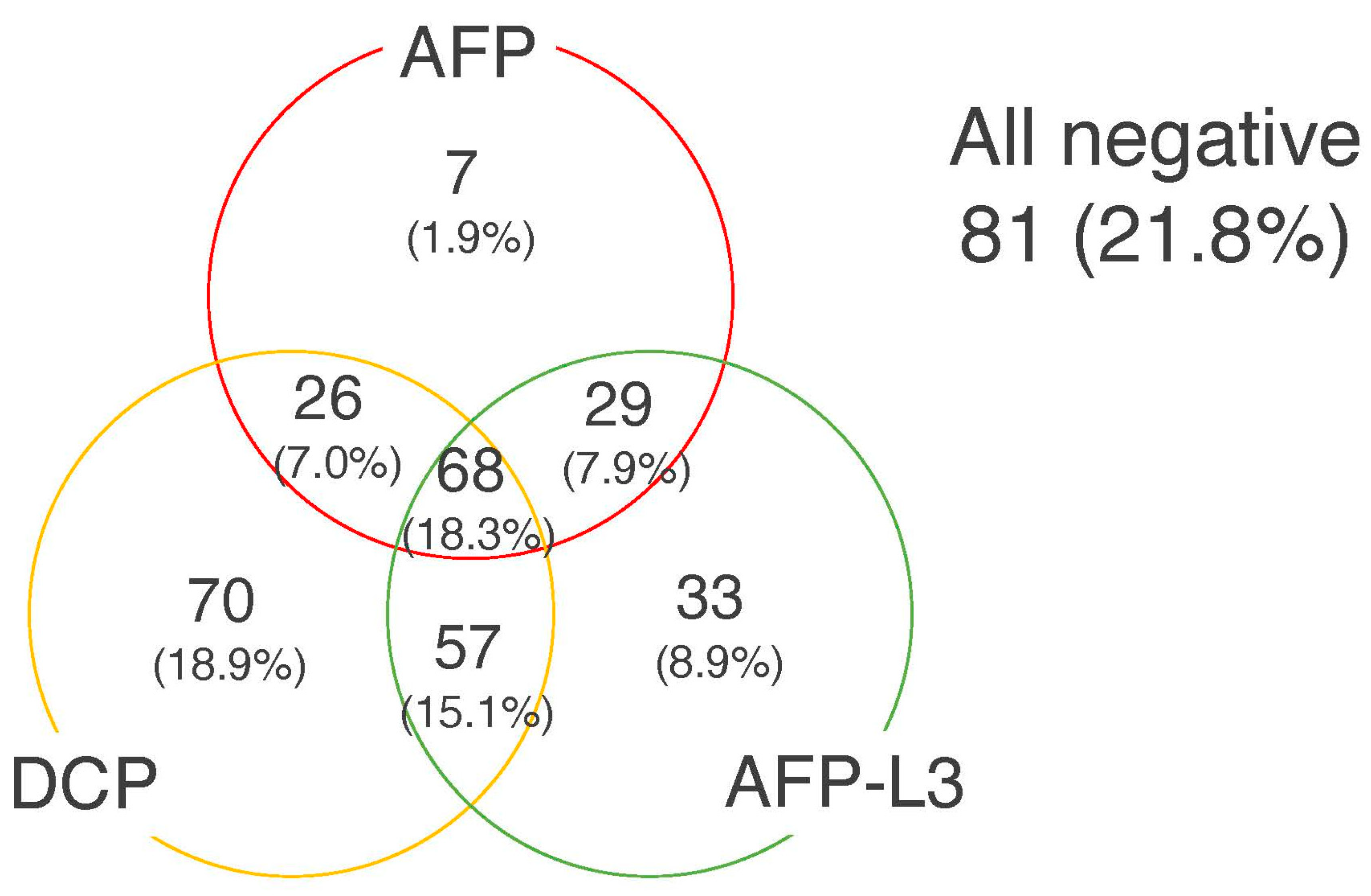
3.3. Tumor Marker Score
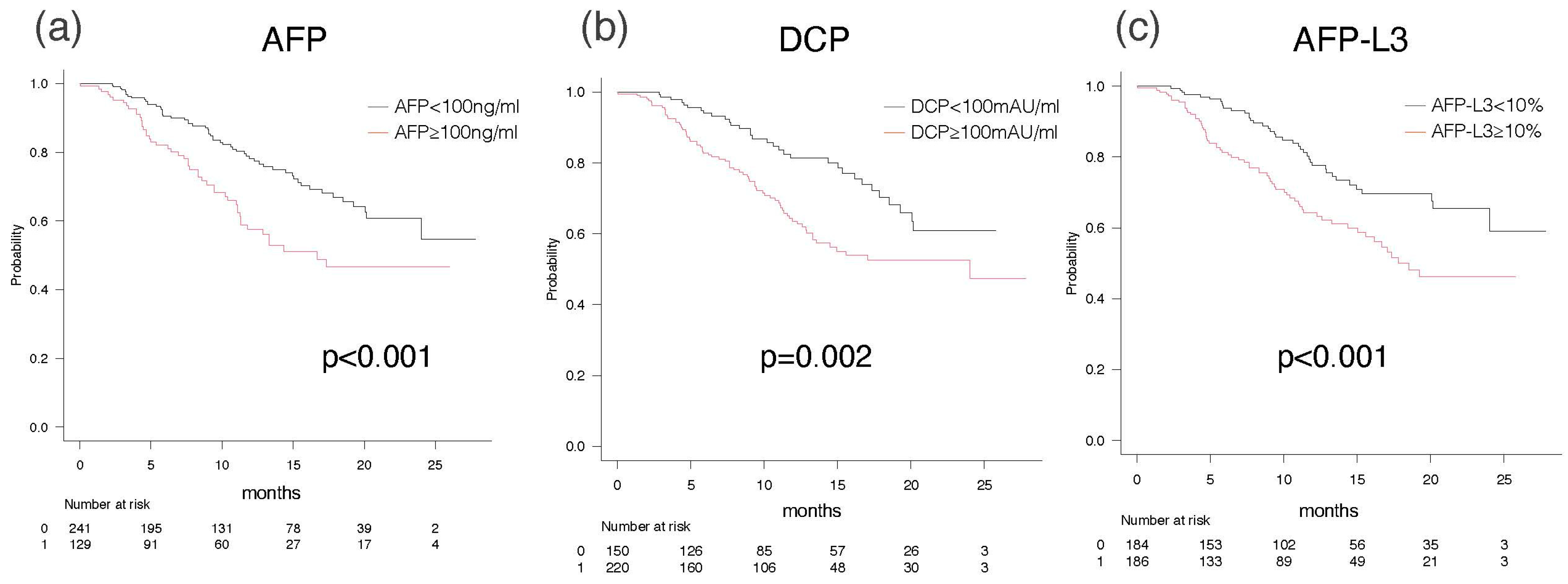
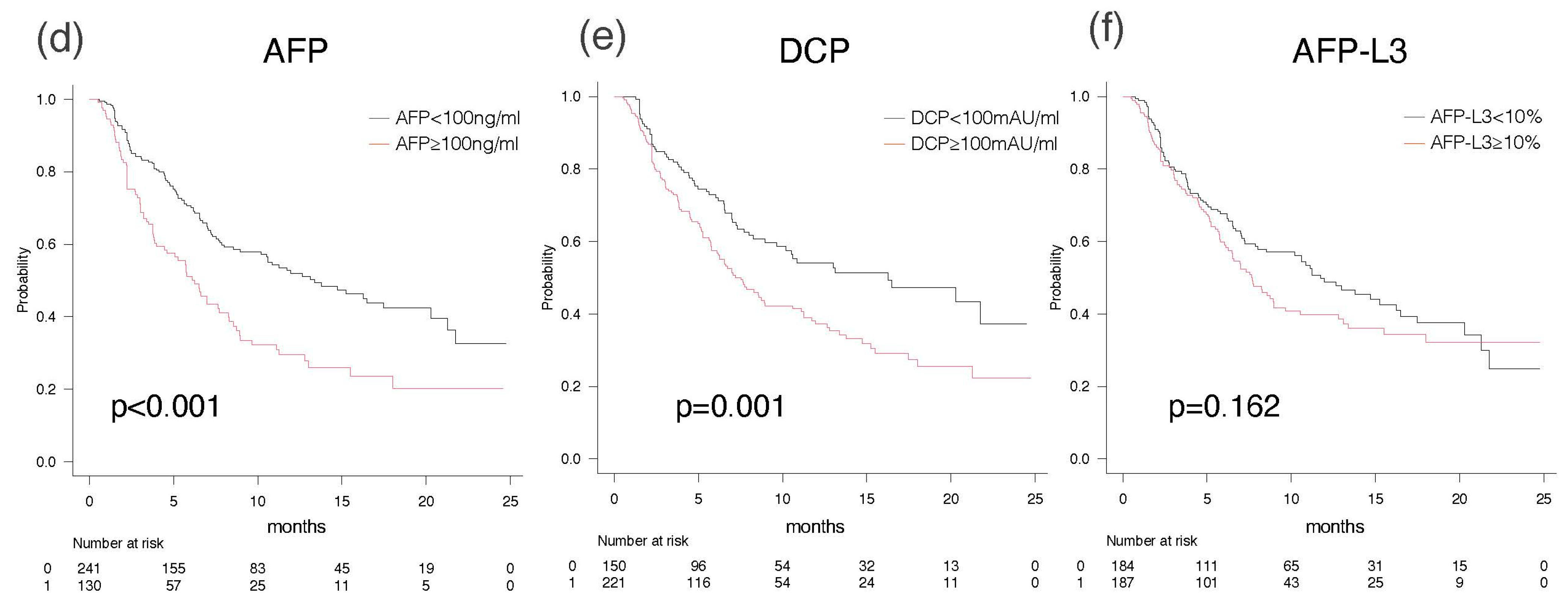
3.4. Overall Survival and Progression-Free Survival According to Elevation of Each Tumor Marker
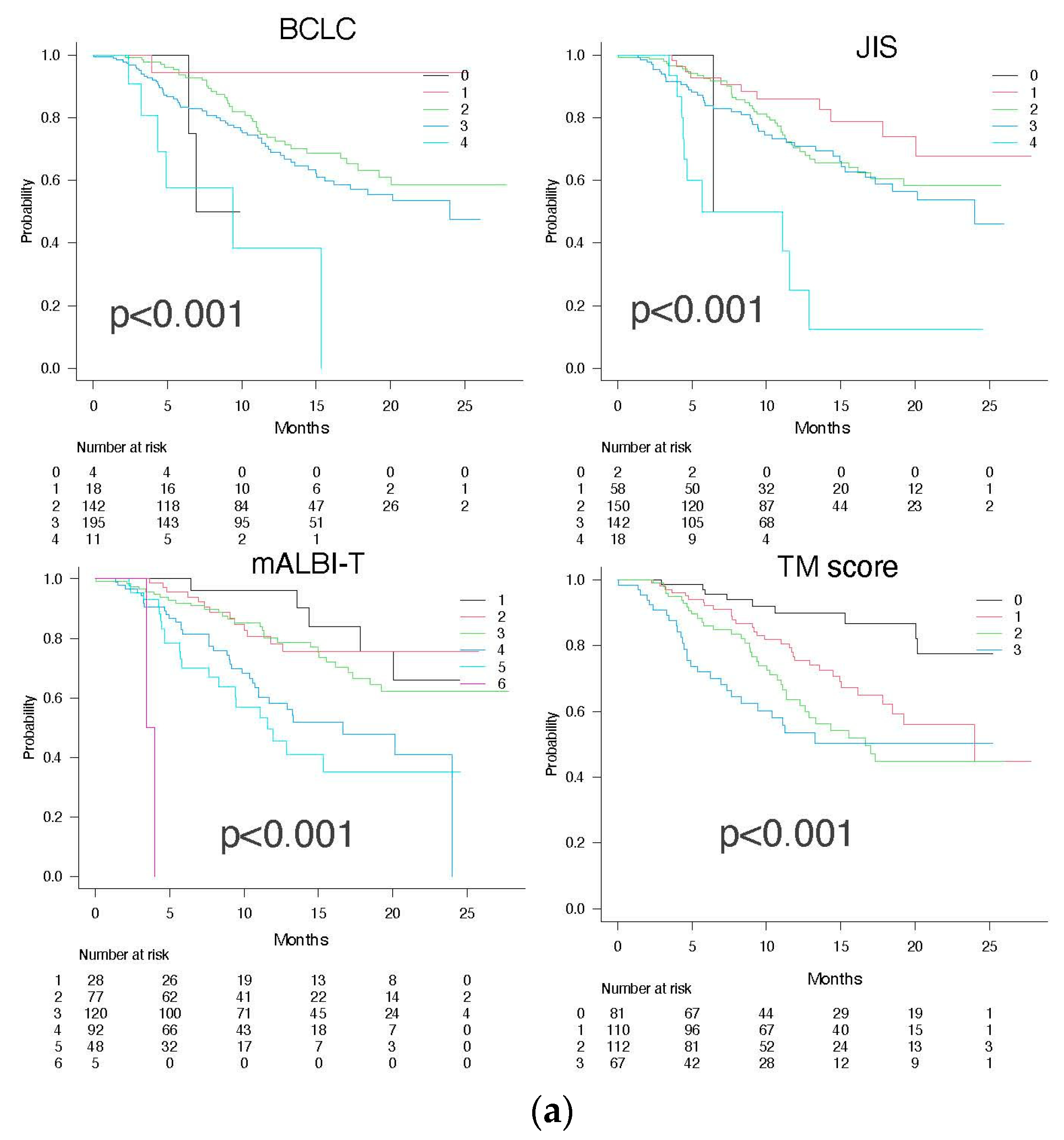
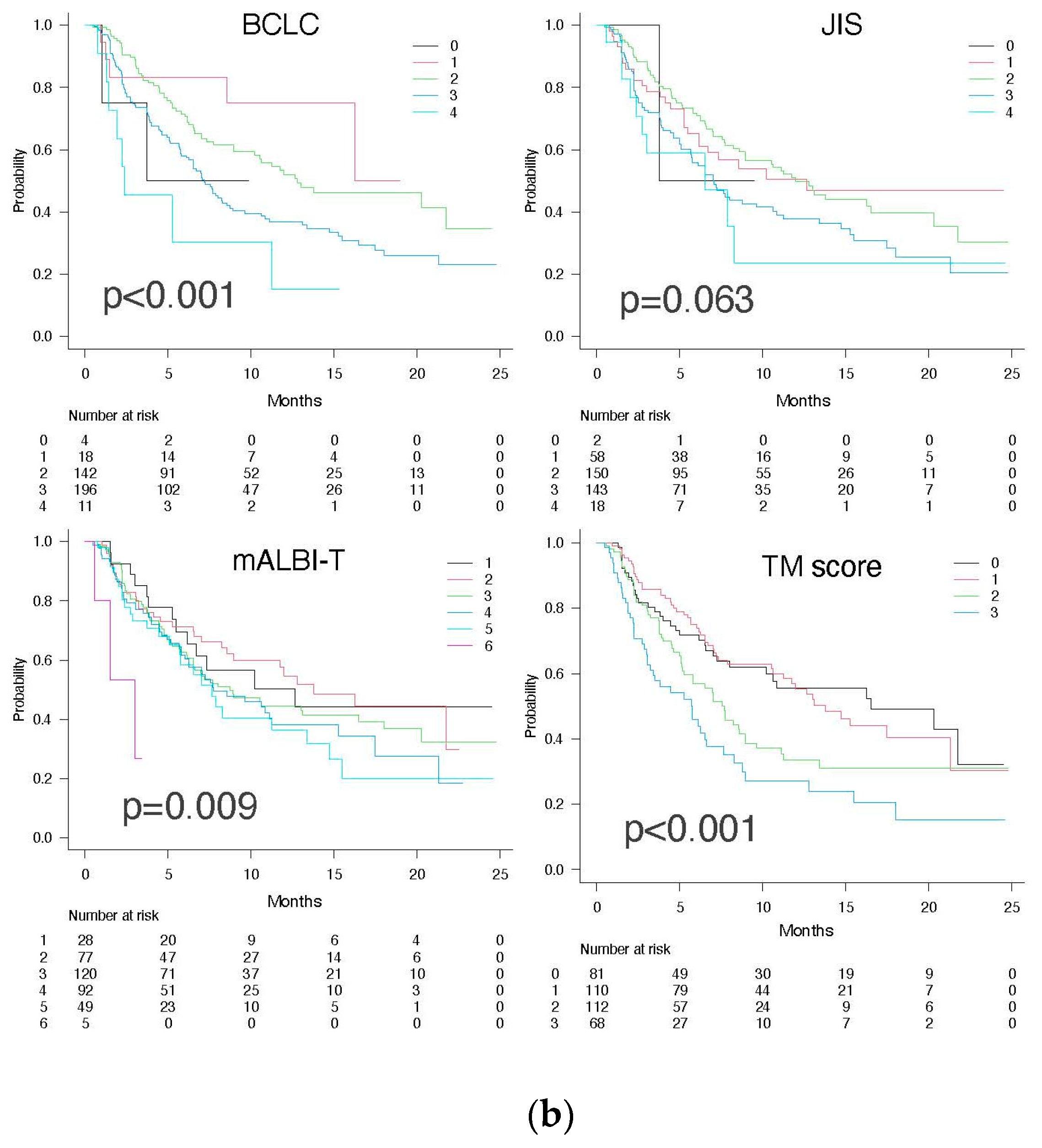
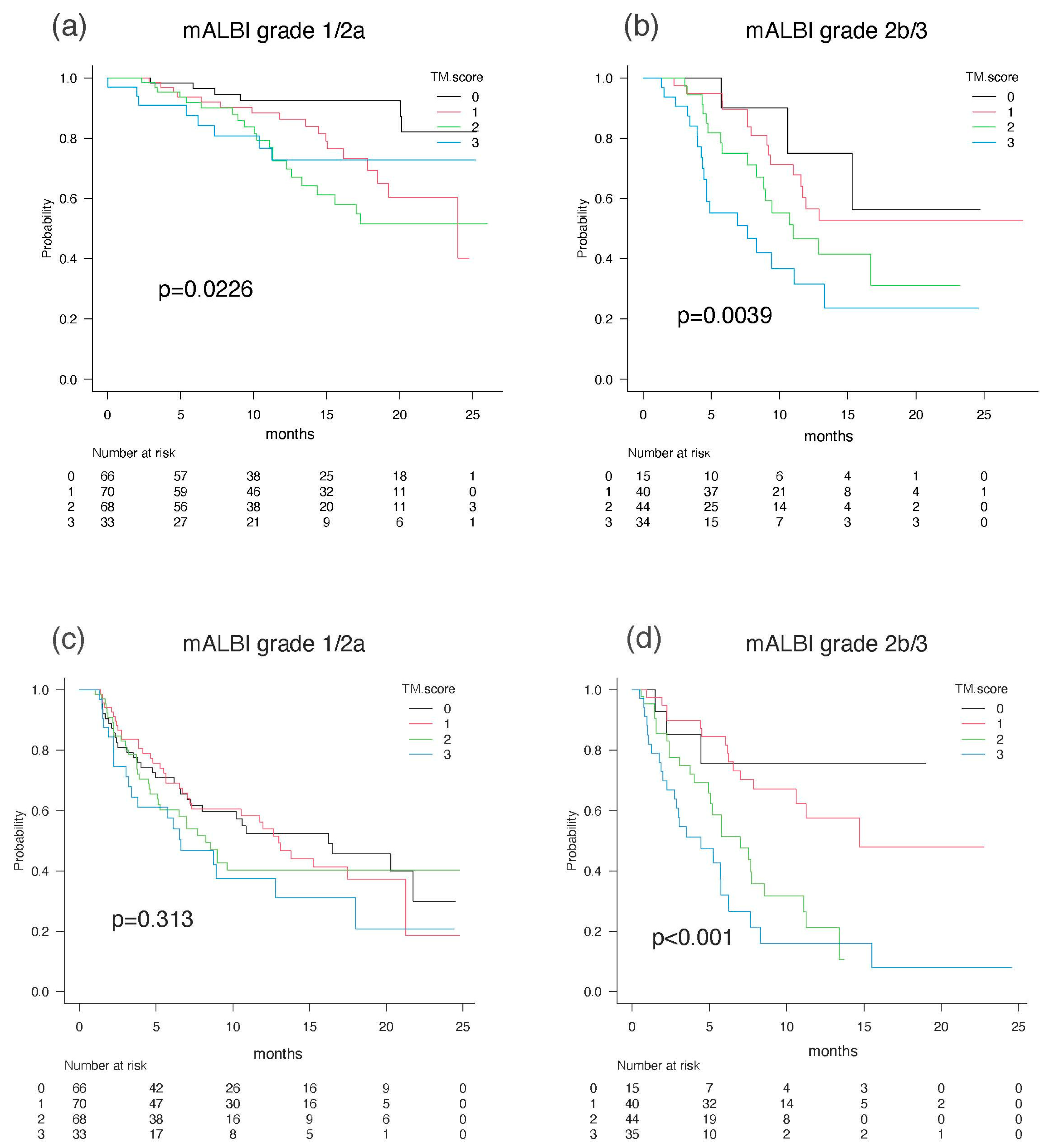
3.5. Predictive Value According to TM Score, BCLC Stage, JIS, and mALBI-T Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef] [PubMed]
- A new prognostic system for hepatocellular carcinoma: A retrospective study of 435 patients: The Cancer of the Liver Italian Program (CLIP) investigators. Hepatology 1998, 28, 751–755. [CrossRef]
- Kudo, M.; Chung, H.; Osaki, Y. Prognostic staging system for hepatocellular carcinoma (CLIP score): Its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J. Gastroenterol. 2003, 38, 207–215. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Kudo, M. Newly Proposed ALBI Grade and ALBI-T Score as Tools for Assessment of Hepatic Function and Prognosis in Hepatocellular Carcinoma Patients. Liver Cancer 2019, 8, 312–325. [Google Scholar] [CrossRef]
- Scheiner, B.; Pomej, K.; Kirstein, M.M.; Hucke, F.; Finkelmeier, F.; Waidmann, O.; Himmelsbach, V.; Schulze, K.; von Felden, J.; Fründt, T.W.; et al. Prognosis of patients with hepatocellular carcinoma treated with immunotherapy—Development and validation of the CRAFITY score. J. Hepatol. 2022, 76, 353–363. [Google Scholar] [CrossRef]
- Suzuki, M.; Shiraha, H.; Fujikawa, T.; Takaoka, N.; Ueda, N.; Nakanishi, Y.; Koike, K.; Takaki, A.; Shiratori, Y. Des-gamma-carboxy prothrombin is a potential autologous growth factor for hepatocellular carcinoma. J. Biol. Chem. 2005, 280, 6409–6415. [Google Scholar] [CrossRef]
- Yue, P.; Gao, Z.H.; Xue, X.; Cui, S.X.; Zhao, C.R.; Yuan, Y.; Yin, Z.; Inagaki, Y.; Kokudo, N.; Tang, W.; et al. Des-γ-carboxyl prothrombin induces matrix metalloproteinase activity in hepatocellular carcinoma cells by involving the ERK1/2 MAPK signalling pathway. Eur. J. Cancer 2011, 47, 1115–1124. [Google Scholar] [CrossRef]
