
Gene Expressions and High Lymphocyte Count May Predict Durable Clinical Benefits in Patients with Advanced Non-Small-Cell Lung Cancer Treated with Immune Checkpoint Inhibitors
 ,
,  , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Data Collection and Data Management
2.3. Tissue Samples and Routine Diagnostics
2.4. Gene Expression Profiling
2.5. Next Generation Sequencing
2.6. Statistical Analyses
2.6.1. Descriptive Statistics, Logistic Regression, and Survival Analyses
2.6.2. Bioinformatics
Differential Expression of Genes
Gene Expression Signatures
3. Results
3.1. Baseline Patient Characteristics
3.2. Treatment Characteristics
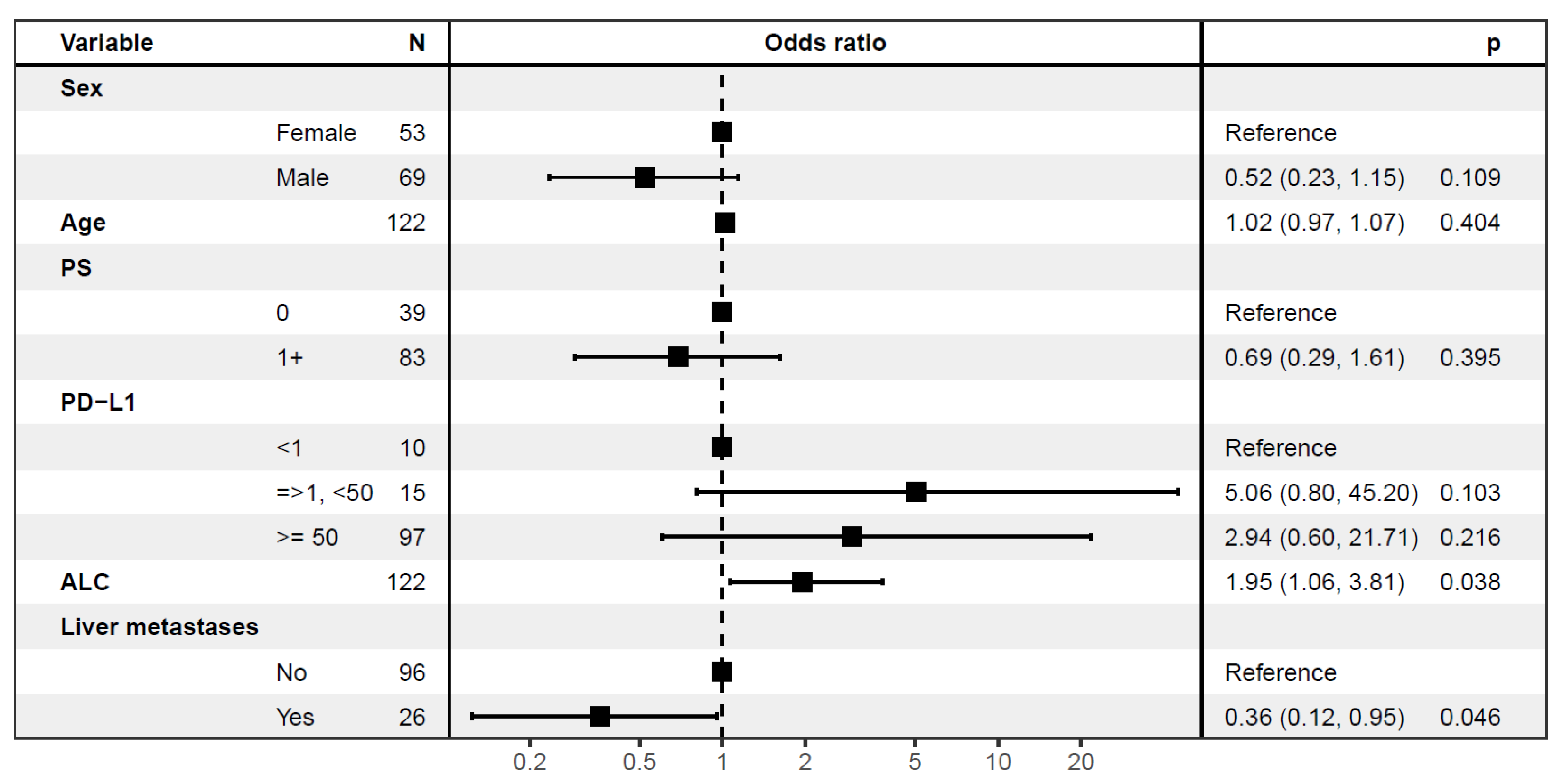
3.3. Predictive Factors of Durable Clinical Benefit
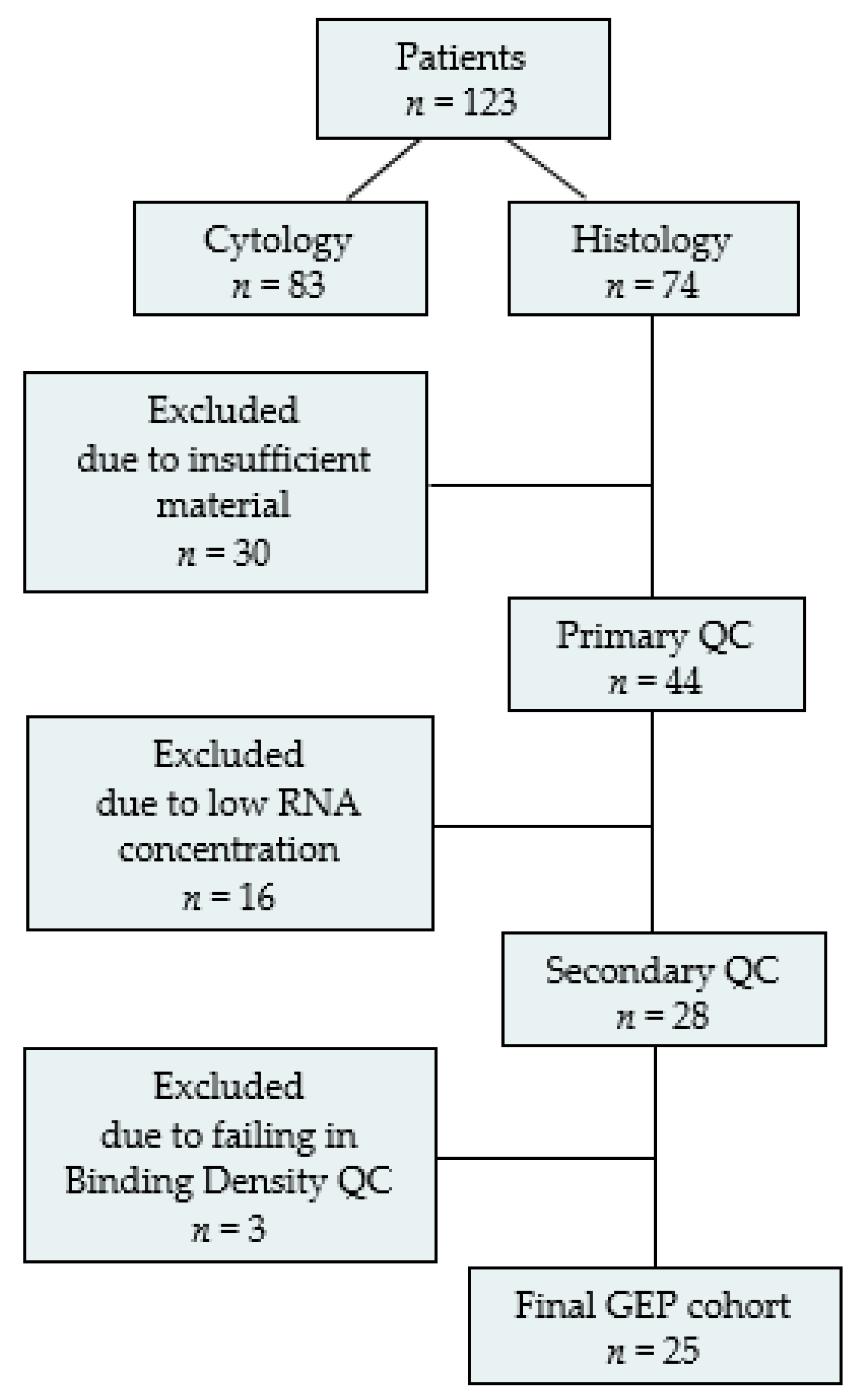
3.4. The GEP Subpopulation
3.4.1. Treatment Characteristics and Clinical Outcomes
3.4.2. Gene Expression Analyses
3.5. Next Generation Sequencing
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crino, L.; Eberhardt, W.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Perez-Gracia, J.L.; Han, J.Y. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2015, 387, 1540–1550. