
Vaping, Environmental Toxicants Exposure, and Lung Cancer Risk
 ,
,  ,
,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
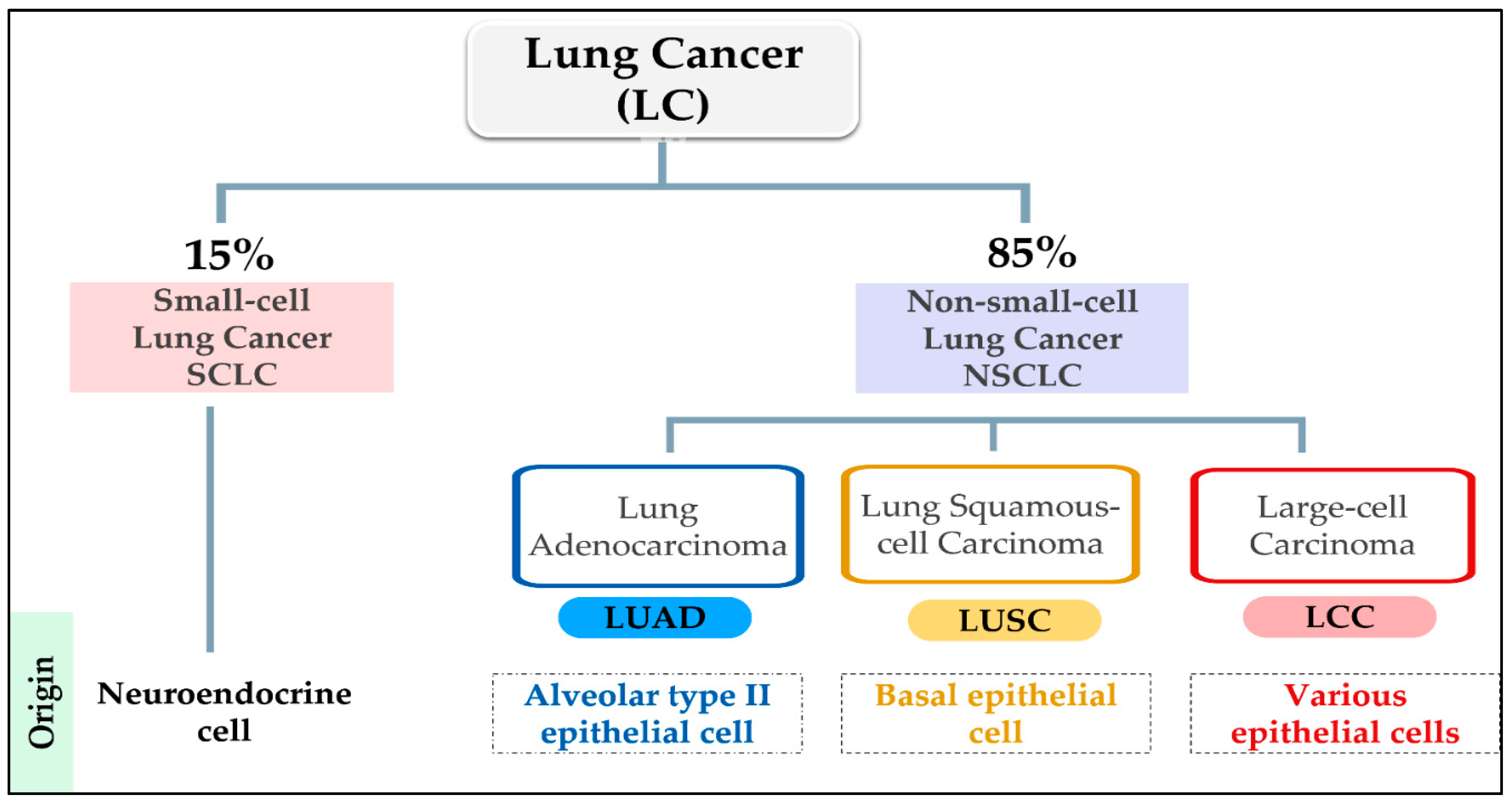
3. Epidemiology of Lung Cancer
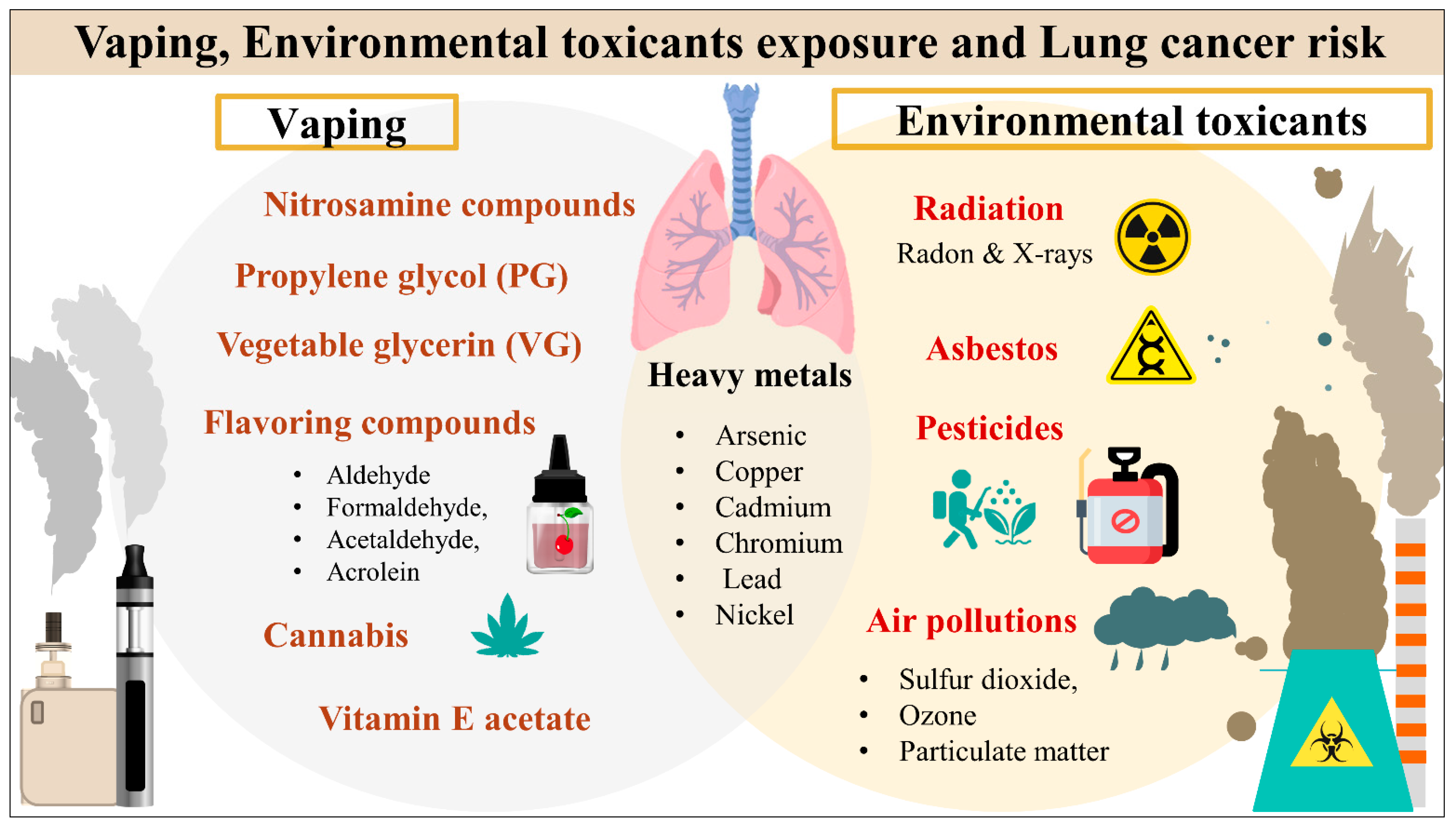
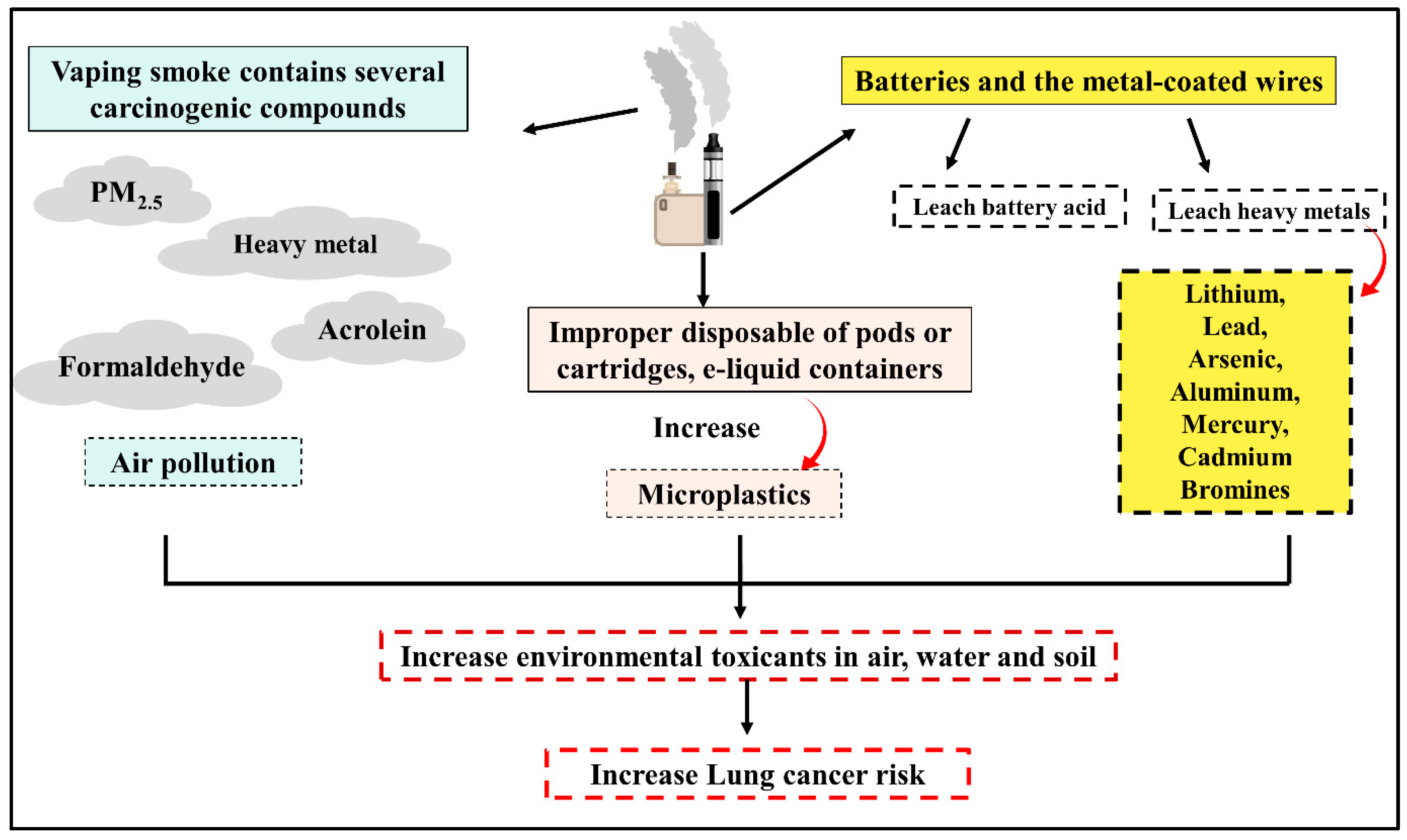
4. Vaping and Environmental Toxicants Interact as Lung Cancer Risk Factors
5. Vaping and Lung Cancer
5.1. Nitrosamine Compounds
5.2. Propylene Glycol and Vegetable Glycerin
5.3. Flavoring Compounds
5.4. Cannabidiol (CBD) Vaping Products
6. Environmental Toxicants and Lung Cancer
6.1. Radiation
6.1.1. Radon
6.1.2. Medical Radiation
6.2. Air Pollution
Airborne Particulate Matter (PM)
6.3. Heavy Metals
6.3.1. Cadmium (Cd)
6.3.2. Arsenic (As)
6.4. Asbestos
6.5. Pesticides
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85. [Google Scholar] [CrossRef] [PubMed]
- Baum, P.; Winter, H.; Eichhorn, M.E.; Roesch, R.M.; Taber, S.; Christopoulos, P.; Wiegering, A.; Lenzi, J. Trends in Age- and Sex-Specific Lung Cancer Mortality in Europe and Northern America: Analysis of Vital Registration Data from the WHO Mortality Database between 2000 and 2017. Eur. J. Cancer 2022, 171, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Sharma, R. Mapping of Global, Regional and National Incidence, Mortality and Mortality-to-Incidence Ratio of Lung Cancer in 2020 and 2050. Int. J. Clin. Oncol. 2022, 27, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Thandra, K.C.; Barsouk, A.; Saginala, K.; Aluru, J.S.; Barsouk, A. Epidemiology of Lung Cancer. Contemp. Oncol. 2021, 25, 45. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- National Lung Screening Trial Research Team. Reduced Lung-Cancer Mortality with Low-Dose Computed Tomographic Screening. N. Engl. J. Med. 2011, 365. [Google Scholar] [CrossRef]
- Araghi, M.; Fidler-Benaoudia, M.; Arnold, M.; Rutherford, M.; Bardot, A.; Ferlay, J.; Bucher, O.; De, P.; Engholm, G.; Gavin, A.; et al. International Differences in Lung Cancer Survival by Sex, Histological Type and Stage at Diagnosis: An ICBP SURVMARK-2 Study. Thorax 2022, 77, 378–390. [Google Scholar] [CrossRef]
- Smok-Kalwat, J.; Mertowska, P.; Mertowski, S.; Smolak, K.; Kozińska, A.; Koszałka, F.; Kwaśniewski, W.; Grywalska, E.; Góźdź, S. The Importance of the Immune System and Molecular Cell Signaling Pathways in the Pathogenesis and Progression of Lung Cancer. Int. J. Mol. Sci. 2023, 24, 1506. [Google Scholar] [CrossRef]
- Shankar, A.; Dubey, A.; Saini, D.; Singh, M.; Prasad, C.P.; Roy, S.; Bharati, S.J.; Rinki, M.; Singh, N.; Seth, T.; et al. Environmental and Occupational Determinants of Lung Cancer. Transl. Lung Cancer Res. 2019, 8, S31–S49. [Google Scholar] [CrossRef]
- Benusiglio, P.R.; Fallet, V.; Sanchis-Borja, M.; Coulet, F.; Cadranel, J. Lung Cancer Is Also a Hereditary Disease. Eur. Respir. Rev. 2021, 30. [Google Scholar] [CrossRef]
- Schwartz, A.G.; Bailey-Wilson, J.E.; Amos, C.I. 6—Genetic Susceptibility to Lung Cancer. In IASLC Thoracic Oncology, 2nd ed.; Pass, H.I., Ball, D., Scagliotti, G.V., Eds.; Elsevier: Philadelphia, PA, USA, 2018; pp. 46–51.e2. ISBN 978-0-323-52357-8. [Google Scholar]
- Weir, B.A.; Woo, M.S.; Getz, G.; Perner, S.; Ding, L.; Beroukhim, R.; Lin, W.M.; Province, M.A.; Kraja, A.; Johnson, L.A.; et al. Characterizing the Cancer Genome in Lung Adenocarcinoma. Nature 2007, 450, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Comprehensive Genomic Characterization of Squamous Cell Lung Cancers. Nature 2012, 489, 519–525. [CrossRef]
- Bracken-Clarke, D.; Kapoor, D.; Baird, A.M.; Buchanan, P.J.; Gately, K.; Cuffe, S.; Finn, S.P. Vaping and Lung Cancer—A Review of Current Data and Recommendations. Lung Cancer 2021, 153, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Agusti, A.; Vogelmeier, C.F.; Halpin, D.M.G. Tackling the Global Burden of Lung Disease through Prevention and Early Diagnosis. Lancet Respir. Med. 2022, 10, 1013–1015. [Google Scholar] [CrossRef]
- Kuditipudi, A.D.; Dirisanala, S.; Ganti, N.; Laller, S.; Williams, I.; Taj, S.; Arora, K.S.; Hameed, A.; Lei, Y.W.; Venkata, V.S.; et al. 247: Epidemiology and Prevalenceof Lung Disease Among E-Cigarette Users in the Usa: A National Study. Crit. Care Med. 2023, 51, 108. [Google Scholar] [CrossRef]
- Cullen, K.A. Notes from the Field: Use of Electronic Cigarettes and Any Tobacco Product Among Middle and High School Students—United States, 2011–2018. MMWR Morb. Mortal. Wkly. Rep. 2018, 67. [Google Scholar] [CrossRef]
- Cornelius, M.E. Tobacco Product Use Among Adults—United States, 2019. MMWR Morb. Mortal. Wkly. Rep. 2020, 69. [Google Scholar] [CrossRef]
- Tsai, J.; Walton, K.; Coleman, B.N.; Sharapova, S.R.; Johnson, S.E.; Kennedy, S.M.; Caraballo, R.S. Reasons for Electronic Cigarette Use Among Middle and High School Students—National Youth Tobacco Survey, United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 196–200. [Google Scholar] [CrossRef]
- Gentzke, A.S. Tobacco Product Use Among Middle and High School Students—United States, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69. [Google Scholar] [CrossRef]
- Hartnett, K.P.; Kite-Powell, A.; Patel, M.T.; Haag, B.L.; Sheppard, M.J.; Dias, T.P.; King, B.A.; Melstrom, P.C.; Ritchey, M.D.; Stein, Z.; et al. Syndromic Surveillance for E-Cigarette, or Vaping, Product Use–Associated Lung Injury. N. Engl. J. Med. 2020, 382, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Petrella, F.; Rizzo, S.; Masiero, M.; Marzorati, C.; Casiraghi, M.; Bertolaccini, L.; Mazzella, A.; Pravettoni, G.; Spaggiari, L. Clinical Impact of Vaping on Cardiopulmonary Function and Lung Cancer Development: An Update. Eur. J. Cancer Prev. 2023. [Google Scholar] [CrossRef]
- Muthumalage, T.; Friedman, M.R.; McGraw, M.D.; Ginsberg, G.; Friedman, A.E.; Rahman, I. Chemical Constituents Involved in E-Cigarette, or Vaping Product Use-Associated Lung Injury (EVALI). Toxics 2020, 8, 25. [Google Scholar] [CrossRef] [PubMed]
- Stefaniak, A.B.; LeBouf, R.F.; Ranpara, A.C.; Leonard, S.S. Toxicology of Flavoring- and Cannabis-Containing e-Liquids Used in Electronic Delivery Systems. Pharmacol. Ther. 2021, 224, 107838. [Google Scholar] [CrossRef]
- Gonzalez-Jimenez, N.; Gray, N.; Pappas, R.S.; Halstead, M.; Lewis, E.; Valentin-Blasini, L.; Watson, C.; Blount, B. Analysis of Toxic Metals in Aerosols from Devices Associated with Electronic Cigarette, or Vaping, Product Use Associated Lung Injury. Toxics 2021, 9, 240. [Google Scholar] [CrossRef]
- Khlystov, A.; Samburova, V. Flavoring Compounds Dominate Toxic Aldehyde Production during E-Cigarette Vaping. Environ. Sci. Technol. 2016, 50, 13080–13085. [Google Scholar] [CrossRef]
