



MRI-Based Radiomics Combined with Deep Learning for Distinguishing IDH-Mutant WHO Grade 4 Astrocytomas from IDH-Wild-Type Glioblastomas
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Determination of IDH Mutational Status by Immunohistochemistry and Sequencing
2.3. MRI Data Acquisition
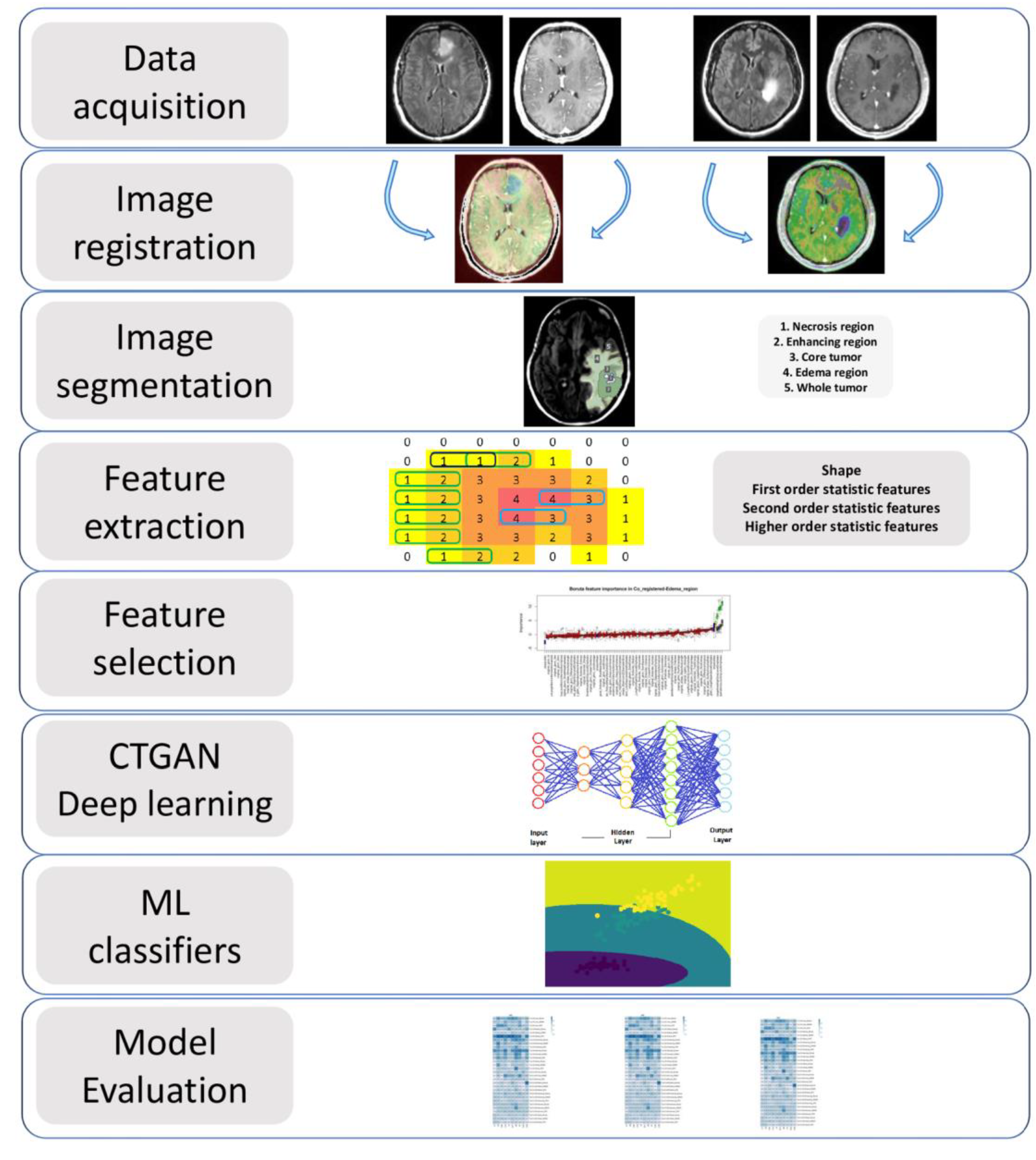
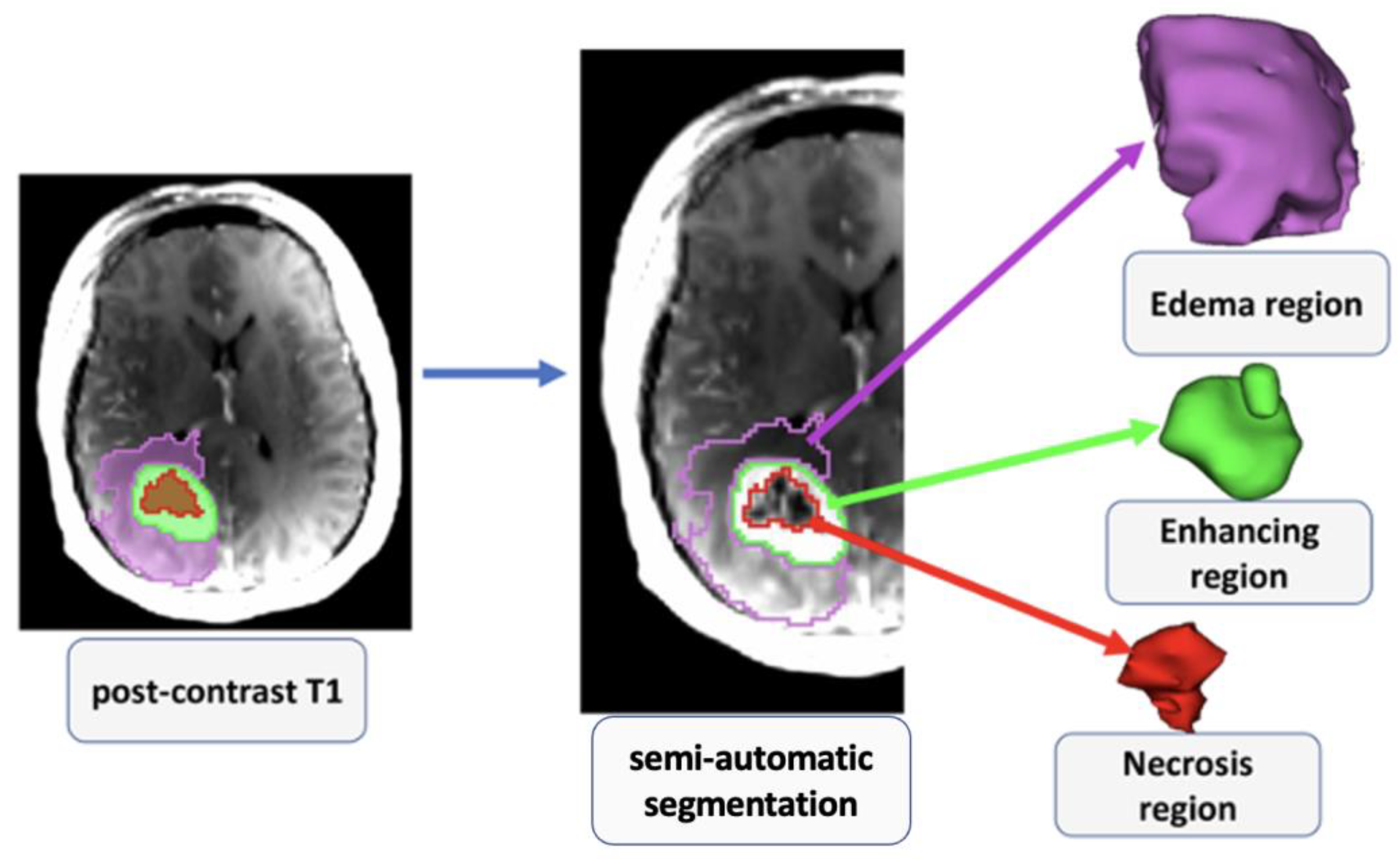
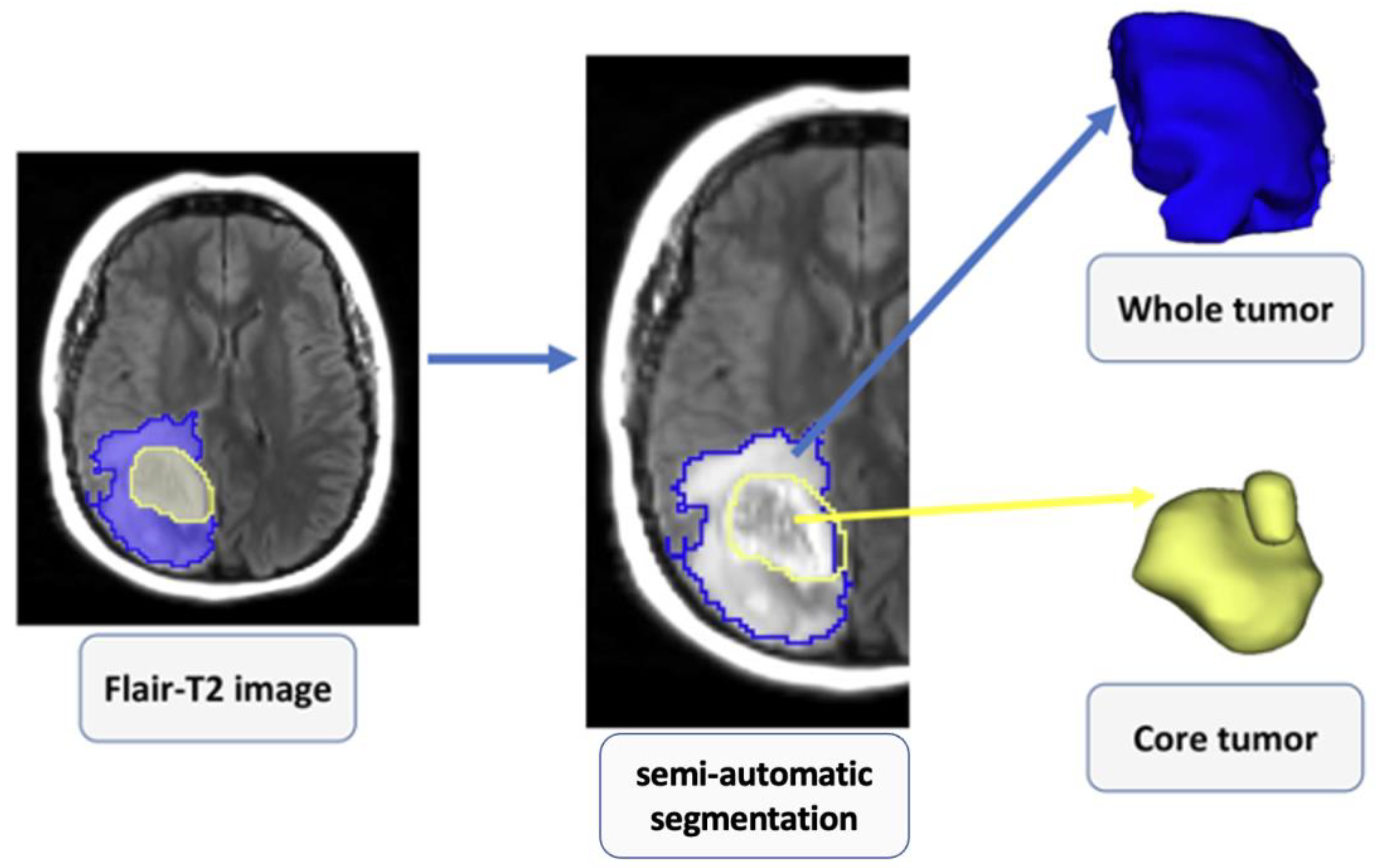
2.4. Image Processing
2.5. Radiomic Feature Extraction
2.6. Radiomics Feature Selection/Dimension Reduction
2.7. Deep Learning Approach for Data Augmentation
2.8. Machine Learning Classifiers for Prediction Model Building
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wen, P.Y.; Weller, M.; Lee, E.Q.; Alexander, B.M.; Barnholtz-Sloan, J.S.; Barthel, F.P.; Batchelor, T.T.; Bindra, R.S.; Chang, S.M.; Chiocca, E.A. Glioblastoma in adults: A Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) consensus review on current management and future directions. Neuro Oncol. 2020, 22, 1073–1113. [Google Scholar] [CrossRef] [PubMed]
- Alexander, B.M.; Cloughesy, T.F. Platform Trials Arrive on Time for Glioblastoma; Oxford University Press: New York, NY, USA, 2018; pp. 723–725. [Google Scholar]
- Thakkar, J.P.; Dolecek, T.A.; Horbinski, C.; Ostrom, Q.T.; Lightner, D.D.; Barnholtz-Sloan, J.S.; Villano, J.L. Epidemiologic and Molecular Prognostic Review of GlioblastomaGBM Epidemiology and Biomarkers. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1985–1996. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Vigneswaran, K.; Neill, S.; Hadjipanayis, C.G. Beyond the World Health Organization grading of infiltrating gliomas: Advances in the molecular genetics of glioma classification. Ann. Transl. Med. 2015, 3, 95. [Google Scholar]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.; Pfister, S.M.; Reifenberger, G. The 2021 WHO classification of tumors of the central nervous system: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Yan, W.; Zhang, W.; You, G.; Bao, Z.; Wang, Y.; Liu, Y.; Kang, C.; You, Y.; Wang, L.; Jiang, T. Correlation of IDH1 mutation with clinicopathologic factors and prognosis in primary glioblastoma: A report of 118 patients from China. PLoS ONE 2012, 7, e30339. [Google Scholar] [CrossRef]
- Zhang, C.-B.; Bao, Z.-S.; Wang, H.-J.; Yan, W.; Liu, Y.-W.; Li, M.-Y.; Zhang, W.; Chen, L.; Jiang, T. Correlation of IDH1/2 mutation with clinicopathologic factors and prognosis in anaplastic gliomas: A report of 203 patients from China. J. Cancer Res. Clin. Oncol. 2014, 140, 45–51. [Google Scholar] [CrossRef]
