
Palbociclib Combined with an Aromatase Inhibitor in Patients with Breast Cancer with Lung or Liver Metastases in US Clinical Practice

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design and Data Source
2.2. Patients
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patients
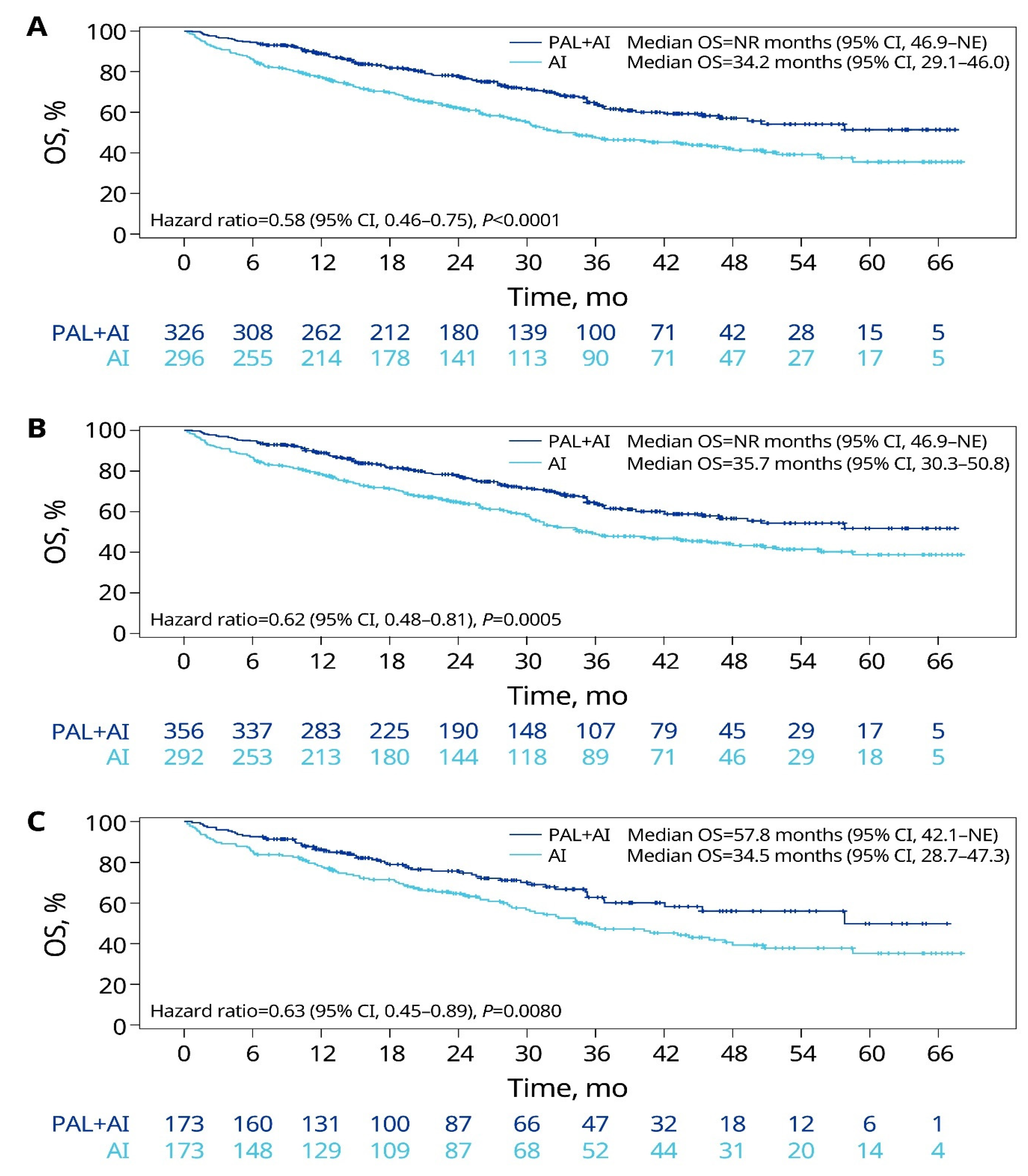
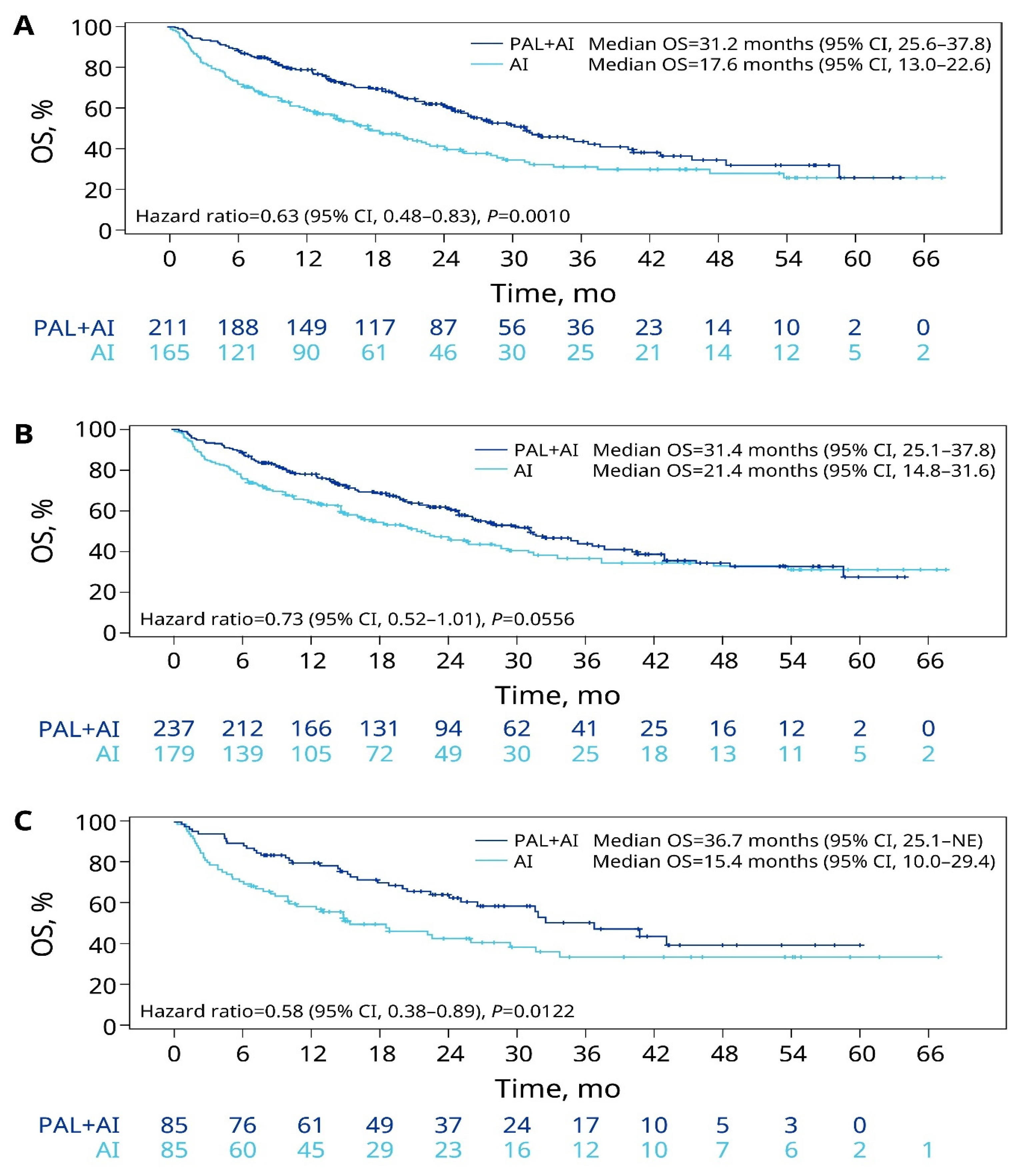
3.2. Overall Survival
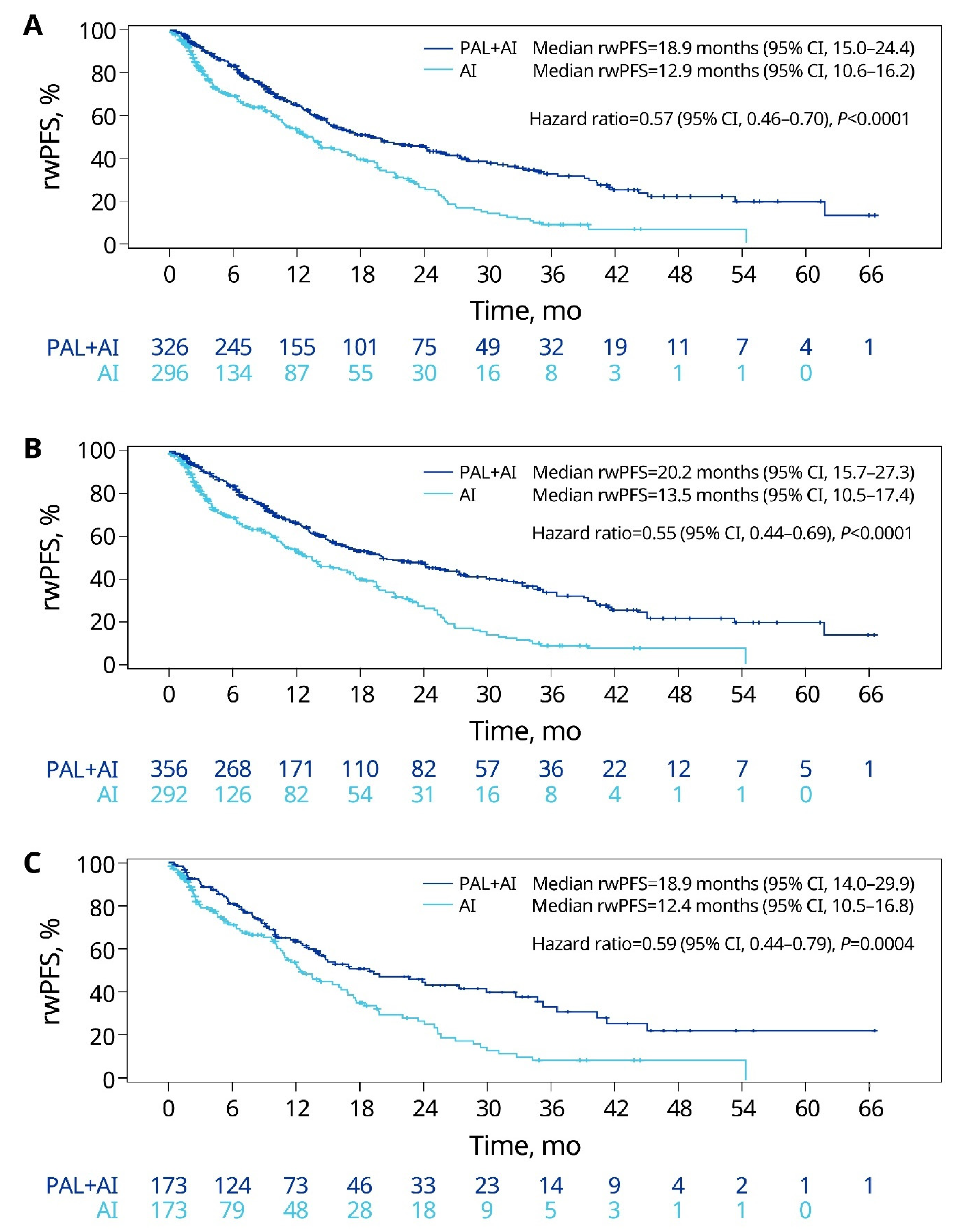
3.3. Real-World Progression-Free Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gallicchio, L.; Devasia, T.P.; Tonorezos, E.; Mollica, M.A.; Mariotto, A. Estimation of the numbers of individuals living with metastatic cancer in the United States. J. Natl. Cancer Inst. 2022, 114, 1476–1483. [Google Scholar] [CrossRef] [PubMed]
- NCI. SEER Cancer Stat Facts. 2022. Available online: https://seer.cancer.gov/statfacts/html/breast.html (accessed on 7 July 2023).
- Wu, Q.; Li, J.; Zhu, S.; Wu, J.; Chen, C.; Liu, Q.; Wei, W.; Zhang, Y.; Sun, S. Breast cancer subtypes predict the preferential site of distant metastases: A SEER based study. Oncotarget 2017, 8, 27990–27996. [Google Scholar] [CrossRef] [PubMed]
- Harb, W.A. Management of patients with hormone receptor-positive breast cancer with visceral disease: Challenges and treatment options. Cancer Manag. Res. 2015, 7, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Kolben, T.; Bardenhewer, M.; Kolben, T.M.; Rickerl, L.; Degenhardt, T.; Mahner, S.; Harbeck, N.; Wuerstlein, R. Metastatic breast cancer: Is there a differential therapy efficacy between visceral and non-visceral metastatic breast cancer? Breast Care 2020, 15, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Robertson, J.F.R.; Di Leo, A.; Johnston, S.; Chia, S.; Bliss, J.M.; Paridaens, R.J.; Lichfield, J.; Bradbury, I.; Campbell, C. Meta-analyses of visceral versus non-visceral metastatic hormone receptor-positive breast cancer treated by endocrine monotherapies. NPJ Breast Cancer 2021, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Yang, J.; Liu, Y.; You, H.; Dong, Y.; Lyu, J. Prognostic factors and survival outcomes according to tumor subtype in patients with breast cancer lung metastases. PeerJ 2019, 7, e8298. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.Y.; Gong, Y.; Ye, F.G.; Ling, H.; Hu, X. Incidence and prognostic factors of patients with synchronous liver metastases upon initial diagnosis of breast cancer: A population-based study. Cancer Manag. Res. 2018, 10, 5937–5950. [Google Scholar] [CrossRef]
- Liu, D.; Wu, J.; Lin, C.; Andriani, L.; Ding, S.; Shen, K.; Zhu, L. Breast subtypes and prognosis of breast cancer patients with initial bone metastasis: A population-based study. Front. Oncol. 2020, 10, 580112. [Google Scholar] [CrossRef]