- Fiore, M.; Oliveri Conti, G.; Caltabiano, R.; Buffone, A.; Zuccarello, P.; Cormaci, L.; Cannizzaro, M.A.; Ferrante, M. Role of Emerging Environmental Risk Factors in Thyroid Cancer: A Brief Review. Int. J. Environ. Res. Public Health 2019, 16, 1185. [Google Scholar] [CrossRef]
- Kruger, E.; Toraih, E.A.; Hussein, M.H.; Shehata, S.A.; Waheed, A.; Fawzy, M.S.; Kandil, E. Thyroid Carcinoma: A Review for 25 Years of Environmental Risk Factors Studies. Cancers 2022, 14, 6172. [Google Scholar] [CrossRef]
- du Plessis, M.; Fourie, C.; Stone, W.; Engelbrecht, A.-M. The Impact of Endocrine Disrupting Compounds and Carcinogens in Wastewater: Implications for Breast Cancer. Biochimie 2023, 209, 103–115. [Google Scholar] [CrossRef]
- Valdez-Flores, C.; Erraguntla, N.; Budinsky, R.; Cagen, S.; Kirman, C.R. An Updated Lymphohematopoietic and Bladder Cancers Risk Evaluation for Occupational and Environmental Exposures to 1,3-Butadiene. Chem.-Biol. Interact. 2022, 366, 110077. [Google Scholar] [CrossRef]
- Rahaman, M.S.; Rahman, M.M.; Mise, N.; Sikder, M.T.; Ichihara, G.; Uddin, M.K.; Kurasaki, M.; Ichihara, S. Environmental Arsenic Exposure and Its Contribution to Human Diseases, Toxicity Mechanism and Management. Environ. Pollut. 2021, 289, 117940. [Google Scholar] [CrossRef] [PubMed]
- Jaafarzadeh, N.; Poormohammadi, A.; Almasi, H.; Ghaedrahmat, Z.; Rahim, F.; Zahedi, A. Arsenic in Drinking Water and Kidney Cancer: A Systematic Review. Rev. Environ. Health 2022, 38, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Moubarz, G.; Saad-Hussein, A.; Shahy, E.M.; Mahdy-Abdallah, H.; Mohammed, A.M.F.; Saleh, I.A.; Abo-Zeid, M.A.M.; Abo-Elfadl, M.T. Lung Cancer Risk in Workers Occupationally Exposed to Polycyclic Aromatic Hydrocarbons with Emphasis on the Role of DNA Repair Gene. Int. Arch. Occup. Environ. Health 2023, 96, 313–329. [Google Scholar] [CrossRef]
- Lagoa, R.; Marques-da-Silva, D.; Diniz, M.; Daglia, M.; Bishayee, A. Molecular Mechanisms Linking Environmental Toxicants to Cancer Development: Significance for Protective Interventions with Polyphenols. Semin. Cancer Biol. 2022, 80, 118–144. [Google Scholar] [CrossRef] [PubMed]
- Farland, W.H. The US Environmental Protection Agency’s Risk Assessment Guidelines: Current Status and Future Directions. Toxicol. Ind. Health 1992, 8, 205–212. [Google Scholar]
- International Agency for Research on Cancer IARC Monographs on the Identification of Carcinogenic Hazards to Humans. IARC Monogr. Meet. 2019, 124, 1–4.
- Wang, Z.; Yang, C. Metal Carcinogen Exposure Induces Cancer Stem Cell-like Property through Epigenetic Reprograming: A Novel Mechanism of Metal Carcinogenesis. Semin. Cancer Biol. 2019, 57, 95–104. [Google Scholar] [CrossRef]
- Bade, B.C.; Cruz, C.S.D. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar]
- Marshall, G.; Ferreccio, C.; Yuan, Y.; Bates, M.N.; Steinmaus, C.; Selvin, S.; Liaw, J.; Smith, A.H. Fifty-Year Study of Lung and Bladder Cancer Mortality in Chile Related to Arsenic in Drinking Water. J. Natl. Cancer Inst. 2007, 99, 920–928. [Google Scholar] [CrossRef]
- Lantz, P.M.; Mendez, D.; Philbert, M.A. Radon, Smoking, and Lung Cancer: The Need to Refocus Radon Control Policy. Am. J. Public Health 2013, 103, 443–447. [Google Scholar] [CrossRef]
- Zou, K.; Sun, P.; Huang, H.; Zhuo, H.; Qie, R.; Xie, Y.; Luo, J.; Li, N.; Li, J.; He, J.; et al. Etiology of Lung Cancer: Evidence from Epidemiologic Studies. J. Natl. Cancer Cent. 2022, 2, 216–225. [Google Scholar] [CrossRef]
- Huang, J.; Deng, Y.; Tin, M.S.; Lok, V.; Ngai, C.H.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.-J.; Elcarte, E.; et al. Distribution, Risk Factors, and Temporal Trends for Lung Cancer Incidence and Mortality: A Global Analysis. Chest 2022, 161, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Forjaz, G.; Mooradian, M.J.; Meza, R.; Kong, C.Y.; Cronin, K.A.; Mariotto, A.B.; Lowy, D.R.; Feuer, E.J. The Effect of Advances in Lung-Cancer Treatment on Population Mortality. N. Engl. J. Med. 2020, 383, 640–649. [Google Scholar] [CrossRef]
- Malhotra, J.; Boffetta, P. Epidemiology of Occupational Lung Cancer. In Occupational Cancers; Anttila, S., Boffetta, P., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 287–294. ISBN 978-3-030-30766-0. [Google Scholar]
- Ezzati, M.; Lopez, A.D. Estimates of Global Mortality Attributable to Smoking in 2000. Lancet 2003, 362, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Spyratos, D.; Zarogoulidis, P.; Porpodis, K.; Tsakiridis, K.; Machairiotis, N.; Katsikogiannis, N.; Kougioumtzi, I.; Dryllis, G.; Kallianos, A.; Rapti, A.; et al. Occupational Exposure and Lung Cancer. J. Thorac. Dis. 2013, 5, S440. [Google Scholar]
- Wang, X.; Wang, T.; Hua, J.; Cai, M.; Qian, Z.; Wang, C.; Li, H.; McMillin, S.E.; Aaron, H.E.; Xie, C.; et al. Histological Types of Lung Cancer Attributable to Fine Particulate, Smoking, and Genetic Susceptibility. Sci. Total Environ. 2023, 858, 159890. [Google Scholar] [CrossRef]
- Larsson, S.C.; Carter, P.; Kar, S.; Vithayathil, M.; Mason, A.M.; Michaëlsson, K.; Burgess, S. Smoking, Alcohol Consumption, and Cancer: A Mendelian Randomisation Study in UK Biobank and International Genetic Consortia Participants. PLoS Med. 2020, 17, e1003178. [Google Scholar] [CrossRef]
- Lipfert, F.W.; Wyzga, R.E. Longitudinal Relationships between Lung Cancer Mortality Rates, Smoking, and Ambient Air Quality: A Comprehensive Review and Analysis. Crit. Rev. Toxicol. 2019, 49, 790–818. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Personal habits and indoor combustions. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100 Pt E, 1–538. [Google Scholar]
- Burkhardt, T.; Scherer, M.; Scherer, G.; Pluym, N.; Weber, T.; Kolossa-Gehring, M. Time Trend of Exposure to Secondhand Tobacco Smoke and Polycyclic Aromatic Hydrocarbons between 1995 and 2019 in Germany—Showcases for Successful European Legislation. Environ. Res. 2023, 216, 114638. [Google Scholar] [CrossRef]
- Mourino, N.; Pérez-Ríos, M.; Yolton, K.; Lanphear, B.P.; Chen, A.; Buckley, J.P.; Kalkwarf, H.J.; Cecil, K.M.; Braun, J.M. Pre- and Postnatal Exposure to Secondhand Tobacco Smoke and Cardiometabolic Risk at 12 Years: Periods of Susceptibility. Environ. Res. 2023, 224, 115572. [Google Scholar] [CrossRef] [PubMed]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Some Nitrobenzenes and other Industrial Chemicals. Lyon (FR): International Agency for Research on Cancer; 2020. (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 123.). Available online: https://www.ncbi.nlm.nih.gov/books/NBK561907/ (accessed on 21 June 2023).
