

Exploratory Assessment of Nutritional Evaluation Tools as Predictors of Complications and Sarcopenia in Patients with Colorectal Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Body Composition
2.3. Nutritional Status and Muscle Quality
2.4. Statistical Analysis
3. Results
3.1. General Characterization of the Population Study
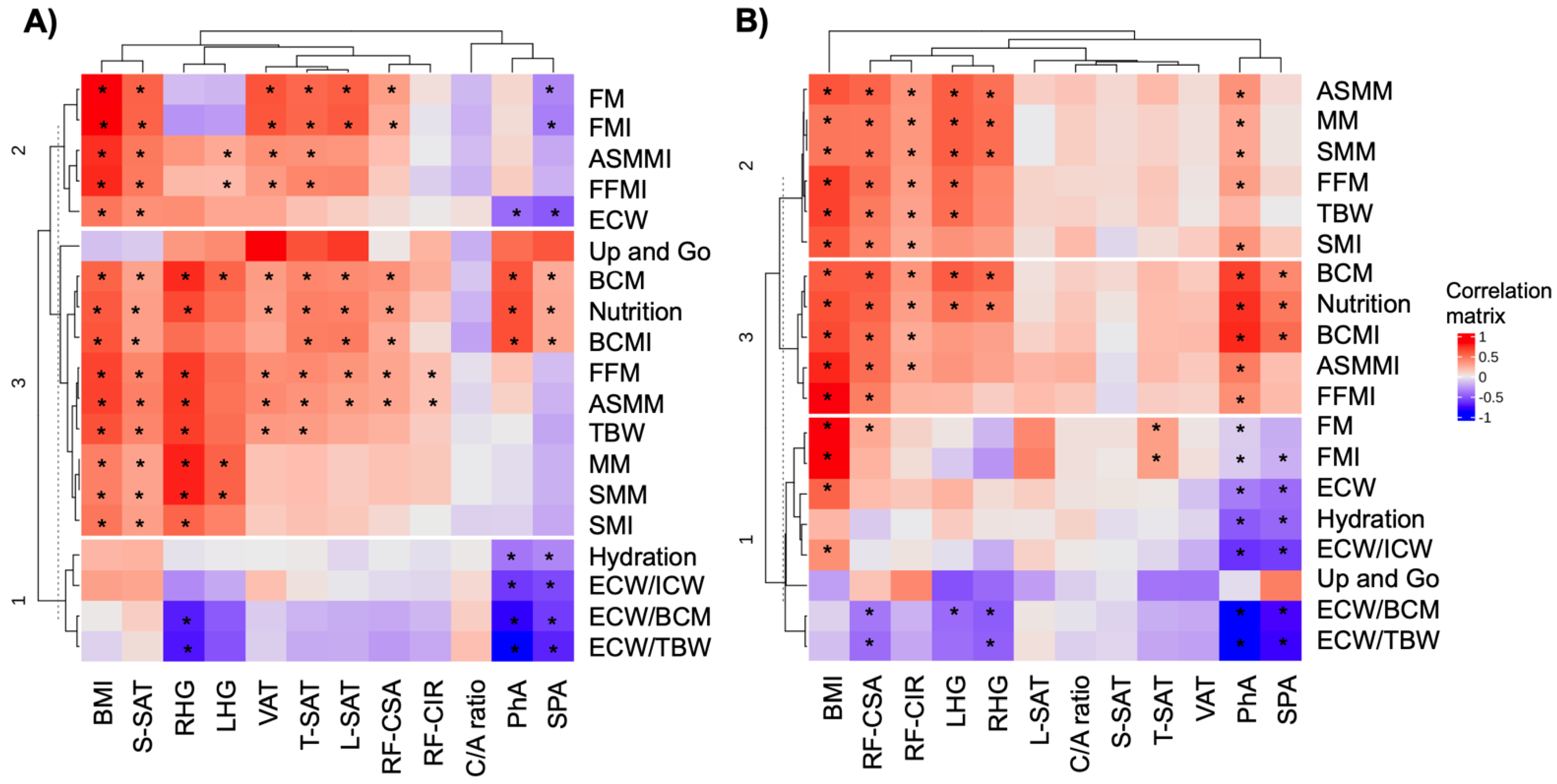
3.2. Correlation Analysis between Nutritional Assessment Methods and Nutritional Status