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet J. Transl. Name Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Gettinger, S.; Horn, L.; Jackman, D.; Spigel, D.; Antonia, S.; Hellmann, M.; Powderly, J.; Heist, R.; Sequist, L.V.; Smith, D.C.; et al. Five-Year Follow-Up of Nivolumab in Previously Treated Advanced Non-Small-Cell Lung Cancer: Results From the CA209-003 Study. J. Clin. Oncol. 2018, 36, 1675–1684. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes with Pembrolizumab Versus Chemotherapy for Metastatic Non-Small-Cell Lung Cancer with PD-L1 Tumor Proportion Score ≥ 50. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef]
- Mouritzen, M.T.; Carus, A.; Ladekarl, M.; Meldgaard, P.; Nielsen, A.W.M.; Livbjerg, A.; Larsen, J.W.; Skuladottir, H.; Kristiansen, C.; Wedervang, K.; et al. Nationwide Survival Benefit after Implementation of First-Line Immunotherapy for Patients with Advanced NSCLC-Real World Efficacy. Cancers 2021, 13, 4846. [Google Scholar] [CrossRef] [PubMed]
- DOLG. DOLG Referenceprogram Palliativ NSCLC. 2021. Available online: https://dolg.dk/index.php/palliativ-behandling-ikke-smaacellet-lungekraeft/ (accessed on 5 September 2023).