- de Oliveira Alves, N.; Martins Pereira, G.; Di Domenico, M.; Costanzo, G.; Benevenuto, S.; de Oliveira Fonoff, A.M.; de Souza Xavier Costa, N.; Ribeiro Júnior, G.; Satoru Kajitani, G.; Cestari Moreno, N.; et al. Inflammation Response, Oxidative Stress and DNA Damage Caused by Urban Air Pollution Exposure Increase in the Lack of DNA Repair XPC Protein. Environ. Int. 2020, 145, 106150. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Canales, J.; Parra-Cuentas, E.; Wistuba, I.I. Diagnosis and Molecular Classification of Lung Cancer. In Lung Cancer: Treatment and Research; Reckamp, K.L., Ed.; Cancer Treatment and Research; Springer International Publishing: Cham, Switzerland, 2016; pp. 25–46. ISBN 978-3-319-40389-2. [Google Scholar]
- Oser, M.G.; Niederst, M.J.; Sequist, L.V.; Engelman, J.A. Transformation from Non-Small-Cell Lung Cancer to Small-Cell Lung Cancer: Molecular Drivers and Cells of Origin. Lancet Oncol. 2015, 16, e165–e172. [Google Scholar] [CrossRef]
- Hynds, R.E.; Frese, K.K.; Pearce, D.R.; Grönroos, E.; Dive, C.; Swanton, C. Progress towards Non-Small-Cell Lung Cancer Models That Represent Clinical Evolutionary Trajectories. Open Biol. 2021, 11, 200247. [Google Scholar] [CrossRef]
- Curado, M.-P.; Edwards, B.; Shin, H.R.; Storm, H.; Ferlay, J.; Heanue, M.; Boyle, P. Cancer Incidence in Five Continents, Volume IX; IARC Press, International Agency for Research on Cancer: Lyon, France, 2007; ISBN 92-832-2160-5. [Google Scholar]
- Zeng, Z.; Wang, Z.; Li, Y.; Ye, D.; Zeng, J.; Hu, J.; Chen, P.; Xiao, J.; Zou, J.; Li, Z. Nuclear Factor Erythroid 2 (NF-E2)-Related Factor 2 (Nrf2) in Non-Small Cell Lung Cancer. Life Sci. 2020, 254, 117325. [Google Scholar] [CrossRef]
- Denisenko, T.V.; Budkevich, I.N.; Zhivotovsky, B. Cell Death-Based Treatment of Lung Adenocarcinoma. Cell Death Dis. 2018, 9, 1–14. [Google Scholar] [CrossRef]
- Choudhury, N.J.; Marra, A.; Sui, J.S.Y.; Flynn, J.; Yang, S.-R.; Falcon, C.J.; Selenica, P.; Schoenfeld, A.J.; Rekhtman, N.; Gomez, D.; et al. Molecular Biomarkers of Disease Outcomes and Mechanisms of Acquired Resistance to First-Line Osimertinib in Advanced EGFR-Mutant Lung Cancers. J. Thorac. Oncol. 2023, 18, 463–475. [Google Scholar] [CrossRef]
- Panani, A.D.; Roussos, C. Cytogenetic and Molecular Aspects of Lung Cancer. Cancer Lett. 2006, 239, 1–9. [Google Scholar] [CrossRef]
- Ngamwong, Y.; Tangamornsuksan, W.; Lohitnavy, O.; Chaiyakunapruk, N.; Scholfield, C.N.; Reisfeld, B.; Lohitnavy, M. Additive Synergism between Asbestos and Smoking in Lung Cancer Risk: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0135798. [Google Scholar] [CrossRef]
- Mauderly, J.L.; Seilkop, S.K.; Barr, E.B.; Gigliotti, A.P.; Hahn, F.F.; Hobbs, C.H.; Finch, G.L. Carcinogenic Interactions between a Single Inhalation of 239PuO2 and Chronic Exposure to Cigarette Smoke in Rats. Radiat. Res. 2010, 173, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Lin, Y.; Xia, T.; Zhu, Y. Effects of Electronic Cigarettes on Indoor Air Quality and Health. Annu. Rev. Public Health 2020, 41, 363–380. [Google Scholar] [CrossRef]
- Zhang, Y.; Sumner, W.; Chen, D.-R. In Vitro Particle Size Distributions in Electronic and Conventional Cigarette Aerosols Suggest Comparable Deposition Patterns. Nicotine Tob. Res. 2013, 15, 501–508. [Google Scholar] [CrossRef]
- Ruprecht, A.A.; De Marco, C.; Saffari, A.; Pozzi, P.; Mazza, R.; Veronese, C.; Angellotti, G.; Munarini, E.; Ogliari, A.C.; Westerdahl, D.; et al. Environmental Pollution and Emission Factors of Electronic Cigarettes, Heat-Not-Burn Tobacco Products, and Conventional Cigarettes. Aerosol Sci. Technol. 2017, 51, 674–684. [Google Scholar] [CrossRef]
- Nguyen, C.; Li, L.; Sen, C.A.; Ronquillo, E.; Zhu, Y. Fine and Ultrafine Particles Concentrations in Vape Shops. Atmos. Environ. 2019, 211, 159–169. [Google Scholar] [CrossRef]
- Li, Z.; Liu, H.; Qian, Y.; Li, X.; Guo, C.; Wang, Z.; Wei, Y. Influence of Metals from E-Waste Dismantling on Telomerelength and Mitochondrial DNA Copy Number in People Living near Recycling Sites. Environ. Int. 2020, 140, 105769. [Google Scholar] [CrossRef]
- Beutel, M.W.; Harmon, T.C.; Novotny, T.E.; Mock, J.; Gilmore, M.E.; Hart, S.C.; Traina, S.; Duttagupta, S.; Brooks, A.; Jerde, C.L.; et al. A Review of Environmental Pollution from the Use and Disposal of Cigarettes and Electronic Cigarettes: Contaminants, Sources, and Impacts. Sustainability 2021, 13, 12994. [Google Scholar] [CrossRef]
- Hendlin, Y.H. Alert: Public Health Implications of Electronic Cigarette Waste. Am. J. Public Health 2018, 108, 1489. [Google Scholar] [CrossRef]
- National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. E-Cigarette Use among Youth and Young Adults: A Report of the Surgeon General; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538680/ (accessed on 21 June 2023).
- Centers for Disease Control and Prevention. E-Cigarette, or Vaping, Products Visual Dictionary; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. Available online: https://stacks.cdc.gov/view/cdc/103783 (accessed on 21 June 2023).
- Hartmann-Boyce, J.; Chepkin, S.C.; Ye, W.; Bullen, C.; Lancaster, T. Nicotine Replacement Therapy versus Control for Smoking Cessation. Cochrane Database Syst. Rev. 2018, 5, CD000146. [Google Scholar] [CrossRef]
- Do, E.K.; O’Connor, K.; Perks, S.N.; Soule, E.K.; Eissenberg, T.; Amato, M.S.; Graham, A.L.; Martin, C.K.; Höchsmann, C.; Fuemmeler, B.F. E-Cigarette Device and Liquid Characteristics and E-Cigarette Dependence: A Pilot Study of Pod-Based and Disposable E-Cigarette Users. Addict. Behav. 2022, 124, 107117. [Google Scholar] [CrossRef]
- Margham, J.; McAdam, K.; Forster, M.; Liu, C.; Wright, C.; Mariner, D.; Proctor, C. Chemical Composition of Aerosol from an E-Cigarette: A Quantitative Comparison with Cigarette Smoke. Chem. Res. Toxicol. 2016, 29, 1662–1678. [Google Scholar] [CrossRef] [PubMed]
- Felicione, N.J.; Kaiser, L.; Leigh, N.J.; Page, M.K.; Block, A.C.; Schurr, B.E.; O’Connor, R.J.; Goniewicz, M.L. Comparing POD and MOD ENDS Users’ Product Characteristics, Use Behaviors, and Nicotine Exposure. Nicotine Tob. Res. 2023, 25, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Hiemstra, P.S.; Bals, R. Basic Science of Electronic Cigarettes: Assessment in Cell Culture and in Vivo Models. Respir. Res. 2016, 17, 127. [Google Scholar] [CrossRef] [PubMed]
- Fadus, M.C.; Smith, T.T.; Squeglia, L.M. The Rise of E-Cigarettes, Pod Mod Devices, and JUUL among Youth: Factors Influencing Use, Health Implications, and Downstream Effects. Drug Alcohol. Depend. 2019, 201, 85–93. [Google Scholar] [CrossRef]
- Sears, C.G.; Hart, J.L.; Walker, K.L.; Robertson, R.M. Generally Recognized as Safe: Uncertainty Surrounding E-Cigarette Flavoring Safety. Int. J. Environ. Res. Public Health 2017, 14, 1274. [Google Scholar] [CrossRef]
- Hamberger, E.S.; Halpern-Felsher, B. Vaping in Adolescents: Epidemiology and Respiratory Harm. Curr. Opin. Pediatr. 2020, 32, 378–383. [Google Scholar] [CrossRef]
- Glasser, A.M.; Johnson, A.L.; Niaura, R.S.; Abrams, D.B.; Pearson, J.L. Youth Vaping and Tobacco Use in Context in the United States: Results From the 2018 National Youth Tobacco Survey. Nicotine Tob. Res. 2021, 23, 447–453. [Google Scholar] [CrossRef]
- Lee, H.-W.; Park, S.-H.; Weng, M.; Wang, H.-T.; Huang, W.C.; Lepor, H.; Wu, X.-R.; Chen, L.-C.; Tang, M. E-Cigarette Smoke Damages DNA and Reduces Repair Activity in Mouse Lung, Heart, and Bladder as Well as in Human Lung and Bladder Cells. Proc. Natl. Acad. Sci. USA 2018, 115, E1560–E1569. [Google Scholar] [CrossRef]
- Waldum, H.L.; Nilsen, O.G.; Nilsen, T.; Rørvik, H.; Syversen, U.; Sandvik, A.K.; Haugen, O.A.; Torp, S.H.; Brenna, E. Long-Term Effects of Inhaled Nicotine. Life Sci. 1996, 58, 1339–1346. [Google Scholar] [CrossRef]
- Sundar, I.K.; Mullapudi, N.; Yao, H.; Spivack, S.D.; Rahman, I. Lung Cancer and Its Association with Chronic Obstructive Pulmonary Disease: Update on Nexus of Epigenetics. Curr. Opin. Pulm. Med. 2011, 17, 279. [Google Scholar] [CrossRef]
- Muthumalage, T.; Lamb, T.; Friedman, M.R.; Rahman, I. E-Cigarette Flavored Pods Induce Inflammation, Epithelial Barrier Dysfunction, and DNA Damage in Lung Epithelial Cells and Monocytes. Sci. Rep. 2019, 9, 19035. [Google Scholar] [CrossRef]
- Gomes, M.; Teixeira, A.L.; Coelho, A.; Araújo, A.; Medeiros, R. The Role of Inflammation in Lung Cancer. In Inflammation and Cancer; Aggarwal, B.B., Sung, B., Gupta, S.C., Eds.; Advances in Experimental Medicine and Biology; Springer: Basel, Switzerland, 2014; pp. 1–23. ISBN 978-3-0348-0837-8. [Google Scholar]
- Uchiyama, S.; Noguchi, M.; Sato, A.; Ishitsuka, M.; Inaba, Y.; Kunugita, N. Determination of Thermal Decomposition Products Generated from E-Cigarettes. Chem. Res. Toxicol. 2020, 33, 576–583. [Google Scholar] [CrossRef]
- Roe, F.J.C.; Wood, D. Review: Acetaldehyde and Formaldehyde: Is There a Cancer Risk for Man? Indoor Environ. 1992, 1, 8–15. [Google Scholar] [CrossRef]
- Matsumoto, M.; Yamano, S.; Senoh, H.; Umeda, Y.; Hirai, S.; Saito, A.; Kasai, T.; Aiso, S. Carcinogenicity and Chronic Toxicity of Acrolein in Rats and Mice by Two-Year Inhalation Study. Regul. Toxicol. Pharmacol. 2021, 121, 104863. [Google Scholar] [CrossRef] [PubMed]
- Smets, J.; Baeyens, F.; Chaumont, M.; Adriaens, K.; Van Gucht, D. When Less Is More: Vaping Low-Nicotine vs. High-Nicotine E-Liquid Is Compensated by Increased Wattage and Higher Liquid Consumption. Int. J. Environ. Res. Public Health 2019, 16, 723. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Yang, S.; Seng, S. Mechanisms of Cancer Induction by Tobacco-Specific NNK and NNN. Cancers 2014, 6, 1138–1156. [Google Scholar] [CrossRef]
- Tang, M.; Wu, X.-R.; Lee, H.-W.; Xia, Y.; Deng, F.-M.; Moreira, A.L.; Chen, L.-C.; Huang, W.C.; Lepor, H. Electronic-Cigarette Smoke Induces Lung Adenocarcinoma and Bladder Urothelial Hyperplasia in Mice. Proc. Natl. Acad. Sci. USA 2019, 116, 21727–21731. [Google Scholar] [CrossRef]
- Stepanov, I.; Carmella, S.G.; Han, S.; Pinto, A.; Strasser, A.A.; Lerman, C.; Hecht, S.S. Evidence for Endogenous Formation of N′-Nitrosonornicotine in Some Long-Term Nicotine Patch Users. Nicotine Tob. Res. 2009, 11, 99–105. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Hukkanen, J.; Jacob, P. Nicotine Chemistry, Metabolism, Kinetics and Biomarkers. In Nicotine Psychopharmacology; Henningfield, J.E., London, E.D., Pogun, S., Eds.; Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2009; pp. 29–60. ISBN 978-3-540-69248-5. [Google Scholar]
- Shahab, L.; Goniewicz, M.L.; Blount, B.C.; Brown, J.; McNeill, A.; Alwis, K.U.; Feng, J.; Wang, L.; West, R. Nicotine, Carcinogen, and Toxin Exposure in Long-Term E-Cigarette and Nicotine Replacement Therapy Users. Ann. Intern. Med. 2017, 166, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Gao, Y.; Li, D.; Gao, N. Emission and Gas/Particle Partitioning Characteristics of Nicotine in Aerosols for Electronic Cigarettes. Chem. Res. Toxicol. 2022, 35, 890–897. [Google Scholar] [CrossRef]
- Agency for Toxic Substances and Disease Registry (ATSDR) Toxicological Profile for Propylene Glycol. 1997. Available online: http://medbox.iiab.me/modules/en-cdc/www.atsdr.cdc.gov/substances/toxsubstance.asp_toxid=240 (accessed on 21 June 2023).