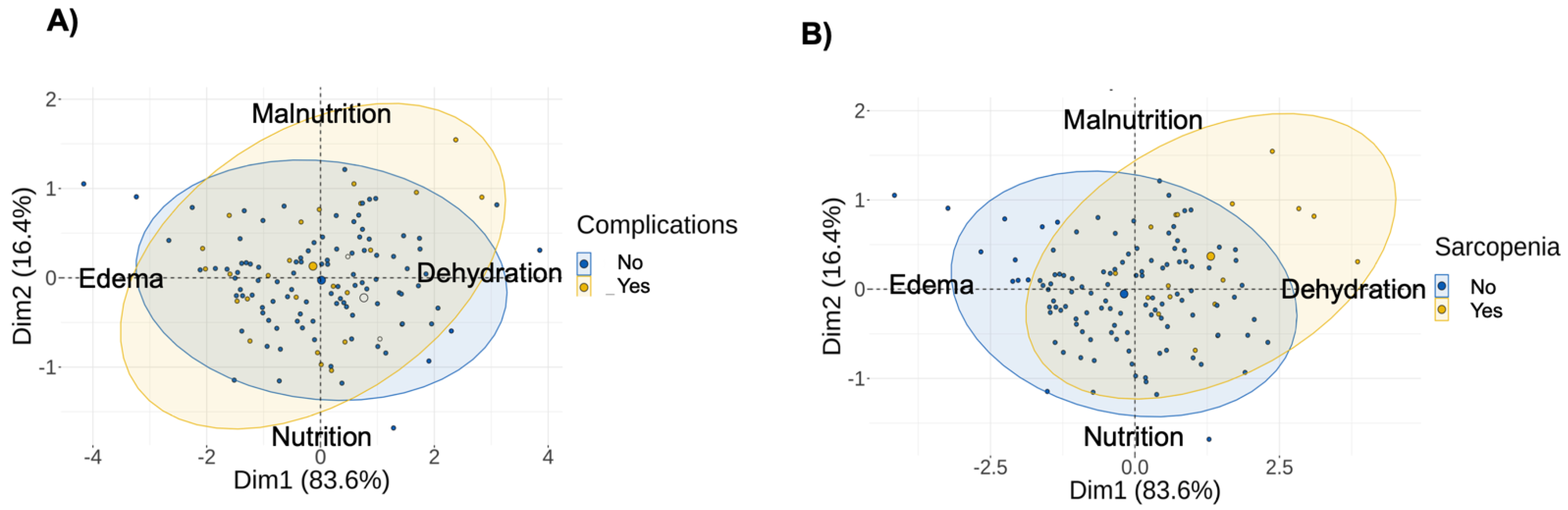
3.3. Correlation between Nutritional Assessment Methods and Cancer Outcomes
3.4. PhA as a Prognostic Predictor of Complications and Sarcopenia in Colorectal Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Agency for Research on Cancer (IARC). GLOBOCAN 2018: Latest Global Cancer Data. Available online: https://www.iarc.who.int/infographics/globocan-2018-latest-global-cancer-data/ (accessed on 10 September 2022).
