
British Gynaecological Cancer Society Recommendations for Evidence Based, Population Data Derived Quality Performance Indicators for Ovarian Cancer

 , , , , , ,
, , , , , ,  , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Background
2. Learning from Other Health Systems: The Case for Evidence-Based, Population Data Derived, Routinely Evaluated QPIs
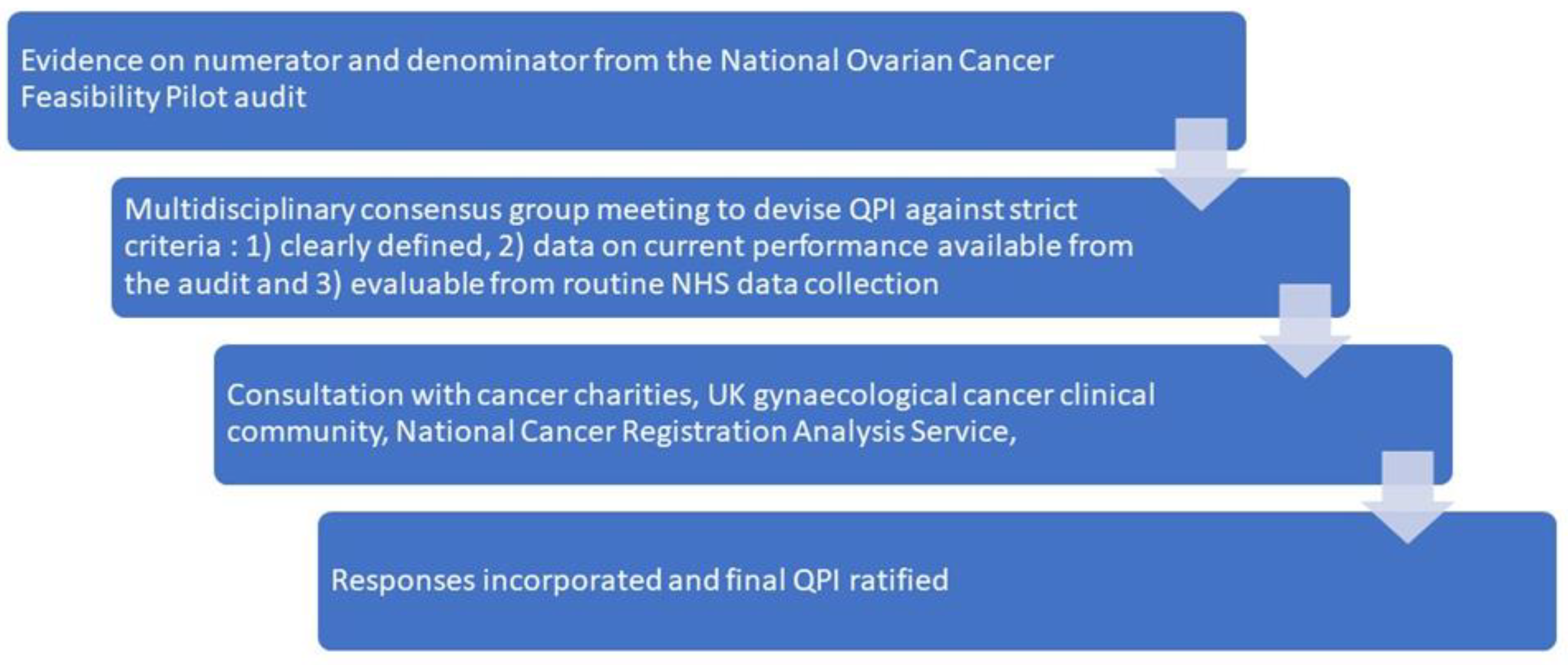
3. Principles Underlying Identification of Metrics as QPIs from Population-Based Data
3.1. QPI 1: Patients to Be Discussed at Diagnosis at a Specialist Multidisciplinary Team (MDT) Prior to a Decision for Treatment; Target 95%
3.1.1. Rationale
3.1.2. Best Practice Solutions
3.2. QPI 2: Patients Diagnosed with FIGO Stage II-IV or Unstaged Ovarian Cancer to Receive Anticancer Treatment (of Any Type); Target 80%
3.2.1. Rationale
3.2.2. Best Practice Solutions
3.3. QPI 3: Patients with FIGO Stage II-IV/Unstaged Ovarian Cancer to Receive Cytoreductive Surgery. Target: Minimum Target 55%; Optimal Target 70%
3.3.1. Rationale
3.3.2. Best Practice Solutions
3.4. QPI 4a: Patients with Ovarian Cancer Should Have Recording of FIGO Stage and WHO Performance Status at Initial Presentation; Target 95%. QPI 4b: Patients with Ovarian Cancer Who Undergo Cytoreductive Surgery Should Have the Quantity of Postoperative Residual Disease Recorded; Target 95%
3.4.1. Rationale
3.4.2. Best Practice Solutions
3.5. QPI 5a: Patients with Non-Mucinous Epithelial Ovarian Cancer to Be Tested for Germline BRCA1/2 Testing; Target 90%. QPI 5b: Patients with Advanced High Grade Serous and Clear Cell Carcinoma on Histology to Be Tested for Tumour BRCA1/2 Testing; Target 90%
3.5.1. Rationale
3.5.2. Best Practice Solutions
3.6. QPI 6: Patients to Be Enrolled into an NCRI Portfolio Study at Diagnosis or at Any Point during Treatment; Minimum Target 5%
3.6.1. Rationale
3.6.2. Best Practice Solutions
3.7. QPI Considered and Not Approved at This Point
- National data capture on residual disease is limited (currently around 80%), thus a metric for the completeness of cytoreduction is not reportable;
- Current evidence does not support any defined metrics on the proportion of women with advance disease (FIGO Stage IIIC and above) who should receive either primary surgery or delayed primary surgery after neoadjuvant chemotherapy. Four completed randomised controlled trials have demonstrated equivalence in overall survival [30]; results of ongoing randomised studies are awaited [49,50,51,52,53].
4. Implementing Metrics in Practice
5. Discussion
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Woo, Y.L.; Kyrgiou, M.; Bryant, A.; Everett, T.; Dickinson, H.O. Centralisation of services for gynaecological cancers—A Cochrane systematic review. Gynecol. Oncol. 2012, 126, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. A Policy Framework for Commissioning Cancer Services; Department of Health: London, UK, 1995; Volume 51.