- Aguilar, E.J.; Ricciuti, B.; Gainor, J.F.; Kehl, K.L.; Kravets, S.; Dahlberg, S.; Nishino, M.; Sholl, L.M.; Adeni, A.; Subegdjo, S.; et al. Outcomes to first-line pembrolizumab in patients with non-small-cell lung cancer and very high PD-L1 expression. Ann. Oncol. 2019, 30, 1653–1659. [Google Scholar] [CrossRef]
- Lemery, S.; Keegan, P.; Pazdur, R. First FDA approval Agnostic of Cancer Site—When a Biomarker Defines the Indication. N. Engl. J. Med. 2017, 377, 1409–1412. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. FDA Approves Pembrolizumab for Adults and Children with TMB-H Solid Tumors. Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pembrolizumab-adults-and-children-tmb-h-solid-tumors (accessed on 5 September 2023).
- Stenzinger, A.; Endris, V.; Budczies, J.; Merkelbach-Bruse, S.; Kazdal, D.; Dietmaier, W.; Pfarr, N.; Siebolts, U.; Hummel, M.; Herold, S.; et al. Harmonization and Standardization of Panel-Based Tumor Mutational Burden Measurement: Real-World Results and Recommendations of the Quality in Pathology Study. J. Thorac. Oncol. 2020, 15, 1177–1189. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Bibeau, F.; Ligtenberg, M.J.L.; Singh, N.; Nottegar, A.; Bosse, T.; Miller, R.; Riaz, N.; Douillard, J.Y.; Andre, F.; et al. ESMO recommendations on microsatellite instability testing for immunotherapy in cancer, and its relationship with PD-1/PD-L1 expression and tumour mutational burden: A systematic review-based approach. Ann. Oncol. 2019, 30, 1232–1243. [Google Scholar] [CrossRef]
- Vanderwalde, A.; Spetzler, D.; Xiao, N.; Gatalica, Z.; Marshall, J. Microsatellite instability status determined by next-generation sequencing and compared with PD-L1 and tumor mutational burden in 11,348 patients. Cancer Med. 2018, 7, 746–756. [Google Scholar] [CrossRef]
- Hause, R.J.; Pritchard, C.C.; Shendure, J.; Salipante, S.J. Classification and characterization of microsatellite instability across 18 cancer types. Nat. Med. 2016, 22, 1342. [Google Scholar] [CrossRef] [PubMed]
- Lopez de Rodas, M.; Nagineni, V.; Ravi, A.; Datar, I.J.; Mino-Kenudson, M.; Corredor, G.; Barrera, C.; Behlman, L.; Rimm, D.L.; Herbst, R.S.; et al. Role of tumor infiltrating lymphocytes and spatial immune heterogeneity in sensitivity to PD-1 axis blockers in non-small cell lung cancer. J. Immunother. Cancer 2022, 10, e004440. [Google Scholar] [CrossRef] [PubMed]
- Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-γ–related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef]
- Danaher, P.; Warren, S.; Lu, R.; Samayoa, J.; Sullivan, A.; Pekker, I.; Wallden, B.; Marincola, F.M.; Cesano, A. Pan-cancer adaptive immune resistance as defined by the Tumor Inflammation Signature (TIS): Results from The Cancer Genome Atlas (TCGA). J. Immunother. Cancer 2018, 6, 63. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- McDermott, D.F.; Huseni, M.A.; Atkins, M.B.; Motzer, R.J.; Rini, B.I.; Escudier, B.; Fong, L.; Joseph, R.W.; Pal, S.K.; Reeves, J.A.; et al. Clinical activity and molecular correlates of response to atezolizumab alone or in combination with bevacizumab versus sunitinib in renal cell carcinoma. Nat. Med. 2018, 24, 749–757. [Google Scholar] [CrossRef]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2 trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef]
