
Dosimetry of a Novel 111Indium-Labeled Anti-P-Cadherin Monoclonal Antibody (FF-21101) in Non-Human Primates
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Radiolabeling Preparation of FF-21101(111In)
2.2. Determination of Specific Activity
2.3. Experimental Animals
2.4. Gamma Camera and SPECT System
2.5. Gamma Camera and SPECT Imaging Protocol
2.6. CT Imaging
2.7. Image Analysis for Dosimetry Calculations
2.8. Blood Sampling
2.9. Residence Time and Absorbed Dose Calculations
3. Results
3.1. FF-21101(111In) Synthesis
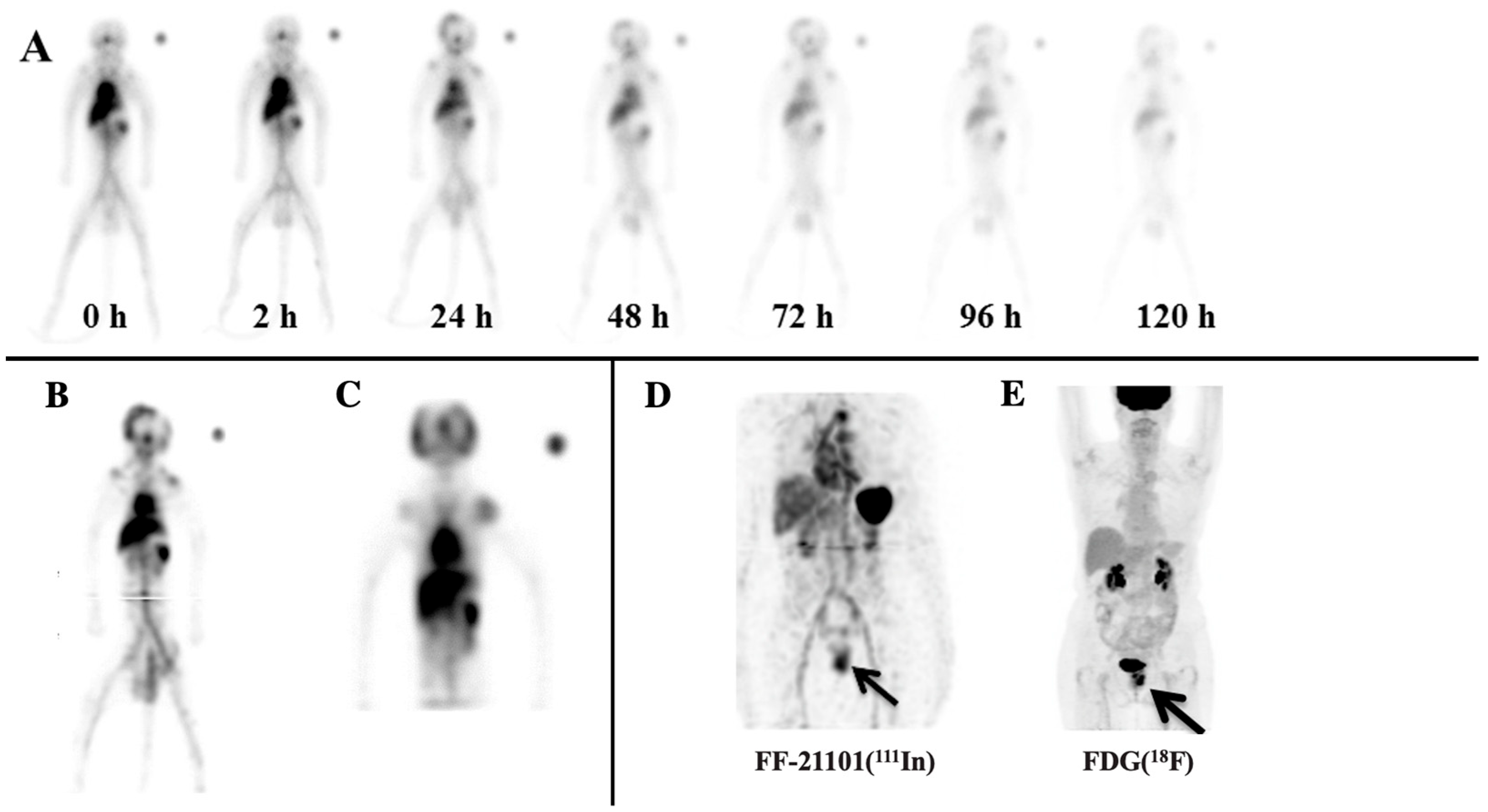
3.2. Planar/SPECT Imaging of FF-21101(111In)
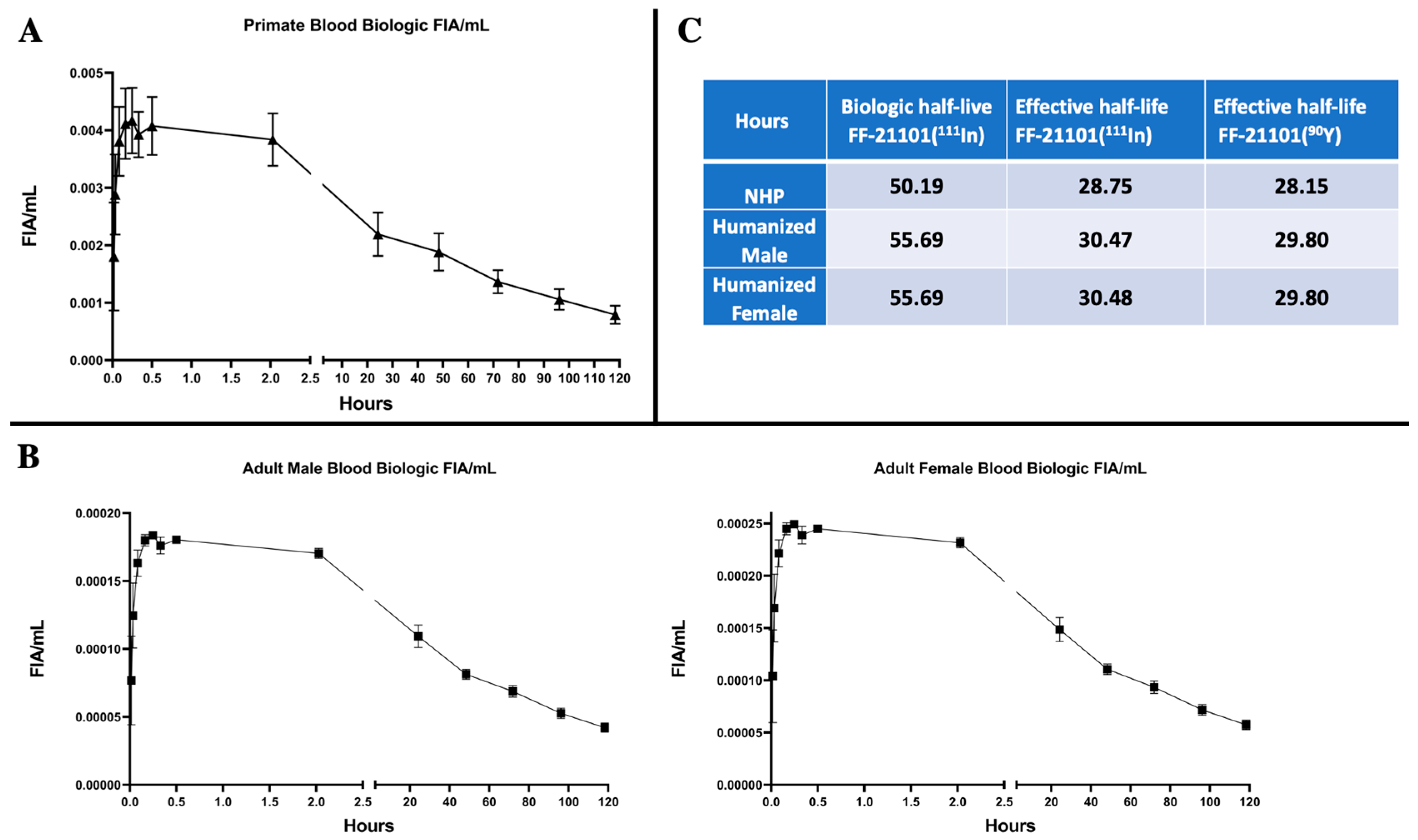
3.3. Pharmacokinetics of FF-21101(111In)
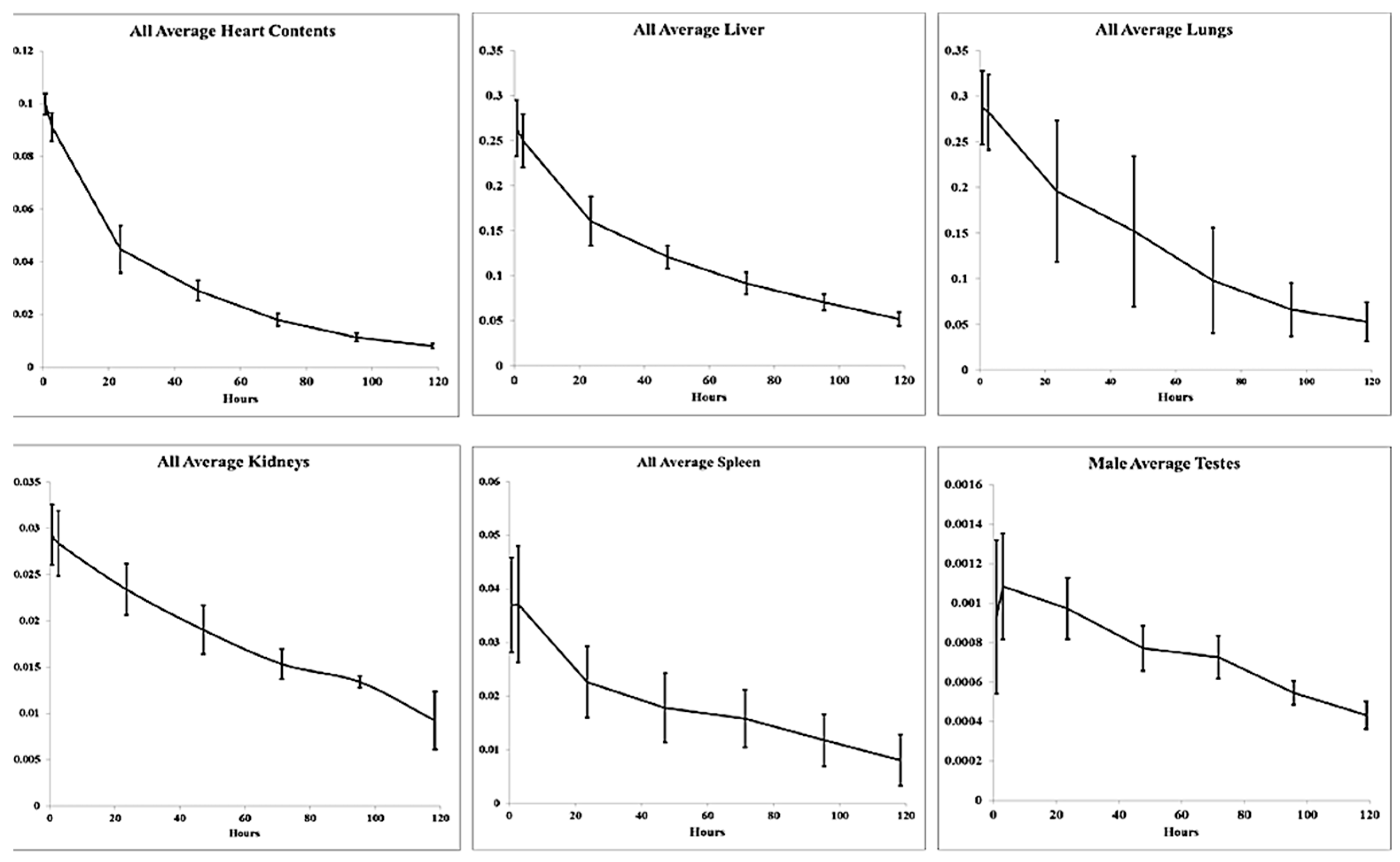
3.4. Radiation Dosimetry
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Conacci-Sorrell, M.E.; Ben-Yedidia, T. Nr-CAM is a target gene of the beta-catenin/LEF-1 pathway in melanoma and colon cancer and its expression enhances motility and confers tumorigenesis. Genes Dev. 2002, 16, 2058–2072. [Google Scholar] [CrossRef] [PubMed]
- Takeichi, M. The cadherins: Cell-cell adhesion molecules controlling animal morphogenesis. Development 1988, 102, 639–655. [Google Scholar] [CrossRef] [PubMed]
- Shimoyama, Y.; Hirohashi, S. Cadherin cell-adhesion molecules in human epithelial tissues and carcinomas. Cancer Res. 1989, 49, 2128–2133. [Google Scholar] [PubMed]
- Gamallo, C.; Moreno-Bueno, G. The prognostic significance of P-cadherin in infiltrating ductal breast carcinoma. Mod. Pathol. 2001, 14, 650–654. [Google Scholar] [CrossRef]
- Stefansson, I.M.; Salvesen, H.B. Prognostic impact of alterations in P-cadherin expression and related cell adhesion markers in endometrial cancer. J. Clin. Oncol. 2004, 22, 1242–1252. [Google Scholar] [CrossRef]
- Zhang, C.C.; Yan, Z. PF-03732010: A fully human monoclonal antibody against P-cadherin with antitumor and antimetastatic activity. Clin. Cancer Res. 2010, 16, 5177–5188. [Google Scholar] [CrossRef]
- A Study of PF-03732010 in Patients with Advanced Solid Tumors. ClinicalTrials.gov ID NCT00557505. Available online: https://clinicaltrials.gov/study/NCT00557505?tab=results (accessed on 21 June 2023).
