
Significance of 8-OHdG Expression as a Predictor of Survival in Colorectal Cancer

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population and Clinical Specimens
2.2. Definition of Clinicopathologic Factors
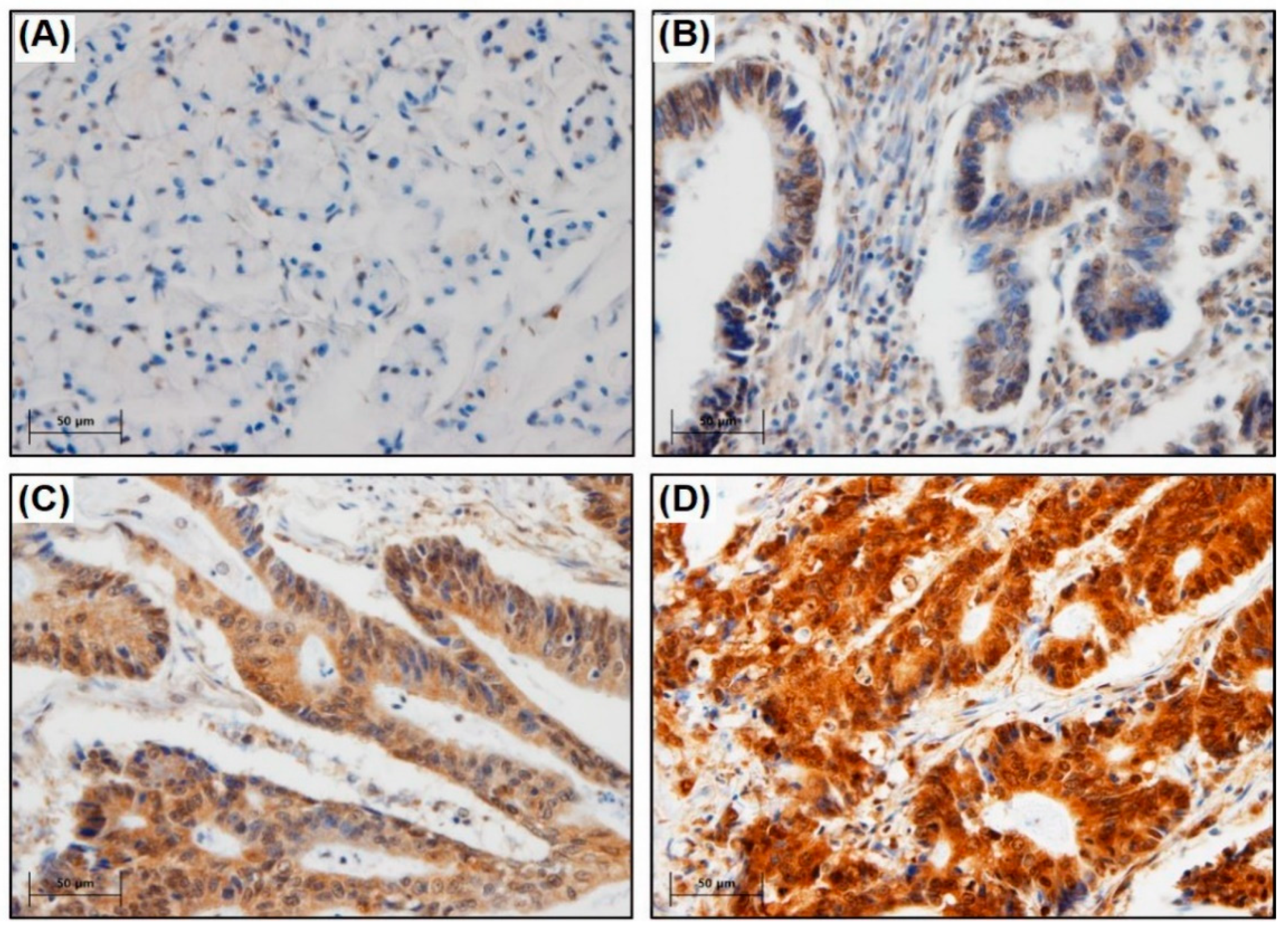
2.3. Tissue Microarray (TMA) and IHC
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
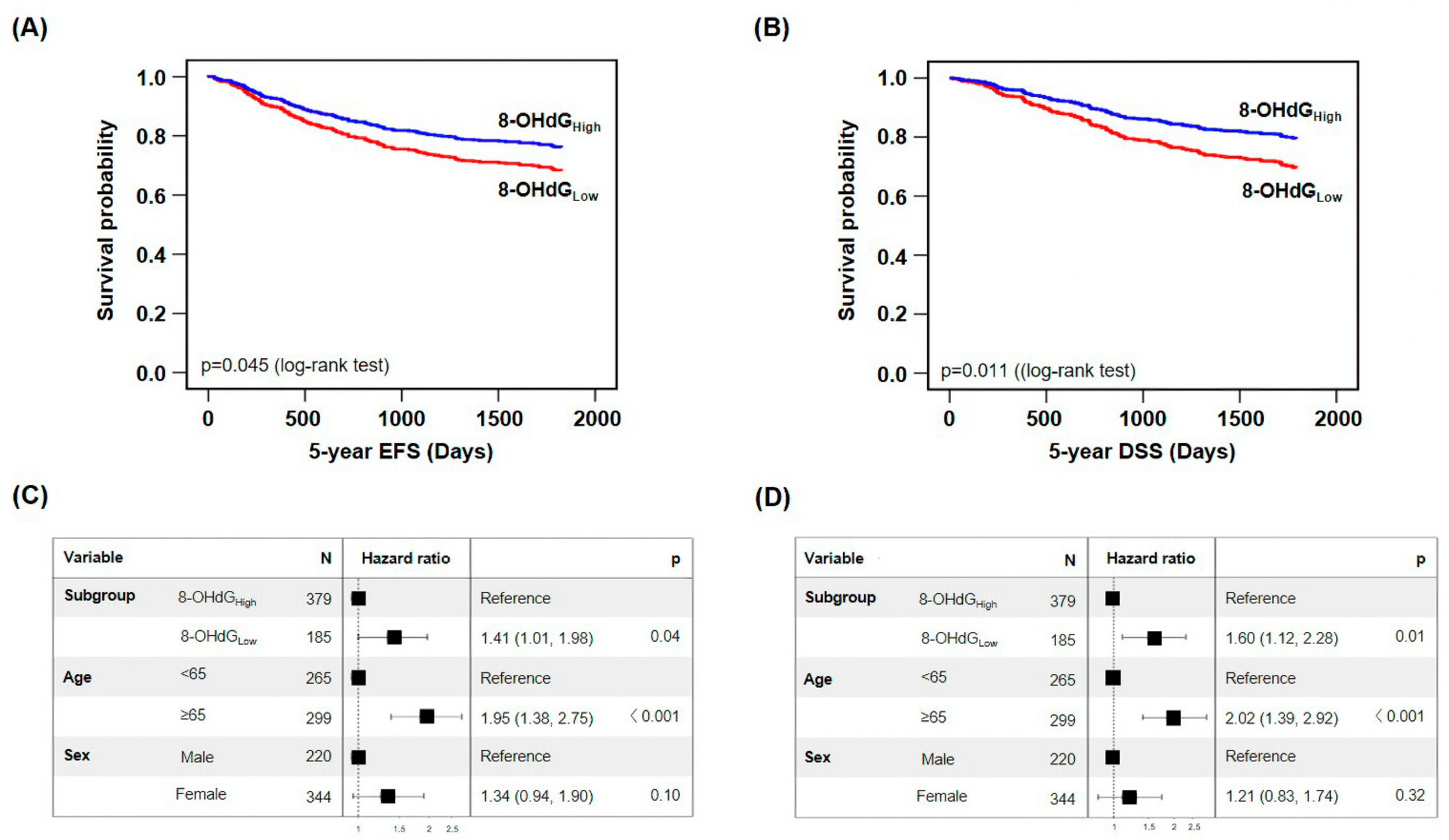
3.2. Low 8-OHdG Expression Is Related to Poor Prognosis
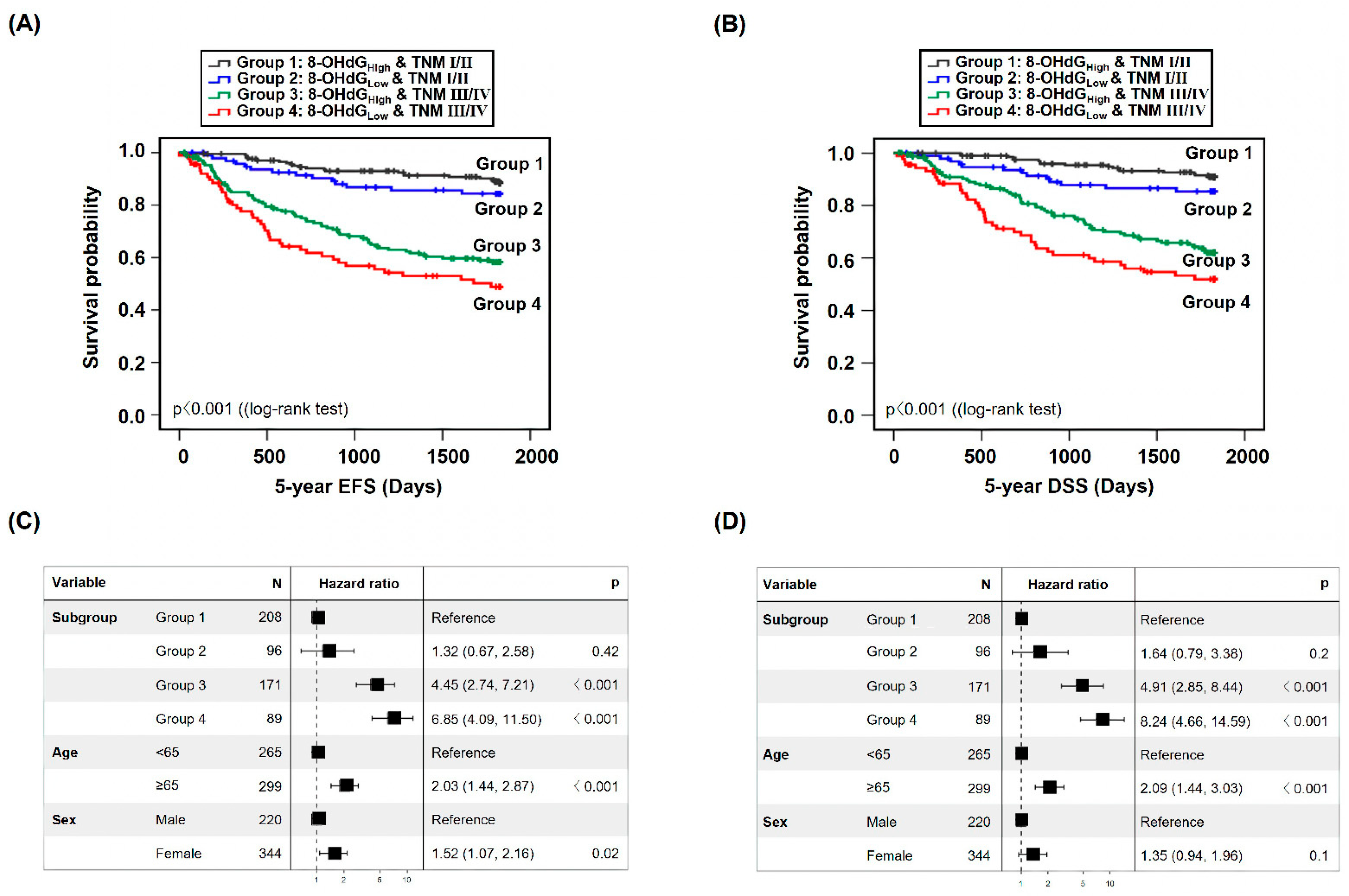
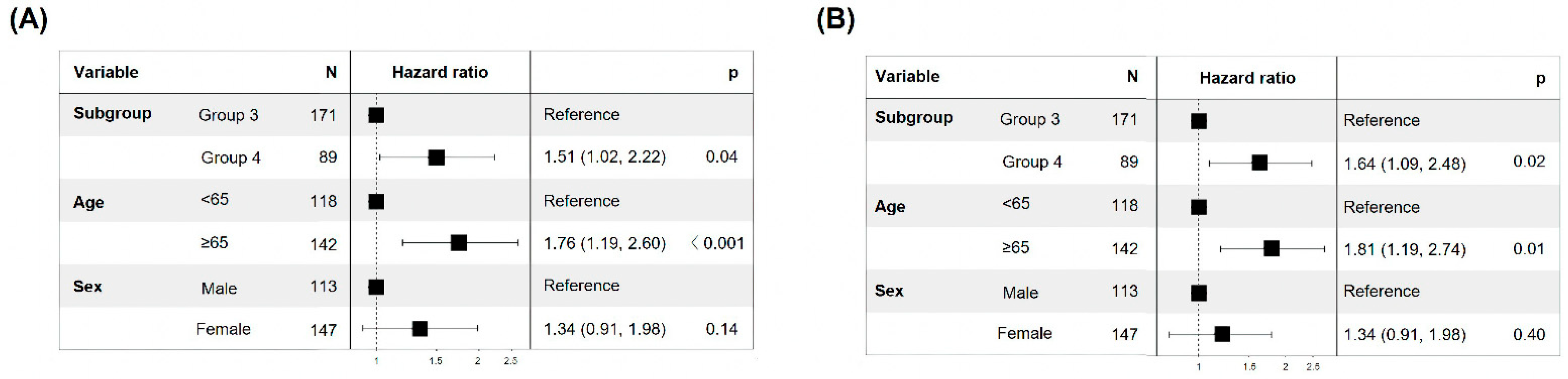
3.3. Low Expression of 8-OHdG at Advanced Stage Is Associated with Poor Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xi, Y.; Xu, P. Global colorectal cancer burden in 2020 and projections to 2040. Transl. Oncol. 2021, 14, 101174. [Google Scholar] [CrossRef] [PubMed]
- Lewandowska, A.; Rudzki, G.; Lewandowski, T.; Stryjkowska-Gora, A.; Rudzki, S. Risk Factors for the Diagnosis of Colorectal Cancer. Cancer Control 2022, 29, 10732748211056692. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.; Tuli, H.S.; Varol, A.; Thakral, F.; Yerer, M.B.; Sak, K.; Varol, M.; Jain, A.; Khan, M.A.; Sethi, G. Role of Reactive Oxygen Species in Cancer Progression: Molecular Mechanisms and Recent Advancements. Biomolecules 2019, 9, 735. [Google Scholar] [CrossRef] [PubMed]
- Tauffenberger, A.; Magistretti, P.J. Reactive Oxygen Species: Beyond Their Reactive Behavior. Neurochem. Res. 2021, 46, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Juan, C.A.; Perez De La Lastra, J.M.; Plou, F.J.; Perez-Lebena, E. The Chemistry of Reactive Oxygen Species (ROS) Revisited: Outlining Their Role in Biological Macromolecules (DNA, Lipids and Proteins) and Induced Pathologies. Int. J. Mol. Sci. 2021, 22, 4642. [Google Scholar] [CrossRef] [PubMed]