- Kowanetz, M.; Zou, W.; Gettinger, S.N.; Koeppen, H.; Kockx, M.; Schmid, P.; Kadel, E.E., 3rd; Wistuba, I.; Chaft, J.; Rizvi, N.A.; et al. Differential regulation of PD-L1 expression by immune and tumor cells in NSCLC and the response to treatment with atezolizumab (anti-PD-L1). Proc. Natl. Acad. Sci. USA 2018, 115, E10119–E10126. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, K.E.; Karlsson, A.; Leveen, P.; Brunnstrom, H.; Reutersward, C.; Holm, K.; Jonsson, M.; Annersten, K.; Rosengren, F.; Jirstrom, K.; et al. Clinical framework for next generation sequencing based analysis of treatment predictive mutations and multiplexed gene fusion detection in non-small cell lung cancer. Oncotarget 2017, 8, 34796–34810. [Google Scholar] [CrossRef] [PubMed]
- Mezquita, L.; Auclin, E.; Ferrara, R.; Charrier, M.; Remon, J.; Planchard, D.; Ponce, S.; Ares, L.P.; Leroy, L.; Audigier-Valette, C.; et al. Association of the Lung Immune Prognostic Index with Immune Checkpoint Inhibitor Outcomes in Patients with Advanced Non-Small Cell Lung Cancer. JAMA Oncol. 2018, 4, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Tanizaki, J.; Haratani, K.; Hayashi, H.; Chiba, Y.; Nakamura, Y.; Yonesaka, K.; Kudo, K.; Kaneda, H.; Hasegawa, Y.; Tanaka, K.; et al. Peripheral Blood Biomarkers Associated with Clinical Outcome in Non-Small Cell Lung Cancer Patients Treated with Nivolumab. J. Thorac. Oncol. 2018, 13, 97–105. [Google Scholar] [CrossRef]
- Cortellini, A.; Ricciuti, B.; Borghaei, H.; Naqash, A.R.; D’Alessio, A.; Fulgenzi, C.A.M.; Addeo, A.; Banna, G.L.; Pinato, D.J. Differential prognostic effect of systemic inflammation in patients with non-small cell lung cancer treated with immunotherapy or chemotherapy: A post hoc analysis of the phase 3 OAK trial. Cancer 2022, 128, 3067–3079. [Google Scholar] [CrossRef]
- Lee, Y.J.; Park, Y.S.; Lee, H.W.; Park, T.Y.; Lee, J.K.; Heo, E.Y. Peripheral lymphocyte count as a surrogate marker of immune checkpoint inhibitor therapy outcomes in patients with non-small-cell lung cancer. Sci. Rep. 2022, 12, 626. [Google Scholar] [CrossRef]
- Bourbonne, V.; Geier, M.; Schick, U.; Lucia, F. Multi-Omics Approaches for the Prediction of Clinical Endpoints after Immunotherapy in Non-Small Cell Lung Cancer: A Comprehensive Review. Biomedicines 2022, 10, 1237. [Google Scholar] [CrossRef]
- Ricciuti, B.; Wang, X.; Alessi, J.V.; Rizvi, H.; Mahadevan, N.R.; Li, Y.Y.; Polio, A.; Lindsay, J.; Umeton, R.; Sinha, R.; et al. Association of High Tumor Mutation Burden in Non-Small Cell Lung Cancers with Increased Immune Infiltration and Improved Clinical Outcomes of PD-L1 Blockade Across PD-L1 Expression Levels. JAMA Oncol. 2022, 8, 1160–1168. [Google Scholar] [CrossRef]
- Karasaki, T.; Nagayama, K.; Kuwano, H.; Nitadori, J.I.; Sato, M.; Anraku, M.; Hosoi, A.; Matsushita, H.; Morishita, Y.; Kashiwabara, K.; et al. An Immunogram for the Cancer-Immunity Cycle: Towards Personalized Immunotherapy of Lung Cancer. J. Thorac. Oncol. 2017, 12, 791–803. [Google Scholar] [CrossRef]
- Danske Regioner, Koordineringsrådet for Ibrugtagning af Sygehusmedicin (KRIS). Lung Cancer Treatment-Approvals from Danish Authorities. Available online: https://www.regioner.dk/kris/anbefalinger (accessed on 5 September 2023).
