


Classification of Pancreatic Ductal Adenocarcinoma Using MALDI Mass Spectrometry Imaging Combined with Neural Networks

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient and Sample Cohort
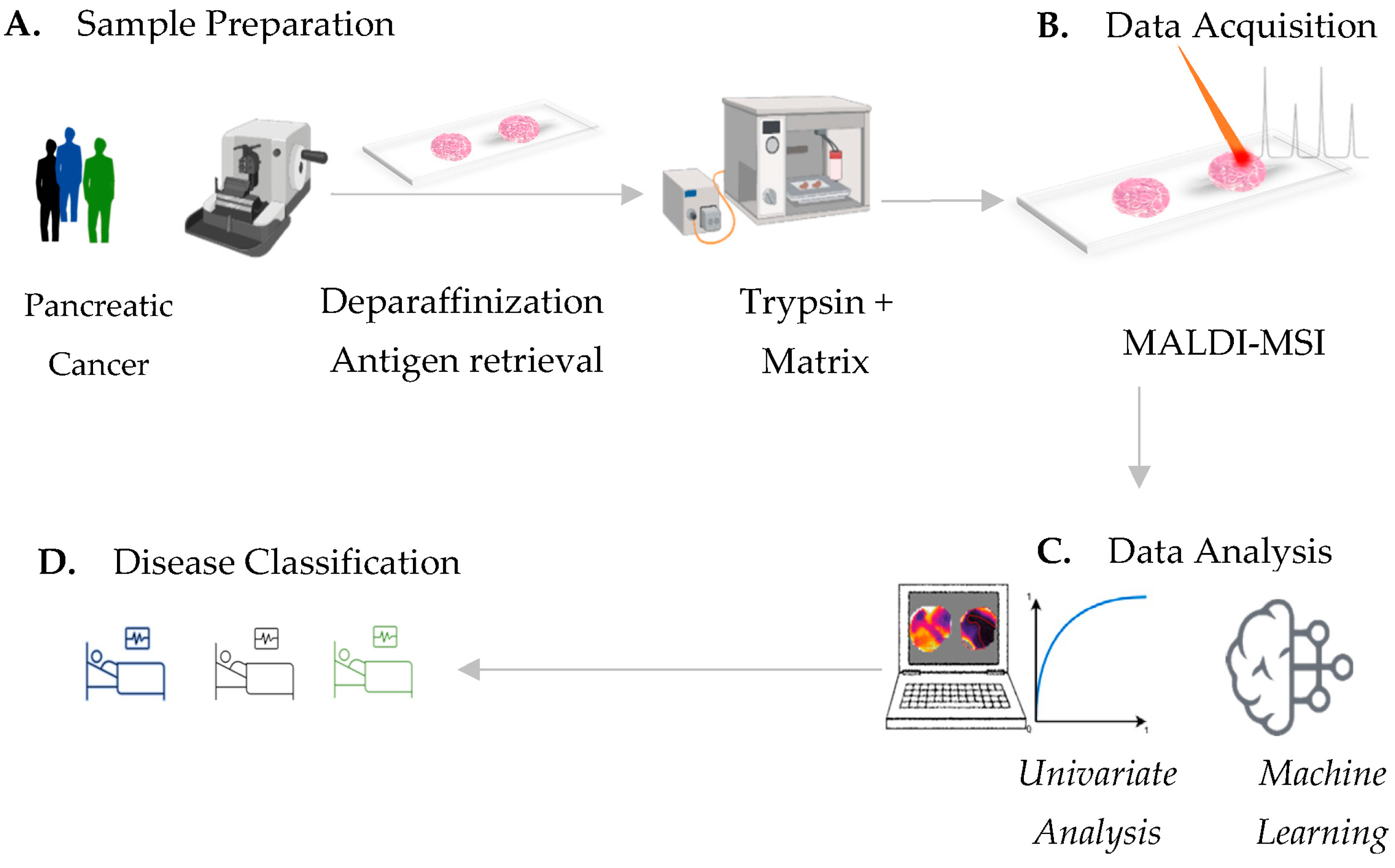
2.2. MALDI-MSI
2.3. Processing of MALDI-MSI Data
2.4. Univariate Statistical Analyses
2.5. Protein Identification by Electrospray Ionization Tandem Mass Spectrometry
2.6. Model Architectures for PDAC Classification
2.7. Dataset Design
2.8. Filtering of Noise Spectra
2.9. Classification
3. Results
3.1. Acquisition of MALDI-MSI Data
3.2. Discriminative m/z Values between Pancreatic Ductal Adenocarcinoma and Ampullary Carcinoma
3.3. Discriminative Proteins Identified from Pancreatic Carcinoma Tissues
3.4. Pancreatic-Ductal-Adenocarcinoma Classifier Identification by Using Neuronal-Network-Evaluation Strategies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kleeff, J.; Korc, M.; Apte, M.; La Vecchia, C.; Johnson, C.D.; Biankin, A.V.; Neale, R.E.; Tempero, M.; Tuveson, D.A.; Hruban, R.H.; et al. Pancreatic Cancer. Nat. Rev. Dis. Prim. 2016, 2, 16022. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [Green Version]
- Quante, A.S.; Ming, C.; Rottmann, M.; Engel, J.; Boeck, S.; Heinemann, V.; Westphalen, C.B.; Strauch, K. Projections of Cancer Incidence and Cancer-Related Deaths in Germany by 2020 and 2030. Cancer Med. 2016, 5, 2649–2656. [Google Scholar] [CrossRef]
- Gapstur, S.M.; Jacobs, E.J.; Deka, A.; McCullough, M.L.; Patel, A.V.; Thun, M.J. Association of Alcohol Intake with Pancreatic Cancer Mortality in Never Smokers. Arch. Intern. Med. 2011, 171, 444–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelucchi, C.; Galeone, C.; Polesel, J.; Manzari, M.; Zucchetto, A.; Talamini, R.; Franceschi, S.; Negri, E.; La Vecchia, C. Smoking and Body Mass Index and Survival in Pancreatic Cancer Patients. Pancreas 2014, 43, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.H.; Chou, J.F.; Ludwig, E.; O’Reilly, E.; Allen, P.J.; Jarnagin, W.R.; Bayuga, S.; Simon, J.; Gonen, M.; Reisacher, W.R.; et al. Allergies, Obesity, Other Risk Factors and Survival from Pancreatic Cancer. Int. J. Cancer 2010, 127, 2412–2419. [Google Scholar] [CrossRef] [PubMed]
- Delitto, D.; Zhang, D.; Han, S.; Black, B.S.; Knowlton, A.E.; Vlada, A.C.; Sarosi, G.A.; Behrns, K.E.; Thomas, R.M.; Lu, X.; et al. Nicotine Reduces Survival via Augmentation of Paracrine HGF–MET Signaling in the Pancreatic Cancer MicroenvironmentThe Effect of Nicotine on c-Met in Pancreatic Cancer. Clin. Cancer Res. 2016, 22, 1787–1799. [Google Scholar] [CrossRef] [Green Version]
- Uomo, G. Periampullary Carcinoma: Some Important News in Histopathology. JOP. J. Pancreas 2014, 15, 213–215. [Google Scholar]