- Kanth, P.; Inadomi, J. Screening and prevention of colorectal cancer. BMJ 2021, 374, n1855. [Google Scholar] [CrossRef] [PubMed]
- Phillips, B.E.; Smith, K.; Liptrot, S.; Atherton, P.J.; Varadhan, K.; Rennie, M.J.; Larvin, M.; Lund, J.N.; Williams, J.P. Effect of colon cancer and surgical resection on skeletal muscle mitochondrial enzyme activity in colon cancer patients: A pilot study. J. Cachexia Sarcopenia Muscle 2013, 4, 71. [Google Scholar] [CrossRef] [PubMed]
- Kocarnik, J.M.; Hua, X.; Hardikar, S.; Robinson, J.; Lindor, N.M.; Win, A.K.; Hopper, J.L.; Figueiredo, J.C.; Potter, J.D.; Campbell, P.T.; et al. Long-term weight loss after colorectal cancer diagnosis is associated with lower survival: The Colon Cancer Family Registry. Cancer 2017, 123, 4701. [Google Scholar] [CrossRef] [Green Version]
- Bossi, P.; Delrio, P.; Mascheroni, A.; Zanetti, M. The Spectrum of Malnutrition/Cachexia/Sarcopenia in Oncology According to Different Cancer Types and Settings: A Narrative Review. Nutrients 2021, 13, 1980. [Google Scholar] [CrossRef] [PubMed]
- Bhuachalla, E.N.; Daly, L.; Cushen, S.; O’Mahony, D.; Bambury, R.; O’Reilly, S.; Mceneaney, P.; Twomey, M.; Ryan, A.; Power, D.G. Cancer-associated malnutrition: Prevalence of cachexia, sarcopenia and impact on health-related quality of life and survival in a cohort of Irish ambulatory patients receiving chemotherapy. Am. Soc. Clin. Oncol. 2016, 34 (Suppl. 15), 10137. [Google Scholar] [CrossRef]
- Henriques, V.T.; Martinez, E.Z.; Divino-Filho, J.C.; Pecoits-Filho, R.; da Costa, J.A.C. Increase in BMI over time is associated with fluid overload and signs of wasting in incident peritoneal dialysis patients. J. Ren. Nutr. 2013, 23, e51–e57. [Google Scholar] [CrossRef]
- García, C.G.; Almeida, J.M.G.; Aguilar, I.M.V.; Castañeda, V.B.; Guerrero, D.B. Morphofunctional assessment of patient’s nutritional status: A global approach. Nutr. Hosp. 2021, 38, 592–600. [Google Scholar] [CrossRef]
- Fernández-Jiménez, R.; Dalla-Rovere, L.; García-Olivares, M.; Abuín-Fernández, J.; Sánchez-Torralvo, F.J.; Doulatram-Gamgaram, V.K.; Hernández-Sanchez, A.M.; García-Almeida, J.M. Phase Angle and Handgrip Strength as a Predictor of Disease-Related Malnutrition in Admitted Patients: 12-Month Mortality. Nutrients 2022, 14, 1851. [Google Scholar] [CrossRef]
- Cornejo-Pareja, I.; Vegas-Aguilar, I.M.; García-Almeida, J.M.; Bellido-Guerrero, D.; Talluri, A.; Lukaski, H.; Tinahones, F.J. Phase angle and standardized phase angle from bioelectrical impedance measurements as a prognostic factor for mortality at 90 days in patients with COVID-19: A longitudinal cohort study. Clin. Nutr. 2021, 41, 3106–3114. [Google Scholar] [CrossRef]
- Pereira, M.M.E.; Queiroz, M.D.S.C.; de Albuquerque, N.M.C.; Rodrigues, J.; Wiegert, E.V.M.; Calixto-Lima, L.; de Oliveira, L.C. The Prognostic Role of Phase Angle in Advanced Cancer Patients: A Systematic Review. Nutr. Clin. Pract. 2018, 33, 813–824. [Google Scholar] [CrossRef]
- Arab, A.; Karimi, E.; Vingrys, K.; Shirani, F. Is phase angle a valuable prognostic tool in cancer patients’ survival? A systematic review and meta-analysis of available literature. Clin. Nutr. 2021, 40, 3182–3190. [Google Scholar] [CrossRef] [PubMed]