- Rugo, H.S.; Finn, R.S.; Dieras, V.; Ettl, J.; Lipatov, O.; Joy, A.A.; Harbeck, N.; Castrellon, A.; Iyer, S.; Lu, D.R.; et al. Palbociclib plus letrozole as first-line therapy in estrogen receptor-positive/human epidermal growth factor receptor 2-negative advanced breast cancer with extended follow-up. Breast Cancer Res. Treat. 2019, 174, 719–729. [Google Scholar] [CrossRef]
- Goetz, M.P.; Toi, M.; Campone, M.; Sohn, J.; Paluch-Shimon, S.; Huober, J.; Park, I.H.; Tredan, O.; Chen, S.C.; Manso, L.; et al. MONARCH 3: Abemaciclib as initial therapy for advanced breast cancer. J. Clin. Oncol. 2017, 35, 3638–3646. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.S.; Sonke, G.S.; Hart, L.; Campone, M.; Petrakova, K.; Winer, E.P.; Janni, W.; et al. Overall survival with ribociclib plus letrozole in advanced breast cancer. N. Engl. J. Med. 2022, 386, 942–950. [Google Scholar] [CrossRef]
- Gerratana, L.; Fanotto, V.; Bonotto, M.; Bolzonello, S.; Minisini, A.M.; Fasola, G.; Puglisi, F. Pattern of metastasis and outcome in patients with breast cancer. Clin. Exp. Metastasis 2015, 32, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Mohan, S.C.; Wei, J.; Seki, E.; Liu, M.; Basho, R.; Giuliano, A.E.; Zhao, Y.; Cui, X. Breast cancer liver metastasis: Pathogenesis and clinical implications. Front. Oncol. 2022, 12, 1043771. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Zhu, Y.; Liu, X.; Liao, X.; He, J.; Niu, L. The clinicopathological features and survival outcomes of patients with different metastatic sites in stage IV breast cancer. BMC Cancer 2019, 19, 1091. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Senkus, E.; Costa, A.; Papadopoulos, E.; Aapro, M.; Andre, F.; Harbeck, N.; Aguilar Lopez, B.; Barrios, C.H.; Bergh, J.; et al. 4th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 4). Ann. Oncol. 2018, 29, 1634–1657. [Google Scholar] [CrossRef] [PubMed]
- McAndrew, N.P.; Finn, R.S. Clinical review on the management of hormone receptor-positive metastatic breast cancer. JCO Oncol. Pract. 2022, 18, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Beaver, J.A.; Amiri-Kordestani, L.; Charlab, R.; Chen, W.; Palmby, T.; Tilley, A.; Zirkelbach, J.F.; Yu, J.; Liu, Q.; Zhao, L.; et al. FDA approval: Palbociclib for the treatment of postmenopausal patients with estrogen receptor-positive, HER2-negative metastatic breast cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2015, 21, 4760–4766. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Rugo, H.S.; Dieras, V.C.; Harbeck, N.; Im, S.A.; Gelmon, K.; Walshe, J.M.; Martin, M.; Mac Gregor, M.C.; Bananis, E.; et al. Overall survival (OS) with first-line palbociclib plus letrozole (PAL+LET) versus placebo plus letrozole (PBO+LET) in women with estrogen receptor-positive/human epidermal growth factor receptor 2-negative advanced breast cancer (ER+/HER2− ABC): Analyses from PALOMA-2. J. Clin. Oncol. 2022, 40 (Suppl. S17), LBA1003. [Google Scholar] [CrossRef]