- Strosberg, J.; Krenning, E. 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 1391–1392. [Google Scholar] [CrossRef]
- Hofman, M.S.; Violet, J. [(177)Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): A single-centre, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 825–833. [Google Scholar] [CrossRef]
- Emmanouilides, C.; Witzig, T.E. Safety and efficacy of yttrium-90 ibritumomab tiuxetan in older patients with non-Hodgkin’s lymphoma. Cancer Biother. Radiopharm. 2007, 22, 684–691. [Google Scholar] [CrossRef]
- Oriuchi, N.; Higuchi, T. Current status of cancer therapy with radiolabeled monoclonal antibody. Ann. Nucl. Med. 2005, 19, 355–365. [Google Scholar] [CrossRef]
- Basch, E. Toward patient-centered drug development in oncology. N. Engl. J. Med. 2013, 369, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Stokke, C.; Gabina, P.M. Dosimetry-based treatment planning for molecular radiotherapy: A summary of the 2017 report from the Internal Dosimetry Task Force. EJNMMI Phys. 2017, 4, 27. [Google Scholar] [CrossRef] [PubMed]
- Vilgrain, V.; Pereira, H. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): An open-label randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1624–1636. [Google Scholar] [CrossRef] [PubMed]
- Bastiaannet, R.; van Roekel, C. First Evidence for a Dose-Response Relationship in Patients Treated with (166)Ho Radioembolization: A Prospective Study. J. Nucl. Med. 2020, 61, 608–612. [Google Scholar] [CrossRef]
- Heppeler, A.; Froidevaux, S. Radiometal-labelled macrocyclic chelator-derivatized somatostatin analogue with superb tumour-targeting properties and potential for receptor mediated internal radiotherapymediated. Chem. Eur. J. 1999, 5, 1974–1981. [Google Scholar] [CrossRef]
- O’Donoghue, J.A.; Bardies, M. Relationships between tumor size and curability for uniformly targeted therapy with beta-emitting radionuclides. J. Nucl. Med. 1995, 36, 1902–1909. [Google Scholar]