- Guerra, N.; Tan, Y.X.; Joncker, N.T.; Choy, A.; Gallardo, F.; Xiong, N.; Knoblaugh, S.; Cado, D.; Greenberg, N.M.; Raulet, D.H. NKG2D-deficient mice are defective in tumor surveillance in models of spontaneous malignancy. Immunity 2008, 28, 571–580. [Google Scholar] [CrossRef]
- Pardee, A.D.; Shi, J.; Butterfield, L.H. Tumor-derived α-fetoprotein impairs the differentiation and T cell stimulatory activity of human dendritic cells. J. Immunol. 2014, 193, 5723–5732. [Google Scholar] [CrossRef]
- Ruiz de Galarreta, M.; Bresnahan, E.; Molina-Sánchez, P.; Lindblad, K.E.; Maier, B.; Sia, D.; Puigvehi, M.; Miguela, V.; Casanova-Acebes, M.; Dhainaut, M.; et al. β-Catenin Activation Promotes Immune Escape and Resistance to Anti-PD-1 Therapy in Hepatocellular Carcinoma. Cancer Discov. 2019, 9, 1124–1141. [Google Scholar] [CrossRef]
- Ryu, T.; Takami, Y.; Wada, Y.; Tateishi, M.; Matsushima, H.; Mikagi, K.; Saitsu, H. Double- and Triple-Positive Tumor Markers Predict Early Recurrence and Poor Survival in Patients with Hepatocellular Carcinoma within the Milan Criteria and Child-Pugh Class A. J. Gastrointest. Surg. 2017, 21, 957–966. [Google Scholar] [CrossRef]
- Kiriyama, S.; Uchiyama, K.; Ueno, M.; Ozawa, S.; Hayami, S.; Tani, M.; Yamaue, H. Triple positive tumor markers for hepatocellular carcinoma are useful predictors of poor survival. Ann. Surg. 2011, 254, 984–991. [Google Scholar] [CrossRef]
- Hiraoka, A.; Michitaka, K.; Kumada, T.; Izumi, N.; Kadoya, M.; Kokudo, N.; Kubo, S.; Matsuyama, Y.; Nakashima, O.; Sakamoto, M.; et al. Prediction of Prognosis of Intermediate-Stage HCC Patients: Validation of the Tumor Marker Score in a Nationwide Database in Japan. Liver Cancer 2019, 8, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Ishimaru, Y.; Kawasaki, H.; Aibiki, T.; Okudaira, T.; Toshimori, A.; Kawamura, T.; Yamago, H.; Nakahara, H.; Suga, Y.; et al. Tumor Markers AFP, AFP-L3, and DCP in Hepatocellular Carcinoma Refractory to Transcatheter Arterial Chemoembolization. Oncology 2015, 89, 167–174. [Google Scholar] [CrossRef]