- Danske Regioner, Medicinrådet. Available online: https://medicinraadet.dk/media/gbjmlljl/medicinraadets-anbefaling-vedr-atezolizumab-nsclc-vers-1-0_adlegacy.pdf (accessed on 5 September 2023).
- Garon, E.B.; Rizvi, N.A.; Hui, R.; Leighl, N.; Balmanoukian, A.S.; Eder, J.P.; Patnaik, A.; Aggarwal, C.; Gubens, M.; Horn, L.; et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N. Engl. J. Med. 2015, 372, 2018–2028. [Google Scholar] [CrossRef]
- Illumina. TruSight™ Oncology 500 Datasheet. Available online: https://emea.illumina.com/content/dam/illumina/gcs/assembled-assets/marketing-literature/trusight-oncology-500-data-sheet-m-gl-00173/trusight-oncology-500-and-ht-data-sheet-m-gl-00173.pdf (accessed on 5 September 2023).
- Illumina. Local Run Manager TruSight Oncology 500 v2.2 Analysis Module. Available online: https://support.illumina.com/content/dam/illumina-support/documents/documentation/software_documentation/trusight/trusight-oncology-500/local-run-manager-trusight-tumor-oncology-500-v2.2-workflow-guide-1000000151997-01.pdf (accessed on 5 September 2023).
- Hollander, M.; Eric Chicken Douglas, A. Wolfe Nonparametric Statistical Methods, 3rd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014. [Google Scholar]
- The R Project for Statistical Computing. R: A Language and Environment for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 5 September 2023).
- Ritchie, M.E.; Phipson, B.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.D.; McCarthy, D.J.; Smyth, G.K. edgeR: A Bioconductor package for differential expression analysis of digital gene expression data. Bioinformatics 2010, 26, 139–140. [Google Scholar] [CrossRef]
- Gu, Z.; Eils, R.; Schlesner, M. Complex heatmaps reveal patterns and correlations in multidimensional genomic data. Bioinformatics 2016, 32, 2847–2849. [Google Scholar] [CrossRef] [PubMed]
- Poma, A.M.; Bruno, R.; Pietrini, I.; Alì, G.; Pasquini, G.; Proietti, A.; Vasile, E.; Cappelli, S.; Chella, A.; Fontanini, G. Biomarkers and Gene Signatures to Predict Durable Response to Pembrolizumab in Non-Small Cell Lung Cancer. Cancers 2021, 13, 3828. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Kwon, A.Y.; Jeong, J.Y.; Kim, S.; Kang, H.; Park, J.; Kim, J.H.; Han, O.J.; Lim, S.M.; An, H.J. Immune gene signatures for predicting durable clinical benefit of anti-PD-1 immunotherapy in patients with non-small cell lung cancer. Sci. Rep. 2020, 10, 643. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Q.; Yu, X.; Shuai, Z.; Yao, T.; Yang, X.; Zhang, Y. The influence of baseline characteristics on the efficacy of immune checkpoint inhibitors for advanced lung cancer: A systematic review and meta-analysis. Front. Pharmacol. 2022, 13, 956788. [Google Scholar] [CrossRef]
- Passaro, A.; Attili, I.; Morganti, S.; Del Signore, E.; Gianoncelli, L.; Spitaleri, G.; Stati, V.; Catania, C.; Curigliano, G.; de Marinis, F. Clinical features affecting survival in metastatic NSCLC treated with immunotherapy: A critical review of published data. Cancer Treat. Rev. 2020, 89, 102085. [Google Scholar] [CrossRef]
- Mouritzen, M.T.; Junker, K.F.; Carus, A.; Ladekarl, M.; Meldgaard, P.; Nielsen, A.W.M.; Livbjerg, A.; Larsen, J.W.; Skuladottir, H.; Kristiansen, C.; et al. Clinical features affecting efficacy of immune checkpoint inhibitors in pretreated patients with advanced NSCLC: A Danish nationwide real-world study. Acta Oncol. 2022, 61, 409–416. [Google Scholar] [CrossRef]