- Guidance on Commissioning Cancer Services. Improving Outcomes in Gynaecological Cancers. The Manual. NHS Executive Catalogue No 16149. July 1999. Available online: https://pure.york.ac.uk/portal/en/publications/improving-outcomes-in-gynaecological-cancers-the-manual (accessed on 25 October 2022).
- Department of Health. NHS Cancer Plan; Department of Health: London, UK, 2000.
- Haward, R.A. The Calman-Hine report: A personal retrospective on the UK’s first comprehensive policy on cancer services. Lancet Oncol. 2006, 7, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Norell, C.H.; Butler, J.; Farrell, R.; Altman, A.; Bentley, J.; Cabasag, C.J.; Cohen, P.A.; Fegan, S.; Fung-Kee-Fung, M.; Gourley, C.; et al. Exploring international differences in ovarian cancer treatment: A comparison of clinical practice guidelines and patterns of care. Int. J. Gynecol. Cancer 2020, 30, 1748–1756. [Google Scholar] [CrossRef] [PubMed]
- Barton, D.P.; Adib, T.; Butler, J. Surgical practice of UK gynaecological oncologists in the treatment of primary advanced epithelial ovarian cancer (PAEOC): A questionnaire survey. Gynecol. Oncol. 2013, 131, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Naik, R.; Bayne, L.; Founta, C.; Kehoe, S.; Rustin, G.; Fotopoulou, C. Patient Support Groups Identifying Clinical Equipoise in UK Gynaecological Oncology Surgeons as the Basis for Trials in Ultraradical Surgery for Advanced Ovarian Cancer. Int. J. Gynecol. Cancer 2016, 26, 91–94. [Google Scholar] [CrossRef]
- Khoja, L.; Nolan, K.; Mekki, R.; Milani, A.; Mescallado, N.; Ashcroft, L.; Hasan, J.; Edmondson, R.; Winter-Roach, B.; Kitchener, H.C.; et al. Improved Survival from Ovarian Cancer in Patients Treated in Phase III Trial Active Cancer Centres in the UK. Clin. Oncol. (R. Coll. Radiol.) 2016, 28, 760–765. [Google Scholar] [CrossRef] [Green Version]
- Sundar, S.; Manchanda, R.; Gourley, C.; George, A.; Wallace, A.; Balega, J.; Williams, S.; Wallis, Y.; Edmondson, R.; Nicum, S.; et al. British Gynaecological Cancer Society/British Association of Gynaecological Pathology consensus for germline and tumor testing for BRCA1/2 variants in ovarian cancer in the United Kingdom. Int. J. Gynecol. Cancer 2021, 31, 272–278. [Google Scholar] [CrossRef]
- Munro, A.J. Interpretation of EUROCARE-5. Lancet Oncol. 2014, 15, 2–3. [Google Scholar] [CrossRef]
- Arnold, M.; Rutherford, M.J.; Bardot, A.; Ferlay, J.; Andersson, T.M.L.; Myklebust, T.Å.; Tervonen, H.; Thursfield, V.; Ransom, D.; Shack, L.; et al. Progress in cancer survival, mortality, and incidence in seven high-income countries 1995-2014 (ICBP SURVMARK-2): A population-based study. Lancet Oncol. 2019, 20, 1493–1505. [Google Scholar] [CrossRef] [Green Version]
- Group OCAFPS. Ovarian Cancer Audit Feasibility Pilot. In Disease Profile in England: Incidence, Mortality, Stage and Survival for Ovary, Fallopian Tube and Primary Peritoneal Carcinomas; Public Health England: London, UK, 2020. [Google Scholar]
- Prat, J.; FIGO Committee on Gynecologic Oncology. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int. J. Gynaecol. Obstet. 2014, 124, 1–5. [Google Scholar] [CrossRef]