- Fisher, D.R.; Shen, S. MIRD dose estimate report No. 20: Radiation absorbed-dose estimates for 111In- and 90Y-ibritumomab tiuxetan. J. Nucl. Med. 2009, 50, 644–652. [Google Scholar] [CrossRef]
- Lehnert, M.; Ludwig, H. Update on the rational use of Y-ibritumomab tiuxetan in the treatment of follicular lymphoma. Onco. Targets Ther. 2009, 2, 199–208. [Google Scholar]
- Howell, R.W.; Rao, D.V. Macroscopic dosimetry for radioimmunotherapy: Nonuniform activity distributions in solid tumors. Med. Phys. 1989, 16, 66–74. [Google Scholar] [CrossRef]
- Murthy, R.; Kamat, P. Radioembolization of yttrium-90 microspheres for hepatic malignancy. Semin. Interv. Radiol. 2008, 25, 48–57. [Google Scholar] [CrossRef]
- Camera, L.; Kinuya, S. Comparative biodistribution of indium- and yttrium-labeled B3 monoclonal antibody conjugated to either 2-(p-SCN-Bz)-6-methyl-DTPA (1B4M-DTPA) or 2-(p-SCN-Bz)-1,4,7,10-tetraazacyclododecane tetraacetic acid (2B-DOTA). Eur. J. Nucl. Med. 1994, 21, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.L.; Zhang, J. Theranostic Imaging of Yttrium-90. Biomed. Res. Int. 2015, 2015, 481279. [Google Scholar] [CrossRef] [PubMed]
- Naruki, Y.; Carrasquillo, J.A. Differential cellular catabolism of 111In, 90Y and 125I radiolabeled T101 anti-CD5 monoclonal antibody. Int. J. Rad. Appl. Instrum. B. 1990, 17, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Maecke, H.R.; Riesen, A. The molecular structure of indium-DTPA. J. Nucl. Med. 1989, 30, 1235–1239. [Google Scholar]
- Adams, G.P.; Shaller, C.C. A single treatment of yttrium-90-labeled CHX-A″-C6.5 diabody inhibits the growth of established human tumor xenografts in immunodeficient mice. Cancer Res. 2004, 64, 6200–6206. [Google Scholar] [CrossRef]
- Emami, B.; Lyman, J. Tolerance of normal tissue to therapeutic irradiation. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 109–122. [Google Scholar] [CrossRef]
- Rubin, P.; Casarett, G.W. Clinical radiation pathology as applied to curative radiotherapy. Cancer 1968, 22, 767–778. [Google Scholar] [CrossRef]
- Hope, T.A.; Abbott, A. NANETS/SNMMI Procedure Standard for Somatostatin Receptor-Based Peptide Receptor Radionuclide Therapy with (177)Lu-DOTATATE. J. Nucl. Med. 2019, 60, 937–943. [Google Scholar] [CrossRef]