- Parsons, D.W.; Jones, S.; Zhang, X.; Lin, J.C.-H.; Leary, R.J.; Angenendt, P.; Mankoo, P.; Carter, H.; Siu, I.-M.; Gallia, G.L. An integrated genomic analysis of human glioblastoma multiforme. Science 2008, 321, 1807–1812. [Google Scholar] [CrossRef]
- Yan, H.; Parsons, D.W.; Jin, G.; McLendon, R.; Rasheed, B.A.; Yuan, W.; Kos, I.; Batinic-Haberle, I.; Jones, S.; Riggins, G.J. IDH1 and IDH2 mutations in gliomas. N. Engl. J. Med. 2009, 360, 765–773. [Google Scholar] [CrossRef]
- Preusser, M.; Wöhrer, A.; Stary, S.; Höftberger, R.; Streubel, B.; Hainfellner, J.A. Value and limitations of immunohistochemistry and gene sequencing for detection of the IDH1-R132H mutation in diffuse glioma biopsy specimens. J. Neuropathol. Exp. Neurol. 2011, 70, 715–723. [Google Scholar] [CrossRef]
- Dang, L.; White, D.W.; Gross, S.; Bennett, B.D.; Bittinger, M.A.; Driggers, E.M.; Fantin, V.R.; Jang, H.G.; Jin, S.; Keenan, M.C. Cancer-associated IDH1 mutations produce 2-hydroxyglutarate. Nature 2009, 462, 739–744. [Google Scholar] [CrossRef] [Green Version]
- Pope, W.B.; Prins, R.M.; Albert Thomas, M.; Nagarajan, R.; Yen, K.E.; Bittinger, M.A.; Salamon, N.; Chou, A.P.; Yong, W.H.; Soto, H. Non-invasive detection of 2-hydroxyglutarate and other metabolites in IDH1 mutant glioma patients using magnetic resonance spectroscopy. J. Neuro-Oncol. 2012, 107, 197–205. [Google Scholar] [CrossRef]
- Choi, C.; Ganji, S.K.; DeBerardinis, R.J.; Hatanpaa, K.J.; Rakheja, D.; Kovacs, Z.; Yang, X.-L.; Mashimo, T.; Raisanen, J.M.; Marin-Valencia, I. 2-hydroxyglutarate detection by magnetic resonance spectroscopy in IDH-mutated patients with gliomas. Nat. Med. 2012, 18, 624–629. [Google Scholar] [CrossRef]
- Verma, G.; Mohan, S.; Nasrallah, M.P.; Brem, S.; Lee, J.Y.; Chawla, S.; Wang, S.; Nagarajan, R.; Thomas, M.A.; Poptani, H. Non-invasive detection of 2-hydroxyglutarate in IDH-mutated gliomas using two-dimensional localized correlation spectroscopy (2D L-COSY) at 7 Tesla. J. Transl. Med. 2016, 14, 274. [Google Scholar] [CrossRef]
- Ichimura, K.; Pearson, D.M.; Kocialkowski, S.; Bäcklund, L.M.; Chan, R.; Jones, D.T.; Collins, V.P. IDH1 mutations are present in the majority of common adult gliomas but rare in primary glioblastomas. Neuro Oncol. 2009, 11, 341–347. [Google Scholar] [CrossRef]
- Villanueva-Meyer, J.E.; Mabray, M.C.; Cha, S. Current clinical brain tumor imaging. Neurosurgery 2017, 81, 397–415. [Google Scholar] [CrossRef]
- Hosseini, S.A.; Hajianfar, G.; Shiri, I.; Zaidi, H. Lymphovascular Invasion Prediction in Lung Cancer Using Multi-Segmentation PET Radiomics and Multi-Machine Learning Algorithms. In Proceedings of the 2021 IEEE Nuclear Science Symposium and Medical Imaging Conference (NSS/MIC), Piscataway, NJ, USA, 16–23 October 2021. [Google Scholar]