- Hall, M.; Savvatis, K.; Nixon, K.; Kyrgiou, M.; Hariharan, K.; Padwick, M.; Owens, O.; Cunnea, P.; Campbell, J.; Farthing, A.; et al. Maximal-Effort Cytoreductive Surgery for Ovarian Cancer Patients with a High Tumor Burden: Variations in Practice and Impact on Outcome. Ann. Surg. Oncol. 2019, 26, 2943–2951. [Google Scholar] [CrossRef] [Green Version]
- Shalowitz, D.I.; Epstein, A.J.; Ko, E.M.; Giuntoli, R.L., 2nd. Non-surgical management of ovarian cancer: Prevalence and implications. Gynecol. Oncol. 2016, 142, 30–37. [Google Scholar] [CrossRef]
- Warren, J.L.; Harlan, L.C.; Trimble, E.L.; Stevens, J.; Grimes, M.; Cronin, K.A. Trends in the receipt of guideline care and survival for women with ovarian cancer: A population-based study. Gynecol. Oncol. 2017, 145, 486–492. [Google Scholar] [CrossRef]
- Timmermans, M.; Sonke, G.S.; Slangen, B.F.M.; Baalbergen, A.; Bekkers, R.L.M.; Fons, G.; Gerestein, C.G.; Kruse, A.J.; Roes, E.M.; Zusterzeel, P.L.M.; et al. Outcome of surgery in advanced ovarian cancer varies between geographical regions; opportunities for improvement in The Netherlands. Eur. J. Surg. Oncol. 2019, 45, 1425–1431. [Google Scholar] [CrossRef]
- Brand, A.H.; DiSilvestro, P.A.; Sehouli, J.; Berek, J.S. Cytoreductive surgery for ovarian cancer: Quality assessment. Ann. Oncol. 2017, 28, viii25–viii29. [Google Scholar] [CrossRef]
- Timilshina, N.; Finelli, A.; Tomlinson, G.; Gagliardi, A.; Sander, B.; Alibhai, S.M.H. National consensus quality indicators to assess quality of care for active surveillance in low-risk prostate cancer: An evidence-informed modified Delphi survey of Canadian urologists/radiation oncologists. Can. Urol. Assoc. J. 2021, 16, E212–E219. [Google Scholar] [CrossRef]
- Mariappan, P.; Johnston, A.; Padovani, L.; Clark, E.; Trail, M.; Hamid, S.; Hollins, G.; Simpson, H.; Thomas, B.G.; Hasan, R.; et al. Enhanced Quality and Effectiveness of Transurethral Resection of Bladder Tumour in Non-muscle-invasive Bladder Cancer: A Multicentre Real-world Experience from Scotland’s Quality Performance Indicators Programme. Eur. Urol. 2020, 78, 520–530. [Google Scholar] [CrossRef]
- Maharaj, A.D.; Evans, S.M.; Ioannou, L.J.; Croagh, D.; Earnest, A.; Holland, J.F.; Pilgrim, C.H.C.; Neale, R.E.; Goldstein, D.; Kench, J.G.; et al. The association between quality care and outcomes for a real-world population of Australian patients diagnosed with pancreatic cancer. HPB 2021, 24, 950–962. [Google Scholar] [CrossRef]
- Baxter, M.A.; MacDonald, G.; Malik, J.; Law, A.; Dahle-Smith, Å.; Mmeka, W.; Donat, R.; Shukla, C.; Connor, J.; Houston, C.; et al. Testicular cancer: Improving outcomes with national quality performance indicators. BMJ Open Qual. 2020, 9, e000726. [Google Scholar] [CrossRef] [Green Version]
- Fotopoulou, C.; Concin, N.; Planchamp, F.; Morice, P.; Vergote, I.; Du Bois, A.; Querleu, D. Quality indicators for advanced ovarian cancer surgery from the European Society of Gynaecological Oncology (ESGO): 2020 update. Int. J. Gynecol. Cancer 2020, 30, 436–440. [Google Scholar] [CrossRef]