- Ueno, M.; Hayami, S.; Shigekawa, Y.; Kawai, M.; Hirono, S.; Okada, K.; Tamai, H.; Shingaki, N.; Mori, Y.; Ichinose, M.; et al. Prognostic impact of surgery and radiofrequency ablation on single nodular HCC ≤ 5 cm: Cohort study based on serum HCC markers. J. Hepatol. 2015, 63, 1352–1359. [Google Scholar] [CrossRef]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Hiraoka, A.; Michitaka, K.; Kumada, T.; Izumi, N.; Kadoya, M.; Kokudo, N.; Kubo, S.; Matsuyama, Y.; Nakashima, O.; Sakamoto, M.; et al. Validation and Potential of Albumin-Bilirubin Grade and Prognostication in a Nationwide Survey of 46,681 Hepatocellular Carcinoma Patients in Japan: The Need for a More Detailed Evaluation of Hepatic Function. Liver Cancer 2017, 6, 325–336. [Google Scholar] [CrossRef]
- Kokudo, N.; Takemura, N.; Hasegawa, K.; Takayama, T.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Izumi, N.; Kaneko, S.; et al. Clinical practice guidelines for hepatocellular carcinoma: The Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol. Res. 2019, 49, 1109–1113. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Seymour, L.; Litière, S.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Standardisation and disease-specific adaptations: Perspectives from the RECIST Working Group. Eur. J. Cancer 2016, 62, 138–145. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Peng, S.Y.; Chen, W.J.; Lai, P.L.; Jeng, Y.M.; Sheu, J.C.; Hsu, H.C. High alpha-fetoprotein level correlates with high stage, early recurrence and poor prognosis of hepatocellular carcinoma: Significance of hepatitis virus infection, age, p53 and beta-catenin mutations. Int. J. Cancer 2004, 112, 44–50. [Google Scholar] [CrossRef]
- Galle, P.R.; Foerster, F.; Kudo, M.; Chan, S.L.; Llovet, J.M.; Qin, S.; Schelman, W.R.; Chintharlapalli, S.; Abada, P.B.; Sherman, M.; et al. Biology and significance of alpha-fetoprotein in hepatocellular carcinoma. Liver Int. 2019, 39, 2214–2229. [Google Scholar] [CrossRef]