- Baghmar, S.; Agrawal, N.; Kumar, G.; Bihari, C.; Patidar, Y.; Kumar, S.; Chattopadhyay, T.K.; Panda, D.; Arora, A.; Pamecha, V. Prognostic Factors and the Role of Adjuvant Treatment in Periampullary Carcinoma: A Single-Centre Experience of 95 Patients. J. Gastrointest. Cancer 2019, 50, 361–369. [Google Scholar] [CrossRef]
- Ferchichi, M.; Jouini, R.; Koubaa, W.; Khanchel, F.; Helal, I.; Hadad, D.; Bibani, N.; Chadli-Debbiche, A.; BenBrahim, E. Ampullary and Pancreatic Adenocarcinoma—A Comparative Study. J. Gastrointest. Oncol. 2019, 10, 270. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, R.S.; Bagci, P.; Basturk, O.; Reid, M.D.; Balci, S.; Knight, J.H.; Kong, S.Y.; Memis, B.; Jang, K.-T.; Ohike, N.; et al. Intrapancreatic Distal Common Bile Duct Carcinoma: Analysis, Staging Considerations, and Comparison with Pancreatic Ductal and Ampullary Adenocarcinomas. Mod. Pathol. 2016, 29, 1358–1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heijs, B.; Holst-Bernal, S.; de Graaff, M.A.; Briaire-de Bruijn, I.H.; Rodriguez-Girondo, M.; van de Sande, M.A.; Wuhrer, M.; McDonnell, L.A.; Bovée, J.V. Molecular Signatures of Tumor Progression in Myxoid Liposarcoma Identified by N-Glycan Mass Spectrometry Imaging. Lab. Investig. 2020, 100, 1252–1261. [Google Scholar] [CrossRef]
- Harris, A.; Roseborough, A.; Mor, R.; Yeung, K.K.-C.; Whitehead, S.N. Ganglioside Detection from Formalin-Fixed Human Brain Tissue Utilizing MALDI Imaging Mass Spectrometry. J. Am. Soc. Mass Spectrom. 2020, 31, 479–487. [Google Scholar] [CrossRef]
- Boyle, S.T.; Mittal, P.; Kaur, G.; Hoffmann, P.; Samuel, M.S.; Klingler-Hoffmann, M. Uncovering Tumor–Stroma Inter-Relationships Using MALDI Mass Spectrometry Imaging. J. Proteome Res. 2020, 19, 4093–4103. [Google Scholar] [CrossRef] [PubMed]
- Aichler, M.; Walch, A. MALDI Imaging Mass Spectrometry: Current Frontiers and Perspectives in Pathology Research and Practice. Lab. Investig. 2015, 95, 422–431. [Google Scholar] [CrossRef] [Green Version]
- Grüner, B.M.; Hahne, H.; Mazur, P.K.; Trajkovic-Arsic, M.; Maier, S.; Esposito, I.; Kalideris, E.; Michalski, C.W.; Kleeff, J.; Rauser, S.; et al. MALDI Imaging Mass Spectrometry for in Situ Proteomic Analysis of Preneoplastic Lesions in Pancreatic Cancer. PLoS ONE 2012, 7, e39424. [Google Scholar] [CrossRef]
- Prentice, B.M.; Hart, N.J.; Phillips, N.; Haliyur, R.; Judd, A.; Armandala, R.; Spraggins, J.M.; Lowe, C.L.; Boyd, K.L.; Stein, R.W.; et al. Imaging Mass Spectrometry Enables Molecular Profiling of Mouse and Human Pancreatic Tissue. Diabetologia 2019, 62, 1036–1047. [Google Scholar] [CrossRef] [Green Version]
- Bollwein, C.; Gonçalves, J.P.L.; Utpatel, K.; Weichert, W.; Schwamborn, K. MALDI Mass Spectrometry Imaging for the Distinction of Adenocarcinomas of the Pancreas and Biliary Tree. Molecules 2022, 27, 3464. [Google Scholar] [CrossRef]
