


Immune Checkpoint Pathway Expression in Lymphocyte Subpopulations in Patients with Common Variable Immunodeficiency and Chronic Lymphocytic Leukemia
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Characteristics of Patients and Research Material
2.2. Analysis of the Immunophenotype of Peripheral Blood
2.3. Evaluation of the Concentration of Soluble Forms of Immune Checkpoints and Their Ligands in the Serum
2.4. Statistical Analysis of the Obtained Test Results
3. Result
3.1. Comparative Analysis of Infections and Selected Peripheral Blood Parameters (Morphology, Biochemistry, Immunophenotype) of Patients
3.2. Comparative Analysis of Selected Subpopulations of Peripheral Blood Lymphocytes Showing Positive expression of the Tested Immunological Checkpoints and Their Ligands
3.3. Analysis of Serum Concentrations of Selected Immunological Checkpoints and Their Ligands
3.4. Analysis of the Correlation of the Obtained Test Results with Biological Parameters
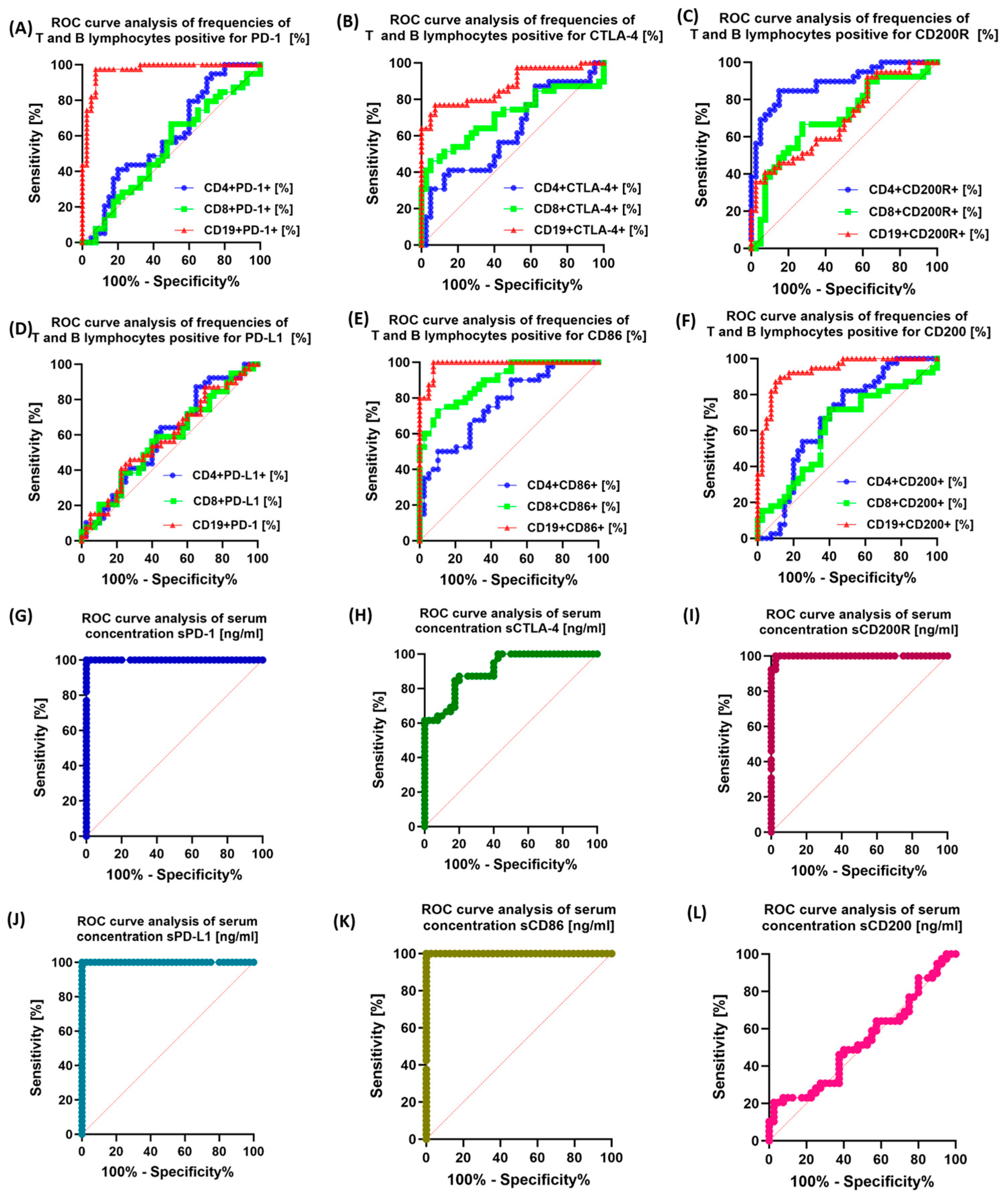
3.5. Assessment of the Potential Diagnostic Utility of Examined Immunological Checkpoints and Their Corresponding Ligands
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ebrahim, H.; Fisha, T.; Debash, H.; Bisetegn, H. Patterns of Bone Marrow Confirmed Malignant and Non-Malignant Hematological Disorders in Patients with Abnormal Hematological Parameters in Northeast Ethiopia. J. Blood Med. 2022, 13, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Sochacka-Ćwikła, A.; Mączyński, M.; Regiec, A. FDA-Approved Drugs for Hematological Malignancies—The Last Decade Review. Cancers 2021, 14, 87. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Wu, J.; Wang, Q.; Liang, Y.; Li, X.; Chen, G.; Ma, L.; Liu, X.; Zhou, F. Global Burden of Hematologic Malignancies and Evolution Patterns over the Past 30 years. Blood Cancer J. 2023, 13, 82. [Google Scholar] [CrossRef] [PubMed]
- Verhoeven, D.; Stoppelenburg, A.J.; Meyer-Wentrup, F.; Boes, M. Increased Risk of Hematologic Malignancies in Primary Immunodeficiency Disorders: Opportunities for Immunotherapy. Clin. Immunol. 2018, 190, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Aliyath, A.; Eni-Olotu, A.; Donaldson, N.; Trivedi, P. Malignancy-Associated Immune Responses: Lessons from Human Inborn Errors of Immunity. Immunology 2023, 170, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Haas, O.A. Primary Immunodeficiency and Cancer Predisposition Revisited: Embedding Two Closely Related Concepts Into an Integrative Conceptual Framework. Front. Immunol. 2019, 9, 3136. [Google Scholar] [CrossRef]