- Kobayashi, M.; Hosaka, T.; Ikeda, K.; Seko, Y.; Kawamura, Y.; Sezaki, H.; Akuta, N.; Suzuki, F.; Suzuki, Y.; Saitoh, S.; et al. Highly sensitive AFP-L3% assay is useful for predicting recurrence of hepatocellular carcinoma after curative treatment pre- and postoperatively. Hepatol. Res. 2011, 41, 1036–1045. [Google Scholar] [CrossRef]
- Farinati, F.; Marino, D.; De Giorgio, M.; Baldan, A.; Cantarini, M.; Cursaro, C.; Rapaccini, G.; Del Poggio, P.; Di Nolfo, M.A.; Benvegnù, L.; et al. Diagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: Both or neither? Am. J. Gastroenterol. 2006, 101, 524–532. [Google Scholar] [CrossRef]
- Imamura, H.; Matsuyama, Y.; Miyagawa, Y.; Ishida, K.; Shimada, R.; Miyagawa, S.; Makuuchi, M.; Kawasaki, S. Prognostic significance of anatomical resection and des-gamma-carboxy prothrombin in patients with hepatocellular carcinoma. Br. J. Surg. 1999, 86, 1032–1038. [Google Scholar] [CrossRef]
- Fujiyama, S.; Tanaka, M.; Maeda, S.; Ashihara, H.; Hirata, R.; Tomita, K. Tumor markers in early diagnosis, follow-up and management of patients with hepatocellular carcinoma. Oncology 2002, 62 (Suppl. 1), 57–63. [Google Scholar] [CrossRef]
- Shimada, M.; Takenaka, K.; Fujiwara, Y.; Gion, T.; Kajiyama, K.; Maeda, T.; Shirabe, K.; Sugimachi, K. Des-gamma-carboxy prothrombin and alpha-fetoprotein positive status as a new prognostic indicator after hepatic resection for hepatocellular carcinoma. Cancer 1996, 78, 2094–2100. [Google Scholar] [CrossRef]
- Miyaaki, H.; Nakashima, O.; Kurogi, M.; Eguchi, K.; Kojiro, M. Lens culinaris agglutinin-reactive alpha-fetoprotein and protein induced by vitamin K absence II are potential indicators of a poor prognosis: A histopathological study of surgically resected hepatocellular carcinoma. J. Gastroenterol. 2007, 42, 962–968. [Google Scholar] [CrossRef]
- Gao, Q.; Qiu, S.J.; Fan, J.; Zhou, J.; Wang, X.Y.; Xiao, Y.S.; Xu, Y.; Li, Y.W.; Tang, Z.Y. Intratumoral balance of regulatory and cytotoxic T cells is associated with prognosis of hepatocellular carcinoma after resection. J. Clin. Oncol. 2007, 25, 2586–2593. [Google Scholar] [CrossRef]