- Casadonte, R.; Kriegsmann, M.; Perren, A.; Baretton, G.; Deininger, S.-O.; Kriegsmann, K.; Welsch, T.; Pilarsky, C.; Kriegsmann, J. Development of a Class Prediction Model to Discriminate Pancreatic Ductal Adenocarcinoma from Pancreatic Neuroendocrine Tumor by MALDI Mass Spectrometry Imaging. Proteomics Clin. Appl. 2019, 13, 1800046. [Google Scholar] [CrossRef]
- Chorowski, J.K.; Bahdanau, D.; Serdyuk, D.; Cho, K.; Bengio, Y. Attention-Based Models for Speech Recognition. Adv. Neural Inf. Process. Syst. 2015, 28, 577–585. [Google Scholar]
- Le’Clerc Arrastia, J.; Heilenkötter, N.; Otero Baguer, D.; Hauberg-Lotte, L.; Boskamp, T.; Hetzer, S.; Duschner, N.; Schaller, J.; Maass, P. Deeply Supervised UNet for Semantic Segmentation to Assist Dermatopathological Assessment of Basal Cell Carcinoma. J. Imaging 2021, 7, 71. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep Learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Verbeeck, N.; Caprioli, R.M.; Van de Plas, R. Unsupervised Machine Learning for Exploratory Data Analysis in Imaging Mass Spectrometry. Mass Spectrom. Rev. 2020, 39, 245–291. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Hundsdoerfer, P.; Schulte, J.H.; Astrahantseff, K.; Boral, S.; Schmelz, K.; Eggert, A.; Klein, O. Discovery of Spatial Peptide Signatures for Neuroblastoma Risk Assessment by MALDI Mass Spectrometry Imaging. Cancers 2021, 13, 3184. [Google Scholar] [CrossRef] [PubMed]
- Leuschner, J.; Schmidt, M.; Fernsel, P.; Lachmund, D.; Boskamp, T.; Maass, P. Supervised Non-Negative Matrix Factorization Methods for MALDI Imaging Applications. Bioinformatics 2019, 35, 1940–1947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassuhn, W.; Klein, O.; Darb-Esfahani, S.; Lammert, H.; Handzik, S.; Taube, E.T.; Schmitt, W.D.; Keunecke, C.; Horst, D.; Dreher, F.; et al. Classification of Molecular Subtypes of High-Grade Serous Ovarian Cancer by MALDI-Imaging. Cancers 2021, 13, 1512. [Google Scholar] [CrossRef] [PubMed]
- Alexandrov, T.; Becker, M.; Deininger, S.; Ernst, G.; Wehder, L.; Grasmair, M.; Von Eggeling, F.; Thiele, H.; Maass, P. Spatial Segmentation of Imaging Mass Spectrometry Data with Edge-Preserving Image Denoising and Clustering. J. Proteome Res. 2010, 9, 6535–6546. [Google Scholar] [CrossRef] [Green Version]
- Alexandrov, T.; Becker, M.; Guntinas-Lichius, O.; Ernst, G.; von Eggeling, F. MALDI-Imaging Segmentation Is a Powerful Tool for Spatial Functional Proteomic Analysis of Human Larynx Carcinoma. J. Cancer Res. Clin. Oncol. 2013, 139, 85–95. [Google Scholar] [CrossRef]