- Ji, W.; Liu, X.; Zheng, K.; Yang, H.; Cui, J.; Li, W. Correlation of phase angle with sarcopenia and its diagnostic value in elderly men with cancer. Nutrition 2021, 84, 111110. [Google Scholar] [CrossRef]
- Souza, N.C.; Avesani, C.M.; Prado, C.M.; Martucci, R.B.; Rodrigues, V.D.; de Pinho, N.B.; Heymsfield, S.B.; Gonzalez, M.C. Phase angle as a marker for muscle abnormalities and function in patients with colorectal cancer. Clin. Nutr. 2021, 40, 4799–4806. [Google Scholar] [CrossRef] [PubMed]
- Valentino, N.P.; Gomes, T.L.; Barreto, C.S.; Borges, T.C.; Soares, J.D.; Pichard, C.; Laviano, A.; Pimentel, G.D. Low phase angle is associated with the risk for sarcopenia in unselected patients with cancer: Effects of hydration. Nutrition 2021, 84, 111122. [Google Scholar] [CrossRef] [PubMed]
- Maurício, S.F.; Xiao, J.; Prado, C.M.; Gonzalez, M.C.; Correia, M.I.T.D. Different nutritional assessment tools as predictors of postoperative complications in patients undergoing colorectal cancer resection. Clin. Nutr. 2018, 37, 1505–1511. [Google Scholar] [CrossRef]
- Albores, J.M.; Adsay, S.J.; Crawford, N.V. WHO Classification of Tumours. Digestive System Tumours; Bosman, F.T., Hruban, R.H., Carneiro, F., Theise, N.D., Eds.; WHO: Geneva, Switzerland, 2010; Volume 3. [Google Scholar]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.; et al. GLIM criteria for the diagnosis of malnutrition-A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziętarska, M.; Krawczyk-Lipiec, J.; Kraj, L.; Zaucha, R.; Małgorzewicz, S. Nutritional status assessment in colorectal cancer patients qualified to systemic treatment. Contemp. Oncol. 2017, 21, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.L.; Grundmann, O.; Williams, J.J.; Gordan, L.; George, T.J., Jr. Body composition changes differ by gender in stomach, colorectal, and biliary cancer patients with cachexia: Results from a pilot study. Cancer Med. 2018, 7, 3695–3703. [Google Scholar] [CrossRef] [Green Version]
- Gupta, D.; Lammersfeld, C.A.; Burrows, J.L.; Dahlk, S.L.; Vashi, P.G.; Grutsch, J.F.; Hoffman, S.; Lis, C.G. Bioelectrical impedance phase angle in clinical practice: Implications for prognosis in advanced colorectal cancer. Am. J. Clin. Nutr. 2004, 80, 1634–1638. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G.; Dahlk, S.L.; King, J.; Vashi, P.G.; Grutsch, J.F.; Lammersfeld, C.A. The relationship between bioelectrical impedance phase angle and subjective global assessment in advanced colorectal cancer. Nutr. J. 2008, 7, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergara-Fernandez, O.; Trejo-Avila, M.; Salgado-Nesme, N. Sarcopenia in patients with colorectal cancer: A comprehensive review. World J. Clin. Cases 2020, 8, 1188. [Google Scholar] [CrossRef] [PubMed]
- Fayh, A.P.T.; de Sousa, I.M. Comparison of revised EWGSOP2 criteria of sarcopenia in patients with cancer using different parameters of muscle mass. PLoS ONE 2021, 16, e0257446. [Google Scholar] [CrossRef]
- De Souza, B.U.; Souza, N.C.S.; Martucci, R.B.; Rodrigues, V.D.; De Pinho, N.B.; Gonzalez, M.C.; Avesani, C.M. Factors Associated with Sarcopenia in Patients with Colorectal Cancer. Nutr. Cancer 2018, 70, 176–183. [Google Scholar] [CrossRef]