- Booth, C.M.; Karim, S.; Mackillop, W.J. Real-world data: Towards achieving the achievable in cancer care. Nat. Rev. Clin. Oncol. 2019, 16, 312–325. [Google Scholar] [CrossRef]
- Patt, D.; Liu, X.; Li, B.; McRoy, L.; Layman, R.M.; Brufsky, A. Real-world treatment patterns and outcomes of palbociclib plus an aromatase inhibitor for metastatic breast cancer: Flatiron database analysis. Clin. Breast Cancer 2022, 22, 601–610. [Google Scholar] [CrossRef]
- Goyal, R.K.; Chen, H.; Abughosh, S.M.; Holmes, H.M.; Candrilli, S.D.; Johnson, M.L. Overall survival associated with CDK4/6 inhibitors in patients with HR+/HER2- metastatic breast cancer in the United States: A SEER-Medicare population-based study. Cancer 2023, 129, 1051–1063. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, C.; Goyal, P.; Agarwal, A.; Tripathi, R.; Dodagoudar, C.; Baghmar, S.; Sharma, A.; Batra, U.; Talwar, V.; Goyal, S.; et al. Multicentric real world evidence with palbociclib in hormone positive HER2 negative metastatic breast cancer in Indian population. Sci. Rep. 2021, 11, 16236. [Google Scholar] [CrossRef] [PubMed]
- Brufsky, A.; Liu, X.; Li, B.; McRoy, L.; Layman, R.M. Real-world tumor response of palbociclib plus letrozole versus letrozole for metastatic breast cancer in US clinical practice. Target. Oncol. 2021, 16, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Brufsky, A.; Mitra, D.; Davis, K.L.; Nagar, S.P.; McRoy, L.; Cotter, M.J.; Stearns, V. Treatment patterns and outcomes associated with palbociclib plus letrozole for postmenopausal women with HR(+)/HER2(-) advanced breast cancer enrolled in an expanded access program. Clin. Breast Cancer 2019, 19, 317–325.e314. [Google Scholar] [CrossRef] [PubMed]
- DeMichele, A.; Cristofanilli, M.; Brufsky, A.; Liu, X.; Mardekian, J.; McRoy, L.; Layman, R.M.; Emir, B.; Torres, M.A.; Rugo, H.S.; et al. Comparative effectiveness of first-line palbociclib plus letrozole versus letrozole alone for HR+/HER2- metastatic breast cancer in US real-world clinical practice. Breast Cancer Res. 2021, 23, 37. [Google Scholar] [CrossRef] [PubMed]
- Rugo, H.S.; Brufsky, A.; Liu, X.; Li, B.; McRoy, L.; Chen, C.; Layman, R.M.; Cristofanilli, M.; Torres, M.A.; Curigliano, G.; et al. Real-world study of overall survival with palbociclib plus aromatase inhibitor in HR+/HER2- metastatic breast cancer. NPJ Breast Cancer 2022, 8, 114. [Google Scholar] [CrossRef] [PubMed]
- Mycock, K.; Hanson, K.A.; Taylor-Stokes, G.; Milligan, G.; Atkinson, C.; Mitra, D.; Preciado, S.; Law, E.H. Real-world treatment patterns and clinical outcomes associated with palbociclib combination therapy: A multinational, pooled analysis from the Ibrance Real world Insights Study. Clin. Ther. 2022, 44, 1588–1601. [Google Scholar] [CrossRef] [PubMed]