- Tiuxetan, I. ZEVALINTM. 2001, USA/Package Insert/ZEVALIN. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2002/ibriide021902lb.pdf (accessed on 27 April 2023).
- FDA. First radiopharmaceutical for non-Hodgkin’s lymphoma. FDA Consum. 2002, 36, 3. Available online: https://permanent.access.gpo.gov/lps1609/www.fda.gov/fdac/departs/2002/302_upd.html#lymphoma (accessed on 26 April 2023).
- Sgouros, G.; Dewaraja, Y.K. Tumor Response to Radiopharmaceutical Therapies: The Knowns and the Unknowns. J. Nucl. Med. 2021, 62 (Suppl. S3), 12S–22S. [Google Scholar]
- Subbiah, V.; Erwin, W. Phase I Study of P-cadherin-targeted Radioimmunotherapy with (90)Y-FF-21101 Monoclonal Antibody in Solid Tumors. Clin. Cancer Res. 2020, 26, 5830–5842. [Google Scholar] [CrossRef] [PubMed]
- Kranz, M.; Sattler, B. Radiation dosimetry of the alpha(4)beta(2) nicotinic receptor ligand (+)-[(18)F]flubatine, comparing preclinical PET/MRI and PET/CT to first-in-human PET/CT results. EJNMMI Phys. 2016, 3, 25. [Google Scholar] [CrossRef] [PubMed]
- Garrow, A.A.; Andrews, J.P.M. Preclinical dosimetry models and the prediction of clinical doses of novel positron emission tomography radiotracers. Sci. Rep. 2020, 10, 15985. [Google Scholar] [CrossRef]
- Doss, M.; Kolb, H.C. Biodistribution and radiation dosimetry of the integrin marker 18F-RGD-K5 determined from whole-body PET/CT in monkeys and humans. J. Nucl. Med. 2012, 53, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Lobo, E.D.; Hansen, R.J. Antibody pharmacokinetics and pharmacodynamics. J. Pharm. Sci. 2004, 93, 2645–2668. [Google Scholar] [CrossRef]
- Malik, P.; Phipps, C. Pharmacokinetic Considerations for Antibody-Drug Conjugates against Cancer. Pharm. Res. 2017, 34, 2579–2595. [Google Scholar] [CrossRef]
- Sgouros, G. Bone marrow dosimetry for radioimmunotherapy: Theoretical considerations. J. Nucl Med. 1993, 34, 689–694. [Google Scholar]
- Macey, D.J.; Williams, L.E. AAPM Report No 71, A Primer for Radioimmunotherapy and Radionuclide Therapy; Medical Physics Publishing: Madison, WI, USA, 2001. [Google Scholar]