- Zorov, D.B.; Juhaszova, M.; Sollott, S.J. Mitochondrial reactive oxygen species (ROS) and ROS-induced ROS release. Physiol. Rev. 2014, 94, 909–950. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, Y.; Zhang, X.; Lu, Y.; Chen, H. New insights in intestinal oxidative stress damage and the health intervention effects of nutrients: A review. J. Funct. Foods 2020, 75, 104248. [Google Scholar] [CrossRef]
- Bardelcikova, A.; Soltys, J.; Mojzis, J. Oxidative Stress, Inflammation and Colorectal Cancer: An Overview. Antioxidants 2023, 12, 901. [Google Scholar] [CrossRef]
- Sullivan, L.B.; Chandel, N.S. Mitochondrial reactive oxygen species and cancer. Cancer Metab. 2014, 2, 17. [Google Scholar] [CrossRef]
- Fleming, A.M.; Burrows, C.J. On the irrelevancy of hydroxyl radical to DNA damage from oxidative stress and implications for epigenetics. Chem. Soc. Rev. 2020, 49, 6524–6528. [Google Scholar] [CrossRef]
- Hahm, J.Y.; Park, J.; Jang, E.S.; Chi, S.W. 8-Oxoguanine: From oxidative damage to epigenetic and epitranscriptional modification. Exp. Mol. Med. 2022, 54, 1626–1642. [Google Scholar] [CrossRef] [PubMed]
- Preston, T.J.; Henderson, J.T.; Mccallum, G.P.; Wells, P.G. Base excision repair of reactive oxygen species-initiated 7,8-dihydro-8-oxo-2′-deoxyguanosine inhibits the cytotoxicity of platinum anticancer drugs. Mol. Cancer Ther. 2009, 8, 2015–2026. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Wang, Y.; Guo, W.; Zhou, Y.; Lv, C.; Chen, X.; Liu, K. The significance of the alteration of 8-OHdG in serous ovarian carcinoma. J. Ovarian Res. 2013, 6, 74. [Google Scholar] [CrossRef]