- Cao, D.J.; Aldy, K.; Hsu, S.; McGetrick, M.; Verbeck, G.; De Silva, I.; Feng, S. Review of Health Consequences of Electronic Cigarettes and the Outbreak of Electronic Cigarette, or Vaping, Product Use-Associated Lung Injury. J. Med. Toxicol. 2020, 16, 295–310. [Google Scholar] [CrossRef]
- Kosmider, L.; Sobczak, A.; Fik, M.; Knysak, J.; Zaciera, M.; Kurek, J.; Goniewicz, M.L. Carbonyl Compounds in Electronic Cigarette Vapors: Effects of Nicotine Solvent and Battery Output Voltage. Nicotine Tob. Res. 2014, 16, 1319–1326. [Google Scholar] [CrossRef]
- Woodall, M.; Jacob, J.; Kalsi, K.K.; Schroeder, V.; Davis, E.; Kenyon, B.; Khan, I.; Garnett, J.P.; Tarran, R.; Baines, D.L. E-Cigarette Constituents Propylene Glycol and Vegetable Glycerin Decrease Glucose Uptake and Its Metabolism in Airway Epithelial Cells in Vitro. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2020, 319, L957–L967. [Google Scholar] [CrossRef]
- Sleiman, M.; Logue, J.M.; Montesinos, V.N.; Russell, M.L.; Litter, M.I.; Gundel, L.A.; Destaillats, H. Emissions from Electronic Cigarettes: Key Parameters Affecting the Release of Harmful Chemicals. Environ. Sci. Technol. 2016, 50, 9644–9651. [Google Scholar] [CrossRef]
- Bitzer, Z.T.; Goel, R.; Reilly, S.M.; Foulds, J.; Muscat, J.; Elias, R.J.; Richie, J.P., Jr. Effects of Solvent and Temperature on Free Radical Formation in Electronic Cigarette Aerosols. Chem. Res. Toxicol. 2018, 31, 4–12. [Google Scholar] [CrossRef]
- Escobar, Y.-N.H.; Nipp, G.; Cui, T.; Petters, S.S.; Surratt, J.D.; Jaspers, I. In Vitro Toxicity and Chemical Characterization of Aerosol Derived from Electronic Cigarette Humectants Using a Newly Developed Exposure System. Chem. Res. Toxicol. 2020, 33, 1677–1688. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.D.; Chung, S.; Baumlin, N.; Sun, L.; Silswal, N.; Dennis, J.S.; Yoshida, M.; Sabater, J.; Horrigan, F.T.; Salathe, M. E-Cigarette Aerosols of Propylene Glycol Impair BK Channel Activity and Parameters of Mucociliary Function. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2023, 324, L468–L479. [Google Scholar] [CrossRef] [PubMed]
- Bellier, J.; Nokin, M.-J.; Lardé, E.; Karoyan, P.; Peulen, O.; Castronovo, V.; Bellahcène, A. Methylglyoxal, a Potent Inducer of AGEs, Connects between Diabetes and Cancer. Diabetes Res. Clin. Pract. 2019, 148, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Bellahcène, A.; Nokin, M.-J.; Castronovo, V.; Schalkwijk, C. Methylglyoxal-Derived Stress: An Emerging Biological Factor Involved in the Onset and Progression of Cancer. Semin. Cancer Biol. 2018, 49, 64–74. [Google Scholar] [CrossRef]
- Huynh, D.; Huang, J.; Le, L.T.T.; Liu, D.; Liu, C.; Pham, K.; Wang, H. Electronic Cigarettes Promotes the Lung Colonization of Human Breast Cancer in NOD-SCID-Gamma Mice. Int. J. Clin. Exp. Pathol. 2020, 13, 2075–2081. [Google Scholar]
- Effah, F.; Taiwo, B.; Baines, D.; Bailey, A.; Marczylo, T. Pulmonary Effects of E-Liquid Flavors: A Systematic Review. J. Toxicol. Environ. Health Part B 2022, 25, 343–371. [Google Scholar] [CrossRef] [PubMed]
- Gillman, I.G.; Pennington, A.S.C.; Humphries, K.E.; Oldham, M.J. Determining the Impact of Flavored E-Liquids on Aldehyde Production during Vaping. Regul. Toxicol. Pharmacol. 2020, 112, 104588. [Google Scholar] [CrossRef] [PubMed]
- Song, M.-A.; Reisinger, S.A.; Freudenheim, J.L.; Brasky, T.M.; Mathé, E.A.; McElroy, J.P.; Nickerson, Q.A.; Weng, D.Y.; Wewers, M.D.; Shields, P.G. Effects of Electronic Cigarette Constituents on the Human Lung: A Pilot Clinical Trial. Cancer Prev. Res. 2020, 13, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Ogunwale, M.A.; Li, M.; Ramakrishnam Raju, M.V.; Chen, Y.; Nantz, M.H.; Conklin, D.J.; Fu, X.-A. Aldehyde Detection in Electronic Cigarette Aerosols. ACS Omega 2017, 2, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Yogeswaran, S.; Muthumalage, T.; Rahman, I. Comparative Reactive Oxygen Species (ROS) Content among Various Flavored Disposable Vape Bars, Including Cool (Iced) Flavored Bars. Toxics 2021, 9, 235. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Rahman, I. Current Concepts on Oxidative/Carbonyl Stress, Inflammation and Epigenetics in Pathogenesis of Chronic Obstructive Pulmonary Disease. Toxicol. Appl. Pharmacol. 2011, 254, 72–85. [Google Scholar] [CrossRef]
- Schieber, M.; Chandel, N.S. ROS Function in Redox Signaling and Oxidative Stress. Curr. Biol. 2014, 24, R453–R462. [Google Scholar] [CrossRef]
- Martin, E.M.; Clapp, P.W.; Rebuli, M.E.; Pawlak, E.A.; Glista-Baker, E.; Benowitz, N.L.; Fry, R.C.; Jaspers, I. E-Cigarette Use Results in Suppression of Immune and Inflammatory-Response Genes in Nasal Epithelial Cells Similar to Cigarette Smoke. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2016, 311, L135–L144. [Google Scholar] [CrossRef]
- Song, Y.; Jiang, S.; Li, C.; Loor, J.J.; Jiang, Q.; Yang, Y.; Feng, X.; Liu, S.; He, J.; Wang, K.; et al. Free Fatty Acids Promote Degranulation of Azurophil Granules in Neutrophils by Inducing Production of NADPH Oxidase–Derived Reactive Oxygen Species in Cows with Subclinical Ketosis. J. Dairy Sci. 2022, 105, 2473–2486. [Google Scholar] [CrossRef] [PubMed]
- Zahedi, A.; Phandthong, R.; Chaili, A.; Remark, G.; Talbot, P. Epithelial-to-Mesenchymal Transition of A549 Lung Cancer Cells Exposed to Electronic Cigarettes. Lung Cancer 2018, 122, 224–233. [Google Scholar] [CrossRef]
- Nair, V.; Tran, M.; Behar, R.Z.; Zhai, S.; Cui, X.; Phandthong, R.; Wang, Y.; Pan, S.; Luo, W.; Pankow, J.F.; et al. Menthol in Electronic Cigarettes: A Contributor to Respiratory Disease? Toxicol. Appl. Pharmacol. 2020, 407, 115238. [Google Scholar] [CrossRef] [PubMed]
- Stewart, T.A.; Yapa, K.T.D.S.; Monteith, G.R. Altered Calcium Signaling in Cancer Cells. Biochim. Biophys. Acta (BBA)—Biomembr. 2015, 1848, 2502–2511. [Google Scholar] [CrossRef] [PubMed]
- Clapp, P.W.; Lavrich, K.S.; van Heusden, C.A.; Lazarowski, E.R.; Carson, J.L.; Jaspers, I. Cinnamaldehyde in Flavored E-Cigarette Liquids Temporarily Suppresses Bronchial Epithelial Cell Ciliary Motility by Dysregulation of Mitochondrial Function. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2019, 316, L470–L486. [Google Scholar] [CrossRef] [PubMed]
- Borodovsky, J.T.; Lee, D.C.; Crosier, B.S.; Gabrielli, J.L.; Sargent, J.D.; Budney, A.J. U.S. Cannabis Legalization and Use of Vaping and Edible Products among Youth. Drug Alcohol. Depend. 2017, 177, 299–306. [Google Scholar] [CrossRef]
- Jett, J.; Stone, E.; Warren, G.; Cummings, K.M. Cannabis Use, Lung Cancer, and Related Issues. J. Thorac. Oncol. 2018, 13, 480–487. [Google Scholar] [CrossRef]
- Fataar, F.; Hammond, D. The Prevalence of Vaping and Smoking as Modes of Delivery for Nicotine and Cannabis among Youth in Canada, England and the United States. Int. J. Environ. Res. Public Health 2019, 16, 4111. [Google Scholar] [CrossRef]
- Pomahacova, B.; Van der Kooy, F.; Verpoorte, R. Cannabis Smoke Condensate III: The Cannabinoid Content of Vaporised Cannabis Sativa. Inhal. Toxicol. 2009, 21, 1108–1112. [Google Scholar] [CrossRef]
- Love, C.A.; Kim, H.-Y.H.; Tallman, K.A.; Clapp, P.W.; Porter, N.A.; Jaspers, I. Vaping Induced Cannabidiol (CBD) Oxidation Product CBD Quinone Forms Protein Adducts with KEAP1 and Activates KEAP1-Nrf2 Genes. Chem. Res. Toxicol. 2023. [Google Scholar] [CrossRef]
- Leigh, N.J.; Goniewicz, M.L. Acute Effect of Electronic Cigarette-Generated Aerosol from Flavored CBD-Containing Refill Solutions on Human Bronchial Epithelial Cells. Front. Physiol. 2020, 11. [Google Scholar] [CrossRef]
- Muthumalage, T.; Rahman, I. Cannabidiol Differentially Regulates Basal and LPS-Induced Inflammatory Responses in Macrophages, Lung Epithelial Cells, and Fibroblasts. Toxicol. Appl. Pharmacol. 2019, 382, 114713. [Google Scholar] [CrossRef]
- Zhang, L.R.; Morgenstern, H.; Greenland, S.; Chang, S.-C.; Lazarus, P.; Teare, M.D.; Woll, P.J.; Orlow, I.; Cox, B.; Cannabis and Respiratory Disease Research Group of New Zealand; et al. Cannabis Smoking and Lung Cancer Risk: Pooled Analysis in the International Lung Cancer Consortium. Int. J. Cancer 2015, 136, 894–903. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.F.; Lefever, T.W.; Cortes, R.A.; Grabenauer, M.; Kovach, A.L.; Cox, A.O.; Patel, P.R.; Pollard, G.T.; Marusich, J.A.; Kevin, R.C.; et al. Thermolytic Degradation of Synthetic Cannabinoids: Chemical Exposures and Pharmacological Consequences. J. Pharmacol. Exp. Ther. 2017, 361, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Marrocco, A.; Singh, D.; Christiani, D.; Demokritou, P. E-Cigarette (E-Cig) Liquid Composition and Operational Voltage Define the In Vitro Toxicity of Δ8Tetrahydrocannabinol/Vitamin E Acetate (Δ8THC/VEA) E-Cig Aerosols. Toxicol. Sci. Off. J. Soc. Toxicol. 2022, 187. [Google Scholar] [CrossRef] [PubMed]
- Hooper, R.W.; Garfield, J.L. An Emerging Crisis: Vaping-Associated Pulmonary Injury. Ann. Intern. Med. 2020, 172, 57–58. [Google Scholar] [CrossRef]
- Ellington, S. Update: Product, Substance-Use, and Demographic Characteristics of Hospitalized Patients in a Nationwide Outbreak of E-Cigarette, or Vaping, Product Use–Associated Lung Injury—United States, August 2019–January 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69. [Google Scholar] [CrossRef]
- Blount, B.C.; Karwowski, M.P.; Shields, P.G.; Morel-Espinosa, M.; Valentin-Blasini, L.; Gardner, M.; Braselton, M.; Brosius, C.R.; Caron, K.T.; Chambers, D.; et al. Vitamin E Acetate in Bronchoalveolar-Lavage Fluid Associated with EVALI. N. Engl. J. Med. 2020, 382, 697–705. [Google Scholar] [CrossRef]
- Sund, L.J.; Dargan, P.I.; Archer, J.R.H.; Wood, D.M. E-Cigarette or Vaping-Associated Lung Injury (EVALI): A Review of International Case Reports from Outside the United States of America. Clin. Toxicol. 2023, 61, 91–97. [Google Scholar] [CrossRef]
- Wu, D.; O’Shea, D.F. Potential for Release of Pulmonary Toxic Ketene from Vaping Pyrolysis of Vitamin E Acetate. Proc. Natl. Acad. Sci. USA 2020, 117, 6349–6355. [Google Scholar] [CrossRef]
- Committee on Acute Exposure Guideline Levels; Committee on Toxicology; Board on Environmental Studies and Toxicology; Division on Earth and Life Studies; National Research Council. Acute Exposure Guideline Levels for Selected Airborne Chemicals: Volume 16; National Academies Press (US): Washington, DC, USA, 2014; ISBN 978-0-309-30096-4.