- Mycock, K.; Zhan, L.; Hart, K.; Taylor-Stokes, G.; Milligan, G.; Atkinson, C.; Mitra, D. Real-world treatment patterns and clinical outcomes in patients receiving palbociclib combinations for HR+/HER2- advanced/metastatic breast cancer in Japan: Results from the IRIS study. Cancer Treat. Res. Commun. 2022, 32, 100573. [Google Scholar] [CrossRef]
- Mycock, K.; Zhan, L.; Taylor-Stokes, G.; Milligan, G.; Mitra, D. Real-world palbociclib use in HR+/HER2- advanced breast cancer in Canada: The IRIS study. Curr. Oncol. 2021, 28, 678–688. [Google Scholar] [CrossRef]
- Waller, J.; Mitra, D.; Mycock, K.; Taylor-Stokes, G.; Milligan, G.; Zhan, L.; Iyer, S. Real-world treatment patterns and clinical outcomes in patients receiving palbociclib for hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced or metastatic breast cancer in Argentina: The IRIS study. J. Glob. Oncol. 2019, 5, JGO1800239. [Google Scholar] [CrossRef]
- Lin, J.; McRoy, L.; Fisher, M.D.; Hu, N.; Davis, C.; Mitra, D.; Walker, M.S. Treatment patterns and clinical outcomes of palbociclib-based therapy received in US community oncology practices. Future Oncol. 2021, 17, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N.; Bartlett, M.; Spurden, D.; Hooper, B.; Zhan, L.; Rosta, E.; Cameron, C.; Mitra, D.; Zhou, A. CDK4/6 inhibitors in HR+/HER2- advanced/metastatic breast cancer: A systematic literature review of real-world evidence studies. Future Oncol. 2021, 17, 2107–2122. [Google Scholar] [CrossRef] [PubMed]
- Brufsky, A.; Liu, X.; Li, B.; McRoy, L.; Layman, R.M. Real-world effectiveness of palbociclib plus letrozole vs letrozole alone for metastatic breast cancer with lung or liver metastases: Flatiron database analysis. Front. Oncol. 2022, 12, 865292. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.M.; Nordstrom, B.L.; McLaurin, K.K.; Dalvi, T.B.; McCutcheon, S.C.; Bennett, J.C.; Murphy, B.R.; Singhal, P.K.; McCrea, C.; Shinde, R.; et al. A real-world evidence study of CDK4/6 inhibitor treatment patterns and outcomes in metastatic breast cancer by germline BRCA mutation status. Oncol. Ther. 2021, 9, 575–589. [Google Scholar] [CrossRef] [PubMed]
- Huang Bartlett, C.; Mardekian, J.; Cotter, M.J.; Huang, X.; Zhang, Z.; Parrinello, C.M.; Bourla, A.B. Concordance of real-world versus conventional progression-free survival from a phase 3 trial of endocrine therapy as first-line treatment for metastatic breast cancer. PLoS ONE 2020, 15, e0227256. [Google Scholar] [CrossRef] [PubMed]