- Allegra, A.; Tonacci, A.; Musolino, C.; Pioggia, G.; Gangemi, S. Secondary Immunodeficiency in Hematological Malignancies: Focus on Multiple Myeloma and Chronic Lymphocytic Leukemia. Front. Immunol. 2021, 12, 738915. [Google Scholar] [CrossRef]
- Raje, N.; Dinakar, C. Overview of Immunodeficiency Disorders. Immunol. Allergy Clin. N. Am. 2015, 35, 599–623. [Google Scholar] [CrossRef]
- Ballow, M.; Sánchez-Ramón, S.; Walter, J.E. Secondary Immune Deficiency and Primary Immune Deficiency Crossovers: Hematological Malignancies and Autoimmune Diseases. Front. Immunol. 2022, 13, 928062. [Google Scholar] [CrossRef]
- Mukkamalla, S.K.R.; Taneja, A.; Malipeddi, D.; Master, S.R. Chronic Lymphocytic Leukemia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kipps, T.J.; Stevenson, F.K.; Wu, C.J.; Croce, C.M.; Packham, G.; Wierda, W.G.; O’Brien, S.; Gribben, J.; Rai, K. Chronic Lymphocytic Leukaemia. Nat. Rev. Dis. Prim. 2017, 3, 16096. [Google Scholar] [CrossRef]
- Hallek, M.; Al-Sawaf, O. Chronic Lymphocytic Leukemia: 2022 Update on Diagnostic and Therapeutic Procedures. Am. J. Hematol. 2021, 96, 1679–1705. [Google Scholar] [CrossRef] [PubMed]
- Devi, A.; Thielemans, L.; Ladikou, E.; Nandra, T.K.; Chevassut, T. Lymphocytosis and Chronic Lymphocytic Leukaemia: Investigation and Management. Clin. Med. 2022, 22, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, R. Chronic Lymphocytic Leukaemia: An Updated Approach to Diagnosis and Management in General Practice. Aust. Fam. Physician 2017, 46, 493–496. [Google Scholar] [PubMed]
- Rajabi, B.; Sweetenham, J.W. Mantle Cell Lymphoma: Observation to Transplantation. Ther. Adv. Hematol. 2015, 6, 37–48. [Google Scholar] [CrossRef]
- Schetelig, J.; Dreger, P. Chronic Lymphocytic Leukemia. In The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies; Carreras, E., Dufour, C., Mohty, M., Kröger, N., Eds.; Springer: Cham, Switzerland, 2019; ISBN 978-3-030-02277-8. [Google Scholar]
- Miller, K.D.; Nogueira, L.; Devasia, T.; Mariotto, A.B.; Yabroff, K.R.; Jemal, A.; Kramer, J.; Siegel, R.L. Cancer Treatment and Survivorship Statistics, 2022. CA A Cancer J. Clin. 2022, 72, 409–436. [Google Scholar] [CrossRef]
- McCusker, C.; Upton, J.; Warrington, R. Primary immunodeficiency. Allergy Asthma Clin. Immunol. 2018, 14, 61. [Google Scholar] [CrossRef]
- McCusker, C.; Warrington, R. Primary immunodeficiency. Allergy Asthma Clin. Immunol. 2011, 7, S11. [Google Scholar] [CrossRef]