- Bitzer, Z.T.; Goel, R.; Reilly, S.M.; Elias, R.J.; Silakov, A.; Foulds, J.; Muscat, J.; Richie, J.P. Effect of Flavoring Chemicals on Free Radical Formation in Electronic Cigarette Aerosols. Free Radic. Biol. Med. 2018, 120, 72–79. [Google Scholar] [CrossRef]
- Durrani, K.; El Din, S.-M.A.; Sun, Y.; Rule, A.M.; Bressler, J. Ethyl Maltol Enhances Copper Mediated Cytotoxicity in Lung Epithelial Cells. Toxicol. Appl. Pharmacol. 2021, 410, 115354. [Google Scholar] [CrossRef]
- Weng, M.; Lee, H.-W.; Park, S.-H.; Hu, Y.; Wang, H.-T.; Chen, L.-C.; Rom, W.N.; Huang, W.C.; Lepor, H.; Wu, X.-R.; et al. Aldehydes Are the Predominant Forces Inducing DNA Damage and Inhibiting DNA Repair in Tobacco Smoke Carcinogenesis. Proc. Natl. Acad. Sci. USA 2018, 115, E6152–E6161. [Google Scholar] [CrossRef] [PubMed]
- Canchola, A.; Ahmed, C.M.S.; Chen, K.; Chen, J.Y.; Lin, Y.-H. Formation of Redox-Active Duroquinone from Vaping of Vitamin E Acetate Contributes to Oxidative Lung Injury. Chem. Res. Toxicol. 2022, 35, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Muthumalage, T.; Lucas, J.H.; Wang, Q.; Lamb, T.; McGraw, M.D.; Rahman, I. Pulmonary Toxicity and Inflammatory Response of Vape Cartridges Containing Medium-Chain Triglycerides Oil and Vitamin E Acetate: Implications in the Pathogenesis of EVALI. Toxics 2020, 8, 46. [Google Scholar] [CrossRef]
- Jităreanu, A.; Cara, I.G.; Sava, A.; Mârțu, I.; Caba, I.-C.; Agoroaei, L. The Impact of the Storage Conditions and Type of Clearomizers on the Increase of Heavy Metal Levels in Electronic Cigarette Liquids Retailed in Romania. Toxics 2022, 10, 126. [Google Scholar] [CrossRef] [PubMed]
- Din, A.E.; Mohsen, S.-M. The Flavoring Ethyl Maltol, Found in E-Cigarettes, Mediates Metal Cellular Toxicity. Ph.D. Thesis, Johns Hopkins University, Baltimore, MD, USA, 2020. [Google Scholar]
- Kamilari, E.; Farsalinos, K.; Poulas, K.; Kontoyannis, C.G.; Orkoula, M.G. Detection and Quantitative Determination of Heavy Metals in Electronic Cigarette Refill Liquids Using Total Reflection X-Ray Fluorescence Spectrometry. Food Chem. Toxicol. 2018, 116, 233–237. [Google Scholar] [CrossRef]
- Gray, N.; Halstead, M.; Gonzalez-Jimenez, N.; Valentin-Blasini, L.; Watson, C.; Pappas, R.S. Analysis of Toxic Metals in Liquid from Electronic Cigarettes. Int. J. Environ. Res. Public Health 2019, 16, 4450. [Google Scholar] [CrossRef]
- Na, C.-J.; Jo, S.-H.; Kim, K.-H.; Sohn, J.-R.; Son, Y.-S. The Transfer Characteristics of Heavy Metals in Electronic Cigarette Liquid. Environ. Res. 2019, 174, 152–159. [Google Scholar] [CrossRef]
- Mikheev, V.B.; Brinkman, M.C.; Granville, C.A.; Gordon, S.M.; Clark, P.I. Real-Time Measurement of Electronic Cigarette Aerosol Size Distribution and Metals Content Analysis. Nicotine Tob. Res. 2016, 18, 1895–1902. [Google Scholar] [CrossRef]
- Mo, Y.; Jiang, M.; Zhang, Y.; Wan, R.; Li, J.; Zhong, C.-J.; Li, H.; Tang, S.; Zhang, Q. Comparative Mouse Lung Injury by Nickel Nanoparticles with Differential Surface Modification. J. Nanobiotechnol. 2019, 17, 2. [Google Scholar] [CrossRef]
- Re, D.B.; Hilpert, M.; Saglimbeni, B.; Strait, M.; Ilievski, V.; Coady, M.; Talayero, M.; Wilmsen, K.; Chesnais, H.; Balac, O.; et al. Exposure to E-Cigarette Aerosol over Two Months Induces Accumulation of Neurotoxic Metals and Alteration of Essential Metals in Mouse Brain. Environ. Res. 2021, 202, 111557. [Google Scholar] [CrossRef]
- Wiener, R.C.; Bhandari, R. Association of Electronic Cigarette Use with Lead, Cadmium, Barium, and Antimony Body Burden: NHANES 2015–2016. J. Trace Elem. Med. Biol. 2020, 62, 126602. [Google Scholar] [CrossRef] [PubMed]
- Fowles, J.; Barreau, T.; Wu, N. Cancer and Non-Cancer Risk Concerns from Metals in Electronic Cigarette Liquids and Aerosols. Int. J. Environ. Res. Public Health 2020, 17, 2146. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Aravindakshan, A.; Hilpert, M.; Olmedo, P.; Rule, A.M.; Navas-Acien, A.; Aherrera, A. Metal/Metalloid Levels in Electronic Cigarette Liquids, Aerosols, and Human Biosamples: A Systematic Review. Environ. Health Perspect. 2020, 128, 036001. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Wise, J.T.F.; Wang, L.; Schumann, K.; Zhang, Z.; Shi, X. Dual Roles of Oxidative Stress in Metal Carcinogenesis. JEP(T) 2017, 36. [Google Scholar] [CrossRef]
- Hess, C.A.; Olmedo, P.; Navas-Acien, A.; Goessler, W.; Cohen, J.E.; Rule, A.M. E-Cigarettes as a Source of Toxic and Potentially Carcinogenic Metals. Environ. Res. 2017, 152, 221–225. [Google Scholar] [CrossRef]
- Blair, A.; Freeman, L.B. Lung Cancer among Nonsmokers. Epidemiology 2006, 17, 601–603. [Google Scholar] [CrossRef]
- Samet, J.M.; Avila-Tang, E.; Boffetta, P.; Hannan, L.M.; Olivo-Marston, S.; Thun, M.J.; Rudin, C.M. Lung Cancer in Never Smokers: Clinical Epidemiology and Environmental Risk Factors. Clin. Cancer Res. 2009, 15, 5626–5645. [Google Scholar] [CrossRef]
- Xue, Y.; Wang, L.; Zhang, Y.; Zhao, Y.; Liu, Y. Air Pollution: A Culprit of Lung Cancer. J. Hazard. Mater. 2022, 434, 128937. [Google Scholar] [CrossRef]
- Aalami, A.H.; Hoseinzadeh, M.; Hosseini Manesh, P.; Jiryai Sharahi, A.; Kargar Aliabadi, E. Carcinogenic Effects of Heavy Metals by Inducing Dysregulation of MicroRNAs: A Review. Mol. Biol. Rep. 2022, 49, 12227–12238. [Google Scholar] [CrossRef]
- Brenner, D.R.; Boffetta, P.; Duell, E.J.; Bickeböller, H.; Rosenberger, A.; McCormack, V.; Muscat, J.E.; Yang, P.; Wichmann, H.-E.; Brueske-Hohlfeld, I.; et al. Previous Lung Diseases and Lung Cancer Risk: A Pooled Analysis from the International Lung Cancer Consortium. Am. J. Epidemiol. 2012, 176, 573–585. [Google Scholar] [CrossRef]
- Porro, C.; La Torre, M.E.; Tartaglia, N.; Benameur, T.; Santini, M.; Ambrosi, A.; Messina, G.; Cibelli, G.; Fiorelli, A.; Polito, R.; et al. The Potential Role of Nutrition in Lung Cancer Establishment and Progression. Life 2022, 12, 270. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Gümüş, Z.H.; Colarossi, C.; Memeo, L.; Wang, X.; Kong, C.Y.; Boffetta, P. SCLC: Epidemiology, Risk Factors, Genetic Susceptibility, Molecular Pathology, Screening, and Early Detection. J. Thorac. Oncol. 2023, 18, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Tu, Z.; Chen, H.; Liu, Z. Identifying Modifiable Risk Factors of Lung Cancer: Indications from Mendelian Randomization. PLoS ONE 2021, 16, e0258498. [Google Scholar] [CrossRef] [PubMed]
- Tran, K.B.; Lang, J.J.; Compton, K.; Xu, R.; Acheson, A.R.; Henrikson, H.J.; Kocarnik, J.M.; Penberthy, L.; Aali, A.; Abbas, Q.; et al. The Global Burden of Cancer Attributable to Risk Factors, 2010–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 563–591. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-J.; Gan, R.-Y.; Li, S.; Zhou, Y.; Li, A.-N.; Xu, D.-P.; Li, H.-B. Antioxidant Phytochemicals for the Prevention and Treatment of Chronic Diseases. Molecules 2015, 20, 21138–21156. [Google Scholar] [CrossRef]
- Zhai, T.; Li, S.; Hu, W.; Li, D.; Leng, S. Potential Micronutrients and Phytochemicals against the Pathogenesis of Chronic Obstructive Pulmonary Disease and Lung Cancer. Nutrients 2018, 10, 813. [Google Scholar] [CrossRef]
- Dogan, S.; Shen, R.; Ang, D.C.; Johnson, M.L.; D’Angelo, S.P.; Paik, P.K.; Brzostowski, E.B.; Riely, G.J.; Kris, M.G.; Zakowski, M.F.; et al. Molecular Epidemiology of EGFR and KRAS Mutations in 3,026 Lung Adenocarcinomas: Higher Susceptibility of Women to Smoking-Related KRAS-Mutant Cancers. Clin. Cancer Res. 2012, 18, 6169–6177. [Google Scholar] [CrossRef]
- Alexandrov, L.B.; Ju, Y.S.; Haase, K.; Van Loo, P.; Martincorena, I.; Nik-Zainal, S.; Totoki, Y.; Fujimoto, A.; Nakagawa, H.; Shibata, T.; et al. Mutational Signatures Associated with Tobacco Smoking in Human Cancer. Science 2016, 354, 618–622. [Google Scholar] [CrossRef]
- Landi, M.T.; Synnott, N.C.; Rosenbaum, J.; Zhang, T.; Zhu, B.; Shi, J.; Zhao, W.; Kebede, M.; Sang, J.; Choi, J.; et al. Tracing Lung Cancer Risk Factors Through Mutational Signatures in Never-Smokers: The Sherlock-Lung Study. Am. J. Epidemiol. 2021, 190, 962–976. [Google Scholar] [CrossRef]
- Ernst, S.M.; Mankor, J.M.; van Riet, J.; von der Thüsen, J.H.; Dubbink, H.J.; Aerts, J.G.J.V.; de Langen, A.J.; Smit, E.F.; Dingemans, A.-M.C.; Monkhorst, K. Tobacco Smoking-Related Mutational Signatures in Classifying Smoking-Associated and Nonsmoking-Associated NSCLC. J. Thorac. Oncol. 2023, 18, 487–498. [Google Scholar] [CrossRef]
- Inamura, K.; Hamada, T.; Bullman, S.; Ugai, T.; Yachida, S.; Ogino, S. Cancer as Microenvironmental, Systemic and Environmental Diseases: Opportunity for Transdisciplinary Microbiomics Science. Gut 2022, 71, 2107–2122. [Google Scholar] [CrossRef] [PubMed]
- El Ghissassi, F.; Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; Galichet, L.; et al. A Review of Human Carcinogens—Part D: Radiation. Lancet Oncol. 2009, 10, 751–752. [Google Scholar] [CrossRef] [PubMed]
- Schauer, D.A.; Linton, O.W. NCRP Report No. 160, Ionizing Radiation Exposure of the Population of the United States, Medical Exposure—Are We Doing Less with More, and Is There a Role for Health Physicists? Health Phys. 2009, 97, 1. [Google Scholar] [CrossRef] [PubMed]
- Spencer, J.E. Radon Gas: A Geologic Hazard in Arizona; Arizona Geological Survey Down-to-Earth Series DTE-2; University of Arizona: Tucson, AZ, USA, 1992; 24p, Available online: http://hdl.handle.net/10150/628821 (accessed on 21 June 2023).
- Report No. 160—Ionizing Radiation Exposure of the Population of the United States (2009); NCRP: Bethesda, MD, USA; Available online: https://ncrponline.org/shop/reports/report-no-160-ionizing-radiation-exposure-of-the-population-of-the-united-states/ (accessed on 12 April 2023).
- Akerblom, G.; Wilson, C. Radon—Geological Aspects of an Environmental Problem: Environmental Radon Investigation in Sweden—Regional Environmental Documentation of Natural Radiation in Sweden; Sveriges Geologiska Undersoekning: Uppsala, Sweden, 1982. [Google Scholar]
- Kreienbrock, L.; Kreuzer, M.; Gerken, M.; Dingerkus, G.; Wellmann, J.; Keller, G.; Erich Wichmann, H. Case-Control Study on Lung Cancer and Residential Radon in Western Germany. Am. J. Epidemiol. 2001, 153, 42–52. [Google Scholar] [CrossRef]
- Zeeb, H.; Shannoun, F.; World Health Organization. WHO Handbook on Indoor Radon: A Public Health Perspective; World Health Organization: Geneva, Switzerland, 2009; Available online: https://apps.who.int/iris/handle/10665/44149 (accessed on 21 June 2023).