- Klein, O.; Strohschein, K.; Nebrich, G.; Oetjen, J.; Trede, D.; Thiele, H.; Alexandrov, T.; Giavalisco, P.; Duda, G.N.; von Roth, P.; et al. MALDI Imaging Mass Spectrometry: Discrimination of Pathophysiological Regions in Traumatized Skeletal Muscle by Characteristic Peptide Signatures. Proteomics 2014, 14, 2249–2260. [Google Scholar] [CrossRef]
- Vaswani, A.; Shazeer, N.; Parmar, N.; Uszkoreit, J.; Jones, L.; Gomez, A.N.; Kaiser, L.; Polosukhin, I. Attention Is All You Need. Adv. Neural Inf. Process. Syst. 2017, 30, 5998–6008. [Google Scholar]
- Shin, S.J.; Smith, J.A.; Rezniczek, G.A.; Pan, S.; Chen, R.; Brentnall, T.A.; Wiche, G.; Kelly, K.A. Unexpected Gain of Function for the Scaffolding Protein Plectin Due to Mislocalization in Pancreatic Cancer. Proc. Natl. Acad. Sci. USA 2013, 110, 19414–19419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bausch, D.; Thomas, S.; Mino-Kenudson, M.; Fernández-del, C.C.; Bauer, T.W.; Williams, M.; Warshaw, A.L.; Thayer, S.P.; Kelly, K.A. Plectin-1 as a Novel Biomarker for Pancreatic CancerPlectin-1 as a Novel Biomarker for Pancreatic Cancer. Clin. Cancer Res. 2011, 17, 302–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Liu, X.; Huang, R.; Liu, X.; Liang, Z.; Liu, T. Upregulation of Nucleoprotein AHNAK Is Associated with Poor Outcome of Pancreatic Ductal Adenocarcinoma Prognosis via Mediating Epithelial-Mesenchymal Transition. J. Cancer 2019, 10, 3860. [Google Scholar] [CrossRef] [Green Version]
- Svoronos, C.; Tsoulfas, G.; Souvatzi, M.; Chatzitheoklitos, E. Prognostic Value of COL6A3 in Pancreatic Adenocarcinoma. Ann. Hepato-Biliary-Pancreat. Surg. 2020, 24, 52. [Google Scholar] [CrossRef]
- Kang, C.Y.; Wang, J.; Axell-House, D.; Soni, P.; Chu, M.-L.; Chipitsyna, G.; Sarosiek, K.; Sendecki, J.; Hyslop, T.; Al-Zoubi, M.; et al. Clinical Significance of Serum COL6A3 in Pancreatic Ductal Adenocarcinoma. J. Gastrointest. Surg. 2014, 18, 7–15. [Google Scholar] [CrossRef]
- McCombie, G.; Staab, D.; Stoeckli, M.; Knochenmuss, R. Spatial and Spectral Correlations in MALDI Mass Spectrometry Images by Clustering and Multivariate Analysis. Anal. Chem. 2005, 77, 6118–6124. [Google Scholar] [CrossRef] [PubMed]
- Deininger, S.-O.; Becker, M.; Suckau, D. Tutorial: Multivariate Statistical Treatment of Imaging Data for Clinical Biomarker Discovery. Mass Spectrom. Imaging 2010, 656, 385–403. [Google Scholar]
- Jones, E.A.; van Remoortere, A.; van Zeijl, R.J.; Hogendoorn, P.C.; Bovée, J.V.; Deelder, A.M.; McDonnell, L.A. Multiple Statistical Analysis Techniques Corroborate Intratumor Heterogeneity in Imaging Mass Spectrometry Datasets of Myxofibrosarcoma. PLoS ONE 2011, 6, e24913. [Google Scholar] [CrossRef] [Green Version]