- An, A.R.; Kim, K.M.; Park, H.S.; Jang, K.Y.; Moon, W.S.; Kang, M.J.; Lee, Y.C.; Kim, J.H.; Chae, H.J.; Chung, M.J. Association between Expression of 8-OHdG and Cigarette Smoking in Non-small Cell Lung Cancer. J. Pathol. Transl. Med. 2019, 53, 217–224. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Zhao, Y.; Wang, N.; Zhang, L.; Wang, C. 8-Hydroxy-2′-deoxyguanosine expression predicts outcome of esophageal cancer. Ann. Diagn. Pathol. 2014, 18, 326–328. [Google Scholar] [CrossRef]
- Lee, J.D.; Cai, Q.; Shu, X.O.; Nechuta, S.J. The role of biomarkers of oxidative stress in breast cancer risk and prognosis: A systematic review of the epidemiologic literature. J. Women’s Health 2017, 26, 467–482. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.; Srivastava, J.K.; Shankar, E.; Kanwal, R.; Nawab, A.; Sharma, H.; Bhaskaran, N.; Ponsky, L.E.; Fu, P.; Maclennan, G.T. Oxidative stress and antioxidant status in high-risk prostate cancer subjects. Diagnostics 2020, 10, 126. [Google Scholar] [CrossRef]
- Pylvas, M.; Puistola, U.; Laatio, L.; Kauppila, S.; Karihtala, P. Elevated serum 8-OHdG is associated with poor prognosis in epithelial ovarian cancer. Anticancer Res. 2011, 31, 1411–1415. [Google Scholar]
- Shen, J.; Deininger, P.; Hunt, J.D.; Zhao, H. 8-Hydroxy-2′-deoxyguanosine (8-OH-dG) as a potential survival biomarker in patients with nonsmall-cell lung cancer. Cancer 2007, 109, 574–580. [Google Scholar] [CrossRef]
- Sova, H.; Jukkola-Vuorinen, A.; Puistola, U.; Kauppila, S.; Karihtala, P. 8-Hydroxydeoxyguanosine: A new potential independent prognostic factor in breast cancer. Br. J. Cancer 2010, 102, 1018–1023. [Google Scholar] [CrossRef]