- Hosseini, S.A.; Hajianfar, G.; Shiri, I.; Zaidi, H. Lung Cancer Recurrence Prediction Using Radiomics Features of PET Tumor Sub-Volumes and Multi-Machine Learning Algorithms. In Proceedings of the 2021 IEEE Nuclear Science Symposium and Medical Imaging Conference (NSS/MIC), Piscataway, NJ, USA, 16–23 October 2021. [Google Scholar]
- Hosseini, S.A.; Shiri, I.; Hajianfar, G.; Bahadorzadeh, B.; Ghafarian, P.; Zaidi, H.; Ay, M.R. Synergistic impact of motion and acquisition/reconstruction parameters on 18F-FDG PET radiomic features in non-small cell lung cancer: Phantom and clinical studies. Med. Phys. 2022, 49, 3783–3796. [Google Scholar] [CrossRef]
- Hosseini, S.A.; Hajianfar, G.; Shiri, I.; Zaidi, H. PET Image Radiomics Feature Variability in Lung Cancer: Impact of Image Segmentation. In Proceedings of the 2021 IEEE Nuclear Science Symposium and Medical Imaging Conference (NSS/MIC), Piscataway, NJ, USA, 16–23 October 2021. [Google Scholar]
- Hosseini, S.A.; Shiri, I.; Hajianfar, G.; Ghafarian, P.; Karam, M.B.; Ay, M.R. The impact of preprocessing on the PET-CT radiomics features in non-small cell lung cancer. Front. Biomed. Technol. 2021, 8, 261–272. [Google Scholar] [CrossRef]
- Ruan, Z.; Mei, N.; Lu, Y.; Xiong, J.; Li, X.; Zheng, W.; Liu, L.; Yin, B. A Comparative and Summative Study of Radiomics-based Overall Survival Prediction in Glioblastoma Patients. J. Comput. Assist. Tomogr. 2022, 46, 470–479. [Google Scholar] [CrossRef]
- Aftab, K.; Aamir, F.B.; Mallick, S.; Mubarak, F.; Pope, W.B.; Mikkelsen, T.; Rock, J.P.; Enam, S.A. Radiomics for precision medicine in glioblastoma. J. Neuro-Oncol. 2022, 156, 217–231. [Google Scholar] [CrossRef]
- Baine, M.; Burr, J.; Du, Q.; Zhang, C.; Liang, X.; Krajewski, L.; Zima, L.; Rux, G.; Zhang, C.; Zheng, D. The potential use of radiomics with pre-radiation therapy MR imaging in predicting risk of pseudoprogression in glioblastoma patients. J. Imaging 2021, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Patel, M.; Natarajan, K.; Ughratdar, I.; Sanghera, P.; Jena, R.; Watts, C.; Sawlani, V. Machine learning-based radiomic, clinical and semantic feature analysis for predicting overall survival and MGMT promoter methylation status in patients with glioblastoma. Magn. Reson. Imaging 2020, 74, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Kinoshita, M.; Fujita, K.; Fukai, J.; Hayashi, N.; Uematsu, Y.; Okita, Y.; Nonaka, M.; Moriuchi, S.; Uda, T. Radiomics and MGMT promoter methylation for prognostication of newly diagnosed glioblastoma. Sci. Rep. 2019, 9, 14435. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.A.; Shiri, I.; Hajianfar, G.; Bagley, S.; Nasrallah, M.; O’Rourke, D.M.; Mohan, S.; Chawla, S. MRI based Radiomics for Distinguishing IDH-mutant from IDH wild-type Grade-4 Astrocytomas. In Proceedings of the 31st Annual Meeting of ISMRM, London, UK, 7–12 May 2022. [Google Scholar]
- Lee, M.H.; Kim, J.; Kim, S.-T.; Shin, H.-M.; You, H.-J.; Choi, J.W.; Seol, H.J.; Nam, D.-H.; Lee, J.-I.; Kong, D.-S. Prediction of IDH1 mutation status in glioblastoma using machine learning technique based on quantitative radiomic data. World Neurosurg. 2019, 125, e688–e696. [Google Scholar] [CrossRef]
- Hsieh, K.L.-C.; Chen, C.-Y.; Lo, C.-M. Radiomic model for predicting mutations in the isocitrate dehydrogenase gene in glioblastomas. Oncotarget 2017, 8, 45888. [Google Scholar] [CrossRef]
- Nasrallah, M.P.; Binder, Z.A.; Oldridge, D.A.; Zhao, J.; Lieberman, D.B.; Roth, J.J.; Watt, C.D.; Sukhadia, S.; Klinman, E.; Daber, R.D. Molecular neuropathology in practice: Clinical profiling and integrative analysis of molecular alterations in glioblastoma. Acad. Pathol. 2019, 6, 2374289519848353. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Leger, S.; Vallières, M.; Löck, S. Image biomarker standardisation initiative. arXiv 2016, arXiv:1612.07003. [Google Scholar]
- Gupta, A.; Bhatt, D.; Pandey, A. Transitioning from Real to Synthetic data: Quantifying the bias in model. arXiv 2021, arXiv:2105.04144. [Google Scholar]
- Dina, A.S.; Siddique, A.; Manivannan, D. Effect of Balancing Data Using Synthetic Data on the Performance of Machine Learning Classifiers for Intrusion Detection in Computer Networks. arXiv 2022, arXiv:2204.00144. [Google Scholar] [CrossRef]
- Pereira, M.; Kshirsagar, M.; Mukherjee, S.; Dodhia, R.; Ferres, J.L. An Analysis of the Deployment of Models Trained on Private Tabular Synthetic Data: Unexpected Surprises. arXiv 2021, arXiv:2106.10241. [Google Scholar]
- Stadler, T.; Oprisanu, B.; Troncoso, C. Synthetic data–anonymisation groundhog day. In Proceedings of the 31st USENIX Security Symposium (USENIX Security 22), Boston, MA, USA, 10–12 August 2022. [Google Scholar]
- Sepehri, S.; Tankyevych, O.; Upadhaya, T.; Visvikis, D.; Hatt, M.; Cheze Le Rest, C. Comparison and Fusion of Machine Learning Algorithms for Prospective Validation of PET/CT Radiomic Features Prognostic Value in Stage II-III Non-Small Cell Lung Cancer. Diagnostics 2021, 11, 675. [Google Scholar] [CrossRef]