- ICoR Protection. Basic Anatomical and Physiological Data for Use in Radiological Protection: Reference Values; ICRP Report No. 89; ICRP Publication: Pergamon, Turkey; Oxford, UK; New York, NY, USA, 2001. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| FF-21101(111In) Residence Time (h) | 111In-Ibritumomab Tiuxetan Human | |||||||
|---|---|---|---|---|---|---|---|---|
| Source Organ | Overall | Females | Males | Published: [18] | ||||
| Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | |
| Heart Contents | 3.845 | 0.302 | 3.828 | 0.342 | 3.857 | 0.351 | 1.18 | 0.557 |
| Kidneys | 3.412 | 0.566 | 3.556 | 1.095 | 3.316 | 0.082 | 1.4 | 0.351 |
| Liver | 16.414 | 2.194 | 15.914 | 0.529 | 16.747 | 3.012 | 12.9 | 4.92 |
| Lungs | 15.407 | 2.792 | 13.53 | 1.471 | 16.658 | 2.938 | 1.41 | 0.904 |
| Spleen | 3.101 | 0.89 | 2.256 | 0.19 | 3.664 | 0.613 | 1.63 | 0.814 |
| Red Marrow | 3.085 | 0.837 | 3.995 | 0.103 | 2.477 | 0.114 | 11.7 | 4.52 |
| Testes | 0.151 | 0.019 | NA | NA | 0.151 | 0.019 | 0.163 | 0.065 |
| Total Body | 84.828 | 2.905 | 82.191 | 2.627 | 86.585 | 1.357 | 82.183 | 2.062 |
| Remainder of Body | 39.473 | 5.467 | 39.112 | 3.109 | 39.714 | 7.398 | 51.8 | 16.2 |
| FF-21101(90Y) Residence Time (h) | ||||||
|---|---|---|---|---|---|---|
| Source Organ | Overall | Females | Males | |||
| Mean | Std Dev | Mean | Std Dev | Mean | Std Dev | |
| Heart Contents | 3.768 | 0.293 | 3.654 | 0.286 | 3.781 | 0.340 |
| Kidneys | 3.209 | 0.494 | 3.319 | 0.678 | 3.128 | 0.069 |
| Liver | 15.874 | 2.109 | 16.518 | 2.036 | 16.219 | 2.890 |
| Lungs | 14.98 | 2.686 | 18.603 | 9.426 | 16.171 | 2.839 |
| Spleen | 2.972 | 0.838 | 1.843 | 0.573 | 3.510 | 0.550 |
| Red Marrow | 3.028 | 0.818 | 4.300 | 0.665 | 2.434 | 0.110 |
| Testes | 0.142 | 0.018 | NA | NA | 0.142 | 0.018 |
| Total Body | 81.253 | 2.689 | 80.591 | 3.533 | 82.885 | 1.247 |
| Remainder of Body | 37.339 | 5.237 | 32.354 | 8.500 | 37.499 | 7.071 |
| 111In-Ibritumomab Tiexetan Human | ||||||||
|---|---|---|---|---|---|---|---|---|
| Female | Male | Published [18] | ||||||