- Karihtala, P.; Kauppila, S.; Soini, Y.; Arja Jukkola, V. Oxidative stress and counteracting mechanisms in hormone receptor positive, triple-negative and basal-like breast carcinomas. BMC Cancer 2011, 11, 262. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Jeong, S.; An, J.; Park, S.; Nam, S.; Kwon, K.A.; Sahoo, D.; Ghosh, P.; Kim, J.H. Clinicopathologic Significance of Heat Shock Protein 60 as a Survival Predictor in Colorectal Cancer. Cancers 2023, 15, 4052. [Google Scholar] [CrossRef] [PubMed]
- Acevedo-Leon, D.; Monzo-Beltran, L.; Perez-Sanchez, L.; Naranjo-Morillo, E.; Gomez-Abril, S.A.; Estan-Capell, N.; Banuls, C.; Saez, G. Oxidative Stress and DNA Damage Markers in Colorectal Cancer. Int. J. Mol. Sci. 2022, 23, 11664. [Google Scholar] [CrossRef] [PubMed]
- Srinivas, U.S.; Tan, B.W.Q.; Vellayappan, B.A.; Jeyasekharan, A.D. ROS and the DNA damage response in cancer. Redox Biol. 2019, 25, 101084. [Google Scholar] [CrossRef] [PubMed]
- Someah, M.S.; Golbabaei, F.; Arjomandi, R.; Semiromi, F.B.; Mohammadi, A. Oxidative Stress and DNA Damages Induced by Occupational Exposure to Asbestos: A Systematic Review. Iran. J. Public Health 2023, 52, 1613–1625. [Google Scholar] [CrossRef]
- Klaunig, J.E. Oxidative Stress and Cancer. Curr. Pharm. Des. 2018, 24, 4771–4778. [Google Scholar] [CrossRef] [PubMed]
- Klaunig, J.E.; Kamendulis, L.M.; Hocevar, B.A. Oxidative stress and oxidative damage in carcinogenesis. Toxicol. Pathol. 2010, 38, 96–109. [Google Scholar] [CrossRef] [PubMed]
- Hernandez Borrero, L.J.; El-Deiry, W.S. Tumor suppressor p53: Biology, signaling pathways, and therapeutic targeting. Biochim. Biophys. Acta Rev. Cancer 2021, 1876, 188556. [Google Scholar] [CrossRef]
- Cordani, M.; Butera, G.; Pacchiana, R.; Masetto, F.; Mullappilly, N.; Riganti, C.; Donadelli, M. Mutant p53-Associated Molecular Mechanisms of ROS Regulation in Cancer Cells. Biomolecules 2020, 10, 361. [Google Scholar] [CrossRef]