- Conway, J.W.; Rawson, R.V.; Lo, S.; Ahmed, T.; Vergara, I.A.; Gide, T.N.; Attrill, G.H.; Carlino, M.S.; Saw, R.P.M.; Thompson, J.F.; et al. Unveiling the tumor immune microenvironment of organ-specific melanoma metastatic sites. J. Immunother. Cancer 2022, 10, e004884. [Google Scholar] [CrossRef]
- Xie, M.; Li, N.; Xu, X.; Xu, Y.; Li, H.; Zhu, L.; Sheng, J.; Zhou, Z.; Fan, Y. The Efficacy of PD-1/PD-L1 Inhibitors in Patients with Liver Metastasis of Non-Small Cell Lung Cancer: A Real-World Study. Cancers 2022, 14, 4333. [Google Scholar] [CrossRef]
- Cho, Y.; Park, S.; Byun, H.K.; Lee, C.G.; Cho, J.; Hong, M.H.; Kim, H.R.; Cho, B.C.; Kim, S.; Park, J.; et al. Impact of Treatment-Related Lymphopenia on Immunotherapy for Advanced Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Ottonello, S.; Genova, C.; Cossu, I.; Fontana, V.; Rijavec, E.; Rossi, G.; Biello, F.; Dal Bello, M.G.; Tagliamento, M.; Alama, A.; et al. Association Between Response to Nivolumab Treatment and Peripheral Blood Lymphocyte Subsets in Patients with Non-small Cell Lung Cancer. Front. Immunol. 2020, 11, 125. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Li, L.; Luo, W.; Yang, Y.; Ni, Y.; Song, T.; Zhu, Y.; Yang, Y.; Zhang, L. Lymphocyte percentage as a valuable predictor of prognosis in lung cancer. J. Cell Mol. Med. 2022, 26, 1918–1931. [Google Scholar] [CrossRef]
- Jin, J.; Yang, L.; Liu, D.; Li, W. Association of the neutrophil to lymphocyte ratio and clinical outcomes in patients with lung cancer receiving immunotherapy: A meta-analysis. BMJ Open 2020, 10, e035031. [Google Scholar] [CrossRef]
- Wang, C.; Yu, Q.; Song, T.; Wang, Z.; Song, L.; Yang, Y.; Shao, J.; Li, J.; Ni, Y.; Chao, N.; et al. The heterogeneous immune landscape between lung adenocarcinoma and squamous carcinoma revealed by single-cell RNA sequencing. Signal Transduct. Target. Ther. 2022, 7, 289. [Google Scholar] [CrossRef]
- Cooper, W.A.; Russell, P.A.; Cherian, M.; Duhig, E.E.; Godbolt, D.; Jessup, P.J.; Khoo, C.; Leslie, C.; Mahar, A.; Moffat, D.F.; et al. Intra- and Interobserver Reproducibility Assessment of PD-L1 Biomarker in Non-Small Cell Lung Cancer. Clin. Cancer Res. 2017, 23, 4569–4577. [Google Scholar] [CrossRef]
- Wessolly, M.; Stephan-Falkenau, S.; Streubel, A.; Wiesweg, M.; Borchert, S.; Mairinger, E.; Kollmeier, J.; Reis, H.; Bauer, T.; Schmid, K.W.; et al. Digital gene expression analysis of NSCLC-patients reveals strong immune pressure, resulting in an immune escape under immunotherapy. BMC Cancer 2022, 22, 46. [Google Scholar] [CrossRef] [PubMed]
- Moutafi, M.; Martinez-Morilla, S.; Divakar, P.; Vathiotis, I.; Gavrielatou, N.; Aung, T.N.; Yaghoobi, V.; Fernandez, A.I.; Zugazagoitia, J.; Herbst, R.S.; et al. Discovery of Biomarkers of Resistance to Immune Checkpoint Blockade in NSCLC Using High-Plex Digital Spatial Profiling. J. Thorac. Oncol. 2022, 17, 991–1001. [Google Scholar] [CrossRef]
- Aiba, T.; Hattori, C.; Sugisaka, J.; Shimizu, H.; Ono, H.; Domeki, Y.; Saito, R.; Kawana, S.; Kawashima, Y.; Terayama, K.; et al. Gene expression signatures as candidate biomarkers of response to PD-1 blockade in non-small cell lung cancers. PLoS ONE 2021, 16, e0260500. [Google Scholar] [CrossRef]
- NanoString Technologies Inc. nCounter Preparing RNA from FFPE Samples—User Manual. Available online: https://nanostring.com/wp-content/uploads/MAN-10050-05-Preparing-RNA-from-FFPE-Samples.pdf (accessed on 5 September 2023).