- Mayor, P.C.; Eng, K.H.; Singel, K.L.; Abrams, S.I.; Odunsi, K.; Moysich, K.B.; Fuleihan, R.; Garabedian, E.; Lugar, P.; Ochs, H.D.; et al. Cancer in Primary Immunodeficiency Diseases: Cancer Incidence in the United States Immune Deficiency Network Registry. J. Allergy Clin. Immunol. 2018, 141, 1028–1035. [Google Scholar] [CrossRef]
- Salavoura, K.; Kolialexi, A.; Tsangaris, G.; Mavrou, A. Development of Cancer in Patients with Primary Immunodeficiencies. Anticancer Res. 2008, 28, 1263–1269. [Google Scholar]
- Tam, J.S.; Routes, J.M. Common Variable Immunodeficiency. Am. J. Rhinol. Allergy 2013, 27, 260–265. [Google Scholar] [CrossRef]
- Chapel, H.; Cunningham-Rundles, C. Update in Understanding Common Variable Immunodeficiency Disorders (CVIDs) and the Management of Patients with These Conditions. Br. J. Haematol. 2009, 145, 709–727. [Google Scholar] [CrossRef] [PubMed]
- Mormile, I.; Punziano, A.; Riolo, C.A.; Granata, F.; Williams, M.; de Paulis, A.; Spadaro, G.; Rossi, F.W. Common Variable Immunodeficiency and Autoimmune Diseases: A Retrospective Study of 95 Adult Patients in a Single Tertiary Care Center. Front. Immunol. 2021, 12, 652487. [Google Scholar] [CrossRef] [PubMed]
- Bruns, L.; Panagiota, V.; von Hardenberg, S.; Schmidt, G.; Adriawan, I.R.; Sogka, E.; Hirsch, S.; Ahrenstorf, G.; Witte, T.; Schmidt, R.E.; et al. Common Variable Immunodeficiency-Associated Cancers: The Role of Clinical Phenotypes, Immunological and Genetic Factors. Front. Immunol. 2022, 13, 742530. [Google Scholar] [CrossRef] [PubMed]
- Costagliola, G.; Consolini, R. Lymphadenopathy at the Crossroad between Immunodeficiency and Autoinflammation: An Intriguing Challenge. Clin. Exp. Immunol. 2021, 205, 288–305. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.-E.; Cunningham-Rundles, C. Non-Infectious Complications of Common Variable Immunodeficiency: Updated Clinical Spectrum, Sequelae, and Insights to Pathogenesis. Front. Immunol. 2020, 11, 149. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, J.; Mendonca, D.; Conner, M.; Savidge, T.; Swennes, A.; Walter, J.; Petrosino, J.; Kheradmand, F. Selected Abstracts from the 13th Annual Meeting of the Clinical Immunology Society: 2022 Annual Meeting: Immune Deficiency and Dysregulation North American Conference. J. Clin. Immunol. 2022, 42, 1–115. [Google Scholar] [CrossRef]
- Kiaee, F.; Azizi, G.; Rafiemanesh, H.; Zainaldain, H.; Rizvi, F.S.; Alizadeh, M.; Jamee, M.; Mohammadi, S.; Habibi, S.; Sharifi, L.; et al. Malignancy in Common Variable Immunodeficiency: A Systematic Review and Meta-Analysis. Expert Rev. Clin. Immunol. 2019, 15, 1105–1113. [Google Scholar] [CrossRef]