- Hannun, A.; Guo, C.; van der Maaten, L. Measuring data leakage in machine-learning models with Fisher information. In Proceedings of the Thirty-First International Joint Conference on Artificial Intelligence (IJCAI-22), Vienna, Austria, 23–29 July 2022. [Google Scholar]
- Dietterich, T.G. Ensemble methods in machine learning. In Proceedings of the International Workshop on Multiple Classifier Systems, Cagliari, Italy, 21–23 June 2000; Springer: Berlin/Heidelberg, Germany, 2000. [Google Scholar]
- Hartmann, C.; Hentschel, B.; Wick, W.; Capper, D.; Felsberg, J.; Simon, M.; Westphal, M.; Schackert, G.; Meyermann, R.; Pietsch, T. Patients with IDH1 wild type anaplastic astrocytomas exhibit worse prognosis than IDH1-mutated glioblastomas, and IDH1 mutation status accounts for the unfavorable prognostic effect of higher age: Implications for classification of gliomas. Acta Neuropathol. 2010, 120, 707–718. [Google Scholar] [CrossRef]
- Bhandari, A.P.; Liong, R.; Koppen, J.; Murthy, S.; Lasocki, A. Noninvasive determination of IDH and 1p19q status of lower-grade gliomas using MRI radiomics: A systematic review. Am. J. Neuroradiol. 2021, 42, 94–101. [Google Scholar] [CrossRef]
- Akay, A.; Rüksen, M.; Islekel, S. Magnetic resonance imaging-guided stereotactic biopsy: A review of 83 cases with outcomes. Asian J. Neurosurg. 2019, 14, 90. [Google Scholar] [CrossRef]
- Horbinski, C. What do we know about IDH1/2 mutations so far, and how do we use it? Acta Neuropathol. 2013, 125, 621–636. [Google Scholar] [CrossRef]
- Gutman, D.A.; Dunn, W.D.; Grossmann, P.; Cooper, L.A.; Holder, C.A.; Ligon, K.L.; Alexander, B.M.; Aerts, H.J. Somatic mutations associated with MRI-derived volumetric features in glioblastoma. Neuroradiology 2015, 57, 1227–1237. [Google Scholar] [CrossRef]
- Askari, P.; Dimitrov, I.E.; Ganji, S.K.; Tiwari, V.; Levy, M.; Patel, T.R.; Pan, E.; Mickey, B.E.; Malloy, C.R.; Maher, E.A. Spectral fitting strategy to overcome the overlap between 2-hydroxyglutarate and lipid resonances at 2.25 ppm. Magn. Reson. Med. 2021, 86, 1818–1828. [Google Scholar] [CrossRef]
- Choi, C.; Raisanen, J.M.; Ganji, S.K.; Zhang, S.; McNeil, S.S.; An, Z.; Madan, A.; Hatanpaa, K.J.; Vemireddy, V.; Sheppard, C.A. Prospective longitudinal analysis of 2-hydroxyglutarate magnetic resonance spectroscopy identifies broad clinical utility for the management of patients with IDH-mutant glioma. J. Clin. Oncol. 2016, 34, 4030. [Google Scholar] [CrossRef]