- Veselkov, K.A.; Mirnezami, R.; Strittmatter, N.; Goldin, R.D.; Kinross, J.; Speller, A.V.; Abramov, T.; Jones, E.A.; Darzi, A.; Holmes, E.; et al. Chemo-Informatic Strategy for Imaging Mass Spectrometry-Based Hyperspectral Profiling of Lipid Signatures in Colorectal Cancer. Proc. Natl. Acad. Sci. USA 2014, 111, 1216–1221. [Google Scholar] [CrossRef] [Green Version]
- He, H.; Garcia, E.A. Learning from Imbalanced Data. IEEE Trans. Knowl. Data Eng. 2009, 21, 1263–1284. [Google Scholar]
- Bergstra, J.; Bengio, Y. Random Search for Hyper-Parameter Optimization. J. Mach. Learn. Res. 2012, 13, 281–305. [Google Scholar]
- Dilillo, M.; Ait-Belkacem, R.; Esteve, C.; Pellegrini, D.; Nicolardi, S.; Costa, M.; Vannini, E.; De Graaf, E.; Caleo, M.; McDonnell, L. Ultra-High Mass Resolution MALDI Imaging Mass Spectrometry of Proteins and Metabolites in a Mouse Model of Glioblastoma. Sci. Rep. 2017, 7, 603. [Google Scholar] [CrossRef] [Green Version]
- Mezger, S.T.; Mingels, A.M.; Bekers, O.; Heeren, R.M.; Cillero-Pastor, B. Mass Spectrometry Spatial-Omics on a Single Conductive Slide. Anal. Chem. 2021, 93, 2527–2533. [Google Scholar] [CrossRef]
- Spraggins, J.M.; Rizzo, D.G.; Moore, J.L.; Noto, M.J.; Skaar, E.P.; Caprioli, R.M. Next-Generation Technologies for Spatial Proteomics: Integrating Ultra-High Speed MALDI-TOF and High Mass Resolution MALDI FTICR Imaging Mass Spectrometry for Protein Analysis. Proteomics 2016, 16, 1678–1689. [Google Scholar] [CrossRef] [Green Version]
- Mittal, P.; Condina, M.R.; Klingler-Hoffmann, M.; Kaur, G.; Oehler, M.K.; Sieber, O.M.; Palmieri, M.; Kommoss, S.; Brucker, S.; McDonnell, M.D.; et al. Cancer Tissue Classification Using Supervised Machine Learning Applied to MALDI Mass Spectrometry Imaging. Cancers 2021, 13, 5388. [Google Scholar] [CrossRef]
- Mascini, N.E.; Teunissen, J.; Noorlag, R.; Willems, S.M.; Heeren, R.M. Tumor Classification with MALDI-MSI Data of Tissue Microarrays: A Case Study. Methods 2018, 151, 21–27. [Google Scholar] [CrossRef]
- Behrmann, J.; Etmann, C.; Boskamp, T.; Casadonte, R.; Kriegsmann, J.; Maaβ, P. Deep Learning for Tumor Classification in Imaging Mass Spectrometry. Bioinformatics 2018, 34, 1215–1223. [Google Scholar] [CrossRef] [Green Version]
- Klein, O.; Kanter, F.; Kulbe, H.; Jank, P.; Denkert, C.; Nebrich, G.; Schmitt, W.D.; Wu, Z.; Kunze, C.A.; Sehouli, J.; et al. MALDI-Imaging for Classification of Epithelial Ovarian Cancer Histotypes from a Tissue Microarray Using Machine Learning Methods. Proteomics Clin. Appl. 2019, 13, 1700181. [Google Scholar] [CrossRef] [Green Version]
- Kulbe, H.; Klein, O.; Wu, Z.; Taube, E.T.; Kassuhn, W.; Horst, D.; Darb-Esfahani, S.; Jank, P.; Abobaker, S.; Ringel, F.; et al. Discovery of Prognostic Markers for Early-Stage High-Grade Serous Ovarian Cancer by MALDI-Imaging. Cancers 2020, 12, 2000. [Google Scholar] [CrossRef]