- Link, T.; Iwakuma, T. Roles of p53 in extrinsic factor-induced liver carcinogenesis. Hepatoma Res. 2017, 3, 95–104. [Google Scholar] [CrossRef]
- Silwal-Pandit, L.; Langerod, A.; Borresen-Dale, A.L. TP53 Mutations in Breast and Ovarian Cancer. Cold Spring Harb. Perspect. Med. 2017, 7, a026252. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Han, C.Y.; Duan, F.G.; Fan, X.X.; Yao, X.J.; Parks, R.J.; Tang, Y.J.; Wang, M.F.; Liu, L.; Tsang, B.K.; et al. p53 sensitizes chemoresistant non-small cell lung cancer via elevation of reactive oxygen species and suppression of EGFR/PI3K/AKT signaling. Cancer Cell Int. 2019, 19, 188. [Google Scholar] [CrossRef] [PubMed]
- Yugawa, K.; Itoh, S.; Yoshizumi, T.; Yoshiya, S.; Takeishi, K.; Toshima, T.; Harada, N.; Ikegami, T.; Kohashi, K.; Oda, Y.; et al. Prognostic impact of 8-hydroxy-deoxyguanosine and its repair enzyme 8-hysroxy-deoxyguanosine DNA glycosylase in hepatocellular carcinoma. Pathol. Int. 2020, 70, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Murtas, D.; Piras, F.; Minerba, L.; Ugalde, J.; Floris, C.; Maxia, C.; Demurtas, P.; Perra, M.T.; Sirigu, P. Nuclear 8-hydroxy-2′-deoxyguanosine as survival biomarker in patients with cutaneous melanoma. Oncol. Rep. 2010, 23, 329–335. [Google Scholar] [PubMed]
- Kitagawa, H.; Kitajima, Y.; Kai, K.; Komukai, S.; Tanaka, T.; Koga, Y.; Manabe, T.; Noshiromicron, H. Predictive value of the ratio of 8-hydroxydeoxyguanosine levels between cancerous and normal tissues in patients with stage II/III colorectal cancer. Oncol. Rep. 2019, 41, 3041–3050. [Google Scholar] [CrossRef] [PubMed]
- Qing, X.; Shi, D.; Lv, X.; Wang, B.; Chen, S.; Shao, Z. Prognostic significance of 8-hydroxy-2′-deoxyguanosine in solid tumors: A meta-analysis. BMC Cancer 2019, 19, 997. [Google Scholar] [CrossRef] [PubMed]