- Mateti, N.R.; Vaddepally, R.K.; Chandra, A.B.; Skaria, P.E. Myelodysplastic Syndrome in a Patient With Common Variable Immunodeficiency: A Rare Occurrence. Cureus 2022, 14, e28690. [Google Scholar] [CrossRef]
- Műzes, G.; Sipos, F. Autoimmunity and Carcinogenesis: Their Relationship under the Umbrella of Autophagy. Biomedicines 2023, 11, 1130. [Google Scholar] [CrossRef]
- Guo, Z.; Zhang, R.; Yang, A.-G.; Zheng, G. Diversity of Immune Checkpoints in Cancer Immunotherapy. Front. Immunol. 2023, 14, 1121285. [Google Scholar] [CrossRef]
- Paluch, C.; Santos, A.M.; Anzilotti, C.; Cornall, R.J.; Davis, S.J. Immune Checkpoints as Therapeutic Targets in Autoimmunity. Front. Immunol. 2018, 9, 2306. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.; Ganguly, A.; Chatterjee, K.; Spada, S.; Mukherjee, S. Targets of Immune Escape Mechanisms in Cancer: Basis for Development and Evolution of Cancer Immune Checkpoint Inhibitors. Biology 2023, 12, 218. [Google Scholar] [CrossRef] [PubMed]
- Sperk, M.; Van Domselaar, R.; Neogi, U. Immune Checkpoints as the Immune System Regulators and Potential Biomarkers in HIV-1 Infection. Int. J. Mol. Sci. 2018, 19, 2000. [Google Scholar] [CrossRef] [PubMed]
- Mpakali, A.; Stratikos, E. The Role of Antigen Processing and Presentation in Cancer and the Efficacy of Immune Checkpoint Inhibitor Immunotherapy. Cancers 2021, 13, 134. [Google Scholar] [CrossRef] [PubMed]
- Ghaedrahmati, F.; Esmaeil, N.; Abbaspour, M. Targeting Immune Checkpoints: How to Use Natural Killer Cells for Fighting against Solid Tumors. Cancer Commun. 2023, 43, 177–213. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Cho, S.W. The Evasion Mechanisms of Cancer Immunity and Drug Intervention in the Tumor Microenvironment. Front. Pharmacol. 2022, 13, 868695. [Google Scholar] [CrossRef] [PubMed]
- Lao, Y.; Shen, D.; Zhang, W.; He, R.; Jiang, M. Immune Checkpoint Inhibitors in Cancer Therapy—How to Overcome Drug Resistance? Cancers 2022, 14, 3575. [Google Scholar] [CrossRef]
- Waldman, A.D.; Fritz, J.M.; Lenardo, M.J. A Guide to Cancer Immunotherapy: From T Cell Basic Science to Clinical Practice. Nat. Rev. Immunol. 2020, 20, 651–668. [Google Scholar] [CrossRef]
- Arruga, F.; Gyau, B.B.; Iannello, A.; Vitale, N.; Vaisitti, T.; Deaglio, S. Immune Response Dysfunction in Chronic Lymphocytic Leukemia: Dissecting Molecular Mechanisms and Microenvironmental Conditions. Int. J. Mol. Sci. 2020, 21, 1825. [Google Scholar] [CrossRef]
- He, R.; Ding, W.; Viswanatha, D.S.; Chen, D.; Shi, M.; Van Dyke, D.; Tian, S.; Dao, L.N.; Parikh, S.A.M.; Shanafelt, T.D.; et al. PD-1 Expression in Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (CLL/SLL) and Large B-cell Richter Transformation (DLBCL-RT): A Characteristic Feature of DLBCL-RT and Potential Surrogate Marker for Clonal Relatedness. Am. J. Surg. Pathol. 2018, 42, 843–854. [Google Scholar] [CrossRef]