- Abdelmoula, W.M.; Lopez, B.G.-C.; Randall, E.C.; Kapur, T.; Sarkaria, J.N.; White, F.M.; Agar, J.N.; Wells, W.M.; Agar, N.Y. Peak Learning of Mass Spectrometry Imaging Data Using Artificial Neural Networks. Nat. Commun. 2021, 12, 5544. [Google Scholar] [CrossRef] [PubMed]
- Klein, O.; Fogt, F.; Hollerbach, S.; Nebrich, G.; Boskamp, T.; Wellmann, A. Classification of Inflammatory Bowel Disease from Formalin-Fixed, Paraffin-Embedded Tissue Biopsies via Imaging Mass Spectrometry. Proteomics Clin. Appl. 2020, 14, 1900131. [Google Scholar] [CrossRef] [PubMed]
- Boskamp, T.; Lachmund, D.; Casadonte, R.; Hauberg-Lotte, L.; Kobarg, J.H.; Kriegsmann, J.; Maass, P. Using the Chemical Noise Background in MALDI Mass Spectrometry Imaging for Mass Alignment and Calibration. Anal. Chem. 2019, 92, 1301–1308. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet Large Scale Visual Recognition Challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group | PDAC | AC | Other PC | |
|---|---|---|---|---|
| Total n | 446 | 260 | 103 | 83 |
| Age at Surgery | ||||
| >60 years | 311 (70%) | 187 (72%) | 74 (72%) | 50 (60%) |
| <60 years | 135 (30%) | 73 (28%) | 29 (28%) | 33 (40%) |
| Sex | ||||
| female | 211 (47%) | 118 (45%) | 45 (44%) | 48 (58%) |
| male | 235 (53%) | 142 (55%) | 58 (56%) | 35 (42%) |
| Regional Lymph Nodes | ||||
| pN0: No regional lymph-node-metastasis | 115 (26%) | 64 (25%) | 50 (49%) | 1 (1%) |
| pN1: Regional lymph-node-metastasis | 241 (54%) | 180 (69%) | 51 (50%) | 10 (12%) |
| pNx: Cannot be assessed | 90(20%) | 16 (6%) | 2(2%) | 72 (87%) |
| Histologic Grade | ||||
| G1: Well differentiated | 4 (1%) | 3 (1%) | 1(1%) | - |
| G2: Moderately differentiated | 287 (64%) | 181 (70%) | 96 (93%) | 10 (12%) |
| G3: Poorly differentiated | 72 (16%) | 65 (25%) | 6 (6%) | 1 (1%) |
| not assessed | 94 (21%) | 11 (4%) | - | 72 (87%) |
| Model | Kernel Size | Channel | Learning Rate | Batch Size | Heads | Pooling Size |
|---|---|---|---|---|---|---|
| Residual | (200, 100) | (16, 8) | 1 × 10−5 | 100 | - | - |
| Transformer 1 | (256, 256) | (16, 8) | 1 × 10−4 | 100 | 2 | 4 |
| Transformer 2 | (512, 512) | (16, 8) | 1 × 10−4 | 500 | 2 | 8 |
| Training | Validation | Testing | |
|---|---|---|---|
| Dataset 1 | 267 (51.1%) cores | 100 (19.2%) cores | 100 (19.2%) cores |
| 14,384 (50.3%) spectra | 5578 (19.5%) spectra | 8627 (30.2%) spectra | |
| Dataset 2 | 270 (51.7%) cores | 97 (18.6%) cores | 155 (29.7%) cores |
| 14,323 (50.2%) spectra | 5611 (19.7%) spectra | 8619 (30.1%) spectra | |
| Dataset 3 | 254 (48.7%) cores | 102 (19.5%) cores | 166 (31.8%) cores |
| 14,297 (50.1%) spectra | 5577 (19.5%) spectra | 8679 (30.4%) spectra |
| MALDI IMS m/z Value | ROC [AUC] AC/PDAC | LC-MS/MS [Mr+H+ cal.] | Deviation [Da] | MOWSE Score | Sequence | Protein | Gen Symbol |