| Average | Std Dev | Average | Std Dev | Average | Std Dev | Average | Std Dev | |
| Organ | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq |
| Adrenals | 0.310 | 0.028 | 0.251 | 0.011 | 0.281 | 0.037 | 0.202 | 0.041 |
| Brain | 0.067 | 0.013 | 0.059 | 0.010 | 0.063 | 0.011 | 0.082 | 0.020 |
| Breasts | 0.136 | 0.018 | 0.113 | 0.003 | 0.124 | 0.017 | 0.080 | 0.016 |
| Gallbladder Wall | 0.317 | 0.019 | 0.268 | 0.020 | 0.293 | 0.032 | 0.229 | 0.059 |
| LLI Wall | 0.105 | 0.018 | 0.090 | 0.013 | 0.098 | 0.017 | 0.130 | 0.027 |
| Small Intestine | 0.130 | 0.014 | 0.118 | 0.010 | 0.124 | 0.013 | 0.145 | 0.027 |
| Stomach Wall | 0.189 | 0.004 | 0.164 | 0.005 | 0.176 | 0.014 | 0.139 | 0.028 |
| ULI Wall | 0.152 | 0.014 | 0.128 | 0.008 | 0.140 | 0.016 | 0.147 | 0.027 |
| Heart Wall | 0.498 | 0.046 | 0.403 | 0.025 | 0.451 | 0.061 | 0.195 | 0.048 |
| Kidneys | 0.671 | 0.114 | 0.586 | 0.008 | 0.629 | 0.086 | 0.315 | 0.071 |
| Liver | 0.851 | 0.112 | 0.650 | 0.100 | 0.751 | 0.145 | 0.467 | 0.202 |
| Lungs | 0.999 | 0.445 | 0.681 | 0.101 | 0.840 | 0.337 | 0.152 | 0.036 |
| Muscle | 0.124 | 0.004 | 0.104 | 0.005 | 0.114 | 0.012 | 0.103 | 0.021 |
| Ovaries | 0.112 | 0.018 | NA | NA | 0.112 | 0.018 | 0.138 | 0.028 |
| Pancreas | 0.290 | 0.009 | 0.257 | 0.012 | 0.274 | 0.020 | 0.199 | 0.041 |
| Red Marrow | 0.181 | 0.012 | 0.145 | 0.005 | 0.163 | 0.022 | 0.272 | 0.065 |
| Osteogenic Cells | 0.276 | 0.012 | 0.218 | 0.019 | 0.247 | 0.035 | 0.312 | 0.050 |
| Skin | 0.068 | 0.005 | 0.060 | 0.005 | 0.064 | 0.006 | 0.065 | 0.015 |
| Spleen | 0.675 | 0.150 | 0.958 | 0.140 | 0.816 | 0.202 | 0.464 | 0.193 |
| Thymus | 0.197 | 0.022 | 0.167 | 0.012 | 0.182 | 0.023 | 0.114 | 0.024 |
| Thyroid | 0.095 | 0.003 | 0.141 | 0.038 | 0.118 | 0.035 | 0.098 | 0.024 |
| Urinary Bladder Wall | 0.089 | 0.018 | 0.087 | 0.010 | 0.088 | 0.013 | 0.113 | 0.028 |
| Uterus | 0.107 | 0.019 | NA | NA | 0.107 | 0.019 | 0.132 | 0.029 |
| Testes | NA | NA | 0.114 | 0.044 | 0.114 | 0.044 | 0.175 | 0.076 |
| Total Body | 0.162 | 0.009 | 0.133 | 0.002 | 0.148 | 0.017 | 0.124 | 0.022 |
| Effective Dose Eq | 0.382 | 0.054 | 0.339 | 0.023 | 0.360 | 0.044 | ||