- Querleu, D.; Planchamp, F.; Chiva, L.; Fotopoulou, C.; Barton, D.; Cibula, D.; Aletti, G.; Carinelli, S.; Creutzberg, C.; Davidson, B.; et al. European Society of Gynaecologic Oncology Quality Indicators for Advanced Ovarian Cancer Surgery. Int. J. Gynecol. Cancer 2016, 26, 1354–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fotopoulou, C.; Hall, M.; Cruickshank, D.; Gabra, H.; Ganesan, R.; Hughes, C.; Kehoe, S.; Ledermann, J.; Morrison, J.; Naik, R.; et al. British Gynaecological Cancer Society (BGCS) epithelial ovarian/fallopian tube/primary peritoneal cancer guidelines: Recommendations for practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Collaborators GBDUHC. Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1250–1284. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.; Balega, J.; Nevin, J.; Singh, K.; Elattar, A.; Kehoe, S.; Sundar, S. Reporting ‘Denominator’ data is essential for benchmarking and quality standards in ovarian cancer. Gynecol. Oncol. 2017, 146, 94–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Service NCRaA. CancerStats2; Public Health England: London, UK, 2021. [Google Scholar]
- Coleridge, S.L.; Bryant, A.; Kehoe, S.; Morrison, J. Neoadjuvant chemotherapy before surgery versus surgery followed by chemotherapy for initial treatment in advanced ovarian epithelial cancer. Cochrane Database Syst. Rev. 2021, 7, CD005343. [Google Scholar]
- Tattersall, A.; Ryan, N.; Wiggans, A.; Rogozinska, E.; Morrison, J. Poly(ADP-ribose) polymerase (PARP) inhibitors for the treatment of ovarian cancer. Cochrane Database Syst. Rev. 2022; in press. [Google Scholar]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–656. [Google Scholar] [CrossRef]
- Woo, Y.L.; Kyrgiou, M.; Bryant, A.; Everett, T.; Dickinson, H.O. Centralisation of services for gynaecological cancer. Cochrane Database Syst. Rev. 2012, 3, CD007945. [Google Scholar] [CrossRef] [Green Version]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat. Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef]
- Department of Health and Social Care. The NHS Long Term Plan; Department of Health and Social Care: London, UK, 2019.
- Team PEMKaI. Short Term Ovarian Cancer Mortality. In Network NCI; Public Health England: London, UK, 2013. [Google Scholar]
- Improvement NEaN. Rapid Diagnostic Centres Vision and 2019/20 Implementation Specification; NHS England: London, UK, 2019. [Google Scholar]
- Sundar, S.; Rick, C.; Dowling, F.; Au, P.; Snell, K.; Rai, N.; Champaneria, R.; Stobart, H.; Neal, R.; Davenport, C.; et al. Refining Ovarian Cancer Test accuracy Scores (ROCkeTS): Protocol for a prospective longitudinal test accuracy study to validate new risk scores in women with symptoms of suspected ovarian cancer. BMJ Open 2016, 6, e010333. [Google Scholar] [CrossRef] [Green Version]
- Middleton, M. SYMPLIFY Clinical Trial. 2021. Available online: https://www.cancer.ox.ac.uk/research/projects/symplify (accessed on 25 October 2022).