- Ahn, K.S.; O’Brien, D.R.; Kim, Y.H.; Kim, T.S.; Yamada, H.; Park, J.W.; Park, S.J.; Kim, S.H.; Zhang, C.; Li, H.; et al. Associations of Serum Tumor Biomarkers with Integrated Genomic and Clinical Characteristics of Hepatocellular Carcinoma. Liver Cancer 2021, 10, 593–605. [Google Scholar] [CrossRef]
- Spranger, S.; Bao, R.; Gajewski, T.F. Melanoma-intrinsic β-catenin signalling prevents anti-tumour immunity. Nature 2015, 523, 231–235. [Google Scholar] [CrossRef]
- Kudo, M.; Han, K.H.; Ye, S.L.; Zhou, J.; Huang, Y.H.; Lin, S.M.; Wang, C.K.; Ikeda, M.; Chan, S.L.; Choo, S.P.; et al. A Changing Paradigm for the Treatment of Intermediate-Stage Hepatocellular Carcinoma: Asia-Pacific Primary Liver Cancer Expert Consensus Statements. Liver Cancer 2020, 9, 245–260. [Google Scholar] [CrossRef]
- Bonnel, A.R.; Bunchorntavakul, C.; Reddy, K.R. Immune dysfunction and infections in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2011, 9, 727–738. [Google Scholar] [CrossRef]
- Kudo, M.; Matsui, O.; Izumi, N.; Kadoya, M.; Okusaka, T.; Miyayama, S.; Yamakado, K.; Tsuchiya, K.; Ueshima, K.; Hiraoka, A.; et al. Transarterial chemoembolization failure/refractoriness: JSH-LCSGJ criteria 2014 update. Oncology 2014, 87 (Suppl. 1), 22–31. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Pfister, D.; Núñez, N.G.; Pinyol, R.; Govaere, O.; Pinter, M.; Szydlowska, M.; Gupta, R.; Qiu, M.; Deczkowska, A.; Weiner, A.; et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature 2021, 592, 450–456. [Google Scholar] [CrossRef]
- Hatanaka, T.; Kakizaki, S.; Hiraoka, A.; Tada, T.; Hirooka, M.; Kariyama, K.; Tani, J.; Atsukawa, M.; Takaguchi, K.; Itobayashi, E.; et al. Comparative efficacy and safety of atezolizumab and bevacizumab between hepatocellular carcinoma patients with viral and non-viral infection: A Japanese multicenter observational study. Cancer Med. 2023, 12, 5293–5303. [Google Scholar] [CrossRef]
- Espinoza, M.; Muquith, M.; Lim, M.; Zhu, H.; Singal, A.G.; Hsiehchen, D. Disease Etiology and Outcomes after Atezolizumab plus Bevacizumab in Hepatocellular Carcinoma: Post-Hoc Analysis of IMbrave150. Gastroenterology 2023, 165, 286–288.e284. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall Patients | 0 Points | 1 Point | 2 Points | 3 Points | p-Value |