- Riudavets, M.; Garcia de Herreros, M.; Besse, B.; Mezquita, L. Radon and Lung Cancer: Current Trends and Future Perspectives. Cancers 2022, 14, 3142. [Google Scholar] [CrossRef]
- Darby, S.; Hill, D.; Auvinen, A.; Barros-Dios, J.M.; Baysson, H.; Bochicchio, F.; Deo, H.; Falk, R.; Forastiere, F.; Hakama, M.; et al. Radon in Homes and Risk of Lung Cancer: Collaborative Analysis of Individual Data from 13 European Case-Control Studies. BMJ 2005, 330, 223. [Google Scholar] [CrossRef]
- Samet, J.M.; Kutvirt, D.M.; Waxweiler, R.J.; Key, C.R. Uranium Mining and Lung Cancer in Navajo Men. N. Engl. J. Med. 1984, 310, 1481–1484. [Google Scholar] [CrossRef]
- Greenberg, M.; Selikoff, I.J. Lung Cancer in the Schneeberg Mines: A Reappraisal of the Data Reported by Harting and Hesse in 1879. Ann. Occup. Hyg. 1993, 37, 5–14. [Google Scholar] [CrossRef]
- Grosche, B.; Kreuzer, M.; Kreisheimer, M.; Schnelzer, M.; Tschense, A. Lung Cancer Risk among German Male Uranium Miners: A Cohort Study, 1946–1998. Br. J. Cancer 2006, 95, 1280–1287. [Google Scholar] [CrossRef]
- Lorenzo-González, M.; Ruano-Ravina, A.; Torres-Durán, M.; Kelsey, K.T.; Provencio, M.; Parente-Lamelas, I.; Leiro-Fernández, V.; Vidal-García, I.; Castro-Añón, O.; Martínez, C.; et al. Residential Radon, Genetic Polymorphisms in DNA Damage and Repair-Related. Lung Cancer 2019, 135, 10–15. [Google Scholar] [CrossRef]
- Robertson, A.; Allen, J.; Laney, R.; Curnow, A. The Cellular and Molecular Carcinogenic Effects of Radon Exposure: A Review. Int. J. Mol. Sci. 2013, 14, 14024–14063. [Google Scholar] [CrossRef] [PubMed]
- Weaver, D.A.; Hei, T.K.; Hukku, B.; McRaven, J.A.; Willey, J.C. Cytogenetic and Molecular Genetic Analysis of Tumorigenic Human Bronchial Epithelial Cells Induced by Radon Alpha Particles. Carcinogenesis 1997, 18, 1251–1257. [Google Scholar] [CrossRef]
- Meenakshi, C.; Sivasubramanian, K.; Venkatraman, B. Nucleoplasmic Bridges as a Biomarker of DNA Damage Exposed to Radon. Mutat. Res./Genet. Toxicol. Environ. Mutagen. 2017, 814, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.M.; Choi, J.W.; Hong, M.H.; Jung, D.; Lee, C.Y.; Park, S.Y.; Shim, H.S.; Sheen, S.; Kwak, K.I.; Kang, D.R.; et al. Indoor Radon Exposure Increases Tumor Mutation Burden in Never-Smoker Patients with Lung Adenocarcinoma. Lung Cancer 2019, 131, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Wang, D.; Gu, C.; Liu, X.; Pei, W.; Li, J.; Cao, Y.; Jiao, Y.; Tong, J.; Nie, J. Down-Regulation of Let-7 MicroRNA Increased K-Ras Expression in Lung Damage Induced by Radon. Environ. Toxicol. Pharmacol. 2015, 40, 541–548. [Google Scholar] [CrossRef]
- Bersimbaev, R.; Pulliero, A.; Bulgakova, O.; Kussainova, A.; Aripova, A.; Izzotti, A. Radon Biomonitoring and MicroRNA in Lung Cancer. Int. J. Mol. Sci. 2020, 21, 2154. [Google Scholar] [CrossRef]
- Czochor, J.R.; Glazer, P.M. MicroRNAs in Cancer Cell Response to Ionizing Radiation. Antioxid. Redox Signal. 2014, 21, 293–312. [Google Scholar] [CrossRef]
- Wei, W.; Dong, Z.; Gao, H.; Zhang, Y.-Y.; Shao, L.-H.; Jin, L.-L.; Lv, Y.-H.; Zhao, G.; Shen, Y.-N.; Jin, S.-Z. MicroRNA-9 Enhanced Radiosensitivity and Its Mechanism of DNA Methylation in Non-Small Cell Lung Cancer. Gene 2019, 710, 178–185. [Google Scholar] [CrossRef]
- Nie, J.; Wu, J.; Chen, Z.; Jiao, Y.; Zhang, J.; Tian, H.; Li, J.; Tong, J. Expression Profiles of Long Non-Coding RNA in Mouse Lung Tissue Exposed to Radon. J. Toxicol. Environ. Health Part A 2019, 82, 854–861. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Polychlorinated Dibenzo-para-dioxins and Polychlorinated Dibenzofurans. Lyon (FR): International Agency for Research on Cancer; 1997. (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 69.). Available online: https://www.ncbi.nlm.nih.gov/books/NBK409980/ (accessed on 21 June 2023).
- Grantzau, T.; Overgaard, J. Risk of Second Non-Breast Cancer after Radiotherapy for Breast Cancer: A Systematic Review and Meta-Analysis of 762,468 Patients. Radiother. Oncol. 2015, 114, 56–65. [Google Scholar] [CrossRef]
- Neugut, A.I.; Lee, W.C.; Murray, T.; Robinson, E.; Karwoski, K.; Kutcher, G.J. Lung Cancer after Radiation Therapy for Breast Cancer. Cancer 1993, 71, 3054–3057. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, M.; Li, Z.; Yue, J.; Xu, M.; Zhang, Y.; Yung, K.K.L.; Li, R. Fine Particulate Matter Induces Mitochondrial Dysfunction and Oxidative Stress in Human SH-SY5Y Cells. Chemosphere 2019, 218, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Losacco, C.; Perillo, A. Particulate Matter Air Pollution and Respiratory Impact on Humans and Animals. Environ. Sci. Pollut. Res. 2018, 25, 33901–33910. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Zhou, X.; Zhu, Y.; Li, D.; Jing, D.; Su, X.; Pan, P.; Liu, H.; Zhang, Y. Association of Outdoor Air Pollution, Lifestyle, Genetic Factors with the Risk of Lung Cancer: A Prospective Cohort Study. Environ. Res. 2023, 218, 114996. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.-H.; Tsuang, B.-J.; Chiang, C.-J.; Ku, K.-C.; Tseng, J.-S.; Yang, T.-Y.; Hsu, K.-H.; Chen, K.-C.; Yu, S.-L.; Lee, W.-C.; et al. The Relationship Between Air Pollution and Lung Cancer in Nonsmokers in Taiwan. J. Thorac. Oncol. 2019, 14, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-Year Trends of the Global Burden of Disease Attributable to Ambient Air Pollution: An Analysis of Data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Hill, W.; Lim, E.L.; Weeden, C.E.; Lee, C.; Augustine, M.; Chen, K.; Kuan, F.-C.; Marongiu, F.; Evans, E.J.; Moore, D.A.; et al. Lung Adenocarcinoma Promotion by Air Pollutants. Nature 2023, 616, 159–167. [Google Scholar] [CrossRef]
- Mu, L.; Liu, L.; Niu, R.; Zhao, B.; Shi, J.; Li, Y.; Swanson, M.; Scheider, W.; Su, J.; Chang, S.-C.; et al. Indoor Air Pollution and Risk of Lung Cancer among Chinese Female Non-Smokers. Cancer Causes Control 2013, 24, 439–450. [Google Scholar] [CrossRef]
- Guo, H.; Li, W.; Wu, J. Ambient PM2.5 and Annual Lung Cancer Incidence: A Nationwide Study in 295 Chinese Counties. Int. J. Environ. Res. Public Health 2020, 17, 1481. [Google Scholar] [CrossRef]
- Hvidtfeldt, U.A.; Severi, G.; Andersen, Z.J.; Atkinson, R.; Bauwelinck, M.; Bellander, T.; Boutron-Ruault, M.-C.; Brandt, J.; Brunekreef, B.; Cesaroni, G.; et al. Long-Term Low-Level Ambient Air Pollution Exposure and Risk of Lung Cancer—A Pooled Analysis of 7 European Cohorts. Environ. Int. 2021, 146, 106249. [Google Scholar] [CrossRef]
- Stavroulas, I.; Grivas, G.; Michalopoulos, P.; Liakakou, E.; Bougiatioti, A.; Kalkavouras, P.; Fameli, K.M.; Hatzianastassiou, N.; Mihalopoulos, N.; Gerasopoulos, E. Field Evaluation of Low-Cost PM Sensors (Purple Air PA-II) Under Variable Urban Air Quality Conditions, in Greece. Atmosphere 2020, 11, 926. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhu, D.; Cui, B.; Ding, R.; Shi, X.; He, P. Association between Particulate Matter Air Pollution and Lung Cancer. Thorax 2020, 75, 85–87. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.Y.; Yang, J.; He, J.; Yang, X.; Hubbard, R.; Ji, D. An Investigation into the Impact of Variations of Ambient Air Pollution and Meteorological Factors on Lung Cancer Mortality in Yangtze River Delta. Sci. Total Environ. 2021, 779, 146427. [Google Scholar] [CrossRef] [PubMed]
- Pun, V.C.; Kazemiparkouhi, F.; Manjourides, J.; Suh, H.H. Long-Term PM2.5 Exposure and Respiratory, Cancer, and Cardiovascular Mortality in Older US Adults. Am. J. Epidemiol. 2017, 186, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Badaloni, C.; Gariazzo, C.; Stafoggia, M.; Sozzi, R.; Davoli, M.; Forastiere, F. Long-Term Exposure to Urban Air Pollution and Mortality in a Cohort of More than a Million Adults in Rome. Environ. Health Perspect. 2013, 121, 324–331. [Google Scholar] [CrossRef]
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Stafoggia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B.; et al. Air Pollution and Lung Cancer Incidence in 17 European Cohorts: Prospective Analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol. 2013, 14, 813–822. [Google Scholar] [CrossRef]
- Tomczak, A.; Miller, A.B.; Weichenthal, S.A.; To, T.; Wall, C.; van Donkelaar, A.; Martin, R.V.; Crouse, D.L.; Villeneuve, P.J. Long-Term Exposure to Fine Particulate Matter Air Pollution and the Risk of Lung Cancer among Participants of the Canadian National Breast Screening Study. Int. J. Cancer 2016, 139, 1958–1966. [Google Scholar] [CrossRef]
- Hart, J.E.; Spiegelman, D.; Beelen, R.; Hoek, G.; Brunekreef, B.; Schouten, L.J.; van den Brandt, P. Long-Term Ambient Residential Traffic–Related Exposures and Measurement Error–Adjusted Risk of Incident Lung Cancer in the Netherlands Cohort Study on Diet and Cancer. Environ. Health Perspect. 2015, 123, 860–866. [Google Scholar] [CrossRef]
- Balmain, A. Air Pollution’s Role in the Promotion of Lung Cancer. Nature 2023, 616, 35–36. [Google Scholar] [CrossRef]
- Liu, C.; Guo, H.; Cheng, X.; Shao, M.; Wu, C.; Wang, S.; Li, H.; Wei, L.; Gao, Y.; Tan, W.; et al. Exposure to Airborne PM2.5 Suppresses MicroRNA Expression and Deregulates Target Oncogenes That Cause Neoplastic Transformation in NIH3T3 Cells. Oncotarget 2015, 6, 29428–29439. [Google Scholar] [CrossRef]
- Ali, H.; Khan, E. What Are Heavy Metals? Long-Standing Controversy over the Scientific Use of the Term ‘Heavy Metals’—Proposal of a Comprehensive Definition. Toxicol. Environ. Chem. 2018, 100, 6–19. [Google Scholar] [CrossRef]
- Dixit, R.; Wasiullah; Malaviya, D.; Pandiyan, K.; Singh, U.B.; Sahu, A.; Shukla, R.; Singh, B.P.; Rai, J.P.; Sharma, P.K.; et al. Bioremediation of Heavy Metals from Soil and Aquatic Environment: An Overview of Principles and Criteria of Fundamental Processes. Sustainability 2015, 7, 2189–2212. [Google Scholar] [CrossRef]
- Siddiqua, A.; Hahladakis, J.N.; Al-Attiya, W.A.K.A. An Overview of the Environmental Pollution and Health Effects Associated with Waste Landfilling and Open Dumping. Environ. Sci. Pollut. Res. 2022, 29, 58514–58536. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.F.; Kumar, P.S.; Rozbu, M.R.; Chowdhury, A.T.; Nuzhat, S.; Rafa, N.; Mahlia, T.M.I.; Ong, H.C.; Mofijur, M. Heavy Metal Toxicity, Sources, and Remediation Techniques for Contaminated Water and Soil. Environ. Technol. Innov. 2022, 25, 102114. [Google Scholar] [CrossRef]
- Xu, X.; Liao, W.; Lin, Y.; Dai, Y.; Shi, Z.; Huo, X. Blood Concentrations of Lead, Cadmium, Mercury and Their Association with Biomarkers of DNA Oxidative Damage in Preschool Children Living in an e-Waste Recycling Area. Environ. Geochem. Health 2018, 40, 1481–1494. [Google Scholar] [CrossRef]
- Alabi, O.A.; Adeoluwa, Y.M.; Huo, X.; Xu, X.; Bakare, A.A. Environmental Contamination and Public Health Effects of Electronic Waste: An Overview. J. Environ. Health Sci. Eng. 2021, 19, 1209–1227. [Google Scholar] [CrossRef]
- Jaishankar, M.; Tseten, T.; Anbalagan, N.; Mathew, B.B.; Beeregowda, K.N. Toxicity, Mechanism and Health Effects of Some Heavy Metals. Interdiscip. Toxicol. 2014, 7, 60–72. [Google Scholar] [CrossRef]
- Luo, J.; Hendryx, M.; Ducatman, A. Association between Six Environmental Chemicals and Lung Cancer Incidence in the United States. J. Environ. Public Health 2011, 2011, e463701. [Google Scholar] [CrossRef]
- Balali-Mood, M.; Naseri, K.; Tahergorabi, Z.; Khazdair, M.R.; Sadeghi, M. Toxic Mechanisms of Five Heavy Metals: Mercury, Lead, Chromium, Cadmium, and Arsenic. Front. Pharmacol. 2021, 12. [Google Scholar] [CrossRef]
- Lee, N.-W.; Wang, H.-Y.; Du, C.-L.; Yuan, T.-H.; Chen, C.-Y.; Yu, C.-J.; Chan, C.-C. Air-Polluted Environmental Heavy Metal Exposure Increase Lung Cancer Incidence and Mortality: A Population-Based Longitudinal Cohort Study. Sci. Total Environ. 2022, 810, 152186. [Google Scholar] [CrossRef]
- Genchi, G.; Sinicropi, M.S.; Lauria, G.; Carocci, A.; Catalano, A. The Effects of Cadmium Toxicity. Int. J. Environ. Res. Public Health 2020, 17, 3782. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Exposure to Cadmium: A Major Public Health Concern; World Health Organization: Geneva, Switzerland, 2010; Available online: www.who.int/ipcs/features/cadmium.pdf (accessed on 13 January 2015).