- Curtis, M.D.; Griffith, S.D.; Tucker, M.; Taylor, M.D.; Capra, W.B.; Carrigan, G.; Holzman, B.; Torres, A.Z.; You, P.; Arnieri, B.; et al. Development and validation of a high-quality composite real-world mortality endpoint. Health Serv. Res. 2018, 53, 4460–4476. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Gossai, A.; Monroe, S.; Nussbaum, N.C.; Parrinello, C.M. Validation analysis of a composite real-world mortality endpoint for patients with cancer in the United States. Health Serv. Res. 2021, 56, 1281–1287. [Google Scholar] [CrossRef]
- Xiao, W.; Zheng, S.; Liu, P.; Zou, Y.; Xie, X.; Yu, P.; Tang, H.; Xie, X. Risk factors and survival outcomes in patients with breast cancer and lung metastasis: A population-based study. Cancer Med. 2018, 7, 922–930. [Google Scholar] [CrossRef]
- Lin, S.; Mo, H.; Li, Y.; Guan, X.; Chen, Y.; Wang, Z.; Xu, B. Clinicopathological characteristics and survival outcomes in patients with synchronous lung metastases upon initial metastatic breast cancer diagnosis in Han population. BMC Cancer 2021, 21, 1330. [Google Scholar] [CrossRef]
- Wang, W.; Liu, J.; Chen, Y.; Xu, X.; Huo, L.; Wang, X.; Gu, J. An effective tool for predicting survival in breast cancer patients with de novo lung metastasis: Nomograms constructed based on SEER. Front. Surg. 2022, 9, 939132. [Google Scholar] [CrossRef]
- He, M.; Li, J.J.; Zuo, W.J.; Ji, L.; Jiang, Y.Z.; Hu, X.C.; Wang, Z.H.; Shao, Z.M. Metastatic breast cancer patients with lung or liver metastases should be distinguished before being treated with fulvestrant. Cancer Med. 2019, 8, 6212–6220. [Google Scholar] [CrossRef]
- Schettini, F.; Giudici, F.; Giuliano, M.; Cristofanilli, M.; Arpino, G.; Del Mastro, L.; Puglisi, F.; De Placido, S.; Paris, I.; De Placido, P.; et al. Overall suvival of CDK4/6-inhibitor-based treatments in clinically relevant subgroups of metastatic breast cancer: Systematic review and meta-analysis. J. Natl. Cancer Inst. 2020, 112, 1089–1097. [Google Scholar] [CrossRef]
- Gao, J.J.; Cheng, J.; Bloomquist, E.; Sanchez, J.; Wedam, S.B.; Singh, H.; Amiri-Kordestani, L.; Ibrahim, A.; Sridhara, R.; Goldberg, K.B.; et al. CDK4/6 inhibitor treatment for patients with hormone receptor-positive, HER2-negative, advanced or metastatic breast cancer: A US Food and Drug Administration pooled analysis. Lancet Oncol. 2020, 21, 250–260. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Unadjusted | sIPTW | PSM | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Palbociclib + AI (n = 326) | AI Alone (n = 296) | Std Diff | Palbociclib + AI (n = 356) | AI Alone (n = 292) | Std Diff | Palbociclib + AI (n = 173) | AI Alone (n = 173) | Std Diff | |
| Age at mBC diagnosis, years a | |||||||||
| Mean (SD) | 67.0 (10.5) | 71.0 (9.8) | −0.3941 | 68.6 (11.1) | 69.1 (10.1) | −0.0521 | 68.6 (10.3) | 69.9 (9.4) | −0.1408 |
| Median (IQR) | 68 (15) | 72 (16) | 69 (15) | 70 (16) | 69 (16) | 70 (15) | |||
| Female sex a n (%) | 323 (99.1) | 290 (98.0) | −0.0919 | 348 (97.9) | 288 (98.4) | 0.0378 | 172 (99.4) | 172 (99.4) | 0.0000 |
| Race a n (%) | |||||||||