- An, Z.; Ganji, S.K.; Tiwari, V.; Pinho, M.C.; Patel, T.; Barnett, S.; Pan, E.; Mickey, B.E.; Maher, E.A.; Choi, C. Detection of 2-hydroxyglutarate in brain tumors by triple-refocusing MR spectroscopy at 3T in vivo. Magn. Reson. Med. 2017, 78, 40–48. [Google Scholar] [CrossRef]
- Sonoda, Y.; Shibahara, I.; Kawaguchi, T.; Saito, R.; Kanamori, M.; Watanabe, M.; Suzuki, H.; Kumabe, T.; Tominaga, T. Association between molecular alterations and tumor location and MRI characteristics in anaplastic gliomas. Brain Tumor Pathol. 2015, 32, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Baldock, A.L.; Yagle, K.; Born, D.E.; Ahn, S.; Trister, A.D.; Neal, M.; Johnston, S.K.; Bridge, C.A.; Basanta, D.; Scott, J. Invasion and proliferation kinetics in enhancing gliomas predict IDH1 mutation status. Neuro Oncol. 2014, 16, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.; Yu, L.; Li, H.; Ou, Y.; Qiu, X.; Ding, Y.; Han, H.; Zhang, X. Isocitrate dehydrogenase mutation is associated with tumor location and magnetic resonance imaging characteristics in astrocytic neoplasms. Oncol. Lett. 2014, 7, 1895–1902. [Google Scholar] [CrossRef] [PubMed]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, S.; Luo, M.; Li, Y. Machine Learning for the Prediction of Lymph Nodes Micrometastasis in Patients with Non-Small Cell Lung Cancer: A Comparative Analysis of Two Practical Prediction Models for Gross Target Volume Delineation. Cancer Manag. Res. 2021, 13, 4811. [Google Scholar] [CrossRef]
- Zhu, L.; Chen, Y.; Ghamisi, P.; Benediktsson, J.A. Generative adversarial networks for hyperspectral image classification. IEEE Trans. Geosci. Remote Sens. 2018, 56, 5046–5063. [Google Scholar] [CrossRef]
- Creswell, A.; White, T.; Dumoulin, V.; Arulkumaran, K.; Sengupta, B.; Bharath, A.A. Generative adversarial networks: An overview. IEEE Signal Process. Mag. 2018, 35, 53–65. [Google Scholar] [CrossRef]
- Zhang, B.; Chang, K.; Ramkissoon, S.; Tanguturi, S.; Bi, W.L.; Reardon, D.A.; Ligon, K.L.; Alexander, B.M.; Wen, P.Y.; Huang, R.Y. Multimodal MRI features predict isocitrate dehydrogenase genotype in high-grade gliomas. Neuro Oncol. 2017, 19, 109–117. [Google Scholar] [CrossRef]
- Lee, S.; Choi, S.H.; Ryoo, I.; Yoon, T.J.; Kim, T.M.; Lee, S.-H.; Park, C.-K.; Kim, J.-H.; Sohn, C.-H.; Park, S.-H. Evaluation of the microenvironmental heterogeneity in high-grade gliomas with IDH1/2 gene mutation using histogram analysis of diffusion-weighted imaging and dynamic-susceptibility contrast perfusion imaging. J. Neuro-Oncol. 2015, 121, 141–150. [Google Scholar] [CrossRef]