- He, F.; Ru, X.; Wen, T. NRF2, a Transcription Factor for Stress Response and Beyond. Int. J. Mol. Sci. 2020, 21, 4777. [Google Scholar] [CrossRef]
- Cooke, M.S.; Evans, M.D.; Dizdaroglu, M.; Lunec, J. Oxidative DNA damage: Mechanisms, mutation, and disease. FASEB J. 2003, 17, 1195–1214. [Google Scholar] [CrossRef]
- Sakata, K.; Yoshizumi, T.; Izumi, T.; Shimokawa, M.; Itoh, S.; Ikegami, T.; Harada, N.; Toshima, T.; Mano, Y.; Mori, M. The role of DNA Repair Glycosylase OGG1 in Intrahepatic Cholangiocarcinoma. Anticancer Res. 2019, 39, 3241–3248. [Google Scholar] [CrossRef]
- Abuetabh, Y.; Wu, H.H.; Chai, C.; Al Yousef, H.; Persad, S.; Sergi, C.M.; Leng, R. DNA damage response revisited: The p53 family and its regulators provide endless cancer therapy opportunities. Exp. Mol. Med. 2022, 54, 1658–1669. [Google Scholar] [CrossRef]
- Hintsala, H.R.; Jokinen, E.; Haapasaari, K.M.; Moza, M.; Ristimaki, A.; Soini, Y.; Koivunen, J.; Karihtala, P. Nrf2/Keap1 Pathway and Expression of Oxidative Stress Lesions 8-hydroxy-2′-deoxyguanosine and Nitrotyrosine in Melanoma. Anticancer Res. 2016, 36, 1497–1506. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 564) | |
|---|---|
| Age | 64.3 ± 11.4 |
| Sex | |
| Male | 344 (61.0%) |
| Female | 220 (39.0%) |
| Laboratory findings | |
| Hemoglobin (g/dL) | 12.2 ± 2.4 |
| WBC (103/μL) | 7664.0 ± 3.0 |
| CEA (ng/mL) | 27.0 ± 303.1 |
| Pathology | |
| Size (mm) | 52.7 ± 23.2 |
| Location | |
| Cecum | 11 (2.0%) |
| Ascending colon | 91 (16.1%) |
| Hepatic flexure | 8 (1.4%) |
| Transverse colon | 37 (6.6%) |
| Splenic flexure | 4 (0.7%) |
| Descending colon | 18 (3.2%) |
| Sigmoid-descending | 5 (0.9%) |