| White | 218 (66.9) | 183 (61.8) | 0.1055 | 234 (65.9) | 192 (65.6) | 0.0050 | 113 (65.3) | 117 (67.6) | −0.0490 |
| Black | 26 (8.0) | 28 (9.5) | −0.0526 | 30 (8.3) | 24 (8.3) | 0.0012 | 14 (8.1) | 14 (8.1) | 0.0000 |
| Other | 82 (25.2) | 85 (28.7) | −0.0804 | 92 (25.8) | 76 (26.1) | −0.0062 | 46 (26.6) | 42 (24.3) | 0.0531 |
| Practice type | |||||||||
| Community | 302 (92.6) | 271 (91.6) | 0.0402 | 327 (92.1) | 269 (91.9) | 0.0047 | 158 (91.3) | 157 (90.8) | 0.0202 |
| Academic | 24 (7.4) | 25 (8.4) | 28 (7.9) | 24 (8.1) | 15 (8.7) | 16 (9.2) | |||
| mBC disease stage at initial diagnosis, n (%) | |||||||||
| I | 40 (12.3) | 37 (12.5) | −0.0070 | 45 (12.7) | 38 (12.9) | −0.0084 | 19 (11.0) | 23 (13.3) | −0.0708 |
| II | 87 (26.7) | 70 (23.6) | 0.0701 | 91 (25.5) | 76 (25.9) | −0.0072 | 50 (28.9) | 44 (25.4) | 0.0780 |
| III | 36 (11.0) | 50 (16.9) | −0.1693 | 49 (13.8) | 41 (13.9) | −0.0051 | 25 (14.5) | 18 (10.4) | 0.1229 |
| IV | 131 (40.2) | 101 (34.1) | 0.1257 | 130 (36.5) | 104 (35.8) | 0.0148 | 62 (35.8) | 65 (37.6) | −0.0360 |
| Not documented | 32 (9.8) | 38 (12.8) | −0.0955 | 41 (11.6) | 34 (11.5) | 0.0020 | 17 (9.8) | 23 (13.3) | −0.1086 |
| ECOG PS a n (%) | |||||||||
| 0 | 126 (38.7) | 62 (20.9) | 0.3945 | 106 (29.7) | 85 (29) | 0.0158 | 43 (24.9) | 41 (23.7) | 0.0270 |
| 1 | 78 (23.9) | 70 (23.6) | 0.0065 | 87 (24.5) | 70 (24.0) | 0.0119 | 48 (27.7) | 43 (24.9) | 0.0657 |
| 2, 3, or 4 | 37 (11.3) | 51 (17.2) | −0.1686 | 51 (14.3) | 43 (14.6) | −0.0081 | 27 (15.6) | 27 (15.6) | 0.0000 |
| Not documented | 85 (26.1) | 113 (38.2) | −0.2614 | 112 (31.4) | 95 (32.4) | −0.0202 | 55 (31.8) | 62 (35.8) | −0.0856 |
| Bone-only metastasis a,b n (%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Brain metastasis, n (%) | 15 (4.6) | 18 (6.1) | 0.0659 | 14 (3.9) | 23 (7.8) | 0.1686 | 6 (3.5) | 15 (8.7) | 0.2192 |
| Disease-free interval, years a,c n (%) | |||||||||
| De novo mBC | 131 (40.2) | 101 (34.1) | 0.1257 | 130 (36.5) | 104 (35.8) | 0.0148 | 62 (35.8) | 65 (37.6) | −0.0360 |
| ≤1 | 4 (1.2) | 8 (2.7) | −0.1065 | 4 (1.2) | 6 (2.2) | −0.0771 | 3 (1.7) | 2 (1.2) | 0.0485 |
| >1 to 5 | 40 (12.3) | 67 (22.6) | −0.2757 | 48 (13.4) | 69 (23.6) | −0.2627 | 25 (14.5) | 37 (21.4) | −0.1816 |
| >5 | 151 (46.3) | 120 (40.5) | 0.1168 | 174 (48.9) | 112 (38.5) | 0.2110 | 83 (48.0) | 69 (39.9) | 0.1636 |
| Not documented | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| NCI comorbidity index, mean (SD) | 0.28 (0.51) | 0.38 (0.53) | −0.1979 | 0.31 (0.59) | 0.35 (0.50) | −0.0798 | 0.34 (0.61) | 0.34 (0.50) | 0.0097 |
| Number of metastatic sites a,d n (%) | |||||||||
| 1 | 45 (13.8) | 64 (21.6) | −0.2059 | 62 (17.4) | 51 (17.4) | 0.0020 | 25 (14.5) | 23 (13.3) | 0.0334 |
| 2 | 105 (32.2) | 101 (34.1) | −0.0406 | 121 (34.0) | 100 (34.2) | −0.0030 | 64 (37.0) | 60 (34.7) | 0.0482 |