- Metellus, P.; Coulibaly, B.; Colin, C.; de Paula, A.M.; Vasiljevic, A.; Taieb, D.; Barlier, A.; Boisselier, B.; Mokhtari, K.; Wang, X.W. Absence of IDH mutation identifies a novel radiologic and molecular subtype of WHO grade II gliomas with dismal prognosis. Acta Neuropathol. 2010, 120, 719–729. [Google Scholar] [CrossRef]
- Xing, Z.; Yang, X.; She, D.; Lin, Y.; Zhang, Y.; Cao, D. Noninvasive assessment of IDH mutational status in World Health Organization grade II and III astrocytomas using DWI and DSC-PWI combined with conventional MR imaging. Am. J. Neuroradiol. 2017, 38, 1138–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Radiomic Feature Combination | AUC | Accuracy | Sensitivity | Specificity | PR_AUC |
|---|---|---|---|---|---|
| Or_PC_T1_Core_AB_Kbest | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Or_PC_T1_Core_KN_Kbest | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Or_PC_T1_Core_LR_Kbest | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Or_PC_T1_Core_MLP_Kbest | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Or_T2-FLAIR_Enhancing_DT_Kbest | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Or_T2-FLAIR_Enhancing_DT_mRmR | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Or_T2-FLAIR_Enhancing_GB_mRmR | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Or_T2-FLAIR_Enhancing_RF_mRmR | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Or_PC_T1_Enhancing_HGB_RFE | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Or_PC_T1_Enhancing_HGB_mRmR | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Radiomic Feature Combination | AUC | Accuracy | Sensitivity | Specificity | PR_AUC |
|---|---|---|---|---|---|
| Ge_PC_T1_Core_GNB_Kbest | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Ge_PC_T1_Core_PA_RFE | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Ge_T2_FLAIR_Enhancing_Bagging_Kbest | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Ge_T2_FLAIR_Enhancing_DT_Kbest | 0.93 | 0.92 | 1 | 0.86 | 0.92 |
| Ge_T2_FLAIR_Whole_AB_Kbest | 0.90 | 0.92 | 0.80 | 1 | 0.94 |
| Ge_PC_T1_Core_RF_Kbest | 0.90 | 0.92 | 0.80 | 1 | 0.94 |
| Ge_PC_T1_Core_RF_RFE | 0.90 | 0.92 | 0.80 | 1 | 0.94 |
| Ge_PC_T1_Core_HGB_Kbest | 0.90 | 0.92 | 0.80 | 1 | 0.94 |
| Ge_PC_T1_Edema_AB_Kbest | 0.90 | 0.92 | 0.80 | 1 | 0.94 |
| Ge_PC_T1_Edema_Bagging_Kbest | 0.90 | 0.92 | 0.80 | 1 | 0.94 |
| Radiomic Feature Combination | AUC | Accuracy | Sensitivity | Specificity | PR_AUC |
| Ge_PC_T1_Necrosis_Bagging_mRmR | 0.92 | 0.92 | 0.91 | 0.94 | 0.93 |
| Ge_PC_T1_Necrosis_RF_mRmR | 0.92 | 0.92 | 0.91 | 0.94 | 0.93 |
| Ge_PC_T1_Edema_KN_mRmR | 0.92 | 0.92 | 0.91 | 0.94 | 0.93 |
| Ge_PC_T1_Necrosis_KN_RFE | 0.89 | 0.89 | 0.91 | 0.87 | 0.89 |
| Ge_PC_T1_Edema_HGB_RFE | 0.89 | 0.89 | 0.91 | 0.87 | 0.89 |