- Zijlstra, M.; Timmermans, M.; Fransen, H.; Van Der Aa, M.; Reyners, A.; Raijmakers, N.; Van De Poll-Franse, L. Treatment patterns and associated factors in patients with advanced epithelial ovarian cancer: A population-based study. Int. J. Gynecol. Cancer 2019, 29, 1032–1037. [Google Scholar] [CrossRef]
- van der Burg, M.E.; van Lent, M.; Buyse, M.; Kobierska, A.; Colombo, N.; Favalli, G.; Lacave, A.J.; Nardi, M.; Renard, J.; Pecorelli, S. The effect of debulking surgery after induction chemotherapy on the prognosis in advanced epithelial ovarian cancer. Gynecological Cancer Cooperative Group of the European Organization for Research and Treatment of Cancer. N. Engl. J. Med. 1995, 332, 629–634. [Google Scholar] [CrossRef]
- Morgan, R.D.; McNeish, I.A.; Cook, A.D.; James, E.C.; Lord, R.; Dark, G.; Glasspool, R.M.; Krell, J.; Parkinson, C.; Poole, C.J.; et al. Objective responses to first-line neoadjuvant carboplatin-paclitaxel regimens for ovarian, fallopian tube, or primary peritoneal carcinoma (ICON8): Post-hoc exploratory analysis of a randomised, phase 3 trial. Lancet Oncol. 2021, 22, 277–288. [Google Scholar] [CrossRef]
- Cummins, C.; Kumar, S.; Long, J.; Balega, J.; Broadhead, T.; Duncan, T.; Edmondson, R.J.; Fotopoulou, C.; Glasspool, R.M.; Kolomainen, D.; et al. Investigating the Impact of Ultra-Radical Surgery on Survival in Advanced Ovarian Cancer Using Population-Based Data in a Multicentre UK Study. Cancers 2022, 14, 4362. [Google Scholar] [CrossRef]
- ACPGBI, AUGIS and BGCS. Governance Models to Support Patient Safety when Undergoing Maximal Effort Cytoreductive Surgery for Advanced Ovarian/Fallopian Tube/Primary Peritoneal Cancer—A Joint Statement of ACPGBI, ASGBI, AUGIS and BGCS. 2021. Available online: https://ijgc.bmj.com/content/32/9/1216.long (accessed on 25 October 2022).
- NCRaAS. National Disease Registration Service: Staging Data in England; Public Health England: London, UK, 2020. [Google Scholar]
- Rust, K.; Spiliopoulou, P.; Tang, C.Y.; Bell, C.; Stirling, D.; Phang, T.H.F.; Davidson, R.; Mackean, M.; Nussey, F.; Glasspool, R.; et al. Routine germline BRCA1 and BRCA2 testing in patients with ovarian carcinoma: Analysis of the Scottish real-life experience. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 1451–1458. [Google Scholar] [CrossRef] [Green Version]
- NICE.org. Available online: https://www.nice.org.uk/ (accessed on 25 October 2022).
- England RCoSo. Available online: https://www.rcseng.ac.uk/standards-and-research/research/surgical-trials-initiative/surgical-specialty-leads/ (accessed on 25 October 2022).
- Reuss, A.; Du Bois, A.; Harter, P.; Fotopoulou, C.; Sehouli, J.; Aletti, G.; Guyon, F.; Greggi, S.; Mosgaard, B.J.; Reinthaller, A.; et al. TRUST: Trial of Radical Upfront Surgical Therapy in advanced ovarian cancer (ENGOT ov33/AGO-OVAR OP7). Int. J. Gynecol. Cancer 2019, 29, 1327–1331. [Google Scholar] [CrossRef]
- Jiang, R.; Zhu, J.; Kim, J.-W.; Liu, J.; Kato, K.; Kim, H.-S.; Zhang, Y.; Zhang, P.; Zhu, T.; Aoki, D.; et al. Study of upfront surgery versus neoadjuvant chemotherapy followed by interval debulking surgery for patients with stage IIIC and IV ovarian cancer, SGOG SUNNY (SOC-2) trial concept. (2005-0399 (Electronic)). J. Gynecol. Oncol. 2020, 31, e86. [Google Scholar] [CrossRef]
- Kumar, L.; Hariprasad, R.; Kumar, S.; Bhatla, N.; Thulkar, S.; Shukla, N. Neo-adjuvant chemotherapy in advanced epithelial ovarian cancer (EOC): A prospective, randomized study. Indian J. Med. Paediatr. Oncol. 2009, 30, 15. [Google Scholar] [CrossRef]
- Sayed, A. NCT04257786. Primary cyto-reductive surgery vs neo-adjuvant chemotherapy (NAC) in epithelial ovarian cancer. Clinicaltrials.gov. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04257786 (accessed on 25 October 2022).