| 3 | 108 (33.1) | 87 (29.4) | 0.0807 | 107 (30.1) | 95 (32.4) | −0.0509 | 54 (31.2) | 59 (34.1) | −0.0617 |
| 4 | 40 (12.3) | 23 (7.8) | 0.1503 | 38 (10.8) | 24 (8.0) | 0.0943 | 17 (9.8) | 17 (9.8) | 0.0000 |
| ≥5 | 28 (8.6) | 21 (7.1) | 0.0556 | 27 (7.7) | 23 (8.0) | −0.0122 | 13 (7.5) | 14 (8.1) | −0.0216 |
| Median follow-up duration (IQR), months | 26.2 (24.8) | 23.0 (30.3) | 25.6 (25.4) | 23.6 (30.2) | 24.0 (24.5) | 24.2 (31.2) | |||
| Characteristic | Unadjusted | sIPTW | PSM | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Palbociclib + AI (n = 211) | AI Alone (n = 165) | Std Diff | Palbociclib + AI (n = 237) | AI Alone (n = 179) | Std Diff | Palbociclib + AI (n = 85) | AI Alone (n = 85) | Std Diff | |
| Age at mBC diagnosis, years a | |||||||||
| Mean (SD) | 62.9 (11.6) | 70.0 (9.7) | −0.6704 | 65.8 (12.3) | 66.6 (11.1) | −0.0686 | 67.0 (9.9) | 68.6 (9.3) | −0.1713 |
| Median (IQR) | 63 (16) | 71 (17) | 67 (18) | 67 (16) | 68 (13) | 69 (12) | |||
| Female sex a n (%) | 210 (99.5) | 163 (98.8) | −0.0808 | 235 (99.4) | 177 (99.3) | −0.0125 | 85 (100) | 85 (100) | 0.0000 |
| Race a n (%) | |||||||||
| White | 155 (73.5) | 107 (64.8) | 0.1873 | 168 (70.9) | 127 (70.9) | 0.0002 | 64 (75.3) | 66 (77.6) | −0.0555 |
| Black | 10 (4.7) | 17 (10.3) | −0.2121 | 12 (5.2) | 11 (6.1) | −0.0374 | 5 (5.9) | 3 (3.5) | 0.1113 |
| Other | 46 (21.8) | 41 (24.8) | −0.0721 | 56 (23.8) | 41 (23.0) | 0.0203 | 16 (18.8) | 16 (18.8) | 0.0000 |
| Practice type | −0.0016 | −0.0340 | 0.1718 | ||||||
| Community | 193 (91.5) | 151 (91.5) | 216 (91.3) | 165 (92.2) | 80 (94.1) | 76 (89.4) | |||
| Academic | 18 (8.5) | 14 (8.5) | 21 (8.74) | 14 (7.8) | 5 (5.9) | 9 (10.6) | |||
| mBC disease stage at initial diagnosis, n (%) | |||||||||
| I | 32 (15.2) | 27 (16.4) | −0.0329 | 37 (15.6) | 25 (14.2) | 0.0406 | 9 (10.6) | 11 (12.9) | −0.0731 |
| II | 60 (28.4) | 32 (19.4) | 0.2132 | 59 (25.0) | 45 (25.2) | −0.0035 | 19 (22.4) | 20 (23.5) | −0.0280 |
| III | 25 (11.8) | 26 (15.8) | −0.1135 | 32 (13.7) | 25 (14.0) | −0.0094 | 13 (15.3) | 13 (15.3) | 0.0000 |
| IV | 81 (38.4) | 60 (36.4) | 0.0419 | 87 (36.6) | 69 (38.4) | −0.0372 | 36 (42.4) | 38 (44.7) | −0.0475 |
| Not documented | 13 (6.2) | 20 (12.1) | −0.2079 | 22 (9.1) | 15 (8.3) | 0.0296 | 8 (9.4) | 3 (3.5) | 0.2408 |
| ECOG PS a n (%) | |||||||||
| 0 | 86 (40.8) | 41 (24.0) | 0.3438 | 80 (33.8) | 63 (35.1) | −0.0273 | 34 (40.0) | 27 (31.8) | 0.1723 |
| 1 | 49 (23.2) | 27 (16.4) | 0.1728 | 48 (20.1) | 33 (18.7) | 0.0346 | 14 (16.5) | 17 (20.0) | −0.0915 |
| 2, 3, or 4 | 30 (14.2) | 39 (23.6) | −0.2422 | 42 (17.9) | 34 (19.1) | −0.0323 | 14 (16.5) | 16 (18.8) | −0.0618 |
| Not documented | 46 (21.8) | 58 (35.2) | −0.2991 | 67 (28.2) | 48 (27.0) | 0.0265 | 23 (27.1) | 25 (29.4) | −0.0523 |