- Landego, I.; Hewitt, D.; Hibbert, I.; Dhaliwal, D.; Pieterse, W.; Grenier, D.; Wong, R.; Johnston, J.; Banerji, V. PD-1 Inhibition in Malignant Melanoma and Lack of Clinical Response in Chronic Lymphocytic Leukemia in the Same Patients: A Case Series. Curr. Oncol. 2020, 27, 169–172. [Google Scholar] [CrossRef]
- Brusa, D.; Serra, S.; Coscia, M.; Rossi, D.; D’Arena, G.; Laurenti, L.; Jaksic, O.; Fedele, G.; Inghirami, G.; Gaidano, G.; et al. The PD-1/PD-L1 Axis Contributes to T-Cell Dysfunction in Chronic Lymphocytic Leukemia. Haematologica 2013, 98, 953–963. [Google Scholar] [CrossRef]
- Qorraj, M.; Bruns, H.; Böttcher, M.; Weigand, L.; Saul, D.; Mackensen, A.; Jitschin, R.; Mougiakakos, D. The PD-1/PD-L1 Axis Contributes to Immune Metabolic Dysfunctions of Monocytes in Chronic Lymphocytic Leukemia. Leukemia 2017, 31, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Do, P.; Beckwith, K.A.; Cheney, C.; Tran, M.; Beaver, L.; Griffin, B.G.; Mo, X.; Liu, Y.; Lapalombella, R.; Hertlein, E.; et al. Leukemic B Cell CTLA-4 Suppresses Costimulation of T Cells. J. Immunol. 2019, 202, 2806–2816. [Google Scholar] [CrossRef] [PubMed]
- Mittal, A.K.; Chaturvedi, N.K.; Rohlfsen, R.A.; Gupta, P.; Joshi, A.D.; Hegde, G.V.; Bociek, R.G.; Joshi, S.S. Role of CTLA4 in the Proliferation and Survival of Chronic Lymphocytic Leukemia. PLoS ONE 2013, 8, e70352. [Google Scholar] [CrossRef] [PubMed]
- Yano, M.; Nunes, J.; Mo, X.; Rogers, K.A.; Woyach, J.A.; Byrd, J.C.; Muthusamy, N. Differential Regulation of CTLA4 Expression through BTK-Dependent and Independent Mechanisms in CLL. Blood Adv. 2022, 6, 5440–5448. [Google Scholar] [CrossRef]
- Agarwal, S.; Gomez, A.A.; Da, T.; Kuramitsu, S.; Kong, W.; Ravikumar, P.; Gohil, M.; Davis, M.M.; Fraietta, J.A.; Plesa, G.; et al. Abstract 5571: Disruption of Cell-Intrinsic Checkpoint Regulator CTLA-4 in CD19 Directed CAR T Cells Provides Clinical Efficacy in CLL Patients. Cancer Res. 2022, 82, 5571. [Google Scholar] [CrossRef]
- D’Arena, G.; De Feo, V.; Pietrantuono, G.; Seneca, E.; Mansueto, G.; Villani, O.; La Rocca, F.; D’Auria, F.; Statuto, T.; Valvano, L.; et al. CD200 and Chronic Lymphocytic Leukemia: Biological and Clinical Relevance. Front. Oncol. 2020, 10, 584427. [Google Scholar] [CrossRef]