- Shen, L. NCT04515602. Stratified evaluation of PDS and NACT-IDS in ovarian cancer. Clinicaltrials.gov. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04515602 (accessed on 25 October 2022).
- Burton, K. BGCS workforce Suvery for Gynaecological Oncology in the UK. In Proceedings of the BGCS Autumn Scientific Meeting, Cheltenham, UK, 7–8 July 2022; Available online: https://www.bgcs.org.uk/wp-content/uploads/2022/11/BGCS-Workforce-Summary.pdf (accessed on 25 October 2022).
- Timmermans, M.; Schuurman, M.S.; Ho, V.K.; Massuger, L.F.; Nijman, H.W.; van Gorp, T.; Sonke, G.S.; Kruitwagen, R.F.; van der Aa, M.A. Centralization of ovarian cancer in the Netherlands: Hospital of diagnosis no longer determines patients’ probability of undergoing surgery. Gynecol. Oncol. 2018, 148, 56–61. [Google Scholar] [CrossRef]
- Dahm-Kahler, P.; Palmqvist, C.; Staf, C.; Holmberg, E.; Johannesson, L. Centralized primary care of advanced ovarian cancer improves complete cytoreduction and survival—A population-based cohort study. Gynecol. Oncol. 2016, 142, 211–216. [Google Scholar] [CrossRef]
- Palmqvist, C.; Staf, C.; Mateoiu, C.; Johansson, M.; Albertsson, P.; Dahm-Kahler, P. Increased disease-free and relative survival in advanced ovarian cancer after centralized primary treatment. Gynecol. Oncol. 2020, 159, 409–417. [Google Scholar] [CrossRef]
- Falconer, H.; Joneborg, U.; Krawiec, K.; Palsdottir, K.; Bottai, M.; Salehi, S. Ultra-radical upfront surgery does not improve survival in women with advanced epithelial ovarian cancer; a natural experiment in a complete population. Gynecol. Oncol. 2020, 159, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Soerensen, S.; Bjørn, S.F.; Jochumsen, K.; Jensen, P.T.; Thranov, I.R.; Hare-Bruun, H.; Seibæk, L.; Høgdall, C. Danish Gynecological Cancer Database. Clin. Epidemiol. 2016, 8, 485–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggink, F.A.; Vermue, M.C.; Van der Spek, C.; Arts, H.J.; Apperloo, M.J.; Nijman, H.W.; Niemeijer, G.C. The impact of centralization of services on treatment delay in ovarian cancer: A study on process quality. Int. J. Qual. Health Care 2017, 29, 810–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarazi, M.; Guest, K.; Cook, A.J.; Balasubramaniam, D.; Bailey, C.M.H. Two and five year survival for colorectal cancer after resection with curative intent: A retrospective cohort study. Int. J. Surg. 2018, 55, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Adizie, J.B.; Khakwani, A.; Beckett, P.; Hubbard, R.; Navani, N.; Harden, S.V.; Woolhouse, I. Impact of organisation and specialist service delivery on lung cancer outcomes. Thorax 2019, 74, 546–550. [Google Scholar] [CrossRef]
- Parry, M.G.; Boyle, J.M.; Nossiter, J.; Morris, M.; Sujenthiran, A.; Berry, B.; Cathcart, P.; Aggarwal, A.; van der Meulen, J.; Payne, H.; et al. Determinants of variation in radical local treatment for men with high-risk localised or locally advanced prostate cancer in England. Prostate Cancer Prostatic Dis. 2021; online ahead of print. [Google Scholar]
- Colombo, N.; Sessa, C.; du Bois, A.; Ledermann, J.; McCluggage, W.G.; McNeish, I.; Morice, P.; Pignata, S.; Ray-Coquard, I.; Vergote, I.; et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Ann. Oncol. 2019, 30, 672–705. [Google Scholar] [CrossRef] [Green Version]
- Vanderpuye, V.D.; Clemenceau, J.R.V.; Temin, S.; Aziz, Z.; Burke, W.M.; Cevallos, N.L.; Chuang, L.T.; Colgan, T.J.; del Carmen, M.G.; Fujiwara, K.; et al. Assessment of Adult Women With Ovarian Masses and Treatment of Epithelial Ovarian Cancer: ASCO Resource-Stratified Guideline. JCO Glob. Oncol. 2021, 7, 1032–1066. [Google Scholar] [CrossRef]
- Fotopoulou, C.; Gourley, C.; Ledermann, J.; Hall, M.; Ayub, J.; Fildes, L.; Roebuck, N.; Lord, R.; Miller, R.; Sundar, S. 109 Understanding current multidisciplinary team structures and management practices for advanced ovarian cancer in the UK: The KNOW-OC survey. Int. J. Gynecol. Cancer 2021, 31 (Suppl. S3), A198–A199. [Google Scholar]