| Bone-only metastasis a,b n (%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Brain metastasis, n (%) | 11 (5.2) | 8 (4.8) | −0.0167 | 13 (5.4) | 16 (8.8) | 0.1324 | 5 (5.9) | 5 (5.9) | 0.0000 |
| Disease-free interval, years a,c n (%) | |||||||||
| De novo mBC | 81 (38.4) | 60 (36.4) | 0.0419 | 87 (36.6) | 69 (38.4) | −0.0372 | 36 (42.4) | 38 (44.7) | −0.0475 |
| ≤1 | 10 (4.7) | 5 (3.0) | 0.0885 | 9 (3.9) | 5 (2.6) | 0.0719 | 3 (3.5) | 1 (1.2) | 0.1557 |
| >1 to 5 | 34 (16.1) | 47 (28.5) | −0.3005 | 34 (14.6) | 54 (30.5) | −0.3885 | 7 (8.2) | 28 (32.9) | −0.6417 |
| >5 | 86 (40.8) | 52 (31.5) | 0.1933 | 106 (45.0) | 50 (28.1) | 0.3564 | 39 (45.9) | 18 (21.2) | 0.5422 |
| Not documented | 0 | 1 (0.6) | −0.1104 | 0 | 1 (0.4) | −0.0935 | 0 | 0 | 0 |
| NCI comorbidity index, mean (SD) | 0.25 (0.40) | 0.33 (0.50) | −0.1684 | 0.29 (0.46) | 0.28 (0.48) | 0.0200 | 0.29 (0.44) | 0.27 (0.38) | 0.0462 |
| Number of metastatic sites a,d n (%) | |||||||||
| 1 | 40 (19.0) | 29 (17.6) | 0.0358 | 44 (18.8) | 31 (17.6) | 0.0297 | 18 (21.2) | 12 (14.1) | 0.1860 |
| 2 | 69 (32.7) | 63 (38.2) | −0.1148 | 84 (35.3) | 65 (36.4) | −0.0223 | 29 (34.1) | 31 (36.5) | −0.0493 |
| 3 | 52 (24.6) | 41 (24.8) | −0.0047 | 54 (22.8) | 42 (23.3) | −0.0131 | 19 (22.4) | 24 (28.2) | −0.1356 |
| 4 | 26 (12.3) | 16 (9.7) | 0.0839 | 28 (11.7) | 16 (9.0) | 0.0900 | 9 (10.6) | 10 (11.8) | −0.0373 |
| ≥5 | 24 (11.4) | 16 (9.7) | 0.0547 | 27 (11.4) | 24 (13.7) | −0.0682 | 10 (11.8) | 8 (9.4) | 0.0765 |
| Median follow-up duration (IQR), months | 20.1 (21.4) | 13.1 (20.4) | 20.0 (21.4) | 14.8 (19.1) | 22.4 (21.5) | 13.0 (21.2) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brufsky, A.; Liu, X.; Li, B.; McRoy, L.; Chen, C.; Layman, R.M.; Rugo, H.S. Palbociclib Combined with an Aromatase Inhibitor in Patients with Breast Cancer with Lung or Liver Metastases in US Clinical Practice. Cancers 2023, 15, 5268. https://doi.org/10.3390/cancers15215268
Brufsky A, Liu X, Li B, McRoy L, Chen C, Layman RM, Rugo HS. Palbociclib Combined with an Aromatase Inhibitor in Patients with Breast Cancer with Lung or Liver Metastases in US Clinical Practice. Cancers. 2023; 15(21):5268. https://doi.org/10.3390/cancers15215268
Chicago/Turabian StyleBrufsky, Adam, Xianchen Liu, Benjamin Li, Lynn McRoy, Connie Chen, Rachel M. Layman, and Hope S. Rugo. 2023. "Palbociclib Combined with an Aromatase Inhibitor in Patients with Breast Cancer with Lung or Liver Metastases in US Clinical Practice" Cancers 15, no. 21: 5268. https://doi.org/10.3390/cancers15215268
APA StyleBrufsky, A., Liu, X., Li, B., McRoy, L., Chen, C., Layman, R. M., & Rugo, H. S. (2023). Palbociclib Combined with an Aromatase Inhibitor in Patients with Breast Cancer with Lung or Liver Metastases in US Clinical Practice. Cancers, 15(21), 5268. https://doi.org/10.3390/cancers15215268