- Mora, A.; Bosch, R.; Cuellar, C.; Vicente, E.P.; Blanco, L.; Martino, R.; Ubeda, J.M.; Sierra, J.; Moreno, C.; Nomdedeu, J. CD200 Is a Useful Marker in the Diagnosis of Chronic Lymphocytic Leukemia. Cytom. Part B Clin. Cytom. 2019, 96, 143–148. [Google Scholar] [CrossRef]
- Iova, A.; Vlădăreanu, A.; Bumbea, H.; Begu, M.; Vasile, D.; Andruş, E. CD 200—A Useful Marker in Chronic B Lymphoprolipherative Disorders. J. Med. Life 2012, 5, 66–70. [Google Scholar]
- Brent, J.; Guzman, D.; Bangs, C.; Grimbacher, B.; Fayolle, C.; Huissoon, A.; Bethune, C.; Thomas, M.; Patel, S.; Jolles, S.; et al. Clinical and Laboratory Correlates of Lung Disease and Cancer in Adults with Idiopathic Hypogammaglobulinaemia. Clin. Exp. Immunol. 2016, 184, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Lougaris, V.; Tabellini, G.; Vitali, M.; Baronio, M.; Patrizi, O.; Tampella, G.; Biasini, A.; Moratto, D.; Parolini, S.; Plebani, A. Defective Natural Killer–Cell Cytotoxic Activity in NFKB2-Mutated CVID-Like Disease. J. Allergy Clin. Immunol. 2015, 135, 1641–1643. [Google Scholar] [CrossRef] [PubMed]
- Wehr, C. Trying to Understand NK Cell Function in Vivo Points towards a Severity Score for CVID Patients. EBioMedicine 2016, 6, 18–19. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.K.; Huissoon, A.P. T-Cell Abnormalities in Common Variable Immunodeficiency: The Hidden Defect. J. Clin. Pathol. 2016, 69, 672–676. [Google Scholar] [CrossRef]
- Coraglia, A.; Galassi, N.; Fernández Romero, D.S.; Juri, M.C.; Felippo, M.; Malbrán, A.; de Bracco, M.M.E. Common Variable Immunodeficiency and Circulating TFH. J. Immunol. Res. 2016, 2016, 4951587. [Google Scholar] [CrossRef] [PubMed]
- Azizi, G.; Rezaei, N.; Kiaee, F.; Tavakolinia, N.; Yazdani, R.; Mirshafiey, A.; Aghamohammadi, A. T Cell Abnormalities in Common Variable Immunodeficiency. J. Investig. Allergol. Clin. Immunol. 2016, 26, 233–243. [Google Scholar] [CrossRef]
- Verma, N.; Burns, S.O.; Walker, L.S.K.; Sansom, D.M. Immune Deficiency and Autoimmunity in Patients with CTLA-4 (CD152) Mutations. Clin. Exp. Immunol. 2017, 190, 1–7. [Google Scholar] [CrossRef]
- Salami, F.; Fekrvand, S.; Yazdani, R.; Shahkarami, S.; Azizi, G.; Bagheri, Y.; Delavari, S.; Shariati, S.; Mahdaviani, S.A.; Nabavi, M.; et al. Evaluation of Expression of LRBA and CTLA-4 Proteins in Common Variable Immunodeficiency Patients. Immunol. Investig. 2022, 51, 381–394. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Correlations of Immunological Parameters with the Number of Infections for CVID Patients | |||
| A Pair of Variables | R | t (n − 2) | p |
| CD8+ CD200+ and gastrointestinal infections | −0.331 | −2132 | 0.040 * |
| CD4+ CTLA-4+ and skin infections | 0.365 | 2386 | 0.022 * |