| Ge_PC_T1_Necrosis_KN_RFE | 0.88 | 0.89 | 0.82 | 0.94 | 0.90 |
| Ge_PC_T1_Necrosis_KN_RFE | 0.88 | 0.89 | 0.82 | 0.94 | 0.90 |
| Ge_PC_T1_Edema_HGB_RFE | 0.88 | 0.89 | 0.82 | 0.94 | 0.90 |
| Ge_PC_T1_Edema_HGB_RFE | 0.88 | 0.89 | 0.82 | 0.94 | 0.90 |
| Ge_PC_T1_Core_KN_RFE | 0.88 | 0.89 | 0.82 | 0.94 | 0.90 |
| Radiomic Feature Combination | AUC | Accuracy | Sensitivity | Specificity | PR_AUC |
|---|---|---|---|---|---|
| Ge_PC_T1_Core_LR_Kbest | 0.91 | 0.92 | 0.86 | 0.96 | 0.92 |
| Ge_PC_T1_Core_Ridge_Kbest | 0.89 | 0.89 | 0.86 | 0.92 | 0.88 |
| Ge_PC_T1_Core_SVC_mRmR | 0.86 | 0.89 | 0.71 | 1 | 0.91 |
| Ge_PC_T1_Core_LDA_Kbest | 0.84 | 0.84 | 0.86 | 0.83 | 0.83 |
| Ge_T2_FLAIR_Core_HGB_Kbest | 0.82 | 0.79 | 0.93 | 0.71 | 0.80 |
| Ge_T2_FLAIR_Core_LR_Kbest | 0.81 | 0.84 | 0.71 | 0.92 | 0.83 |
| Ge_PC_T1_Edema_GB_Kbest | 0.81 | 0.84 | 0.71 | 0.92 | 0.83 |
| Ge_T2_FLAIR_Core_LDA_Kbest | 0.81 | 0.81 | 0.78 | 0.83 | 0.80 |
| Ge_T2_FLAIR_Core_Ridge_Kbest | 0.81 | 0.81 | 0.78 | 0.83 | 0.80 |
| Ge_PC_T1_Enhancing_QDA_Kbest | 0.80 | 0.79 | 0.86 | 0.75 | 0.79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosseini, S.A.; Hosseini, E.; Hajianfar, G.; Shiri, I.; Servaes, S.; Rosa-Neto, P.; Godoy, L.; Nasrallah, M.P.; O’Rourke, D.M.; Mohan, S.; et al. MRI-Based Radiomics Combined with Deep Learning for Distinguishing IDH-Mutant WHO Grade 4 Astrocytomas from IDH-Wild-Type Glioblastomas. Cancers 2023, 15, 951. https://doi.org/10.3390/cancers15030951
Hosseini SA, Hosseini E, Hajianfar G, Shiri I, Servaes S, Rosa-Neto P, Godoy L, Nasrallah MP, O’Rourke DM, Mohan S, et al. MRI-Based Radiomics Combined with Deep Learning for Distinguishing IDH-Mutant WHO Grade 4 Astrocytomas from IDH-Wild-Type Glioblastomas. Cancers. 2023; 15(3):951. https://doi.org/10.3390/cancers15030951
Chicago/Turabian StyleHosseini, Seyyed Ali, Elahe Hosseini, Ghasem Hajianfar, Isaac Shiri, Stijn Servaes, Pedro Rosa-Neto, Laiz Godoy, MacLean P. Nasrallah, Donald M. O’Rourke, Suyash Mohan, and et al. 2023. "MRI-Based Radiomics Combined with Deep Learning for Distinguishing IDH-Mutant WHO Grade 4 Astrocytomas from IDH-Wild-Type Glioblastomas" Cancers 15, no. 3: 951. https://doi.org/10.3390/cancers15030951
APA StyleHosseini, S. A., Hosseini, E., Hajianfar, G., Shiri, I., Servaes, S., Rosa-Neto, P., Godoy, L., Nasrallah, M. P., O’Rourke, D. M., Mohan, S., & Chawla, S. (2023). MRI-Based Radiomics Combined with Deep Learning for Distinguishing IDH-Mutant WHO Grade 4 Astrocytomas from IDH-Wild-Type Glioblastomas. Cancers, 15(3), 951. https://doi.org/10.3390/cancers15030951