- Von Haehling, S.; Morley, J.E.; Coats, A.J.; Anker, S.D. Ethical guidelines for publishing in the journal of cachexia, sarcopenia and muscle: Update 2017. J. Cachexia Sarcopenia Muscle 2017, 8, 1081–1083. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All | Female | Male | p Value | |
|---|---|---|---|---|
| N = 127 | N = 51 | N = 76 | ||
| Demographic variables Age (years) | 66.5 (8.89) | 67.9 (7.77) | 65.5 (9.51) | 0.131 |
| Weight (kg) | 76.5 (15.8) | 70.8 (15.2) | 80.3 (15.2) | 0.001 * |
| BMI (kg/m2) | 27.6 (4.51) | 27.6 (4.95) | 27.5 (4.22) | 0.889 |
| BIA | ||||
| PhA (°) | 5.79 (0.84) | 5.39 (0.66) | 6.07 (0.84) | <0.001 * |
| SPA (°) | 0.76 (1.11) | 1.06 (1.21) | 0.56 (0.99) | 0.016 * |
| FM (kg) | 19.1 (7.40) | 21.4 (7.34) | 17.7 (7.14) | 0.009 |
| SMI (cm2/m2) | 9.40 (1.82) | 7.81 (1.23) | 10.4 (1.32) | <0.001 * |
| Echography exploration | ||||
| RF-CSA | 4.10 (1.61) | 3.41 (1.58) | 4.53 (1.48) | <0.001 * |
| RF-CIR | 8.82 (1.53) | 8.21 (1.62) | 9.22 (1.34) | 0.001 * |
| RF-Y axis (thickness) | 1.29 (0.39) | 1.12 (0.36) | 1.40 (0.37) | <0.001 * |
| S-SAT | 0.89 (0.55) | 1.29 (0.58) | 0.64 (0.33) | <0.001 * |
| T-SAT | 1.66 (0.79) | 2.08 (0.80) | 1.39 (0.66) | <0.001 * |
| L-SAT | 0.89 (0.99) | 1.10 (0.57) | 0.76 (1.17) | 0.048 * |
| VAT | 0.57 (0.39) | 0.61 (0.43) | 0.54 (0.37) | 0.438 |
| Functional measurement | ||||
| HGS (right hand) | 27.6 (10.2) | 20.5 (5.62) | 31.5 (10.1) | <0.001 |
| HGS (left hand) | 26.3 (10.6) | 18.3 (5.60) | 30.6 (10.2) | <0.001 * |
| Biochemical variables | ||||
| Glucose (mg/dL) | 104 (21.9) | 105 (21.6) | 104 (22.3) | 0.808 |
| Triglycerides (mg/dL) | 127 (40.6) | 127 (39.4) | 127 (41.9) | 0.941 |
| Total cholesterol (mg/dL) | 188 (40.7) | 197 (41.3) | 181 (39.3) | 0.047 * |
| Albumin (g/dL) | 3.66 (0.51) | 3.67 (0.43) | 3.65 (0.56) | 0.861 |
| CRP (mg/L) | 8.73 (9.10) | 7.26 (8.57) | 9.88 (9.44) | 0.213 |
| 25-hydroxyvitamin D (ng/mL) | 20.2 (7.61) | 18.3 (7.89) | 22.4 (6.85) | 0.081 |
| Clinicopathological variables TNMs: | 0.553 | |||
| T1 + T2 | 35 (29.7%) | 12 (25.5%) | 23 (32.4%) | |
| T3 + T4 | 83 (70.3%) | 35 (74.5%) | 48 (67.6%) | |
| Cancer location: | 1.000 | |||
| Colon | 80 (64.0%) | 32 (64.0%) | 48 (64.0%) | |
| Rectum | 45 (36.0%) | 18 (36.0%) | 27 (36.0%) | |
| Treatment #: | 0.733 | |||
| No | 46 (36.8%) | 17 (34.0%) | 29 (38.7%) | |
| Yes | 79 (63.2%) | 33 (66.0%) | 46 (61.3%) | |
| Complications | 0.19 (0.40) | 0.10 (0.30) | 0.25 (0.44) | 0.022 * |
| Ileostomy/colostomy ##: | 0.965 | |||
| No | 96 (76.8%) | 39 (78.0%) | 57 (76.0%) | |
| Yes | 29 (23.2%) | 11 (22.0%) | 18 (24.0%) | |
| Hospital stays (days) | 7.38 (4.30) | 6.78 (3.74) | 7.78 (4.61) | 0.185 |
| Survival: | 0.523 | |||
| No | 114 (91.2%) | 47 (94.0%) | 67 (89.3%) | |
| Yes | 11 (8.80%) | 3 (6.00%) | 8 (10.7%) |
| Variables | Complications | Sarcopenia | ||
|---|---|---|---|---|
| OR [95% CI] | OR [95% CI] | OR [95% CI] | OR [95% CI] | |
| Males | Females | Males | Females | |
| Anthropometric | ||||
| BMI (kg/m2) | 0.89 [0.78;1.02] | 0.86 [0.70;1.06] | 0.42 [0.24;0.74] * | 0.63 [0.43;0.91] * |
| BIA | ||||