| CD8+ PDL-1+ and gastrointestinal infections | 0.483 | 3357 | 0.002 * |
| CD8+ PDL-1+ and total number of infections | 0.458 | 3136 | 0.003 * |
| sPD-L1 and skin infections | 0.318 | 2042 | 0.048 * |
| Correlations of Immunological Parameters with the Number of Infections for CLL Patients | |||
| A Pair of Variables | R | t (n − 2) | p |
| CD4+ CD200+ and infections of the upper and lower respiratory tract | 0.374 | 2484 | 0.018 * |
| CD4+ CD200+ and Skin infections | 0.380 | 2534 | 0.016 * |
| CD4+ CD200+ and total number of infections | 0.477 | 3346 | 0.002 * |
| CD19+ CD200R+ and gastrointestinal infections | 0.349 | 2294 | 0.027 * |
| CD4+ CD200R+ and urinary tract infections | −0.344 | −2260 | 0.030 * |
| CD8+ CD200R+ and gastrointestinal infections | 0.325 | 2118 | 0.041 * |
| CD8+ CTLA-4+ and urinary tract infections | 0.376 | 2502 | 0.017 * |
| CD8+ PD-1+ and infections of the upper and lower respiratory tract | 0.315 | 2046 | 0.048 * |
| CD8+ PDL-1+ and infections of the upper and lower respiratory tract | −0.366 | −2425 | 0.020 * |
| CD8+ PDL-1+ and total number of infections | −0.394 | −2646 | 0.012 * |
| sPD-L1 and skin infections | 0.349 | 2293 | 0.027 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mertowska, P.; Mertowski, S.; Smolak, K.; Kita, A.; Kita, G.; Guz, K.; Pasiarski, M.; Grywalska, E. Immune Checkpoint Pathway Expression in Lymphocyte Subpopulations in Patients with Common Variable Immunodeficiency and Chronic Lymphocytic Leukemia. Cancers 2023, 15, 5184. https://doi.org/10.3390/cancers15215184
Mertowska P, Mertowski S, Smolak K, Kita A, Kita G, Guz K, Pasiarski M, Grywalska E. Immune Checkpoint Pathway Expression in Lymphocyte Subpopulations in Patients with Common Variable Immunodeficiency and Chronic Lymphocytic Leukemia. Cancers. 2023; 15(21):5184. https://doi.org/10.3390/cancers15215184
Chicago/Turabian StyleMertowska, Paulina, Sebastian Mertowski, Konrad Smolak, Aleksandra Kita, Gabriela Kita, Katarzyna Guz, Marcin Pasiarski, and Ewelina Grywalska. 2023. "Immune Checkpoint Pathway Expression in Lymphocyte Subpopulations in Patients with Common Variable Immunodeficiency and Chronic Lymphocytic Leukemia" Cancers 15, no. 21: 5184. https://doi.org/10.3390/cancers15215184
APA StyleMertowska, P., Mertowski, S., Smolak, K., Kita, A., Kita, G., Guz, K., Pasiarski, M., & Grywalska, E. (2023). Immune Checkpoint Pathway Expression in Lymphocyte Subpopulations in Patients with Common Variable Immunodeficiency and Chronic Lymphocytic Leukemia. Cancers, 15(21), 5184. https://doi.org/10.3390/cancers15215184