- Taha, M.M.; Mahdy-Abdallah, H.; Shahy, E.M.; Ibrahim, K.S.; Elserougy, S. Impact of Occupational Cadmium Exposure on Bone in Sewage Workers. Int. J. Occup. Environ. Health 2018, 24, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Mezynska, M.; Brzóska, M.M. Environmental Exposure to Cadmium—A Risk for Health of the General Population in Industrialized Countries and Preventive Strategies. Environ. Sci. Pollut. Res. 2018, 25, 3211–3232. [Google Scholar] [CrossRef] [PubMed]
- Nawrot, T.S.; Martens, D.S.; Hara, A.; Plusquin, M.; Vangronsveld, J.; Roels, H.A.; Staessen, J.A. Association of Total Cancer and Lung Cancer with Environmental Exposure to Cadmium: The Meta-Analytical Evidence. Cancer Causes Control 2015, 26, 1281–1288. [Google Scholar] [CrossRef]
- Demir, N.; Enon, S.; Turksoy, V.A.; Kayaalti, Z.; Kaya, S.; Cangir, A.K.; Soylemezoglu, T.; Savas, I. Association of Cadmium but Not Arsenic Levels in Lung Cancer Tumor Tissue with Smoking, Histopathological Type and Stage. Asian Pac. J. Cancer Prev. 2014, 15, 2965–2970. [Google Scholar] [CrossRef]
- Ahamed, M.; Akhtar, M.J.; Alhadlaq, H.A. Combined Effect of Single-Walled Carbon Nanotubes and Cadmium on Human Lung Cancer Cells. Environ. Sci. Pollut. Res. 2022, 29, 87844–87857. [Google Scholar] [CrossRef]
- Liu, J.; Qu, W.; Kadiiska, M.B. Role of Oxidative Stress in Cadmium Toxicity and Carcinogenesis. Toxicol. Appl. Pharmacol. 2009, 238, 209–214. [Google Scholar] [CrossRef]
- Waisberg, M.; Joseph, P.; Hale, B.; Beyersmann, D. Molecular and Cellular Mechanisms of Cadmium Carcinogenesis. Toxicology 2003, 192, 95–117. [Google Scholar] [CrossRef]
- Rao, C.V.; Pal, S.; Mohammed, A.; Farooqui, M.; Doescher, M.P.; Asch, A.S.; Yamada, H.Y. Biological Effects and Epidemiological Consequences of Arsenic Exposure, and Reagents That Can Ameliorate Arsenic Damage in Vivo. Oncotarget 2017, 8, 57605–57621. [Google Scholar] [CrossRef]
- Smith, A.H.; Ercumen, A.; Yuan, Y.; Steinmaus, C.M. Increased Lung Cancer Risks Are Similar Whether Arsenic Is Ingested or Inhaled. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 343–348. [Google Scholar] [CrossRef]
- Monteiro De Oliveira, E.C.; Caixeta, E.S.; Santos, V.S.V.; Pereira, B.B. Arsenic Exposure from Groundwater: Environmental Contamination, Human Health Effects, and Sustainable Solutions. J. Toxicol. Environ. Health Part B 2021, 24, 119–135. [Google Scholar] [CrossRef] [PubMed]
- Folesani, G.; Galetti, M.; Petronini, P.G.; Mozzoni, P.; La Monica, S.; Cavallo, D.; Corradi, M. Interaction between Occupational and Non-Occupational Arsenic Exposure and Tobacco Smoke on Lung Cancerogenesis: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 4167. [Google Scholar] [CrossRef] [PubMed]
- Hertz-Picciotto, I.; Smith, A.H.; Holtzman, D.; Lipsett, M.; Alexeeff, G. Synergism between Occupational Arsenic Exposure and Smoking in the Induction of Lung Cancer. Epidemiology 1992, 3, 23. [Google Scholar] [CrossRef] [PubMed]
- CDC. Immediately Dangerous to Life or Health Concentrations (IDLH): Arsine—NIOSH Publications and Products. Available online: https://www.cdc.gov/niosh/idlh/7784421.html (accessed on 15 April 2023).
- Thomas, D.J. Molecular Processes in Cellular Arsenic Metabolism. Toxicol. Appl. Pharmacol. 2007, 222, 365–373. [Google Scholar] [CrossRef]
- Lewis, A.S.; Beyer, L.A.; Zu, K. Considerations in Deriving Quantitative Cancer Criteria for Inorganic Arsenic Exposure via Inhalation. Environ. Int. 2015, 74, 258–273. [Google Scholar] [CrossRef] [PubMed]
- Steinmaus, C.M.; Ferreccio, C.; Romo, J.A.; Yuan, Y.; Cortes, S.; Marshall, G.; Moore, L.E.; Balmes, J.R.; Liaw, J.; Golden, T.; et al. Drinking Water Arsenic in Northern Chile: High Cancer Risks 40 Years after Exposure Cessation. Cancer Epidemiol. Biomark. Prev. 2013, 22, 623–630. [Google Scholar] [CrossRef]
- Dauphiné, D.C.; Ferreccio, C.; Guntur, S.; Yuan, Y.; Hammond, S.K.; Balmes, J.; Smith, A.H.; Steinmaus, C. Lung Function in Adults Following in Utero and Childhood Exposure to Arsenic in Drinking Water: Preliminary Findings. Int. Arch. Occup. Environ. Health 2011, 84, 591–600. [Google Scholar] [CrossRef]
- Steinmaus, C.; Ferreccio, C.; Acevedo, J.; Yuan, Y.; Liaw, J.; Durán, V.; Cuevas, S.; García, J.; Meza, R.; Valdés, R.; et al. Increased Lung and Bladder Cancer Incidence in Adults after In Utero and Early-Life Arsenic Exposure. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1529–1538. [Google Scholar] [CrossRef]
- Georgakilas, A.G. Oxidative Stress, DNA Damage and Repair in Carcinogenesis: Have We Established a Connection? Cancer Lett. 2012, 327, 3–4. [Google Scholar] [CrossRef]
- Islam, R.; Zhao, L.; Zhang, X.; Liu, L.-Z. MiR-218-5p/EGFR Signaling in Arsenic-Induced Carcinogenesis. Cancers 2023, 15, 1204. [Google Scholar] [CrossRef]
- Tang, N.; Zhang, Q.; Fang, S.; Han, X.; Wang, Z. Anti-Tumor Activity of High-Dose EGFR Tyrosine Kinase Inhibitor and Sequential Docetaxel in Wild Type EGFR Non-Small Cell Lung Cancer Cell Nude Mouse Xenografts. Oncotarget 2016, 8, 9134–9143. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Ding, H.; Wang, W.; Liao, Z.; Fu, Z.; Hong, Y.; Zhou, Y.; Zhang, C.-Y.; Chen, X. Tumor-Suppressive MiR-218-5p Inhibits Cancer Cell Proliferation and Migration via EGFR in Non-Small Cell Lung Cancer. Oncotarget 2016, 7, 28075–28085. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Cui, J.; Wu, L.; He, C.; Chen, G. The Role of PD-1/PD-L1 Checkpoint in Arsenic Lung Tumorigenesis. Toxicol. Appl. Pharmacol. 2021, 426, 115633. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Huang, L.; Liu, Y.; Yi, M.; Chu, Q.; Jiao, D.; Wu, K. Metabolic Profiles of Regulatory T Cells and Their Adaptations to the Tumor Microenvironment: Implications for Antitumor Immunity. J. Hematol. Oncol. 2022, 15, 104. [Google Scholar] [CrossRef]
- Cooper, K.L.; Liu, R.; Zhou, X. Particulate Arsenic Trioxide Induces Higher DNA Damage and Reactive Oxygen Species than Soluble Arsenite in Lung Epithelial Cells. Toxicol. Appl. Pharmacol. 2022, 457, 116320. [Google Scholar] [CrossRef]
- Kameda, T.; Takahashi, K.; Kim, R.; Jiang, Y.; Movahed, M.; Park, E.-K.; Rantanen, J. Asbestos: Use, Bans and Disease Burden in Europe. Bull. World Health Organ. 2014, 92, 790–797. [Google Scholar] [CrossRef]
- Norbet, C.; Joseph, A.; Rossi, S.S.; Bhalla, S.; Gutierrez, F.R. Asbestos-Related Lung Disease: A Pictorial Review. Curr. Probl. Diagn. Radiol. 2015, 44, 371–382. [Google Scholar] [CrossRef]
- Huang, S.X.L.; Jaurand, M.-C.; Kamp, D.W.; Whysner, J.; Hei, T.K. Role of Mutagenicity in Asbestos Fiber-Induced Carcinogenicity and Other Diseases. J. Toxicol. Environ. Health Part B 2011, 14, 179–245. [Google Scholar] [CrossRef]
- Ospina, D.; Villegas, V.E.; Rodríguez-Leguizamón, G.; Rondón-Lagos, M. Analyzing Biological and Molecular Characteristics and Genomic Damage Induced by Exposure to Asbestos. Cancer Manag. Res. 2019, 11, 4997–5012. [Google Scholar] [CrossRef]
- Wolff, H.; Vehmas, T.; Oksa, P.; Rantanen, J.; Vainio, H. Asbestos, Asbestosis, and Cancer, the Helsinki Criteria for Diagnosis and Attribution 2014: Recommendations. Scand. J. Work Environ. Health 2015, 41, 5–15. [Google Scholar] [CrossRef]
- Donovan, E.P.; Donovan, B.L.; McKinley, M.A.; Cowan, D.M.; Paustenbach, D.J. Evaluation of Take Home (Para-Occupational) Exposure to Asbestos and Disease: A Review of the Literature. Crit. Rev. Toxicol. 2012, 42, 703–731. [Google Scholar] [CrossRef] [PubMed]
- Bersimbaev, R.; Bulgakova, O.; Aripova, A.; Kussainova, A.; Ilderbayev, O. Role of MicroRNAs in Lung Carcinogenesis Induced by Asbestos. J. Pers. Med. 2021, 11, 97. [Google Scholar] [CrossRef] [PubMed]
- Klebe, S.; Leigh, J.; Henderson, D.W.; Nurminen, M. Asbestos, Smoking and Lung Cancer: An Update. Int. J. Environ. Res. Public Health 2020, 17, 258. [Google Scholar] [CrossRef]
- Markowitz, S.B.; Levin, S.M.; Miller, A.; Morabia, A. Asbestos, Asbestosis, Smoking, and Lung Cancer. New Findings from the North American Insulator Cohort. Am. J. Respir. Crit. Care Med. 2013, 188, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, S. Asbestos-Related Lung Cancer and Malignant Mesothelioma of the Pleura: Selected Current Issues. Semin. Respir. Crit. Care Med. 2015, 36, 334–346. [Google Scholar] [CrossRef]
- Upadhyay, D.; Kamp, D.W. Asbestos-Induced Pulmonary Toxicity: Role of DNA Damage and Apoptosis. Exp. Biol. Med. 2003, 228, 650–659. [Google Scholar] [CrossRef]
- Liu, G.; Cheresh, P.; Kamp, D.W. Molecular Basis of Asbestos-Induced Lung Disease. Annu. Rev. Pathol. Mech. Dis. 2013, 8, 161–187. [Google Scholar] [CrossRef]
- Santarelli, L.; Gaetani, S.; Monaco, F.; Bracci, M.; Valentino, M.; Amati, M.; Rubini, C.; Sabbatini, A.; Pasquini, E.; Zanotta, N.; et al. Four-MiRNA Signature to Identify Asbestos-Related Lung Malignancies. Cancer Epidemiol. Biomark. Prev. 2019, 28, 119–126. [Google Scholar] [CrossRef]
- Micolucci, L.; Akhtar, M.M.; Olivieri, F.; Rippo, M.R.; Procopio, A.D. Diagnostic Value of MicroRNAs in Asbestos Exposure and Malignant Mesothelioma: Systematic Review and Qualitative Meta-Analysis. Oncotarget 2016, 7, 58606–58637. [Google Scholar] [CrossRef]
- Mahmood, I.; Imadi, S.R.; Shazadi, K.; Gul, A.; Hakeem, K.R. Effects of Pesticides on Environment. In Plant, Soil and Microbes: Volume 1: Implications in Crop Science; Springer: Berlin/Heidelberg, Germany, 2016; pp. 253–269. [Google Scholar]
- Thakur, S.; Sarkar, B.; Dhiman, M.; Mantha, A.K. Organophosphate-Pesticides Induced Survival Mechanisms and APE1-Mediated Nrf2 Regulation in Non-Small-Cell Lung Cancer Cells. J. Biochem. Mol. Toxicol. 2021, 35, e22640. [Google Scholar] [CrossRef]
- Ecobichon, D.J. Pesticide Use in Developing Countries. Toxicology 2001, 160, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Bharate, S.B.; Prins, J.M.; George, K.M.; Thompson, C.M. Thionate versus Oxon: Comparison of Stability, Uptake, and Cell Toxicity of (14CH3O)2-Labeled Methyl Parathion and Methyl Paraoxon with SH-SY5Y Cells. J. Agric. Food Chem. 2010, 58, 8460–8466. [Google Scholar] [CrossRef] [PubMed]
- Paz-Trejo, C.; Gómez-Arroyo, S. Genotoxic Evaluation of Common Commercial Pesticides in Human Peripheral Blood Lymphocytes. Toxicol. Ind. Health 2017, 33, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Bonner, M.R.; Freeman, L.E.B.; Hoppin, J.A.; Koutros, S.; Sandler, D.P.; Lynch, C.F.; Hines, C.J.; Thomas, K.; Blair, A.; Alavanja, M.C. Occupational Exposure to Pesticides and the Incidence of Lung Cancer in the Agricultural Health Study. Environ. Health Perspect. 2017, 125, 544–551. [Google Scholar] [CrossRef]
- Kim, B.; Park, E.Y.; Kim, J.; Park, E.; Oh, J.-K.; Lim, M.K. Occupational Exposure to Pesticides and Lung Cancer Risk: A Propensity Score Analyses. Cancer Res. Treat. 2021, 54, 130–139. [Google Scholar] [CrossRef]