| Effective Dose | 0.279 | 0.050 | 0.241 | 0.015 | 0.260 | 0.039 | ||
| 90Y-Ibritumomab Tiuxetan Human | ||||||||
|---|---|---|---|---|---|---|---|---|
| Female | Male | Published [18] | ||||||
| Average | Std Dev | Average | Std Dev | Average | Std Dev | Average | Std Dev | |
| Organ | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq | mSv/MBq |
| Adrenals | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Brain | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Breasts | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Gallbladder Wall | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| LLI Wall | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Small Intestine | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Stomach Wall | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| ULI Wall | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Heart Wall | 2.707 | 0.231 | 2.513 | 0.190 | 2.610 | 0.217 | 1.080 | 0.394 |
| Kidneys | 6.333 | 1.296 | 5.497 | 0.119 | 5.915 | 0.942 | 2.440 | 0.610 |
| Liver | 6.353 | 0.785 | 4.573 | 0.817 | 5.463 | 1.210 | 3.640 | 1.389 |
| Lungs | 12.277 | 6.206 | 8.710 | 1.528 | 10.493 | 4.489 | 0.761 | 0.488 |
| Muscle | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Ovaries | 0.306 | 0.081 | NA | NA | 0.306 | 0.081 | 0.379 | 0.118 |
| Pancreas | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Red Marrow | 1.008 | 0.071 | 0.705 | 0.053 | 0.857 | 0.175 | 2.730 | 0.909 |
| Osteogenic Cells | 1.283 | 0.023 | 0.742 | 0.087 | 1.013 | 0.302 | 2.140 | 0.519 |
| Skin | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Spleen | 6.41 | 1.989 | 10.010 | 1.552 | 8.210 | 2.536 | 4.650 | 2.327 |
| Thymus | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Thyroid | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Urinary Bladder Wall | 0.306 | 0.081 | 0.274 | 0.052 | 0.290 | 0.063 | 0.379 | 0.118 |
| Uterus | 0.306 | 0.081 | NA | NA | 0.306 | 0.081 | 0.379 | 0.118 |
| Testes | NA | NA | 1.860 | 0.233 | 1.860 | 0.233 | 2.160 | 0.842 |
| Total Body | 0.738 | 0.035 | 0.588 | 0.010 | 0.663 | 0.086 | 0.587 | 0.107 |