|---|---|---|---|---|---|---|
| Age, yrs * | 74 [69, 81] | 75 [70, 80] | 74 [69, 79] | 74 [69, 81] | 75 [69, 81] | 0.827 |
| Gender, male: female | 291:80 | 62:19 | 87:23 | 88:24 | 54:14 | 0.971 |
| BMI, kg/m2 * | 23.6 [21.2, 26.1] | 24.5 [22.0, 26.5] | 23.7 [21.1, 26.3] | 23.2 [21.2, 26.1] | 23.1 [20.6, 24.9] | 0.170 |
| ECOG PS | 0.063 | |||||
| 0 | 300 (80.9) | 69 (85.2) | 97 (88.2) | 88 (78.6) | 46 (67.6) | |
| 1 | 55 (14.8) | 10 (12.3) | 12 (10.9) | 17 (15.2) | 16 (23.5) | |
| ≧2 | 16 (4.3) | 0 | 1 (0.9) | 7 (6.3) | 6 (8.9) | |
| Etiology of liver disease | 0.320 | |||||
| HBV | 128 (34.5) | 31 (38.3) | 36 (32.7) | 39 (34.8) | 22 (32.4) | |
| HCV | 52 (14.0) | 11 (13.6) | 17 (15.5) | 18 (16.1) | 6 (8.8) | |
| Alcohol | 76 (20.5) | 14 (17.3) | 27 (24.5) | 15 (13.4) | 20 (29.4) | |
| NASH | 29 (7.8) | 6 (7.4) | 8 (7.3) | 13 (11.6) | 2 (2.9) | |
| Others | 115 (31.0) | 25 (30.9) | 30 (27.3) | 40 (35.7) | 20 (29.4) | |
| BCLC stage | 0.022 | |||||
| Very early (0) | 4 (1.1) | 1 (1.2) | 0 | 2 (1.8) | 1 (1.5) | |
| Early (A) | 18 (4.9) | 6 (7.4) | 7 (6.4) | 3 (2.7) | 2 (2.9) | |
| Intermediate (B) | 142 (38.3) | 37 (45.7) | 52 (47.3) | 35 (31.2) | 18 (26.5) | |
| Advanced (C) | 196 (52.8) | 35 (43.2) | 50 (45.5) | 69 (61.6) | 42 (61.8) | |
| Terminal (D) | 11 (3.0) | 2 (2.5) | 1 (0.9) | 3 (2.7) | 5 (7.4) | |
| Child–Pugh score, n (%) | 0.003 | |||||
| 5 | 225 (60.6) | 52 | 77 | 65 | 32 | |
| 6 | 103 (27.8) | 25 | 24 | 33 | 20 | |
| ≧7 | 43 (11.6) | 4 | 9 | 14 | 16 | |
| ALBI score * | −2.47 [−3.47, −0.81] | −2.60 [−2.95, −2.34] | −2.49 [−2.74, −2.20] | −2.40 [−2.68, −2.06] | −2.23 [−2.61, −1.92] | <0.001 |
| mALBI grade, n (%) | 0.006 | |||||
| 1 | 144 (38.8) | 41 (50.6) | 45 (40.9) | 39 (34.8) | 19 (27.9) | |
| 2a | 93 (25.1) | 25 (30.9) | 25 (22.7) | 29 (25.9) | 14 (20.6) | |
| 2b | 126 (34.0) | 15 (18.5) | 39 (35.5) | 39 (34.8) | 33 (48.5) | |
| 3 | 8 (2.2) | 0 | 1 (0.9) | 5 (4.5) | 2 (2.9) | |
| Serum albumin (g/dL) * | 3.8 [3.4, 4.1] | 4.0 [3.6, 4.3] | 3.8 [3.5, 4.1] | 3.8 [3.4, 4.1] | 3.6 [3.2, 3.9] | 0.001 |