- Falzone, L.; Scandurra, G.; Lombardo, V.; Gattuso, G.; Lavoro, A.; Distefano, A.B.; Scibilia, G.; Scollo, P. A multidisciplinary approach remains the best strategy to improve and strengthen the management of ovarian cancer (Review). Int. J. Oncol. 2021, 59, 1–14. [Google Scholar] [CrossRef]
- Bengrine, L.; Bakrin, N.; Rousseau, F.; Lavoué, V.; Falandry, C. Multi-Disciplinary Care Planning of Ovarian Cancer in Older Patients: General Statement-A Position Paper from SOFOG-GINECO-FRANCOGYN-SFPO. Cancers 2022, 14, 1295. [Google Scholar] [CrossRef]
- Temkin, S.M.; Smeltzer, M.P.; Dawkins, M.D.; Boehmer, L.M.; Senter, L.; Black, D.R.; Blank, S.V.; Yemelyanova, A.; Magliocco, A.M.; Finkel, M.A.; et al. Improving the quality of care for patients with advanced epithelial ovarian cancer: Program components, implementation barriers, and recommendations. Cancer 2021, 128, 654–664. [Google Scholar] [CrossRef]
- Digital, N. Ovarian Cancer Audit Feasibility Pilot. 2022. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/ovarian-cancer-audit-feasibility-pilot (accessed on 25 October 2022).
- Leung, D.; Funingana, G. Ovarian Cancer Action. Available online: https://ovarian.org.uk/our-research/improve-uk/improve-uk-Birmingham-Cambridge/ (accessed on 25 October 2022).


{kind=link}
| QPI | Number | Indicator | Target | Description and Reporting |
|---|---|---|---|---|
| Patients to be discussed at diagnosis at a specialist MDT prior to a decision for treatment. | QPI 1 | Process | Target 95% | Number of patients with ovarian cancer discussed at the MDT prior to a decision for definitive treatment. Numerator: Number of patients with ovarian cancer discussed at the MDT prior to a decision for definitive treatment. Denominator: All patients diagnosed with ovarian cancer. Exclusions: Borderline ovarian tumours. Reportable by: Hospital Trust; Integrated Cancer System; and Cancer Alliance. Reported on: CancerStats2 and in public domain reports |
| Patients diagnosed with Stage II-IV or unstaged Ovarian cancer to receive anticancer treatment of any type. | QPI 2 | Process | Target 80% | Numerator: patients with stage II-IV or unstaged ovarian cancer receiving anticancer treatment. Denominator: All patients with stage II-IV or unstaged ovarian cancer diagnosed. Exclusions: Borderline ovarian tumours. Reportable by: Hospital Trust; Integrated Cancer System; and Cancer Alliance. Reported on: CancerStats2 and in public domain reports. Data in public domain to be reported adjusted for age and deprivation. |
| Patients with Stage II-IV/unstaged ovarian cancer to receive cytoreductive surgery. | QPI 3 | Structural | Minimum target 55%; Optimal target 70%. | Numerator: patients receiving primary surgery or delayed debulking surgery after neoadjuvant chemotherapy. Denominator: All Stage II-IV/unstaged patients with ovarian cancer. Exclusion: Borderline ovarian tumours. Reportable by: Hospital Trust; Integrated Cancer System; and Cancer Alliance. Reported on: CancerStats2 and in public domain reports. Data in public domain to be reported adjusted for age and deprivation. |
| Patients with ovarian cancer should have recording of FIGO stage, WHO performance status, at diagnosis. | QPI 4a | Outcome | Target 95% | For performance status and stage. Numerator: All patients with ovarian cancer discussed at MDT. Denominator: All patients with ovarian cancer. Exclusion: borderline ovarian tumours. Reportable by: Hospital Trust; Integrated Cancer System; and Cancer Alliance. Reported on: CancerStats2 and in public domain reports. |