- Hirsch, F.R.; Walker, J.; Higgs, B.W.; Cooper, Z.A.; Raja, R.G.; Wistuba, I.I. The Combiome Hypothesis: Selecting Optimal Treatment for Cancer Patients. Clin. Lung Cancer 2022, 23, 1–13. [Google Scholar] [CrossRef]
- Amrein, M.A.; Bührer, E.D.; Amrein, M.L.; Li, Q.; Rothschild, S.; Riether, C.; Jaggi, R.; Savic-Prince, S.; Bubendorf, L.; Gautschi, O.; et al. Chemotherapy negatively impacts the tumor immune microenvironment in NSCLC: An analysis of pre- and post-treatment biopsies in the multi-center SAKK19/09 study. Cancer Immunol. Immunother. 2021, 70, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Higgs, B.W.; Morehouse, C.A.; Streicher, K.; Brohawn, P.Z.; Pilataxi, F.; Gupta, A.; Ranade, K. Interferon Gamma Messenger RNA Signature in Tumor Biopsies Predicts Outcomes in Patients with Non-Small Cell Lung Carcinoma or Urothelial Cancer Treated with Durvalumab. Clin. Cancer Res. 2018, 24, 3857–3866. [Google Scholar] [CrossRef] [PubMed]
- Giovanelli, P.; Sandoval, T.A.; Cubillos-Ruiz, J.R. Dendritic Cell Metabolism and Function in Tumors. Trends Immunol. 2019, 40, 699–718. [Google Scholar] [CrossRef] [PubMed]
- Zou, S.; Tong, Q.; Liu, B.; Huang, W.; Tian, Y.; Fu, X. Targeting STAT3 in Cancer Immunotherapy. Mol. Cancer 2020, 19, 145. [Google Scholar] [CrossRef]
- Mantovani, A.; Marchesi, F.; Jaillon, S.; Garlanda, C.; Allavena, P. Tumor-associated myeloid cells: Diversity and therapeutic targeting. Cell. Mol. Immunol. 2021, 18, 566–578. [Google Scholar] [CrossRef]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef]
- Neuzillet, C.; Tijeras-Raballand, A.; Cohen, R.; Cros, J.; Faivre, S.; Raymond, E.; de Gramont, A. Targeting the TGFβ pathway for cancer therapy. Pharmacol. Ther. 2015, 147, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Gulley, J.L.; Schlom, J.; Barcellos-Hoff, M.H.; Wang, X.J.; Seoane, J.; Audhuy, F.; Lan, Y.; Dussault, I.; Moustakas, A. Dual inhibition of TGF-β and PD-L1: A novel approach to cancer treatment. Mol. Oncol. 2022, 16, 2117–2134. [Google Scholar] [CrossRef]
- Goldstein, J.D.; Burlion, A.; Zaragoza, B.; Sendeyo, K.; Polansky, J.K.; Huehn, J.; Piaggio, E.; Salomon, B.L.; Marodon, G. Inhibition of the JAK/STAT Signaling Pathway in Regulatory T Cells Reveals a Very Dynamic Regulation of Foxp3 Expression. PLoS ONE 2016, 11, e0153682. [Google Scholar] [CrossRef]
- Seif, F.; Khoshmirsafa, M.; Aazami, H.; Mohsenzadegan, M.; Sedighi, G.; Bahar, M. The role of JAK-STAT signaling pathway and its regulators in the fate of T helper cells. Cell Commun. Signal. 2017, 15, 23. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | GEP n (%) | No GEP n (%) | Total n (%) | p-Value |
|---|---|---|---|---|
| Patients | 25 (20) | 98 (80) | 123 (100) | |
| Age, median years (range) | 68 (52–82) | 67 (46–86) | 67 (46–86) | 0.90 |
| Sex | ||||
| Male | 12 (48) | 57 (58) | 69 (56) | |
| Female | 13 (52) | 41 (42) | 54 (44) | 0.38 |
| Performance status | ||||
| 0 | 7 (28) | 32 (33) | 39 (32) | |
| 1 | 11 (44) | 53 (54) | 64 (52) | 0.23 |
| ≥2 | 7 (28) | 13 (13) | 20 (16) | |
| Smoking status | ||||