| Total bilirubin (mg/dL) * | 0.8 [0.6, 1.1] | 0.7 [0.5, 1.0] | 0.8 [0.6, 1.1] | 0.8 [0.6, 1.1] | 0.9 [0.7, 1.3] | 0.002 |
| Platelet count (109/L) * | 13.7 [10.2, 18.9] | 13.4 [10.4, 18.7] | 13.0 [10.5, 17.4] | 13.8 [10.1, 19.5] | 15.6 [10.3, 22.9] | 0.216 |
| Prothrombin time (%) * | 88.0 [77.4, 99.0] | 89.4 [84.9, 99.5] | 91.0 [80.0, 100.0] | 86.7 [77.0, 97.3] | 83.5 [72.9, 97.0] | 0.041 |
| Extrahepatic spread, n (%) | 110 (29.6%) | 26 (32.1) | 30 (27.3) | 37 (33.0) | 17 (25.0) | 0.604 |
| Macrovascular invasion, n (%) | 59 (15.9) | 3 (3.7) | 11 (10.0) | 22 (19.6) | 23 (33.8) | <0.001 |
| AFP ≧ 100 ng/mL, n (%) | 130 (35.0) | 0 (0) | 7 (6.4) | 55 (49.1) | 68 (100) | <0.001 |
| AFP-L3 ≧ 10%, n (%) | 187 (50.4) | 0 (0) | 33 (30.0) | 86 (76.8) | 68 (100) | <0.001 |
| DCP ≧ 100 mAU/mL | 221 (59.6) | 0 (0) | 70 (63.6) | 83 (74.1) | 68 (100) | <0.001 |
| OS | PFS | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| AFP ≥ 100 ng/mL | 1.890 | 1.289–2.772 | 0.001 | 1.865 | 1.393–2.496 | <0.001 |
| AFP-L3 ≥ 10% | 1.928 | 1.301–2.857 | 0.001 | 1.227 | 0.920–1.635 | 0.164 |
| DCP ≥ 100 mAU/mL | 1.915 | 1.264–2.901 | 0.002 | 1.636 | 1.208–2.215 | 0.001 |
| Tumor marker score | ||||||
| 0 | 1.0 | 1.0 | ||||
| 1 | 2.525 | 1.205–5.294 | 0.014 | 1.022 | 0.661–1.581 | 0.923 |
| 2 | 3.796 | 1.834–7.857 | <0.001 | 1.595 | 1.044–2.437 | 0.031 |
| 3 | 4.977 | 2.338–10.60 | <0.001 | 2.345 | 1.495–3.677 | <0.001 |
| 0 Points | 1 Point | 2 Points | 3 Points | p-Value | |
|---|---|---|---|---|---|
| Radiological response, n (%) | 0.136 | ||||
| CR | 5 (6.9) | 7 (6.7) | 3 (2.9) | 2 (3.3) | |
| PR | 18 (25.0) | 24 (22.9) | 33 (32.4) | 12 (19.7) | |
| SD | 35 (48.6) | 62 (59.0) | 45 (44.1) | 30 (49.2) | |
| PD | 14 (19.4) | 12 (11.4) | 21 (20.6) | 17 (27.9) | |
| ORR, n (%) | 23 (31.9) | 31 (29.5) | 36 (35.3) | 14 (23.0) | 0.416 |
| DCR, n (%) | 58 (80.6) | 93 (88.6) | 81 (79.4) | 44 (72.1) | 0.058 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age | 1.035 | 1.011–1.060 | 0.004 | 1.037 | 1.013–1.061 | 0.002 |
| Gender (=Female) | 0.772 | 0.469–1.268 | 0.307 | |||