| Sigmoid colon | 141 (25.0%) |
| Rectosigmoid colon | 104 (18.4%) |
| Rectum | 145 (25.7%) |
| Differentiation | |
| WD | 37 (6.6%) |
| MD | 476 (84.4%) |
| PD | 24 (4.3%) |
| Mucinous | 24 (4.3%) |
| SRC | 2 (0.4%) |
| TNM stage | |
| Ⅰ | 98 (17.4%) |
| Ⅱ | 206 (36.5%) |
| Ⅲ | 189 (33.5%) |
| Ⅳ | 71 (12.6%) |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Total (n = 564) | 8-OHdG (n = 185), Low | 8-OHdG (n = 379), High | p | OR (CI) | p | |
| Age (years) | 0.464 | 0.464 | ||||
| < 65 | 265 (47.0%) | 91 (49.2%) | 174 (45.9%) | 1 (Reference) | ||
| ≥65 | 299 (53.0%) | 94 (50.8%) | 205 (54.1%) | 1.414 (0.082–1.622) | ||
| Sex | 0.133 | 0.082 | ||||
| Male | 344 (61.0%) | 121 (65.4%) | 223 (58.8%) | 1 (Reference) | ||
| Female | 220 (39.0%) | 64 (34.6%) | 156 (41.2%) | 1.420 (0.956–2.109) | ||
| Diabetes mellitus | 0.672 | 0.553 | ||||
| No | 464 (82.3%) | 154 (83.2%) | 310 (81.8%) | 1 (Reference) | ||
| Yes | 100 (17.7%) | 31 (16.8%) | 69 (18.2%) | 1.159 (0.712–1.887) | ||
| Smoking | 0.666 | 0.877 | ||||
| No | 433 (76.8%) | 140 (75.7%) | 293 (77.3%) | 1 (Reference) | ||
| Yes | 131 (23.2%) | 45 (24.3%) | 86 (22.7%) | 0.965 (0.616–1.513) | ||
| Family history | 0.371 | 0.408 | ||||
| No | 543 (96.3%) | 180 (97.3%) | 363 (95.8%) | 1 (Reference) | ||
| Yes | 21 (3.7%) | 5 (2.7%) | 16 (4.2%) | 1.546 (0.551–4.341) | ||
| Anemia | 0.247 | 0.215 | ||||
| No | 291 (51.6%) | 89 (48.1%) | 202 (53.3%) | 1 (Reference) | ||
| Yes | 273 (48.4%) | 96 (51.9%) | 177 (46.7%) | 0.785 (0.535–1.273) | ||
| WBC counts | 0.232 | 0.316 | ||||
| Normal | 478 (84.8%) | 152 (82.2%) | 326 (86.0%) | 1 (Reference) | ||
| Abnormal | 86 (15.2%) | 33 (17.8%) | 53 (14.0%) | 0.777 (0.474–1.273) | ||
| Serum CEA | 0.237 | 0.379 | ||||