| PhA (°) | 0.83 [0.47;1.45] | 0.15 [0.03;0.81] * | 0.42 [0.19;0.95] * | 0.27 [0.07;1.07] |
| SPA (°) | 0.93 [0.58;1.48] | 0.53 [0.21;1.33] | 0.48 [0.23;1.01] | 0.55 [0.22;1.36] |
| Echography | ||||
| RF-CSA | 0.72 [0.47;1.09] | 0.22 [0.05;1.01] | 0.51 [0.26;0.97] * | 0.34 [0.09;1.28] |
| RF-CIR | 0.83 [0.54;1.26] | 0.69 [0.35;1.38] | 0.74 [0.42;1.28] | 0.86 [0.46;1.61] |
| L-SAT | 1.30 [0.79;2.15] | 0.82 [0.15;4.56] | 0.29 [0.02;3.58] | 0.03 [0.00;1.83] |
| S-SAT | 0.22 [0.02;2.28] | 0.51 [0.09;3.01] | 0.10 [0.00;3.01] | 0.20 [0.02;1.71] |
| T-SAT | 0.46 [0.17;1.27] | 0.82 [0.25;2.75] | 0.58 [0.18;1.84] | 0.04 [0.00;0.77] * |
| VAT | 0.37 [0.06;2.36] | 0.23 [0.01;7.34] | 1.46 [0.19;11.3] | 0.01 [0.00;13.3] |
| Functional | ||||
| RHG | 0.95 [0.85;1.06] | 0.88 [0.51;1.49] | 1.01 [0.89;1.14] | 0.93 [0.66;1.31] |
| LHG | 0.87 * [0.76;1.00] | 0.99 [0.67;1.45] | 0.99 [0.87;1.11] | 0.92 [0.68;1.25] |
| Inflammation | ||||
| C/A ratio | 1.01 [0.98;1.04] | 1.04 [0.99;1.09] | 1.01 [0.97;1.06] | 1.02 [0.98;1.06] |
| Variables | Complications | Sarcopenia | ||
|---|---|---|---|---|
| HR (SD) | HR (SD) | HR (SD) | HR (SD) | |
| Males | Females | Males | Females | |
| BIA | ||||
| PhA (°) | −0.09 (0.34) | −2.52 (1.19) * | −2.29 (0.96) * | −5.26 (2.78) * |
| SPA (°) | −0.07 (0.23) | −1.08 (0.63) | −1.04 (0.50) * | −3.53 (1.88) |
| Echography | ||||
| RF-CSA | −0.27 (0.26) | −1.32 (0.81) | −0.14 (0.41) | −1.28 (1.10) |
| T-SAT | NA | NA | 0.42 (1.03) | −2.46 (1.72) |
| Functional | ||||
| LHG | −0.45 (0.30) | 252.2 (447) | NA | NA |
| AUC | Cut-off | Sensitivity | Specificity | p Value | |
|---|---|---|---|---|---|
| Complications in females | |||||
| PhA | 0.893 | 4.85 | 80% | 88.9% | 0.001 * |
| Sarcopenia in males | |||||
| PhA | 0.959 | 5.19 | 90.9% | 92.3% | 0.026 * |
| SPA | 0.958 | 0.17 | 90.9% | 92.3% | 0.036 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vegas-Aguilar, I.M.; Guirado-Peláez, P.; Fernández-Jiménez, R.; Boughanem, H.; Tinahones, F.J.; Garcia-Almeida, J.M. Exploratory Assessment of Nutritional Evaluation Tools as Predictors of Complications and Sarcopenia in Patients with Colorectal Cancer. Cancers 2023, 15, 847. https://doi.org/10.3390/cancers15030847
Vegas-Aguilar IM, Guirado-Peláez P, Fernández-Jiménez R, Boughanem H, Tinahones FJ, Garcia-Almeida JM. Exploratory Assessment of Nutritional Evaluation Tools as Predictors of Complications and Sarcopenia in Patients with Colorectal Cancer. Cancers. 2023; 15(3):847. https://doi.org/10.3390/cancers15030847
Chicago/Turabian StyleVegas-Aguilar, Isabel M., Patricia Guirado-Peláez, Rocío Fernández-Jiménez, Hatim Boughanem, Francisco J. Tinahones, and Jose Manuel Garcia-Almeida. 2023. "Exploratory Assessment of Nutritional Evaluation Tools as Predictors of Complications and Sarcopenia in Patients with Colorectal Cancer" Cancers 15, no. 3: 847. https://doi.org/10.3390/cancers15030847
APA StyleVegas-Aguilar, I. M., Guirado-Peláez, P., Fernández-Jiménez, R., Boughanem, H., Tinahones, F. J., & Garcia-Almeida, J. M. (2023). Exploratory Assessment of Nutritional Evaluation Tools as Predictors of Complications and Sarcopenia in Patients with Colorectal Cancer. Cancers, 15(3), 847. https://doi.org/10.3390/cancers15030847