| Organ | Human Average (mGy/mCi) * | Std Dev | Primate Average (mGy/mCi) ** | Std Dev | % Change |
|---|---|---|---|---|---|
| Spleen | 1031.5 | 399.9 | 303.77 | 93.83 | 70.55 |
| Testes | 339.5 | 122.6 | 68.82 | 8.62 | 79.73 |
| Kidneys | 219.7 | 75.8 | 218.86 | 34.85 | 0.38 |
| Lungs | 168.9 | 56.9 | 388.24 | 166.09 | 129.86 |
| Liver | 160.6 | 58.5 | 202.13 | 44.77 | 25.86 |
| Heart Wall | 89.7 | 18.1 | 96.57 | 8.03 | 7.66 |
| Osteogenic Cells | 34.7 | 13.2 | 37.48 | 11.17 | 8.01 |
| Red Marrow | 29.6 | 11 | 31.71 | 6.48 | 7.13 |
| Total Body | 25.7 | 2.6 | 24.53 | 3.18 | 4.55 |
| Ovaries | 14.6 | 4.3 | 11.32 | 3.00 | 22.45 |
| Uterus | 14.6 | 4.3 | 11.32 | 3.00 | 22.45 |
| All other organs | 12.5 | 5.1 | 10.73 | 2.33 | 14.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ravizzini, G.; Erwin, W.; De Palatis, L.; Martiniova, L.; Subbiah, V.; Paolillo, V.; Mitchell, J.; McCoy, A.P.; Gonzalez, J.; Mawlawi, O. Dosimetry of a Novel 111Indium-Labeled Anti-P-Cadherin Monoclonal Antibody (FF-21101) in Non-Human Primates. Cancers 2023, 15, 4532. https://doi.org/10.3390/cancers15184532
Ravizzini G, Erwin W, De Palatis L, Martiniova L, Subbiah V, Paolillo V, Mitchell J, McCoy AP, Gonzalez J, Mawlawi O. Dosimetry of a Novel 111Indium-Labeled Anti-P-Cadherin Monoclonal Antibody (FF-21101) in Non-Human Primates. Cancers. 2023; 15(18):4532. https://doi.org/10.3390/cancers15184532
Chicago/Turabian StyleRavizzini, Gregory, William Erwin, Louis De Palatis, Lucia Martiniova, Vivek Subbiah, Vincenzo Paolillo, Jennifer Mitchell, Asa P. McCoy, Jose Gonzalez, and Osama Mawlawi. 2023. "Dosimetry of a Novel 111Indium-Labeled Anti-P-Cadherin Monoclonal Antibody (FF-21101) in Non-Human Primates" Cancers 15, no. 18: 4532. https://doi.org/10.3390/cancers15184532
APA StyleRavizzini, G., Erwin, W., De Palatis, L., Martiniova, L., Subbiah, V., Paolillo, V., Mitchell, J., McCoy, A. P., Gonzalez, J., & Mawlawi, O. (2023). Dosimetry of a Novel 111Indium-Labeled Anti-P-Cadherin Monoclonal Antibody (FF-21101) in Non-Human Primates. Cancers, 15(18), 4532. https://doi.org/10.3390/cancers15184532