|---|---|---|---|---|---|---|---|
| 1459.7 | 0.721 | 1459.8631 | −0.16 | 38.2 | K.IGDLHPQIVNLLK.S | Collagen alpha-3(VI) chain | COL6A3 |
| 1586.8 | 0.700 | 1586.9265 | −0.16 | 47.7 | R.LQPVLQPLPSPGVGGK.R | ||
| 1267.7 | 0.715 | 1267.6529 | 0.01 | 53 | K.AEGPEVDVNLPK.A | Neuroblast differentiation-associated protein AHNAK | AHNAK |
| 1655.8 | 0.719 | 1654.8170 | 0.96 | 107.4 | K.VDIEAPDVSLEGPEGK.L | ||
| 1461.7 | 0.710 | 1461.7366 | −0.04 | 78.1 | R.SQVMDEATALQLR.E | Plectin | PLEC |
| 1479.8 | 0.714 | 1479.7914 | −0.03 | 58.9 | R.SLQEEHVAVAQLR.E | ||
| 2115.1 | 0.701 | 2115.0175 | 0.08 | 69.6 | R.AGTLSITEFADMLSGNAGGFR.S |
| Model | Split | Accuracy (Spec) | Accuracy (Sample) |
|---|---|---|---|
| Residual | I | 0.86 | 0.86 |
| II | 0.76 | 0.77 | |
| III | 0.77 | 0.76 | |
| 0.80 | 0.80 | ||
| Transformer 1 | I | 0.85 | 0.86 |
| II | 0.78 | 0.77 | |
| III | 0.77 | 0.77 | |
| 0.80 | 0.80 | ||
| Transformer 2 | I | 0.83 | 0.84 |
| II | 0.77 | 0.76 | |
| III | 0.78 | 0.79 | |
| 0.80 | 0.80 |
| Model | Class | Spot/Patient | Sensitivity | Specificity |
|---|---|---|---|---|
| Residual | PDAC | Spot | 0.79 | 0.90 |
| Non-PDAC | Spot | 0.90 | 0.79 | |
| PDAC | Patient | 0.82 | 0.90 | |
| Non-PDAC | Patient | 0.90 | 0.82 | |
| Transformer 1 | PDAC | Spot | 0.81 | 0.89 |
| Non-PDAC | Spot | 0.89 | 0.81 | |
| PDAC | Patient | 0.83 | 0.88 | |
| Non-PDAC | Patient | 0.88 | 0.83 | |
| Transformer 2 | PDAC | Spot | 0.76 | 0.87 |
| Non-PDAC | Spot | 0.87 | 0.76 | |
| PDAC | Patient | 0.78 | 0.89 | |
| Non-PDAC | Patient | 0.89 | 0.78 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanter, F.; Lellmann, J.; Thiele, H.; Kalloger, S.; Schaeffer, D.F.; Wellmann, A.; Klein, O. Classification of Pancreatic Ductal Adenocarcinoma Using MALDI Mass Spectrometry Imaging Combined with Neural Networks. Cancers 2023, 15, 686. https://doi.org/10.3390/cancers15030686
Kanter F, Lellmann J, Thiele H, Kalloger S, Schaeffer DF, Wellmann A, Klein O. Classification of Pancreatic Ductal Adenocarcinoma Using MALDI Mass Spectrometry Imaging Combined with Neural Networks. Cancers. 2023; 15(3):686. https://doi.org/10.3390/cancers15030686
Chicago/Turabian StyleKanter, Frederic, Jan Lellmann, Herbert Thiele, Steve Kalloger, David F. Schaeffer, Axel Wellmann, and Oliver Klein. 2023. "Classification of Pancreatic Ductal Adenocarcinoma Using MALDI Mass Spectrometry Imaging Combined with Neural Networks" Cancers 15, no. 3: 686. https://doi.org/10.3390/cancers15030686
APA StyleKanter, F., Lellmann, J., Thiele, H., Kalloger, S., Schaeffer, D. F., Wellmann, A., & Klein, O. (2023). Classification of Pancreatic Ductal Adenocarcinoma Using MALDI Mass Spectrometry Imaging Combined with Neural Networks. Cancers, 15(3), 686. https://doi.org/10.3390/cancers15030686