| Etiology (=viral) | 1.024 | 0.916–1.145 | 0.675 | |||
| mALBI grade ≥ 2b | 2.804 | 1.908–4.120 | <0.001 | 2.560 | 1.736–3.774 | <0.001 |
| BCLC stage | 1.514 | 1.106–2.073 | 0.009 | 1.237 | 0.909–1.684 | 0.176 |
| Tumor marker score | 1.586 | 1.307–1.924 | <0.001 | 1.480 | 1.210–1.812 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, K.; Tsuji, K.; Hiraoka, A.; Tada, T.; Hirooka, M.; Kariyama, K.; Tani, J.; Atsukawa, M.; Takaguchi, K.; Itobayashi, E.; et al. Usefulness of Tumor Marker Score for Predicting the Prognosis of Hepatocellular Carcinoma Patients Treated with Atezolizumab Plus Bevacizumab: A Multicenter Retrospective Study. Cancers 2023, 15, 4348. https://doi.org/10.3390/cancers15174348
Tanaka K, Tsuji K, Hiraoka A, Tada T, Hirooka M, Kariyama K, Tani J, Atsukawa M, Takaguchi K, Itobayashi E, et al. Usefulness of Tumor Marker Score for Predicting the Prognosis of Hepatocellular Carcinoma Patients Treated with Atezolizumab Plus Bevacizumab: A Multicenter Retrospective Study. Cancers. 2023; 15(17):4348. https://doi.org/10.3390/cancers15174348
Chicago/Turabian StyleTanaka, Kazunari, Kunihiko Tsuji, Atsushi Hiraoka, Toshifumi Tada, Masashi Hirooka, Kazuya Kariyama, Joji Tani, Masanori Atsukawa, Koichi Takaguchi, Ei Itobayashi, and et al. 2023. "Usefulness of Tumor Marker Score for Predicting the Prognosis of Hepatocellular Carcinoma Patients Treated with Atezolizumab Plus Bevacizumab: A Multicenter Retrospective Study" Cancers 15, no. 17: 4348. https://doi.org/10.3390/cancers15174348
APA StyleTanaka, K., Tsuji, K., Hiraoka, A., Tada, T., Hirooka, M., Kariyama, K., Tani, J., Atsukawa, M., Takaguchi, K., Itobayashi, E., Fukunishi, S., Ishikawa, T., Tajiri, K., Ochi, H., Toyoda, H., Ogawa, C., Nishimura, T., Hatanaka, T., Kakizaki, S., ... Kumada, T., on behalf of the Real-life Practice Experts for HCC (RELPEC) Study Group and HCC 48 Group. (2023). Usefulness of Tumor Marker Score for Predicting the Prognosis of Hepatocellular Carcinoma Patients Treated with Atezolizumab Plus Bevacizumab: A Multicenter Retrospective Study. Cancers, 15(17), 4348. https://doi.org/10.3390/cancers15174348