| Normal | 417 (73.9%) | 131 (70.8%) | 286 (75.5%) | 1 (Reference) | ||
| Abnormal | 147 (26.1%) | 54 (29.2%) | 93 (24.5%) | 0.828 (0.543–1.261) | ||
| Tumor location | 0.617 | 0.901 | ||||
| LCC | 416 (73.8%) | 134 (72.4%) | 282 (74.4%) | 1 (Reference) | ||
| RCC | 148 (26.2%) | 51 (27.6%) | 97 (25.6%) | 0.973 (0.636–1.490) | ||
| Tumor | 0.010 | 0.012 | ||||
| Differentiation | 513 (91.0%) | 160 (86.5%) | 353 (93.1%) | 1 (Reference) | ||
| Undifferentiation | 51 (9.0%) | 25 (13.5%) | 26 (6.9%) | 0.461 (0.252–0.844) | ||
| TNM stage | 0.504 | 0.985 | ||||
| Ⅰ/Ⅱ | 304 (53.9%) | 96 (51.9%) | 208 (54.9%) | 1 (Reference) | ||
| Ⅲ/Ⅳ | 260 (46.1%) | 89 (48.1%) | 171 (45.1%) | 0.973 (0.636–1.490) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.; Jeong, S.; Park, S.; Nam, S.; Chung, J.-W.; Kim, K.O.; An, J.; Kim, J.H. Significance of 8-OHdG Expression as a Predictor of Survival in Colorectal Cancer. Cancers 2023, 15, 4613. https://doi.org/10.3390/cancers15184613
Kang M, Jeong S, Park S, Nam S, Chung J-W, Kim KO, An J, Kim JH. Significance of 8-OHdG Expression as a Predictor of Survival in Colorectal Cancer. Cancers. 2023; 15(18):4613. https://doi.org/10.3390/cancers15184613
Chicago/Turabian StyleKang, Myunghee, Soyeon Jeong, Sungjin Park, Seungyoon Nam, Jun-Won Chung, Kyoung Oh Kim, Jungsuk An, and Jung Ho Kim. 2023. "Significance of 8-OHdG Expression as a Predictor of Survival in Colorectal Cancer" Cancers 15, no. 18: 4613. https://doi.org/10.3390/cancers15184613
APA StyleKang, M., Jeong, S., Park, S., Nam, S., Chung, J. -W., Kim, K. O., An, J., & Kim, J. H. (2023). Significance of 8-OHdG Expression as a Predictor of Survival in Colorectal Cancer. Cancers, 15(18), 4613. https://doi.org/10.3390/cancers15184613