| Patients with ovarian cancer undergoing primary or interval debulking surgery should have recording of residual disease. | QPI 4b | Outcome | Target 95% | Numerator: All patients with ovarian cancer undergoing surgery. Denominator: All patients with ovarian cancer. Exclusion: borderline ovarian tumours. Reportable by: Hospital Trust; Integrated Cancer System; and Cancer Alliance. Reported on: CancerStats2 and in public domain reports. |
| Patients with non-mucinous epithelial ovarian cancer on histology to be tested for germline BRCA1/2 testing. | QPI 5a | Outcome | Target 90% | Numerator: All patients with non-mucinous epithelial ovarian cancer histology, including those with missing histology or unspecified histology undergoing testing for germline BRCA1/2. Denominator: All patients with non-mucinous epithelial ovarian cancer histology, including those with missing histology or unspecified histology. Exclusion: borderline ovarian tumours, mucinous epithelial ovarian cancers. Reportable by: Hospital Trust; Integrated Cancer System; and Cancer Alliance. Reported on: CancerStats2 and in public domain reports. |
| Patients with advanced high grade serous and clear cell cancer on histology to be tested for tumour BRCA1/2 testing. | QPI 5b | Outcome | Target 90% | Numerator: All patients with Stage III-IV/unstaged high grade serous or clear cell epithelial ovarian cancer histology, including those with missing histology or unspecified histology tested for tumour BRCA1/2. Denominator: All patients with Stage III-IV/unstaged high grade serous or clear cell epithelial ovarian cancer histology, including those with missing histology or unspecified histology. Exclusion: borderline ovarian tumours. Stage 1–2 cancer, histology types other than high grade serous or clear cell epithelial ovarian cancer. Reportable by: Hospital Trust; Integrated Cancer System; and Cancer Alliance. Reported on: CancerStats2 and in public domain reports. |
| Patients to be enrolled into an NCRI portfolio study at diagnosis. | QPI 6 | Structural | Minimum Target 5% | Numerator: number of patients with ovarian cancer discussed at the MDT recruited into a NCRI portfolio study. Denominator: All patients diagnosed with ovarian cancer. Exclusions: borderline ovarian tumours. Reportable by: Hospital Trust; Integrated Cancer System; and Cancer Alliance. Reported on: Public domain reports. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sundar, S.; Nordin, A.; Morrison, J.; Wood, N.; Ghaem-Maghami, S.; Nieto, J.; Phillips, A.; Butler, J.; Burton, K.; Gornall, R.; et al. British Gynaecological Cancer Society Recommendations for Evidence Based, Population Data Derived Quality Performance Indicators for Ovarian Cancer. Cancers 2023, 15, 337. https://doi.org/10.3390/cancers15020337
Sundar S, Nordin A, Morrison J, Wood N, Ghaem-Maghami S, Nieto J, Phillips A, Butler J, Burton K, Gornall R, et al. British Gynaecological Cancer Society Recommendations for Evidence Based, Population Data Derived Quality Performance Indicators for Ovarian Cancer. Cancers. 2023; 15(2):337. https://doi.org/10.3390/cancers15020337
Chicago/Turabian StyleSundar, Sudha, Andy Nordin, Jo Morrison, Nick Wood, Sadaf Ghaem-Maghami, Jo Nieto, Andrew Phillips, John Butler, Kevin Burton, Rob Gornall, and et al. 2023. "British Gynaecological Cancer Society Recommendations for Evidence Based, Population Data Derived Quality Performance Indicators for Ovarian Cancer" Cancers 15, no. 2: 337. https://doi.org/10.3390/cancers15020337
APA StyleSundar, S., Nordin, A., Morrison, J., Wood, N., Ghaem-Maghami, S., Nieto, J., Phillips, A., Butler, J., Burton, K., Gornall, R., Dobbs, S., Glasspool, R., Peevor, R., Ledermann, J., McNeish, I., Ratnavelu, N., Duncan, T., Frost, J., Lim, K., ... Fotopoulou, C. (2023). British Gynaecological Cancer Society Recommendations for Evidence Based, Population Data Derived Quality Performance Indicators for Ovarian Cancer. Cancers, 15(2), 337. https://doi.org/10.3390/cancers15020337