- Jones, R.R.; Barone-Adesi, F.; Koutros, S.; Lerro, C.C.; Blair, A.; Lubin, J.; Heltshe, S.L.; Hoppin, J.A.; Alavanja, M.C.R.; Freeman, L.E.B. Incidence of Solid Tumours among Pesticide Applicators Exposed to the Organophosphate Insecticide Diazinon in the Agricultural Health Study: An Updated Analysis. Occup. Environ. Med. 2015, 72, 496–503. [Google Scholar] [CrossRef]
- Pesatori, A.C.; Sontag, J.M.; Lubin, J.H.; Consonni, D.; Blair, A. Cohort Mortality and Nested Case-Control Study of Lung Cancer among Structural Pest Control Workers in Florida (United States). Cancer Causes Control 1994, 5, 310–318. [Google Scholar] [CrossRef]
- Boulanger, M.; Tual, S.; Lemarchand, C.; Guizard, A.-V.; Delafosse, P.; Marcotullio, E.; Pons, R.; Piel, C.; Pouchieu, C.; Baldi, I.; et al. Lung Cancer Risk and Occupational Exposures in Crop Farming: Results from the AGRIculture and CANcer (AGRICAN) Cohort. Occup. Environ. Med. 2018, 75, 776–785. [Google Scholar] [CrossRef]
- Bajgar, J. Organophosphates/Nerve Agent Poisoning: Mechanism of Action, Diagnosis, Prophylaxis, And Treatment. In Advances in Clinical Chemistry; Elsevier: Amsterdam, The Netherlands, 2004; Volume 38, pp. 151–216. [Google Scholar]
- Costa, L.G. Current Issues in Organophosphate Toxicology. Clin. Chim. Acta 2006, 366, 1–13. [Google Scholar] [CrossRef]
- Herrmann, J.M.; Riemer, J. Apoptosis Inducing Factor and Mitochondrial NADH Dehydrogenases: Redox-Controlled Gear Boxes to Switch between Mitochondrial Biogenesis and Cell Death. Biol. Chem. 2021, 402, 289–297. [Google Scholar] [CrossRef]
- Franco, R.; Sánchez-Olea, R.; Reyes-Reyes, E.M.; Panayiotidis, M.I. Environmental Toxicity, Oxidative Stress and Apoptosis: Ménage à Trois. Mutat. Res. 2009, 674, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.A.E.; Simons, C.C.J.M.; van den Brandt, P.A.; van Engeland, M.; Weijenberg, M.P. Lifestyle, Diet, and Colorectal Cancer Risk According to (Epi)Genetic Instability: Current Evidence and Future Directions of Molecular Pathological Epidemiology. Curr. Color. Cancer Rep. 2017, 13, 455–469. [Google Scholar] [CrossRef] [PubMed]
- Ogino, S.; Chan, A.T.; Fuchs, C.S.; Giovannucci, E. Molecular Pathological Epidemiology of Colorectal Neoplasia: An Emerging Transdisciplinary and Interdisciplinary Field. Gut 2011, 60, 397–411. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compounds | Experimental Model of the Study | Dose Range | Protein/Gene Level Regulation, Signaling Pathway Activation | Final Outcome | Reference |
|---|---|---|---|---|---|
| Nicotine derivatives (Nitrosamine compounds) | E-cigarette smoke-exposed Mice. Cultured human bronchial epithelial and urothelial cells. In vitro DNA damage-dependent repair synthesis assay. | Mice: (10 mg/mL, 3 h/d, 5 d/wk) for 12 wk | ↓ DNA-repair activity and repair proteins XPC/OGG1/2 in the lung. ↑ mutational susceptibility and tumorigenic transformation of cultured human bronchial epithelial cells | DNA damage, DNA methylation changes, and adduct formation. Increased the lung cancer risk. | [85] |
| E-cigarette JUUL pod flavors “(Fruit Medley, Virginia Tobacco, Cool Mint, Crème Brulee, Cool Cucumber, Mango, and Classic Menthol)” and similar pod flavors (Just Mango-Strawberry Coconut and Caffé Latte)”. | Lung epithelial cells (16-HBE, BEAS-2B) and monocytes (U937) exposed to various pod aerosols | In-vitro aerosol exposure system: “66 puffs during 22 min with a three-second puff duration at 1.6 L/min flow rate and an inter-puff interval of approximately 17 s.” | ↑ acellular ROS ↑ mitochondrial superoxide production in bronchial epithelial cells (16-HBE). ↑ inflammatory mediators, such as IL-8/PGE2 in lung epithelial cells (16-HBE, BEAS-2B) and monocytes (U937) | JUUL pod flavors, “Crème Brulee and Cool Cucumber”, caused epithelial barrier dysfunction in 16-HBE cells. DNA damage upon exposure in monocytes Increase oxidative stress, inflammation, epithelial barrier dysfunction, and DNA damage in lung cells. | [88] |
| Vaping E-cigarette components | Total RNA from nasal scrape biopsies was analyzed using the nCounter Human Immunology v2 Expression panel. | Active E-cigarette users/vapers who have been using E-cigarettes regularly for at least six months | The top five genes with changed expression in E-cigarette users were Zinc Finger and BTB Domain Containing 16 (ZBTB16), EGR1, Polymeric Immunoglobulin Receptor (PIGR), Prostaglandin-Endoperoxide Synthase 2 (PTGS2), and FK506 Binding Protein 5 (FKBP5). | ↓ Expression of immune-related Genes at the level of nasal mucosa. | [118] |
| Menthol or tobacco-flavored EC liquids or aerosols | Human adenocarcinoma alveolar basal epithelial cells (A549). Live cell imaging, Epithelial-to mesenchymal transition (EMT) biomarker analysis, and machine learning/image processing algorithms. | exposure to EC liquids and aerosols from a popular product for 3-8 days. | EMT is accompanied by the acquisition of a fibroblast-like morphology, loss of cell-to-cell junctions, internalization of E-cadherin, and increased motility. Upregulation of EMT markers. Plasma membrane to nuclear translocation of â-catenin | An EMT of lung cancer cells during exposure to EC products | [120] |
| Aerosolization of commercial Cannabidiol (CBD) vaping products | Click chemistry and a novel in vitro vaping product exposure system (VaPES). | A human bronchial epithelial cell line (16HBEs) was exposed to synthetic a-CBD or a-CBDQ (Quinone) for 4 h at a range of concent. (2−35 μM). | A reactive CBD quinone (CBDQ) forms adducts with cysteine residues in human bronchial epithelial cell proteins, including “Keap1” and activates “KEAP1-Nrf2” stress response pathway genes. | Vaping CBD alters protein function and induces cellular stress pathways in the lung. | [128] |
| 49 commercially available e-liquid flavors | Free radicals generated from the flavors were captured/analyzed by electron paramagnetic resonance (EPR). The flavorant composition of each e-liquid was analyzed by gas chromatography mass spectroscopy (GCMS). | The flow meter of the E-cigarette setup was connected to the house vacuum and adjusted to a flow rate of 500 mL/min. | Nearly half of the flavors modulated free radical generation. Ethyl vanillin inhibited the radical formation in a concentration dependent manner. Free radical production was closely linked with the capacity to oxidize biologically relevant lipids. | Flavoring agents could enhance/inhibit the free radicals’ production in flavored E-cigarette aerosols. Some flavorants ↑ lipid peroxidation products. Some flavorants ↑ formation of 8-isoprostane (the oxidation products of arachidonic acid). | [140] |
| Ethyl maltol (EM; sweet flavor) | The Calu-6 and A549 lung epithelial cell lines co-exposed to EM and copper (Cu) | EM at 3 mM concentration as it was not toxic. | Cell viability DNA damage response Reactive oxygen species generation Ferritin light chain and heme oxygenase 1 mRNA upregulation | Co-exposure to EM and Cu at concentrations not toxic for either chemical individually induces oxidative stress, apoptosis, and DNA damage in lung epithelial cells. | [141] |
| Aldehydes | Different organs of mice exposed to mainstream tobacco smoke (MTS). Immortalized human bronchial epithelial cells BEAS-2B and urothelial cells UROtsa. Buccal cells and sputum. Lung tissues of tobacco smokers obtained from the marginal non-cancerous lung tissue samples of cancer patients. | Exposure of mice to MTS (75 mg/m3) for 6 h/d, 5 d/wk for 12 wk. | DNA Damage markers DNA Repair proteins determination. PdG adducts formation in human bronchial epithelial and urothelial cells | DNA damage DNA adducts formation and impairment of DNA repair proteins and activity. | [142] |
| Vitamin E acetate (VEA) | Human bronchial epithelial cells (BEAS-2B). | VEA vaping emissions were generated using a 0.46 L min-1 critical orifice to restrict the flow rate. Emissions were vaped into a glass cold trap submerged in dry ice; condensed emissions were dissolved in acetonitrile (ACN) for chemical analysis and cell culture media for cell exposure analysis. HMOX-1 and NQO1 gene expression analysis after 0, 3, 6, 12, and 24 h exposure to VEA vaping emissions. | Exposure to vaping emissions resulted in significant upregulation of NQO1 and HMOX-1 genes in BEAS-2B cells. | Oxidative damage Acute lung injury Synergistic interactions between thermal decomposition products of VEA could be evident, highlighting “the multifaceted nature of vaping toxicity”. | [143] |
| CBD/counterfeit vape cartridges and their constituents vitamin E acetate (VEA) and medium-chain triglycerides (MCT). | Bronchial epithelial cells (BEAS-2B). In Vivo Mouse Exposures with mouse arterial oxygen saturation and bronchoalveolar lavage (BALF) collection. | For in vitro exposures, cell culture plates were exposed to two 70 mL puffs of the aerosol under air-liquid interface conditions for 10 min. For in vivo exposures, wild-type mice with C57BL/6 background were exposed to 1 h MCT, VEA, and cartridge aerosols with 70 mL puffs, two puffs/min using the Scireq inExpose system | ↑ IL-6, eotaxin, and G-CSF in BALF. ↑ Eicosanoid inflammatory mediators and leukotrienes in mouse BALF. ↑ hydroxyeicosatetraenoic acid (HETEs) and various eicosanoid levels in plasma from E-cig users. ↑ Surfactant-associated protein-A (SP-A) in lung homogenates from male mice exposed to VEA. | Acute exposure to specific vape cartridges induces in vitro cytotoxicity, barrier dysfunction, and inflammation. In vivo, mouse exposure induces acute inflammation with elevated proinflammatory markers. Prolonged exposure may cause significant lung damage, which is involved in the pathogenesis of E-cigarette or vaping products-associated lung injury (EVALI). | [144] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shehata, S.A.; Toraih, E.A.; Ismail, E.A.; Hagras, A.M.; Elmorsy, E.; Fawzy, M.S. Vaping, Environmental Toxicants Exposure, and Lung Cancer Risk. Cancers 2023, 15, 4525. https://doi.org/10.3390/cancers15184525
Shehata SA, Toraih EA, Ismail EA, Hagras AM, Elmorsy E, Fawzy MS. Vaping, Environmental Toxicants Exposure, and Lung Cancer Risk. Cancers. 2023; 15(18):4525. https://doi.org/10.3390/cancers15184525
Chicago/Turabian StyleShehata, Shaimaa A., Eman A. Toraih, Ezzat A. Ismail, Abeer M. Hagras, Ekramy Elmorsy, and Manal S. Fawzy. 2023. "Vaping, Environmental Toxicants Exposure, and Lung Cancer Risk" Cancers 15, no. 18: 4525. https://doi.org/10.3390/cancers15184525
APA StyleShehata, S. A., Toraih, E. A., Ismail, E. A., Hagras, A. M., Elmorsy, E., & Fawzy, M. S. (2023). Vaping, Environmental Toxicants Exposure, and Lung Cancer Risk. Cancers, 15(18), 4525. https://doi.org/10.3390/cancers15184525