| Current | 9 (36) | 33 (34) | 42 (34) | |
| Former | 16 (64) | 63 (64) | 79 (64) | 1 |
| Never | 0 (0) | 2 (2) | 2 (2) | |
| BMI, median (range) | 25 (17–39) | 24 (16–41) | 24 (16–41) | 0.78 |
| TNM stage | ||||
| III | 3 (12) | 14 (14) | 17 (14) | |
| IV | 22 (88) | 84 (86) | 106 (86) | 1 |
| Metastatic sites a | ||||
| Brain | 3 (12) | 7 (7) | 10 (8) | 0.42 |
| Bone | 8 (32) | 25 (26) | 33 (27) | 0.61 |
| Liver | 8 (32) | 18 (18) | 26 (21) | 0.17 |
| Adrenal glands | 3 (12) | 27 (28) | 30 (24) | 0.12 |
| Distant lymph nodes | 5 (20) | 11 (11) | 16 (13) | 0.32 |
| Lung | 8 (32) | 25 (26) | 33 (27) | 0.61 |
| Pleura b | 7 (28) | 36 (37) | 43 (35) | 0.49 |
| Soft tissue c | 4 (4) | 4 (4) | 5 (4) | 1 |
| Other | 2 (8) | 22 (22) | 24 (20) | 0.16 |
| NSCLC subtype | ||||
| Adenocarcinoma | 12 (48) | 72 (74) | 84 (68) | |
| Squamous cell carcinoma | 12 (48) | 17 (17) | 29 (24) | 0.007 |
| Other d | 1 (4) | 9 (9) | 10 (8) | |
| PD-L1 | ||||
| <1% | 4 (16) | 6 (6) | 10 (8) | |
| ≥1% and <50% | 5 (20) | 10 (10) | 15 (12) | 0.08 |
| ≥50% | 16 (64) | 82 (84) | 98 (80) | |
| TMB | ||||
| High | 4 (16) | 20 (20) | 24 (20) | |
| Low | 2 (8) | 25 (26) | 27 (22) | 0.40 |
| Missing | 19 (76) | 53 (54) | 72 (58) | |
| Blood values, median (range) * | ||||
| ALC | 1.40 (0.30–3.15) | 1.36 (0.30–3.60) | 1.40 (0.30–3.60) | 0.83 |
| ANC | 7.30 (3.79–16.2) | 6.50 (2.90–36.3) | 6.70 (2.90–36.3) | 0.70 |
| NLR | 5.16 (1.50–37.7) | 4.31 (1.16–34.7) | 4.40 (1.16–37.7) | 0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mouritzen, M.T.; Ladekarl, M.; Hager, H.; Mattesen, T.B.; Lippert, J.B.; Frank, M.S.; Nøhr, A.K.; Egendal, I.B.; Carus, A. Gene Expressions and High Lymphocyte Count May Predict Durable Clinical Benefits in Patients with Advanced Non-Small-Cell Lung Cancer Treated with Immune Checkpoint Inhibitors. Cancers 2023, 15, 4480. https://doi.org/10.3390/cancers15184480
Mouritzen MT, Ladekarl M, Hager H, Mattesen TB, Lippert JB, Frank MS, Nøhr AK, Egendal IB, Carus A. Gene Expressions and High Lymphocyte Count May Predict Durable Clinical Benefits in Patients with Advanced Non-Small-Cell Lung Cancer Treated with Immune Checkpoint Inhibitors. Cancers. 2023; 15(18):4480. https://doi.org/10.3390/cancers15184480
Chicago/Turabian StyleMouritzen, Mette T., Morten Ladekarl, Henrik Hager, Trine B. Mattesen, Julie B. Lippert, Malene S. Frank, Anne K. Nøhr, Ida B. Egendal, and Andreas Carus. 2023. "Gene Expressions and High Lymphocyte Count May Predict Durable Clinical Benefits in Patients with Advanced Non-Small-Cell Lung Cancer Treated with Immune Checkpoint Inhibitors" Cancers 15, no. 18: 4480. https://doi.org/10.3390/cancers15184480
APA StyleMouritzen, M. T., Ladekarl, M., Hager, H., Mattesen, T. B., Lippert, J. B., Frank, M. S., Nøhr, A. K., Egendal, I. B., & Carus, A. (2023). Gene Expressions and High Lymphocyte Count May Predict Durable Clinical Benefits in Patients with Advanced Non-Small-Cell Lung Cancer Treated with Immune Checkpoint Inhibitors. Cancers, 15(18), 4480. https://doi.org/10.3390/cancers15184480